
Comparative Analysis of Hematological and Immunological Parameters in Patients with Primary Sjögren’s Syndrome and Peripheral Neuropathy

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Groups
3.2. Comparative Analysis of the Laboratory Parameters
3.3. Investigation of PN and Other Extraglandular Manifestations
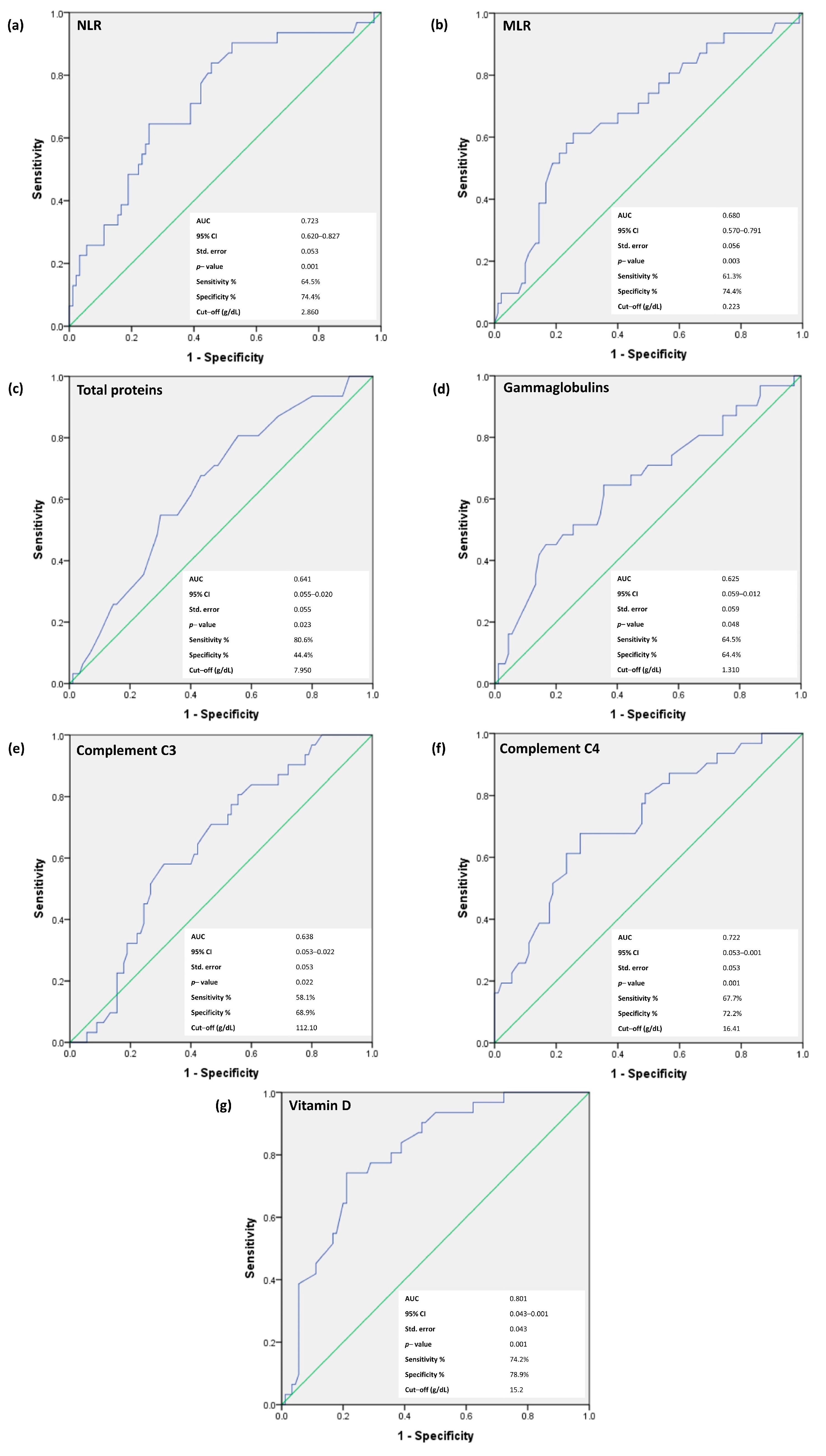
3.4. Receiver-Operating Characteristic (ROC) Curves for NLR, MLR, Total Proteins, Gammaglobulins, C3 and C4, and Vitamin D for the Prediction of Neurological Involvement in pSS Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, R.; Shahane, A. The epidemiology of Sjögren’s syndrome. Clin. Epidemiol. 2014, 6, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Fox, R.I. Sjögren’s syndrome. Lancet 2005, 366, 321–331. [Google Scholar] [CrossRef]
- Casian, M.; Jurcut, C.; Dima, A.; Mihai, A.; Stanciu, S.; Jurcut, R. Cardiovascular Disease in Primary Sjögren’s Syndrome: Raising Clinicians’ Awareness. Front. Immunol. 2022, 13, 865373. [Google Scholar] [CrossRef] [PubMed]
- Balaban, D.V.; Mihai, A.; Dima, A.; Popp, A.; Jinga, M.; Jurcut, C. Celiac disease and Sjögren’s syndrome: A case report and review of literature. World J. Clin. Cases 2020, 8, 4151–4161. [Google Scholar] [CrossRef] [PubMed]
- Carvajal Alegria, G.; Guellec, D.; Devauchelle-Pensec, V.; Saraux, A. Is there specific neurological disorders of primary Sjögren’s syndrome? Jt. Bone Spine 2015, 82, 86–89. [Google Scholar] [CrossRef]
- Baldini, C.; Pepe, P.; Quartuccio, L.; Priori, R.; Bartoloni, E.; Alunno, A.; Gattamelata, A.; Maset, M.; Modesti, M.; Tavoni, A.; et al. Primary Sjogren’s syndrome as a multi-organ disease: Impact of the serological profile on the clinical presentation of the disease in a large cohort of Italian patients. Rheumatology 2014, 53, 839–844. [Google Scholar] [CrossRef]
- Sène, D.; Jallouli, M.; Lefaucheur, J.P.; Saadoun, D.; Costedoat-Chalumeau, N.; Maisonobe, T.; Diemert, M.C.; Musset, L.; Haroche, J.; Piette, J.C.; et al. Peripheral neuropathies associated with primary Sjögren syndrome: Immunologic profiles of nonataxic sensory neuropathy and sensorimotor neuropathy. Medicine 2011, 90, 133–138. [Google Scholar] [CrossRef]
- Carvajal Alegria, G.; Guellec, D.; Mariette, X.; Gottenberg, J.E.; Dernis, E.; Dubost, J.J.; Trouvin, A.P.; Hachulla, E.; Larroche, C.; Le Guern, V.; et al. Epidemiology of neurological manifestations in Sjögren’s syndrome: Data from the French ASSESS Cohort. RMD Open 2016, 2, e000179. [Google Scholar] [CrossRef]
- Birnbaum, J. Peripheral nervous system manifestations of Sjögren syndrome: Clinical patterns, diagnostic paradigms, etiopathogenesis, and therapeutic strategies. Neurologist 2010, 16, 287–297. [Google Scholar] [CrossRef]
- Font, J.; Ramos-Casals, M.; de la Red, G.; Pou, A.; Casanova, A.; García-Carrasco, M.; Cervera, R.; Molina, J.A.; Valls, J.; Bové, A.; et al. Pure sensory neuropathy in primary Sjögren’s syndrome. Longterm prospective followup and review of the literature. J. Rheumatol. 2003, 30, 1552–1557. [Google Scholar]
- Pavlakis, P.P.; Alexopoulos, H.; Kosmidis, M.L.; Mamali, I.; Moutsopoulos, H.M.; Tzioufas, A.G.; Dalakas, M.C. Peripheral neuropathies in Sjögren’s syndrome: A critical update on clinical features and pathogenetic mechanisms. J. Autoimmun. 2012, 39, 27–33. [Google Scholar] [CrossRef]
