
Effects of Non-Invasive Neuromodulation of the Vagus Nerve for Management of Tinnitus: A Systematic Review with Meta-Analysis
 , , , and
, , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. PICO Principle
2.3. Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Level of Evidence
2.6. Data Synthesis and Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Outcomes and Follow-Ups
3.4. Interventions/Control Groups
3.5. Methodological Quality and Risk of Bias
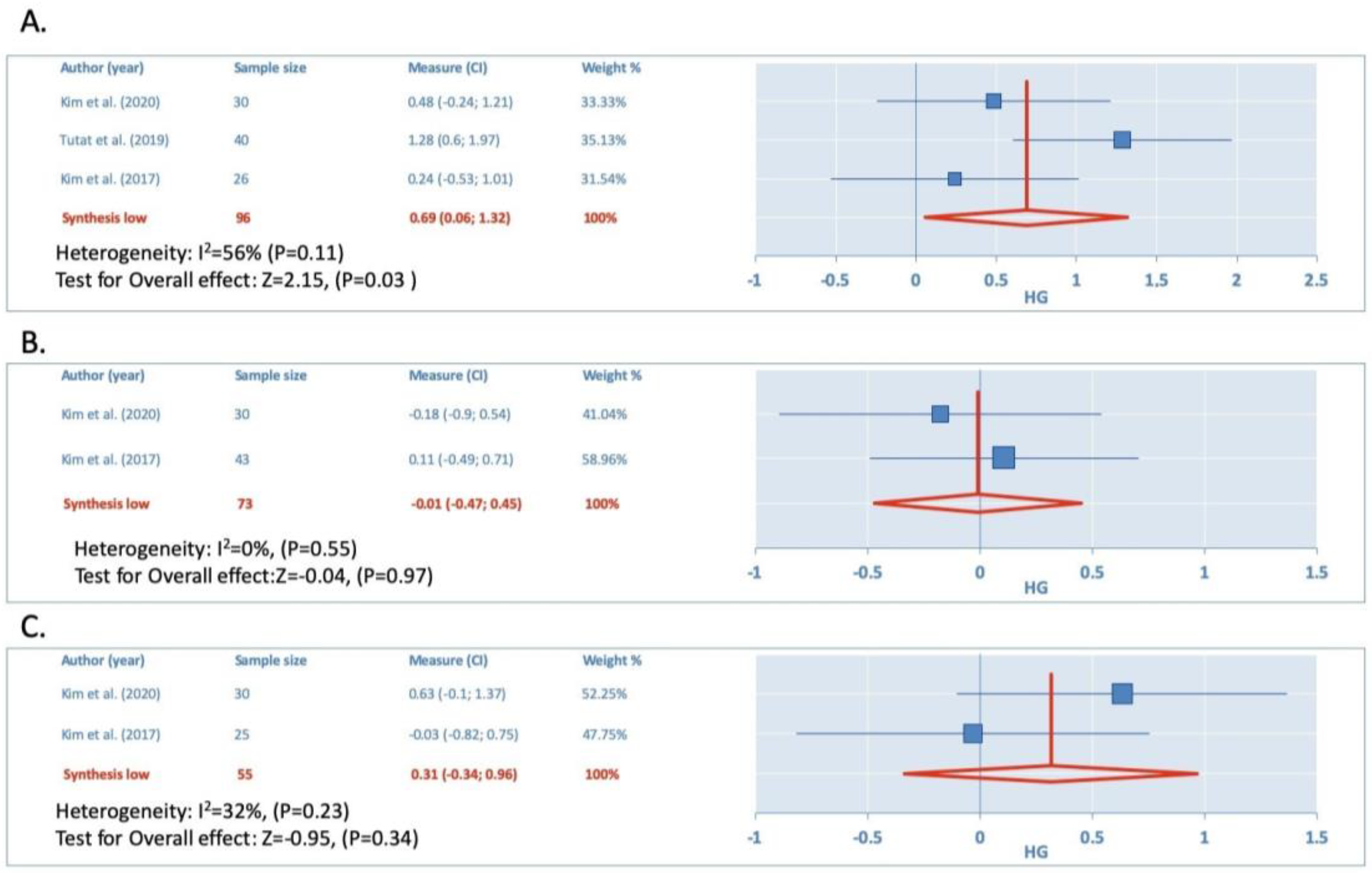
3.6. Unilateral Auricular Stimulation vs. Control
3.7. Unilateral Auricular Stimulation vs. Bilateral Stimulation
3.8. TENS vs. Control
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, T.-T.; Wang, Z.-J.; Yang, S.-B.; Zhu, J.-H.; Zhang, S.-Z.; Cai, S.-J.; Ma, W.-H.; Zhang, D.-Q.; Mei, Z.-G. Transcutaneous electrical stimulation at auricular acupoints innervated by auricular branch of vagus nerve pairing tone for tinnitus: Study protocol for a randomized controlled clinical trial. Trials 2015, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Amiri, S.; Behnezhad, S.; Azad, E. Migraine headache and depression in adults: A systematic Review and Meta-analysis. Neuropsychiatrie 2019, 33, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Yap, J.Y.Y.; Keatch, C.; Lambert, E.; Woods, W.; Stoddart, P.R.; Kameneva, T. Critical Review of Transcutaneous Vagus Nerve Stimulation: Challenges for Translation to Clinical Practice. Front. Neurosci. 2020, 14, 284. [Google Scholar] [CrossRef]
- Badran, B.W.; Dowdle, L.T.; Mithoefer, O.J.; LaBate, N.T.; Coatsworth, J.; Brown, J.C.; DeVries, W.H.; Austelle, C.W.; McTeague, L.M.; George, M.S. Neurophysiologic effects of transcutaneous auricular vagus nerve stimulation (taVNS) via electrical stimulation of the tragus: A concurrent taVNS/fMRI study and review. Brain Stimul. 2018, 11, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Benemei, S.; Labastida-Ramírez, A.; Abramova, E.; Brunelli, N.; Caronna, E.; Diana, P.; Gapeshin, R.; Hofacker, M.D.; Maestrini, I.; Pías, E.M.; et al. Persistent post-traumatic headache: A migrainous loop or not? The preclinical evidence. J. Headache Pain 2020, 21, 90. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.S.; Kim, S.J.; Chang, D.S.; Lee, H.Y.; Suk, W.C. Characteristics of Stimulus Intensity in Transcutaneous Vagus Nerve Stimulation for Chronic Tinnitus. J. Int. Adv. Otol. 2018, 14, 267–272. [Google Scholar] [CrossRef]
- Kaniusas, E.; Kampusch, S.; Tittgemeyer, M.; Panetsos, F.; Gines, R.F.; Papa, M.; Kiss, A.; Podesser, B.; Cassara, A.M.; Tanghe, E.; et al. Current Directions in the Auricular Vagus Nerve Stimulation I–A Physiological Perspective. Front. Neurosci. 2019, 13, 1–23. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, J.; Li, H.; Yan, Z.; Liu, X.; Cao, J.; Park, J.; Wilson, G.; Liu, B.; Kong, J. Transcutaneous auricular vagus nerve stimulation at 1 Hz modulates locus coeruleus activity and resting state functional connectivity in patients with migraine: An fMRI study. NeuroImage Clin. 2019, 24, 101971. [Google Scholar] [CrossRef]
