
Exploring the Experiences of Family Members When a Patient Is Admitted to the ICU with a Severe Traumatic Brain Injury: A Scoping Review


Abstract
:1. Introduction
1.1. Background
1.2. Rationale
1.3. Research Question and Objectives
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
2.5. Selection of Sources of Evidence
2.6. Data Charting Process
2.7. Critical Appraisal
2.8. Synthesis of Results
3. Results
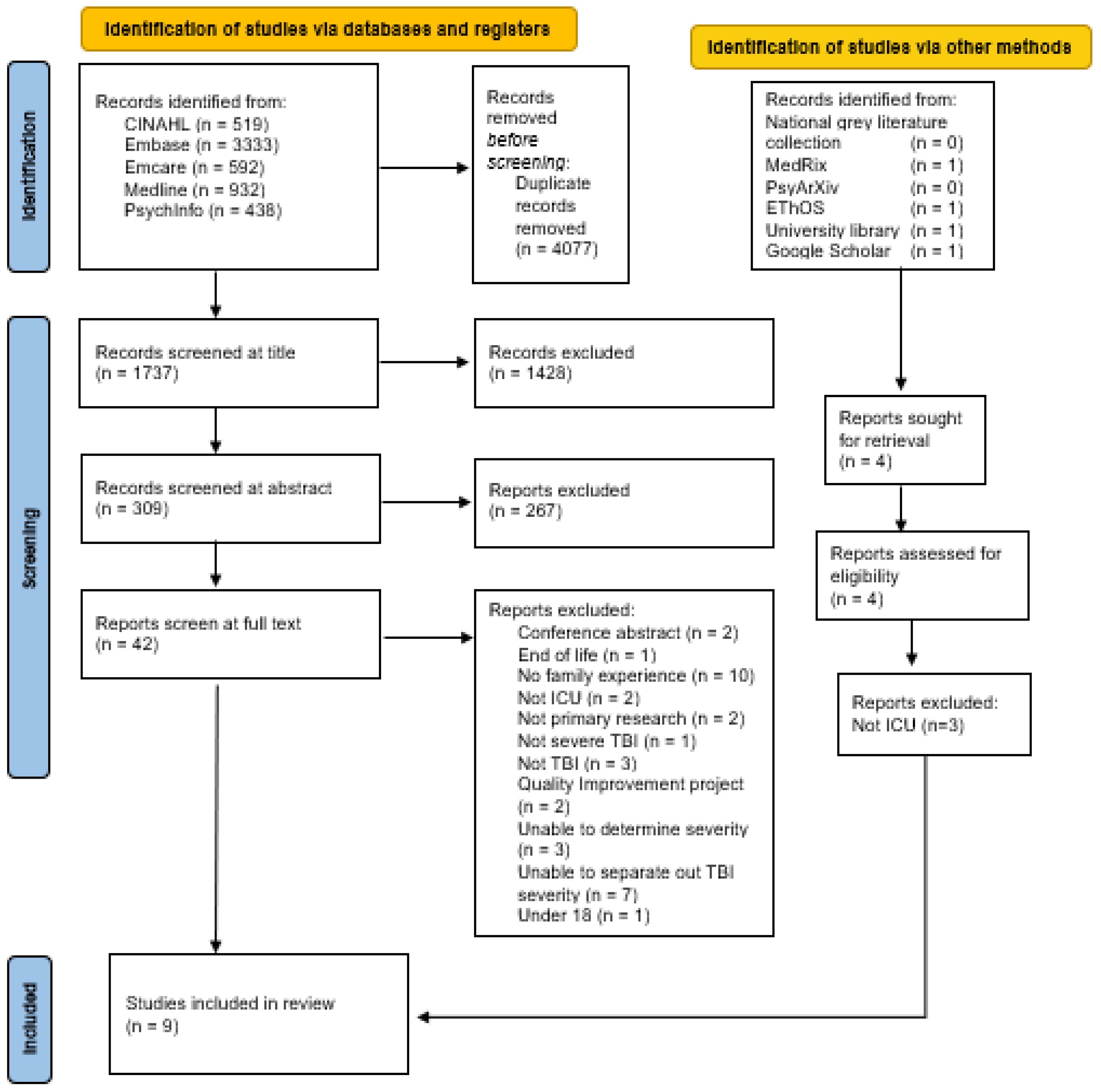
3.1. Selection of Sources of Evidence
3.2. Characteristics of Sources of Evidence
3.3. Methodological Approaches
3.4. Critical Appraisal within Sources of Evidence
3.5. Synthesis of Results
3.6. Narrative Synthesis
3.6.1. Communication with Clinical Team
3.6.2. Uncertainty
Uncertainty in Decision Making
Uncertainty in Prognosis
Existential Uncertainty
3.6.3. Involvement in Care
Family Involvement in ICU Care
Future Involvement after ICU
4. Discussion
Limitations
5. Conclusions
Recommendations or Implications for Further Research and Practice
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Available online: https://www.who.int/ (accessed on 17 April 2023).