- Lauria, G.; Hsieh, S.T.; Johansson, O.; Kennedy, W.R.; Leger, J.M.; Mellgren, S.I.; Nolano, M.; Merkies, I.S.; Polydefkis, M.; Smith, A.G.; et al. European Federation of Neurological Societies/Peripheral Nerve Society Guideline on the use of skin biopsy in the diagnosis of small fiber neuropathy. Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society. Eur. J. Neurol. 2010, 17, 903-e49. [Google Scholar] [CrossRef]
- Skopouli, F.N.; Dafni, U.; Ioannidis, J.P.; Moutsopoulos, H.M. Clinical evolution, and morbidity and mortality of primary Sjögren’s syndrome. Semin. Arthritis Rheum. 2000, 29, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Fargetti, S.; Ugolini-Lopes, M.R.; Pasoto, S.G.; Seguro, L.P.C.; Shinjo, S.K.; Bonfa, E.; Borba, E.F. Short- and Long-Term Outcome of Systemic Lupus Erythematosus Peripheral Neuropathy: Bimodal Pattern of Onset and Treatment Response. Am. J. Clin. Oncol. 2021, 27, S212–S216. [Google Scholar] [CrossRef] [PubMed]
- Rivière, E.; Cohen Aubart, F.; Maisonobe, T.; Maurier, F.; Richez, C.; Gombert, B.; Gousseff, M.; Adoue, D.; Mathian, A.; Hié, M.; et al. Clinicopathological features of multiple mononeuropathy associated with systemic lupus erythematosus: A multicenter study. J. Neurol. 2017, 264, 1218–1226. [Google Scholar] [CrossRef] [PubMed]
- Fresneda Alarcon, M.; McLaren, Z.; Wright, H.L. Neutrophils in the Pathogenesis of Rheumatoid Arthritis and Systemic Lupus Erythematosus: Same Foe Different M.O. Front. Immunol. 2021, 12, 649693. [Google Scholar] [CrossRef] [PubMed]
- Soliman, W.M.; Sherif, N.M.; Ghanima, I.M.; El-Badawy, M.A. Neutrophil to lymphocyte and platelet to lymphocyte ratios in systemic lupus erythematosus: Relation with disease activity and lupus nephritis. Reumatol. Clin. 2020, 16, 255–261. [Google Scholar] [CrossRef]
- Tezcan, D.; Körez, M.K.; Gülcemal, S.; Hakbilen, S.; Akdağ, T.; Yılmaz, S. Evaluation of diagnostic performance of haematological parameters in Behçet’s disease. Int. J. Clin. Pr. 2021, 75, e14638. [Google Scholar] [CrossRef]
- Lian, L.; Xia, Y.Y.; Zhou, C.; Shen, X.M.; Li, X.L.; Han, S.G.; Zheng, Y.; Mao, Z.Q.; Gong, F.R.; Wu, M.Y.; et al. Application of platelet/lymphocyte and neutrophil/lymphocyte ratios in early diagnosis and prognostic prediction in patients with resectable gastric cancer. Cancer Biomark. 2015, 15, 899–907. [Google Scholar] [CrossRef]
- Sarejloo, S.; Khanzadeh, S.; Hosseini, S.; Gargari, M.K.; Lucke-Wold, B.; Mosalamiaghili, S.; Azami, P.; Oftadehbalani, S.; Sadeghvand, S. Role of the Neutrophil to Lymphocyte Ratio in Guillain Barré Syndrome: A Systematic Review and Meta-Analysis. Mediat. Inflamm. 2022, 2022, 3390831. [Google Scholar] [CrossRef]
- Xu, L.; Gao, T.X.; Chang, S.H.; Jiang, S.M.; Zhang, L.J.; Yang, L. Role of lymphocyte-related immune-inflammatory biomarkers in detecting early progression of Guillain-Barré syndrome. J. Clin. Neurosci. 2022, 105, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Zhang, Z.; Lin, F.; Ren, Y.; Liu, D.; Zhong, R.; Liang, Y. Comparisons of neutrophil-, monocyte-, eosinophil-, and basophil- lymphocyte ratios among various systemic autoimmune rheumatic diseases. Apmis 2017, 125, 863–871. [Google Scholar] [CrossRef] [PubMed]