- Richards. 乳鼠心肌提取 HHS Public Access. Physiol. Behav. 2018, 176, 139–148. [Google Scholar]
- Sclocco, R.; Garcia, R.G.; Kettner, N.W.; Isenburg, K.; Fisher, H.P.; Hubbard, C.S.; Ay, I.; Polimeni, J.R.; Goldstein, J.; Makris, N.; et al. The influence of respiration on brainstem and cardiovagal response to auricular vagus nerve stimulation: A multimodal ultrahigh-field (7T) fMRI study. Brain Stimul. 2019, 12, 911–921. [Google Scholar] [CrossRef]
- Kim, H.-J.; Lee, H.-J.; An, S.-Y.; Sim, S.; Park, B.; Kim, S.W.; Lee, J.S.; Hong, S.K.; Choi, H.G. Analysis of the Prevalence and Associated Risk Factors of Tinnitus in Adults. PLoS ONE 2015, 10, e0127578. [Google Scholar] [CrossRef]
- Rhee, J.; Lee, D.; Suh, M.-W.; Lee, J.H.; Hong, Y.-C.; Oh, S.H.; Park, M.K. Prevalence, associated factors, and comorbidities of tinnitus in adolescents. PLoS ONE 2020, 15, e0236723. [Google Scholar] [CrossRef] [PubMed]
- McCormack, A.; Edmondson-Jones, M.; Somerset, S.; Hall, D. A systematic review of the reporting of tinnitus prevalence and severity. Hear. Res. 2016, 337, 70–79. [Google Scholar] [CrossRef]
- Jarach, C.M.; Lugo, A.; Scala, M.; Brandt, P.A.V.D.; Cederroth, C.R.; Odone, A.; Garavello, W.; Schlee, W.; Langguth, B.; Gallus, S. Global Prevalence and Incidence of Tinnitus: A Systematic Review and Meta-analysis. JAMA Neurol. 2022, 79, 888–900. [Google Scholar] [CrossRef]
- Bhatt, J.M.; Bhattacharyya, N.; Lin, H.W. Relationships between tinnitus and the prevalence of anxiety and depression. Laryngoscope 2017, 127, 466–469. [Google Scholar] [CrossRef]
- Lehtimäki, J.; Hyvärinen, P.; Ylikoski, M.; Bergholm, M.; Mäkelä, J.P.; Aarnisalo, A.; Pirvola, U.; Mäkitie, A.; Ylikoski, J. Transcutaneous vagus nerve stimulation in tinnitus: A pilot study. Acta Oto-Laryngologica 2013, 133, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Stegeman, I.; Velde, H.M.; Robe, P.A.J.T.; Stokroos, R.J.; Smit, A.L. Tinnitus treatment by vagus nerve stimulation: A systematic review. PLoS ONE 2021, 16, e0247221. [Google Scholar] [CrossRef] [PubMed]
- Morrison, R.A.; Abe, S.T.; Danaphongse, T.; Ezhil, V.; Somaney, A.; Adcock, K.S.; Rennaker, R.L.; Kilgard, M.P.; Hays, S.A. Common Cholinergic, Noradrenergic, and Serotonergic Drugs Do Not Block VNS-Mediated Plasticity. Front. Neurosci. 2022, 16, 849291. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Oxman, A.D.; Brozek, J.; Glasziou, P.; Bossuyt, P.; Chang, S.; Muti, P.; Jaeschke, R.; Guyatt, G.H. GRADE: Assessing the quality of evidence for diagnostic recommendations. BMJ Evidence-Based Med. 2008, 13, 162–163. [Google Scholar] [CrossRef]
- Deeks, J.J. Chapter 9: Analyzing data and undertaking metanalyses. In Cochrane Handbook for Systematic Reviews of Interventions, version 520 (updated June 2017); Higgins, J.P.T., Churchill, R., Chandler, J., Cumpston, M.S., Eds.; Cochrane: Singapore, 2017; Available online: www.training.cochrane.org/handbook (accessed on 15 October 2022).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Ades, A.E.; Lu, G.; Higgins, J.P.T. The Interpretation of Random-Effects Meta-Analysis in Decision Models. Med. Decis. Mak. 2005, 25, 646–654. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, C.; D’arcy, S.; Pearlmutter, B.A.; Crispino, G.; Lalor, E.C.; Conlon, B.J. An Investigation of Feasibility and Safety of Bi-Modal Stimulation for the Treatment of Tinnitus: An Open-Label Pilot Study. Neuromodulation 2016, 19, 832–837. [Google Scholar] [CrossRef]