- Warren, A.M.; Rainey, E.E.; Weddle, R.J.; Bennett, M.; Roden-Foreman, K.; Foreman, M.L. The intensive care unit experience: Psychological impact on family members of patients with and without traumatic brain injury. Rehabil. Psychol. 2016, 61, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.; Schlebusch, L.; Gaede, B. The impact of stress on depression, ill health and coping in family members caring for patients with acquired brain injury. S. Afr. Fam. Pract. 2020, 62 Pt 4, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Coco, K.; Tossavainen, K.; Jääskeläinen, J.E.; Turunen, H. Support for traumatic brain injury patients’ family members in neurosurgical nursing: A systematic review. J. Neurosci. Nurs. 2011, 43, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Whiffin, C.J.; Gracey, F.; Ellis-Hill, C. The experience of families following traumatic brain injury in adult populations: A meta-synthesis of narrative structures. Int. J. Nurs. Stud. 2021, 123, 104043. [Google Scholar] [CrossRef]
- Nayeri, N.D.; Esmaeili, M.; Farsi, Z.; Chenari, H.A. Taking care experiences of improved comatose patients with traumatic brain injury and their families. J. Fam. Med. Prim. Care 2020, 9, 4815–4820. [Google Scholar] [CrossRef]
- Grayson, L.; Brady, M.C.; Togher, L.; Ali, M. The impact of cognitive-communication difficulties following traumatic brain injury on the family; a qualitative, focus group study. Brain Inj. 2021, 35, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Weitzig, K.; Mitchell, M. The needs of families of ICU trauma patients: An integrative review. Intensive Crit. Care Nurs. 2017, 41, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Engli, M.; Kirsivali-Farmer, K. Needs of family members of critically ill patients with and without acute brain injury. J. Neurosci. Nurs. 1993, 25, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Keenan, A.; Joseph, L. The needs of family members of severe traumatic brain injured patients during critical and acute care: A qualitative study. Can. J. Neurosci. Nurs. 2010, 32, 25–35. [Google Scholar] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; Mcinerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, S.R.; Evans, D.J.W.; Butler, A.R.; Schofield-Robinson, O.J.; Alderson, P. Hypothermia for traumatic brain injury. Cochrane Database Syst. Rev. 2018, 9, CD001048. [Google Scholar] [CrossRef] [PubMed]
- The Endnote Team. EndNote Version 9; Clarivate: Philadelphia, PA, USA, 2013. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Page, M.; McKenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C.; Shamseer, L.; Tetzlaff, J.; Akl, E.; Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. Available online: https://casp-uk.net/ (accessed on 22 February 2023).