- Cafaro, G.; Perricone, C.; Carubbi, F.; Baldini, C.; Quartuccio, L.; Priori, R.; Berardicurti, O.; Ferro, F.; Gandolfo, S.; Gattamelata, A.; et al. Peripheral Nervous System Involvement in Sjögren’s Syndrome: Analysis of a Cohort from the Italian Research Group on Sjögren’s Syndrome. Front. Immunol. 2021, 12, 615656. [Google Scholar] [CrossRef] [PubMed]
- Illescas-Montes, R.; Melguizo-Rodríguez, L.; Ruiz, C.; Costela-Ruiz, V.J. Vitamin D and autoimmune diseases. Life Sci. 2019, 233, 116744. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.; Zhang, J.; Li, Z.; Jin, L.; Zheng, Y.; Zhou, Z.; Zhen, S.; Lu, G. Increased C4 and decreased C3 levels are associated with a poor prognosis in patients with immunoglobulin A nephropathy: A retrospective study. BMC Nephrol. 2017, 18, 231. [Google Scholar] [CrossRef]
- Thurman, J.M.; Yapa, R. Complement Therapeutics in Autoimmune Disease. Front. Immunol. 2019, 10, 672. [Google Scholar] [CrossRef]
- Jordán-González, P.; Gago-Piñero, R.; Varela-Rosario, N.; Pérez-Ríos, N.; Vilá, L.M. Characterization of a subset of patients with primary Sjögren’s syndrome initially presenting with C3 or C4 hypocomplementemia. Eur. J. Rheumatol. 2020, 7, 112–117. [Google Scholar] [CrossRef]
- Cuadrado, M.J.; Calatayud, I.; Urquizu-Padilla, M.; Wijetilleka, S.; Kiani-Alikhan, S.; Karim, M.Y. Immunoglobulin abnormalities are frequent in patients with lupus nephritis. BMC Rheumatol. 2019, 3, 30. [Google Scholar] [CrossRef]
- Liang, M.; Liwen, Z.; Yun, Z.; Yanbo, D.; Jianping, C. Serum Levels of IL-33 and Correlation with IL-4, IL-17A, and Hypergammaglobulinemia in Patients with Autoimmune Hepatitis. Mediat. Inflamm. 2018, 2018, 7964654. [Google Scholar] [CrossRef]
- Dupuis, M.L.; Pagano, M.T.; Pierdominici, M.; Ortona, E. The role of vitamin D in autoimmune diseases: Could sex make the difference? Biol. Sex Differ. 2021, 12, 12. [Google Scholar] [CrossRef]
- Murdaca, G.; Tonacci, A.; Negrini, S.; Greco, M.; Borro, M.; Puppo, F.; Gangemi, S. Emerging role of vitamin D in autoimmune diseases: An update on evidence and therapeutic implications. Autoimmun. Rev. 2019, 18, 102350. [Google Scholar] [CrossRef] [PubMed]
- Agmon-Levin, N.; Kivity, S.; Tzioufas, A.G.; López Hoyos, M.; Rozman, B.; Efes, I.; Shapira, Y.; Shamis, A.; Amital, H.; Youinou, P.; et al. Low levels of vitamin-D are associated with neuropathy and lymphoma among patients with Sjögren’s syndrome. J. Autoimmun. 2012, 39, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Roffe-Vazquez, D.N.; Huerta-Delgado, A.S.; Castillo, E.C.; Villarreal-Calderón, J.R.; Gonzalez-Gil, A.M.; Enriquez, C.; Garcia-Rivas, G.; Elizondo-Montemayor, L. Correlation of Vitamin D with Inflammatory Cytokines, Atherosclerotic Parameters, and Lifestyle Factors in the Setting of Heart Failure: A 12-Month Follow-Up Study. Int. J. Mol. Sci. 2019, 20, 5811. [Google Scholar] [CrossRef] [PubMed]
- Mihai, A.; Caruntu, A.; Opris-Belinski, D.; Jurcut, C.; Dima, A.; Caruntu, C.; Ionescu, R. The Predictive Role of Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), Monocytes-to-Lymphocyte Ratio (MLR) and Gammaglobulins for the Development of Cutaneous Vasculitis Lesions in Primary Sjögren’s Syndrome. J. Clin. Med. 2022, 11, 5525. [Google Scholar] [CrossRef] [PubMed]