- Tutar, B.; Atar, S.; Berkiten, G.; Üstün, O.; Kumral, T.L.; Uyar, Y. The effect of transcutaneous electrical nerve stimulation (TENS) on chronic subjective tinnitus. Am. J. Otolaryngol. 2019, 41, 102326. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Moon, Y.K.; Kim, M.H.; Nam, H.J. Comparing the effects of manual acupuncture, electroacupuncture, and transcutaneous electrical nerve stimulation on chronic tinnitus: A randomized controlled trial. Integr. Med. Res. 2020, 9, 100409. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Kim, K.; Nam, H.J. A comparative study on the effects of systemic manual acupuncture, periauricular electroacupuncture, and digital electroacupuncture to treat tinnitus: A randomized, paralleled, open-labeled exploratory trial. BMC Complement. Altern. Med. 2017, 17, 1–7. [Google Scholar] [CrossRef]
- Yakunina, N.; Kim, S.S.; Nam, E.-C. BOLD fMRI effects of transcutaneous vagus nerve stimulation in patients with chronic tinnitus. PLoS ONE 2018, 13, e0207281. [Google Scholar] [CrossRef]
- Hyvärinen, P.; Yrttiaho, S.; Lehtimäki, J.; Ilmoniemi, R.; Mäkitie, A.; Ylikoski, J.; Mäkelä, J.P.; Aarnisalo, A.A. Transcutaneous Vagus Nerve Stimulation Modulates Tinnitus-Related Beta- and Gamma-Band Activity. Ear Hear. 2015, 36, e76–e85. [Google Scholar] [CrossRef]
- Ylikoski, J.; Markkanen, M.; Pirvola, U.; Lehtimäki, J.A.; Ylikoski, M.; Jing, Z.; Sinkkonen, S.T.; Mäkitie, A. Stress and Tinnitus; Transcutaneous Auricular Vagal Nerve Stimulation Attenuates Tinnitus-Triggered Stress Reaction. Front. Psychol. 2020, 11, 570196. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Mu, K.; Liu, A.; Zhou, L.; Gao, Y.; Shenoy, I.T.; Mei, Z.; Chen, Q. Transauricular vagus nerve stimulation at auricular acupoints Kindey (CO10), Yidan (CO11), Liver (CO12) and Shenmen (TF4) can induce auditory and limbic cortices activation measured by fMRI. Hear. Res. 2018, 359, 1–12. [Google Scholar] [CrossRef]
- Peter, N.; Kleinjung, T. Neuromodulation for tinnitus treatment: An overview of invasive and non-invasive techniques. J. Zhejiang Univ. Sci. B 2018, 20, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.; Boddington, L.; Steffan, P.J.; McCormick, D. Vagus nerve stimulation induces widespread cortical and behavioral activation. Curr. Biol. 2021, 31, 2088–2098.e3. [Google Scholar] [CrossRef] [PubMed]
- Souza, R.R.; Robertson, N.M.; McIntyre, C.K.; Rennaker, R.L.; Hays, S.A.; Kilgard, M.P. Vagus nerve stimulation enhances fear extinction as an inverted-U function of stimulation intensity. Exp. Neurol. 2021, 341, 113718. [Google Scholar] [CrossRef]
- Sivaji, V.; Grasse, D.W.; Hays, S.A.; Bucksot, J.E.; Saini, R.; Kilgard, M.P.; Rennaker, R.L. ReStore: A wireless peripheral nerve stimulation system. J. Neurosci. Methods 2019, 320, 26–36. [Google Scholar] [CrossRef]