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the conduct of narrative synthesis in systematic reviews. Prod. ESRC Methods Prog. 2006, 1, 92. [Google Scholar]
- Bond, A.E.; Draeger, C.R.; Mandleco, B.; Donnelly, M.; Bond, A.E. Needs of family members of patients with severe traumatic brain injury. Implications for evidence-based practice. Crit. Care Nurse 2003, 23, 63–72. [Google Scholar] [CrossRef]
- Kanmani, T.R.; Thimmappur, R.M.; Birudu, R.; Reddy, K.; Raj, P. Burden and psychological distress of intensive care unit caregivers of traumatic brain injury patients. Indian J. Crit. Care Med. 2019, 23, 220. [Google Scholar] [CrossRef]
- Lefebvre, H.; Pelchat, D.; Swaine, B.; Gelinas, I.; Levert, M.J. The experiences of individuals with a traumatic brain injury, families, physicians and health professionals regarding care provided throughout the continuum. Brain Inj. 2005, 19, 585–597. [Google Scholar] [CrossRef]
- Lefebvre, H.; Levert, M.J. Breaking the news of traumatic brain injury and incapacities. Brain Inj. 2006, 20, 711–718. [Google Scholar] [CrossRef]
- Piyakong, D. Challenges faced by Thai families when a loved one has a traumatic brain injury. Arch. Psychiatr. Nurs. 2014, 28, 220–221. [Google Scholar] [CrossRef] [PubMed]
- Kean, S. The experience of ambiguous loss in families of brain injured ICU patients. Nurs. Crit. Care 2010, 15, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Quinn, T.; Moskowitz, J.; Khan, M.W.; Shutter, L.; Goldberg, R.; Col, N.; Mazor, K.M.; Muehlschlegel, S. What families need and physicians deliver: Contrasting communication preferences between surrogate decision-makers and physicians during outcome prognostication in critically ill TBI patients. Neurocrit. Care 2017, 27, 154–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, K.; Quinn, T.; Mazor, K.M.; Muehlschlegel, S. Prognostic uncertainty in critically ill patients with traumatic brain injury: A multicenter qualitative study. Neurocrit. Care 2021, 35, 311–321. [Google Scholar] [CrossRef]
- Vanderbyl, B.L.; Gélinas, C. Family perspectives of traumatically brain-injured patient pain behaviors in the intensive care unit. Pain Manag. Nurs. 2017, 18, 202–213.29. [Google Scholar] [CrossRef]
- Verhaeghe, S.; Defloor, T.; Grypdonck, M. Stress and coping among families of patients with traumatic brain injury: A review of the literature. J. Clin. Nurs. 2005, 14, 1004–1012. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.; Chari, A.; Ganau, M.; Uff, C. Defining New Research Questions and Protocols in the Field of Traumatic Brain Injury through Public Engagement: Preliminary Results and Review of the Literature. Emerg. Med. Int. 2019, 2019, 9101235. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Title and abstract | Population:
|
|
| Full-text | Concept
|
|
| Citation Details | Country | Study Design/Method | Participant Details | Population | Concept | Context |
|---|---|---|---|---|---|---|
| [10] Keenan and Joseph (2010) | Canada | Qualitative semi-structured interviews/Interviews | Mother—9 Father—3 Wife—5 Sister—4 Girlfriend—3 Brother—1 | Twenty-five family members of 15 patients were admitted to the ICU with severe TBI. | Family member’s experience | Timepoint 1—within four days of ICU discharge. Timepoint 2—at discharge from an acute hospital. (Data taken only from time point 1) |
| [20] Bond et al. (2003) | USA | Exploratory qualitative descriptive design/Longitudinal qualitative interview | Mothers—2 Daughter—1 Father—1 Grandmother—1 Sister—1 Uncle—1 | Aged above 18, severe TBI (GCS score < 8) in ICU | Needs of patients’ families | ICU for at least 24 h |
| [21] Kanmani et al. (2019) | India | Descriptive research design/Interviews to administer the quantitative questionnaire | Spouse—9 Daughter/son—17 Parents—24 Secondary relatives—6 Siblings—4 | no age, primary caregivers providing care to a relative with TBI in ICU for more than one week (mild, moderate, and severe) | caregiver distress and burden | ICU for four days |
| [22] Lefebvre et al. (2005) | Canada | Qualitative retrospective study—secondary analysis/Qualitative Interviews | 8 TBI patients & Family members (not specified), physicians, and health professionals | Family members of a patient with TBI—75% severe, 25% moderate | Experiences of individuals who sustained TBI, their families, and the physicians & professionals | Critical care onwards |
| [23] Lefebvre & Levert (2006) | Canada | Qualitative retrospective/Qualitative interviews | 8 TBI patients & Family members (not specified), physicians, and health professionals | Family members of a patient with TBI—75% severe, 25% moderate | Experiences of individuals who sustained TBI, their families, and the physicians & professionals | Retrospective recall from experiences in ICU |