- Vitali, C.; Bombardieri, S.; Jonsson, R.; Moutsopoulos, H.M.; Alexander, E.L.; Carsons, S.E.; Daniels, T.E.; Fox, P.C.; Fox, R.I.; Kassan, S.S.; et al. Classification criteria for Sjögren’s syndrome: A revised version of the European criteria proposed by the American-European Consensus Group. Ann. Rheum. Dis. 2002, 61, 554–558. [Google Scholar] [CrossRef]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheum. 2017, 69, 35–45. [Google Scholar] [CrossRef]
- Sivadasan, A.; Muthusamy, K.; Patel, B.; Benjamin, R.N.; Prabhakar, A.T.; Mathew, V.; Aaron, S.; Alexander, M. Clinical Spectrum, Therapeutic Outcomes, and Prognostic Predictors in Sjogren’s Syndrome-associated Neuropathy. Ann. Indian Acad. Neurol. 2017, 20, 278–283. [Google Scholar] [CrossRef]
- Perzyńska-Mazan, J.; Maślińska, M.; Gasik, R. Neurophysiological Features of Peripheral Nervous System Involvement and Immunological Profile of Patients with Primary Sjögren Syndrome. J. Rheumatol. 2020, 47, 1661–1667. [Google Scholar] [CrossRef]
- Smith, E.M.; Beck, S.L.; Cohen, J. The total neuropathy score: A tool for measuring chemotherapy-induced peripheral neuropathy. Oncol. Nurs. Forum 2008, 35, 96–102. [Google Scholar] [CrossRef]
- Mallik, A.; Weir, A.I. Nerve conduction studies: Essentials and pitfalls in practice. J. Neurol. Neurosurg. Psychiatry 2005, 76 (Suppl. 2), ii23–ii31. [Google Scholar] [CrossRef]
- Casellini, C.M.; Parson, H.K.; Richardson, M.S.; Nevoret, M.L.; Vinik, A.I. Sudoscan, a noninvasive tool for detecting diabetic small fiber neuropathy and autonomic dysfunction. Diabetes Technol. Ther. 2013, 15, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Villon, C.; Orgeolet, L.; Roguedas, A.M.; Misery, L.; Gottenberg, J.E.; Cornec, D.; Jousse-Joulin, S.; Seror, R.; Berthelot, J.M.; Dieude, P.; et al. Epidemiology of cutaneous involvement in Sjögren syndrome: Data from three French pSS populations (TEARS, ASSESS, diapSS). Jt. Bone Spine 2021, 88, 105162. [Google Scholar] [CrossRef]
- Mekinian, A.; Ravaud, P.; Hatron, P.Y.; Larroche, C.; Leone, J.; Gombert, B.; Hamidou, M.; Cantagrel, A.; Marcelli, C.; Rist, S.; et al. Efficacy of rituximab in primary Sjogren’s syndrome with peripheral nervous system involvement: Results from the AIR registry. Ann. Rheum. Dis. 2012, 71, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Chae, C.S.; Park, G.Y.; Choi, Y.M.; Jung, S.; Kim, S.; Sohn, D.; Im, S. Rapid, Objective and Non-invasive Diagnosis of Sudomotor Dysfunction in Patients With Lower Extremity Dysesthesia: A Cross-Sectional Study. Ann. Rehabil. Med. 2017, 41, 1028–1038. [Google Scholar] [CrossRef]
- Fu, X.; Liu, H.; Huang, G.; Dai, S.S. The emerging role of neutrophils in autoimmune-associated disorders: Effector, predictor, and therapeutic targets. MedComm 2021, 2, 402–413. [Google Scholar] [CrossRef]
- Papayannopoulos, V. Neutrophil extracellular traps in immunity and disease. Nat. Rev. Immunol. 2018, 18, 134–147. [Google Scholar] [CrossRef]
- Luo, Y.; Xie, Y.; Zhang, W.; Lin, Q.; Tang, G.; Wu, S.; Huang, M.; Yin, B.; Huang, J.; Wei, W.; et al. Combination of lymphocyte number and function in evaluating host immunity. Aging 2019, 11, 12685–12707. [Google Scholar] [CrossRef]