- Ganzer, P.D.; Darrow, M.J.; Meyers, E.C.; Solorzano, B.R.; Ruiz, A.D.; Robertson, N.M.; Adcock, K.S.; James, J.T.; Jeong, H.S.; Becker, A.M.; et al. Closed-loop neuromodulation restores network connectivity and motor control after spinal cord injury. Elife 2018, 7, e32058. [Google Scholar] [CrossRef]
- Kilgard, M.P.; Rennaker, R.L.; Alexander, J.; Dawson, J. Vagus nerve stimulation paired with tactile training improved sensory function in a chronic stroke patient. Neurorehabilitation 2018, 42, 159–165. [Google Scholar] [CrossRef]
- Tyler, R.; Cacace, A.; Stocking, C.; Tarver, B.; Engineer, N.; Martin, J.; Deshpande, A.; Stecker, N.; Pereira, M.; Kilgard, M.; et al. Vagus Nerve Stimulation Paired with Tones for the Treatment of Tinnitus: A Prospective Randomized Double-blind Controlled Pilot Study in Humans. Sci. Rep. 2017, 7, 11960. [Google Scholar] [CrossRef]
- Stander, J.; Grimmer, K.; Brink, Y. Time as a barrier to evidence uptake—A qualitative exploration of the concept of time for clinical practice guideline uptake by physiotherapists. J. Eval. Clin. Pract. 2020, 27, 280–290. [Google Scholar] [CrossRef]
- Lehane, E.; Agreli, H.; Connor, S.O.; Hegarty, J.; Warren, P.L.; Bennett, D.; Blake, C.; Burke, F.; Corrigan, M.; Drennan, J.; et al. Building capacity: Getting evidence-based practice into healthcare professional curricula. BMJ Evidence-Based Med. 2021, 26, 246. [Google Scholar] [CrossRef]
- Worum, H.; Lillekroken, D.; Roaldsen, K.S.; Ahlsen, B.; Bergland, A. Physiotherapists’ perceptions of challenges facing evidence-based practice and the importance of environmental empowerment in fall prevention in the municipality-a qualitative study. BMC Geriatr. 2020, 20, 432. [Google Scholar] [CrossRef]
- Huang, K.; Liang, S.; Chen, L.; Grellet, A. Acupuncture for tinnitus: A systematic review and meta-analysis of randomized controlled trials. Acupunct. Med. 2021, 39, 264–271. [Google Scholar] [CrossRef]
- Zeng, F.-G.; Richardson, M.; Tran, P.; Lin, H.; Djalilian, H. Tinnitus Treatment Using Noninvasive and Minimally Invasive Electric Stimulation: Experimental Design and Feasibility. Trends Hear. 2019, 23, 2331216518821449. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Design) | Number of Participants & Male/Female | Age (Years) | Duration Tinnitus | Intervention Duration (Sessions/Weeks) Area of Treatment | Comparison and Outcome Measure | Between−Groups Differences (95% CI) [hg] |
|---|---|---|---|---|---|---|
| Kim et al., 2020 [30] (RCT) | G1; at-VNS; 15. G2; MA; 15 G3; 15 13/2 12/3 8/7 | 47.3 ± 9.5 48.6 ± 7.8 46.2 ± 11.0 | 98.1 ± 97.7 months 105.1 ± 142.0 months 107.8 ± 115.9 months | G1; 15; 30-Hz G2; MA G3; 30/90 Hz with a 3-second interval) 20 min for 10 sessions Inner tragus, cymba conchae | THI, VAS loudness, and VAS annoyance PTA, and speech discrimintion test G1 vs. G2 vs. G3 | THI Post−treatment (−0.16, 1.3) [0.57] Short term (−0.25, 1.2) [0.48] VAS Loudness Post−treatment (−032, 1.13) [0.41] Short term (−0.53, 0.9) [0.18] VAS Uncomfortable Post−treatment (−0.45, 0.59) [0.07] Short term (−0.36, 0.68) [0.16] |