| [24] Piyakong (2014) | Thailand | Exploratory qualitative descriptive design/Qualitative interview | Wives—4 Mothers—2 Fathers—2 Niece—1 | Family members of TBI patients; neurological critical care setting (ICU) | Exploring challenges and approaches for resolving challenges | ICU |
| [25] Kean (2010) | Scotland | Constructivist grounded theory/Qualitative interviews | Partner/spouse—1 Mother—3 Father—3 Sister—5 Brother—3 | Family members of patients with TBI, ICU | Families experience ambiguous loss | ICU |
| [26] Quinn et al. (2017) | USA | Qualitative retrospective interviews/Qualitative interviews | Surrogates—16, relationship to TBI patient not stated | Aged 18 or over, primary decision maker for critically ill TBI patient within the last two years (extrapolating that critically ill in level 1 center = severe TBI) | Communication preferences | Level 1 trauma center (neuroICU) |
| [27] Jones et al. (2021) | USA | Secondary analysis of semi-structured interviews/Qualitative interviews | Surrogates—16, relationship to TBI patient not stated | Aged 18 or over, primary decision maker for critically ill TBI patient within the last two years (extrapolating that critically ill in level 1 center = severe TBI) | Communication of uncertainty | Level 1 trauma center (neuroICU) |
| Citation Details | Aim of Study | Method of Analysis | Themes | Outcome Measure (Description/Validated) | Findings |
|---|---|---|---|---|---|
| [10] Keenan and Joseph (2010) | To identify the needs of individual family members of a relative who sustained a severe TBI and to determine if these needs changed over time. | Thematic analysis | (1) Getting the news (2) Uncertainty (3) Making sense of the news (4) Moving on | n/a | Getting the news—vivid memories and intense emotional reactions. Uncertainty—the uncertainty of survival, uncertainty in waiting, and uncertainty of prognosis “he was so critical, like it was hour by hour... that was the hardest... the waiting and the unknown”. Making sense of the news—seeking information from the clinical team and “intense need to know”. Moving on—the shift of focus of how to manage life outside the longer term. The needs of the family—Involvement in Care; Looking for progress; managing life; Holding on to hope; Information, Responding to the family’s needs—Professional support; Community support. |
| [20] Bond et al. (2003) | To explore the needs of patients’ families through individual interviews during the course of the patient’s stay in the ICU | Content analysis | (1) Need to know (2) Need for consistent information (3) Need for involvement in care (4) Need to make sense of the experience | n/a | (1) Families expressing the need for direct contact with the medical team, desire to know the truth, “Please give me some reality” (2) “Unable to know what is real and what is an opinion”. Receiving conflicting information from different physicians (3) Frustration with being left out of patient care—wish to be trusted with care tasks, feeling of being useless in patient care. (4) Wanting more detail about why things are carried out. Frightening experience that leads to relying on faith. |
| [21] Kanmani et al. (2019) | To assess the family burden and psychological distress among TBI caregivers at the emergency ICU | Descriptive statistics & independent burden t-test | n/a | Family burden and depression, anxiety, and stress scale (DAS-21). | The severity of TBI injury was associated with caregiver burden. The severity of TBI was likely to increase the burden on caregivers at ICU. Family burden score—44.7% moderate burden, 55.3% severe burden Statistically significant higher scores are reported in caregivers’ depression, anxiety, and stress levels from severe TBI in comparison to mild/moderate injuries. |
| [22] Lefebvre et al. (2005) | To investigate the experiences of individuals who had sustained a TBI, their families, the physicians, and health professionals involved from the beginning of acute care to their reintegration into daily life. | Content analysis | (1) Unclear communication (2) Feelings of uncertainty (3) Desiring transparency of information (4) Feelings of insignificance in patient care. | Internal validity | Families feel that the information being given to them by professionals regarding prognosis is inadequate, lending to significant uncertainty. They appear to also need support in that uncertainty. Families want to contribute to the care of the individual and feel a responsibility to let the clinical team know ‘who they are’ before the TBI. They experience feeling brushed aside and a lack of recognition for their role in patient care. |