- Sène, D.; Ismael, S.; Forien, M.; Charlotte, F.; Kaci, R.; Cacoub, P.; Diallo, A.; Dieudé, P.; Lioté, F. Ectopic Germinal Center-Like Structures in Minor Salivary Gland Biopsy Tissue Predict Lymphoma Occurrence in Patients with Primary Sjögren’s Syndrome. Arthritis Rheumatol. 2018, 70, 1481–1488. [Google Scholar] [CrossRef]
- Fasano, S.; Mauro, D.; Macaluso, F.; Xiao, F.; Zhao, Y.; Lu, L.; Guggino, G.; Ciccia, F. Pathogenesis of primary Sjögren’s syndrome beyond B lymphocytes. Clin. Exp. Rheumatol. 2020, 38 (Suppl. 126), 315–323. [Google Scholar]
- Wolf, A.A.; Yáñez, A.; Barman, P.K.; Goodridge, H.S. The Ontogeny of Monocyte Subsets. Front. Immunol. 2019, 10, 1642. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.T.; Gao, F.; Gu, K.; Chen, D.K. The Role of Monocytes and Macrophages in Autoimmune Diseases: A Comprehensive Review. Front. Immunol. 2019, 10, 1140. [Google Scholar] [CrossRef] [PubMed]
- Sequí-Sabater, J.M.; Beretta, L. Defining the Role of Monocytes in Sjögren’s Syndrome. Int. J. Mol. Sci. 2022, 23, 12765. [Google Scholar] [CrossRef] [PubMed]
- Ajami, B.; Bennett, J.L.; Krieger, C.; McNagny, K.M.; Rossi, F.M. Infiltrating monocytes trigger EAE progression, but do not contribute to the resident microglia pool. Nat. Neurosci. 2011, 14, 1142–1149. [Google Scholar] [CrossRef]
- Yıldız, F.; Gökmen, O. Haematologic indices and disease activity index in primary Sjogren’s syndrome. Int. J. Clin. Pr. 2021, 75, e13992. [Google Scholar] [CrossRef]
- Xu, T.; Weng, Z.; Pei, C.; Yu, S.; Chen, Y.; Guo, W.; Wang, X.; Luo, P.; Sun, J. The relationship between neutrophil-to-lymphocyte ratio and diabetic peripheral neuropathy in Type 2 diabetes mellitus. Medicine 2017, 96, e8289. [Google Scholar] [CrossRef]
- Bhagavati, S. Autoimmune Disorders of the Nervous System: Pathophysiology, Clinical Features, and Therapy. Front. Neurol. 2021, 12, 664664. [Google Scholar] [CrossRef]
- Oukka, M.; Bettelli, E. Regulation of lymphocyte trafficking in central nervous system autoimmunity. Curr. Opin. Immunol. 2018, 55, 38–43. [Google Scholar] [CrossRef]
- Montague, K.; Simeoli, R.; Valente, J.; Malcangio, M. A novel interaction between CX(3)CR(1) and CCR(2) signalling in monocytes constitutes an underlying mechanism for persistent vincristine-induced pain. J. Neuroinflammation 2018, 15, 101. [Google Scholar] [CrossRef]
- Jamilloux, Y.; Magy, L.; Hurtevent, J.F.; Gondran, G.; de Seze, J.; Launay, D.; Ly, K.H.; Lambert, M.; Hachulla, E.; Hatron, P.Y.; et al. Immunological profiles determine neurological involvement in Sjögren’s syndrome. Eur. J. Intern. Med. 2014, 25, 177–181. [Google Scholar] [CrossRef]
- Macedo, A.C.; Isaac, L. Systemic Lupus Erythematosus and Deficiencies of Early Components of the Complement Classical Pathway. Front. Immunol. 2016, 7, 55. [Google Scholar] [CrossRef] [PubMed]