| Tutar et al., 2019 [29] (RCT) | G1; TENS (unilateral tinnitus); 20 G2; TENS (bilateral tinnitus); 20 G3; Control; 20 NR NR NR | 41.17 ± 10.75 | 31 ± 49 months [range: 3–198 months] | G1 and G2; 1–200 Hz, 10–30 mA, 1000 msec 10 sessions in 1 month for 30 min (maximum of 4 days between each session) Inner tragus, cymba conchae | THI DASS (pure tone audiometry, tympanometry, speech discrimination score G1 vs. G2 vs. G3 | THI Post−treatment (0.11, 1.4) [0.76] |
| Yakunina et al., 2018 [32] (CT) | G1; at-VNS with Tinnitus subjects; 36 G2; at-VNS with Normal subjects.; 37 27/9 18/19 | 51.0 ± 11.9 30.9 ± 8.2 | 63.2 ± 59.5 (3–134) months | G1 & G2; 500 μs, 25 Hz, 0.1 mA Unique session of MRI scan, total of six 5 min fMRI runs Inner tragus, cymba conchae | Hearing and tinnitus assessment MRI | NR |
| Kim et al., 2017 [31] (RCT) | G1; at-VNS (auricular region); 14. G2; MA; 13 G3; at-VNS (distal region), 15 12/2 6/6 10/3 | 54.6 ± 14.3 49.3 ± 15.6 53.9 ± 13.2 | 9.55 ± 11.55 years 7.1 ± 7.85 years 5.7 ± 6.4 years | G1 and G3; 4/100 Hz interval 3 s 20 min for 8 sessions 2 sessions/week Inner tragus, cymba conchae | THIS, VAS loudness, and VAS uncomfortable, PTA, and speech discrimintion test G1 vs. G2 vs. G3G1 vs. G2 Function (IKDC function subscale) G1 vs. G2 G1 vs. G2 | THI Post−treatment (−0.66, 0.85) [0.1] Short Term (−0.64, 0.87) [0.12] VAS Loudness Post−treatment (−0.81, 0.7) [−0.06] Short term (−0.69, 0.82) [0.06] VAS Uncomfortable Post−treatment (−0.88, 0.63) [0.25] Short term (−0.69, 0.82) [0.06] |
| Hamilton et al., 2016 [28] (CT) | G1; Bi-modal stimulation Tinnitus compliant; NR G2; Bi-modal stimulation Tinnitus non-compliant; NR 34 (63%) men | 47.5 ± 11 | >2 years/<2 years 36 (78%)/10 (22%) | G1; Auditory stimulus G2; Bi-modal stimulation. 20 Hz—20 kHz For 14 weeks every visit per 2 weeks, 7 sessions, 47 min each session Inner tragus, cymba conchae | THI, MML, TLM, and VAS loudness G1 vs. G2 | THI Post−treatment (−0.35, 0.93) [0.29] |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tinnitus | |||||||||||
| Kim et al., 2020 [30] | Y | Y | Y | N | N | N | N | Y | Y | Y | 6/10 |
| Tutar et al., 2019 [29] | Y | N | Y | N | N | Y | Y | N | Y | Y | 6/10 |
| Kim et al., 2017 [31] | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7/10 |
| Yakunina et al., 2018 [32] | N | N | N | N | N | N | N | N | Y | Y | 2/10 |
| Hamilton et al., 2016 [28] | N | N | N | N | N | N | N | N | Y | Y | 2/10 |
| Number of Studies | Risk of Bias | Inconsistency | Indirectness of Evidence | Imprecision | Publication Bias | Quality of Evidence | hg [95% CI] |
|---|---|---|---|---|---|---|---|
| Unilateral auricular stimulation vs. Control THI | |||||||
| Post-treatment group (n = 3) | Serious | High | Low/acceptable | No | Very serious | Very Low | 0.69 (0.06, 1.32) |
| Short-term subgroup (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.28 (−0.25, 0.81) |
| Unilateral auricular stimulation vs. Control Vas Loudness | |||||||
