
Joint Response to Exercise Is Affected by Knee Osteoarthritis: An Infrared Thermography Analysis
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
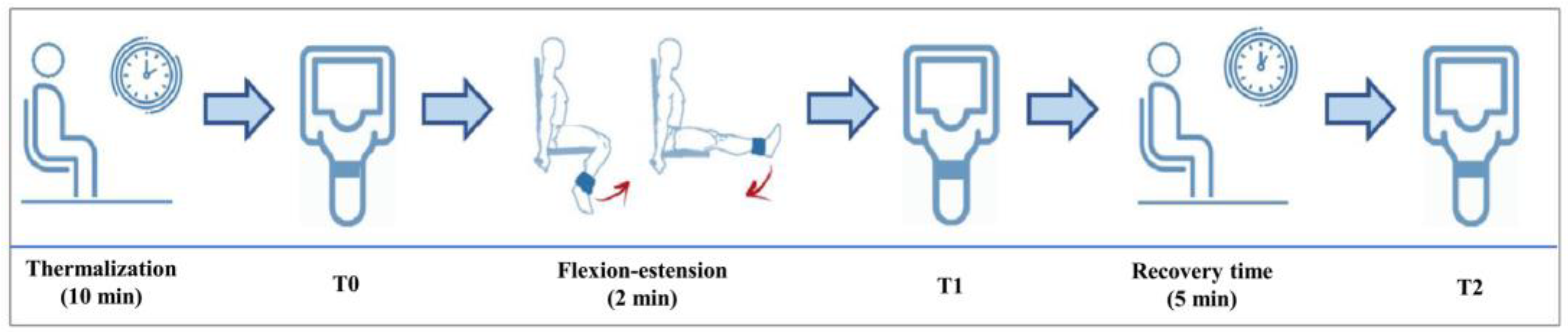