- Fukami, Y.; Koike, H.; Iijima, M.; Mouri, N.; Nishi, R.; Katsuno, M. Role of complement components in vasculitic neuropathy associated with systemic lupus erythematosus and rheumatoid arthritis. Muscle Nerve 2022, 66, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Durcan, L.; Petri, M. The clinical and serological associations of hypocomplementemia in a longitudinal sle cohort. Semin. Arthritis Rheum. 2020, 50, 1081–1086. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Anaya, J.M.; García-Carrasco, M.; Rosas, J.; Bové, A.; Claver, G.; Diaz, L.A.; Herrero, C.; Font, J. Cutaneous vasculitis in primary Sjögren syndrome: Classification and clinical significance of 52 patients. Medicine 2004, 83, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Ye, W.; Chen, S.; Huang, X.; Qin, W.; Zhang, T.; Zhu, X.; Zhu, X.; Lin, C.; Wang, X. Clinical features and risk factors of neurological involvement in Sjögren’s syndrome. BMC Neurosci. 2018, 19, 26. [Google Scholar] [CrossRef]
- Charoenngam, N.; Holick, M.F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef]
- Bucurica, S.; Prodan, I.; Pavalean, M.; Taubner, C.; Bucurica, A.; Socol, C.; Calin, R.; Ionita-Radu, F.; Jinga, M. Association of Vitamin D Deficiency and Insufficiency with Pathology in Hospitalized Patients. Diagnostics 2023, 13, 998. [Google Scholar] [CrossRef]
- Dankers, W.; Colin, E.M.; van Hamburg, J.P.; Lubberts, E. Vitamin D in Autoimmunity: Molecular Mechanisms and Therapeutic Potential. Front. Immunol. 2016, 7, 697. [Google Scholar] [CrossRef]
- Kiraly, S.J.; Kiraly, M.A.; Hawe, R.D.; Makhani, N. Vitamin D as a neuroactive substance: Review. Sci. World J. 2006, 6, 125–139. [Google Scholar] [CrossRef]
- Skalli, S.; Muller, M.; Pradines, S.; Halimi, S.; Wion-Barbot, N. Vitamin D deficiency and peripheral diabetic neuropathy. Eur. J. Intern. Med. 2012, 23, e67–e68. [Google Scholar] [CrossRef]
- Yesil, H.; Sungur, U.; Akdeniz, S.; Gurer, G.; Yalcın, B.; Dundar, U. Association between serum vitamin D levels and neuropathic pain in rheumatoid arthritis patients: A cross-sectional study. Int. J. Rheum. Dis. 2018, 21, 431–439. [Google Scholar] [CrossRef]
- Seeliger, T.; Prenzler, N.K.; Gingele, S.; Seeliger, B.; Körner, S.; Thiele, T.; Bönig, L.; Sühs, K.W.; Witte, T.; Stangel, M.; et al. Neuro-Sjögren: Peripheral Neuropathy with Limb Weakness in Sjögren’s Syndrome. Front. Immunol. 2019, 10, 1600. [Google Scholar] [CrossRef] [PubMed]
- Margaretten, M. Neurologic Manifestations of Primary Sjögren Syndrome. Rheum. Dis. Clin. N. Am. 2017, 43, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Goules, A.V.; Tzioufas, A.G. Lymphomagenesis in Sjögren’s syndrome: Predictive biomarkers towards precision medicine. Autoimmun. Rev. 2019, 18, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Segal, B.; Thomas, W.; Rogers, T.; Leon, J.M.; Hughes, P.; Patel, D.; Patel, K.; Novitzke, J.; Rohrer, M.; Gopalakrishnan, R.; et al. Prevalence, severity, and predictors of fatigue in subjects with primary Sjögren’s syndrome. Arthritis Rheum. 2008, 59, 1780–1787. [Google Scholar] [CrossRef]
- McCoy, S.S.; Baer, A.N. Neurological Complications of Sjögren’s Syndrome: Diagnosis and Management. Curr. Treat. Options Rheumatol. 2017, 3, 275–288. [Google Scholar] [CrossRef]
- Alunno, A.; Carubbi, F.; Bartoloni, E.; Cipriani, P.; Giacomelli, R.; Gerli, R. The kaleidoscope of neurological manifestations in primary Sjögren’s syndrome. Ann. Rheum. Dis. 2019, 37 (Suppl. 118), 192–198. [Google Scholar]