| [23] Lefebvre & Levert (2006) | To investigate the experiences of individuals who had sustained a TBI, their families, the physicians, and health professionals involved in critical care episodes and subsequent rehabilitation. | Content analysis | (1) Shock (2) Lack of information (3) Uncertainty | Internal validity | There is a dividing line between before and after the TBI. There is a lack of information given to families, which restricts their ability to absorb what has happened. This contributes to the difficulty they face. Families sense the uncertainty from health professionals, and this vagueness contributes to their adjustment process from before to after. |
| [24] Piyakong (2014) | To explore challenges and approaches for resolving challenges that Thai family members face when engaging with their loved one with severe traumatic brain injury in the critical care setting | Content analysis | (1) Facing the uncertainty of a loved one’s illness (2) Dealing with personal suffering (3) Changing everyday life patterns. | n/a | Thai family members face the health challenges of uncertainty when a loved one suffers unconsciousness from TBI. Their approaches to managing challenges include the use of familiar resources to connect with the loved one and improve consciousness. |
| [25] Kean (2010) | To explore the families’ experiences with critical illness in the ICU and nurses’ perceptions of families | Ground theory—Constant comparative method | (1) Family experiences—Clinical uncertainty; functional uncertainty (2) Children—Adult’s power of controlling information; children’s agency; fishing for information | n/a | Core experiences—(1) clinical and functional uncertainty—(2) ambiguous loss (physically present, psychologically absent) embedded in (1). (3) Mapping the future; the impact of ambiguous loss on everyday family life embedded in (2) |
| [26] Quinn et al. (2017) | To explore key communication preferences and practices by stakeholders (surrogates and physicians) for the outcome prognostication during goals of care discussions for ciTBI | Thematic analysis | (1) Uncertainty and frustration regarding decision making (2) Seeking honest communication to inform decisions (3) Inconsistency of support in decision making (4) Lack of recognition of distress. | n/a | A majority of surrogate decision-makers felt unprepared in the decision-making process and struggled for many months afterward. Providing numeric prognostic estimates was helpful in this decision-making process. Families felt a sense of hope was important but needed the facts from physicians and not false hope. Emotion distress was caused by inconsistency in communication between physicians and the clinical team. |
| [26] Jones et al. (2021) | To identify strategies used by physicians specifically to communicate uncertainty as well as surrogates’ perceptions of this communication and of uncertainty. | Secondary Analysis using thematic analysis | (1) Ambiguity in goals of care (2) Prognostic uncertainty impacting decision making (3) Worry about making the ‘wrong decision.’ | n/a | Practical decision-making is impacted by feelings of prognostic uncertainty. Too much ambiguity lends to a need for certainty, while too little ambiguity leaves families uncertain about whether hope should be ‘taken away’. Positive communication experiences are described as having questions answered, feeling included, and simple language is used. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayes, K.; Harding, S.; Buckley, K.; Blackwood, B.; Latour, J.M. Exploring the Experiences of Family Members When a Patient Is Admitted to the ICU with a Severe Traumatic Brain Injury: A Scoping Review. J. Clin. Med. 2023, 12, 4197. https://doi.org/10.3390/jcm12134197
Hayes K, Harding S, Buckley K, Blackwood B, Latour JM. Exploring the Experiences of Family Members When a Patient Is Admitted to the ICU with a Severe Traumatic Brain Injury: A Scoping Review. Journal of Clinical Medicine. 2023; 12(13):4197. https://doi.org/10.3390/jcm12134197
Chicago/Turabian StyleHayes, Kati, Sam Harding, Kirsten Buckley, Bronagh Blackwood, and Jos M. Latour. 2023. "Exploring the Experiences of Family Members When a Patient Is Admitted to the ICU with a Severe Traumatic Brain Injury: A Scoping Review" Journal of Clinical Medicine 12, no. 13: 4197. https://doi.org/10.3390/jcm12134197