| Post-treatment group (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | −0.01 (−0.47, 0.45) |
| Short-term subgroup (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | −0.02 (−0.48, 0.44) |
| Unilateral auricular stimulation vs. Control Vas Uncomfortable | |||||||
| Post-treatment group (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.31 (−0.34, 0.96) |
| Short-term subgroup (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.31 (−0.16, 0.77) |
| Unilateral Stimulations vs. Bilateral THI | |||||||
| Post-treatment group (n = 4) | Serious | High | Low/acceptable | No | Very serious | Very Low | 0.21 (−0.13, 0.55) |
| Short-term subgroup (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.3 (−0.22, 0.83) |
| Unilateral Stimulations vs. Bilateral Vas Loudness | |||||||
| Post-treatment group (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.19 (−0.34, 0.71) |
| Short-term subgroup (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.13 (−0.39, 0.65) |
| Unilateral Stimulations vs. Bilateral Vas Uncomfortable | |||||||
| Post-treatment group (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.15 (−0.38, 0.67) |
| Short-term subgroup (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.16 (−0.36, 0.67) |
| Tens vs. Placebo THI | |||||||
| Post-treatment group (n = 3) | Serious | Moderate | low/acceptable | No | Very serious | Very Low | 0.51 (0.1, 0.91) |
| Short-term subgroup (n = 2) | No | Low | low/acceptable | No | Very serious | Moderate | 0.3 (−0.23, 0.83) |
| Tens vs. Placebo Vas Loudness | |||||||
| Post-treatment group (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.19 (−0.34, 0.71) |
| Short-term subgroup (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.13 (−0.39, 0.65) |
| Tens vs. Placebo Vas Uncomfortable | |||||||
| Post-treatment group (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.07 (−0.45, 0−59) |
| Short-term subgroup (n = 2) | No | Low | Low/acceptable | No | Very serious | Moderate | 0.16 (−0.36, 0.68) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Hernando, D.; Fernández-de-las-Peñas, C.; Machado-Martín, A.; Angulo-Díaz-Parreño, S.; García-Esteo, F.J.; Mesa-Jiménez, J.A. Effects of Non-Invasive Neuromodulation of the Vagus Nerve for Management of Tinnitus: A Systematic Review with Meta-Analysis. J. Clin. Med. 2023, 12, 3673. https://doi.org/10.3390/jcm12113673
Fernández-Hernando D, Fernández-de-las-Peñas C, Machado-Martín A, Angulo-Díaz-Parreño S, García-Esteo FJ, Mesa-Jiménez JA. Effects of Non-Invasive Neuromodulation of the Vagus Nerve for Management of Tinnitus: A Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2023; 12(11):3673. https://doi.org/10.3390/jcm12113673
Chicago/Turabian StyleFernández-Hernando, David, Cesar Fernández-de-las-Peñas, Ana Machado-Martín, Santiago Angulo-Díaz-Parreño, Francisco J. García-Esteo, and Juan A. Mesa-Jiménez. 2023. "Effects of Non-Invasive Neuromodulation of the Vagus Nerve for Management of Tinnitus: A Systematic Review with Meta-Analysis" Journal of Clinical Medicine 12, no. 11: 3673. https://doi.org/10.3390/jcm12113673