- Terrier, B.; Lacroix, C.; Guillevin, L.; Hatron, P.Y.; Dhote, R.; Maillot, F.; Diot, E.; Sarrot-Reynauld, F.; Sordet, C.; Dubourg, O.; et al. Diagnostic and prognostic relevance of neuromuscular biopsy in primary Sjögren’s syndrome-related neuropathy. Arthritis Rheum. 2007, 57, 1520–1529. [Google Scholar] [CrossRef]
- Fan, G.; Dai, F.; Chen, S.; Sun, Y.; Qian, H.; Yang, G.; Liu, Y.; Shi, G. Neurological Involvement in Patients with Primary Sjögren’s Syndrome. Am. J. Clin. Oncol. 2021, 27, 50–55. [Google Scholar] [CrossRef]
- Tani, J.; Liao, H.T.; Hsu, H.C.; Chen, L.F.; Chang, T.S.; Shin-Yi Lin, C.; Sung, J.Y. Immune-mediated axonal dysfunction in seropositive and seronegative primary Sjögren’s syndrome. Ann. Clin. Transl. Neurol. 2020, 7, 819–828. [Google Scholar] [CrossRef]
- Descamps, E.; Henry, J.; Labeyrie, C.; Adams, D.; Ghaidaa, A.N.; Vandendries, C.; Adam, C.; Aiello, D.; Mariette, X.; Seror, R. Small fiber neuropathy in Sjögren syndrome: Comparison with other small fiber neuropathies. Muscle Nerve 2020, 61, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Dudley, M.T.; Borkum, M.; Basera, W.; Wearne, N.; Heckmann, J.M. Peripheral neuropathy in HIV patients on antiretroviral therapy: Does it impact function? J. Neurol. Sci. 2019, 406, 116451. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Thomas, S.; Van Doormaal, P.T.; Höke, A. Relation of exercise and pain in patients with idiopathic distal axonal polyneuropathies. J. Peripher. Nerv. Syst. 2020, 25, 388–394. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| PN+ Group | PN− Group | p-Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| No = 31 (25.61%) | No = 90 (74.38%) | ||
| Demographic Characteristics | |||
| Age at pSS diagnosis (years) | 49.65 ± 10.75 | 47.03 ± 11.79 | 0.810 a |
| Sex | 0.569 a | ||
| Female (n, %) Male (n, %) | 31 (100%) | 87 (96.66%) | - |
| - | 3 (3.33%) | - | |
| Glandular Manifestations | |||
| Xerostomia, n (%) | 28 (90.32%) | 83 (92.22%) | 0.497 a |
| Xerophthalmia, n (%) | 26 (83.87%) | 48 (53.33%) | 0.003 a |
| Clinical Scores | |||
| VAS pain score (mm) | 4.90 ± 2.45 | 1.27 ± 1.32 | 0.001 b |
| ESSDAI score | 20.35 ± 7.56 | 15.13 ± 7.57 | 0.001 b |
| ESSDAI score 5–13 | 6 (19.35%) | 44 (48.88%) | 0.001 a |
| ESSDAI score ≥ 14 | 25 (80.64%) | 46 (51.11%) | |
| Laboratory Findings | PN+ Group Mean ± SD | PN− Group Mean ± SD | p-Value |
|---|---|---|---|
| Cells Count | |||
| Neutrophils (109/µL) | 3.42 ± 0.83 | 2.89 ± 0.53 | 0.001 b |
| Lymphocytes (109/µL) | 1.09 ± 0.99 | 1.13 ± 0.09 | 0.025 b |
| Monocyte (109/µL) | 0.25 ± 0.70 | 0.34 ± 0.14 | 0.013 b |
| Platelets (109/L) | 262.65 ± 38.45 | 254.9 ± 54.25 | 0.131 b |
| Cellular Ratios | |||
| NLR | 3.14 ± 0.76 | 2.58 ± 0.58 | 0.001 b |
| MLR | 0.24 ± 0.96 | 0.30 ± 0.12 | 0.003 b |
| PLR | 241.58 ± 37.89 | 228.33 ± 58.72 | 0.056 b |
| Immunological Results | |||
| ANA (U/mL) | 3.48 ± 2.21 | 4.23 ± 2.21 | 0.064 b |
| positive (n, %) | 26 (83.87%) | 77 (85.55%) | 0.777 a |
| Anti-Ro/SSA (U/mL) | 122.50 ± 85.58 | 145.76 ± 79.52 | 0.183 b |
| positive (n, %) | 23 (74.19%) | 79 (87.77%) | 0.089 a |
| Anti-La/SSB (U/mL) | 89.59 ± 138.60 | 91.2 ± 85.99 | 0.303 b |
| positive (n, %) | 17 (54.83%) | 55 (61.11%) | 0.672 a |
| Total proteins (g/dL) | 7.37 ± 0.68 | 7.76 ± 0.91 | 0.019 b |
| Gammaglobulins (g/dL) | 1.28 ± 0.39 | 1.48 ± 0.4 | 0.012 b |
| IgA (mg/L) | 248.39 ± 124.28 | 304.26 ± 160.37 | 0.054 b |
| IgG (mg/L) | 1514.19 ± 646.78 | 1797.25 ± 740.09 | 0.913 b |
| IgM (mg/L) | 175.03 ± 107.73 | 180.28 ± 131.85 | 0.525 b |
| RF (U/mL) | 54.67 ± 72.92 | 54.61 ± 59.98 | 0.529 b |
| C3 (mg/dL) | 113.94 ± 16.26 | 126.78 ± 38.72 | 0.022 b |
| C4 (mg/dL) | 16.17 ± 7.59 | 22.97 ± 8.56 | 0.001 b |
| Vitamin D (ng/mL) | 13.90 ± 7.19 | 24.86 ± 11.04 | 0.001 b |
| Inflammatory Results | |||
| ESR (mm/h) | 33.81 ± 25.81 | 35.48 ± 24.46 | 0.563 b |
| hs- CRP (mg/L) | 27.22 ± 18.21 | 26.06 ± 30.32 | 0.263 b |
| Cryoglobulins, n (%) | 2 (6.45%) | 6 (6.66%) | 0.665 a |
| PN+ Group | PN− Group | p-Value | |
|---|---|---|---|
| Peripheral Neuropathy | |||
| Pure sensory neuropathy | 21 (67.74%) | - | - |
| Sensorimotor polyneuropathy | 10 (32.25%) | - | - |
| Clinical Score | |||
| TNSr | 14.65 ± 3.99 | - | - |
| moderate neuropathy | 25 (80.64%) | ||
| severe neuropathy | 6 (19.35%) | ||
| Sudoscan | 18 (43.90%) | - | - |
| no dysfunction | 11 (35.48%) | - | - |
| moderate dysfunction | 14 (45.16%) | - | - |
| severe dysfunction | 6 (19.35%) | - | - |
| Extraglandular Manifestation | |||
| Purpura, n (%) | 8 (25.80%) | 24 (26.66%) | 0.564 a |
| B-NHL, n (%) | 2 (4.87%) | - | 0.064 a |
| Laboratory Findings | Unstandardized Coefficients | Standardized Coefficients | T | p | 95.0% Confidence Interval for B | ||
|---|---|---|---|---|---|---|---|
| Β | Standard Error | Beta | Lower Bound | Upper Bound | |||
| (Constant) | 0.387 | 0.393 | - | 3.527 | 0.001 * | 0.608 | 2.166 |
| NLR | 0.148 | 0.058 | 0.230 | 2.542 | 0.012 * | 0.033 | 0.263 |
| MLR | −0.741 | 0.276 | −0.211 | −2.680 | 0.008 * | −1.289 | −0.194 |
| Total proteins (g/dL) | −0.066 | 0.038 | −0.133 | −1.759 | 0.081 | −0.141 | 0.008 |
| Gammaglobulins (g/dL) | −0.257 | 0.085 | −0.238 | −3.013 | 0.003 * | −0.426 | −0.088 |
| C3 (mg/dL) | 0.001 | 0.001 | −0.016 | −0.194 | 0.847 | −0.002 | 0.002 |
| C4 (mg/dL) | −0.009 | 0.004 | −0.186 | −2.204 | 0.030 * | −0.018 | −0.001 |
| Vitamin D (ng/mL) | −0.010 | 0.004 | −0.257 | −2.657 | 0.009 * | −0.017 | −0.003 |
| Age | 0.003 | 0.003 | 0.072 | 0.993 | 0.353 | −0.003 | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihai, A.; Chitimus, D.M.; Jurcut, C.; Blajut, F.C.; Opris-Belinski, D.; Caruntu, C.; Ionescu, R.; Caruntu, A. Comparative Analysis of Hematological and Immunological Parameters in Patients with Primary Sjögren’s Syndrome and Peripheral Neuropathy. J. Clin. Med. 2023, 12, 3672. https://doi.org/10.3390/jcm12113672
Mihai A, Chitimus DM, Jurcut C, Blajut FC, Opris-Belinski D, Caruntu C, Ionescu R, Caruntu A. Comparative Analysis of Hematological and Immunological Parameters in Patients with Primary Sjögren’s Syndrome and Peripheral Neuropathy. Journal of Clinical Medicine. 2023; 12(11):3672. https://doi.org/10.3390/jcm12113672
Chicago/Turabian StyleMihai, Ancuta, Diana Maria Chitimus, Ciprian Jurcut, Florin Cristian Blajut, Daniela Opris-Belinski, Constantin Caruntu, Ruxandra Ionescu, and Ana Caruntu. 2023. "Comparative Analysis of Hematological and Immunological Parameters in Patients with Primary Sjögren’s Syndrome and Peripheral Neuropathy" Journal of Clinical Medicine 12, no. 11: 3672. https://doi.org/10.3390/jcm12113672