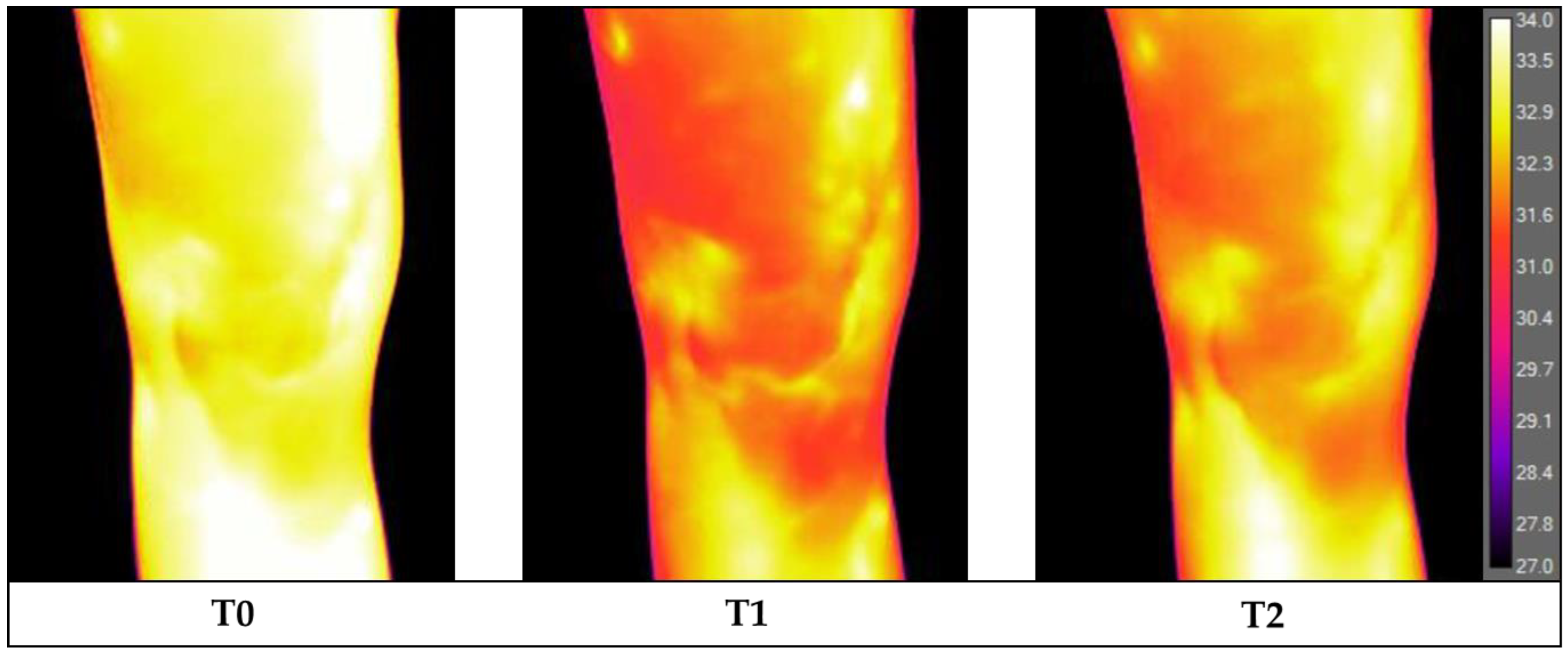
2.1. Infrared Thermography Procedure, Exercise, and Analysis
2.2. Statistical Analysis
3. Results
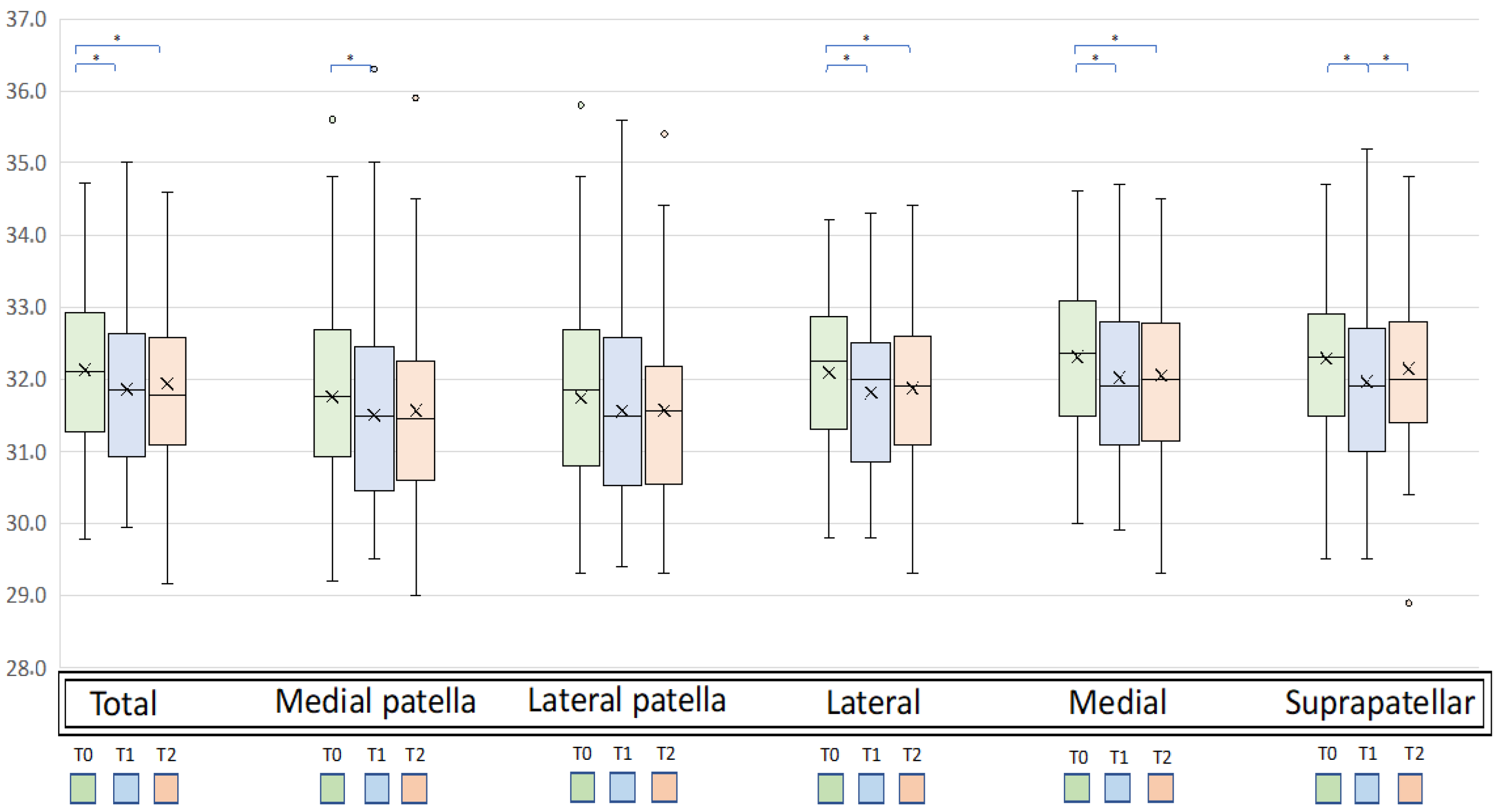
3.1. Temperature Changes
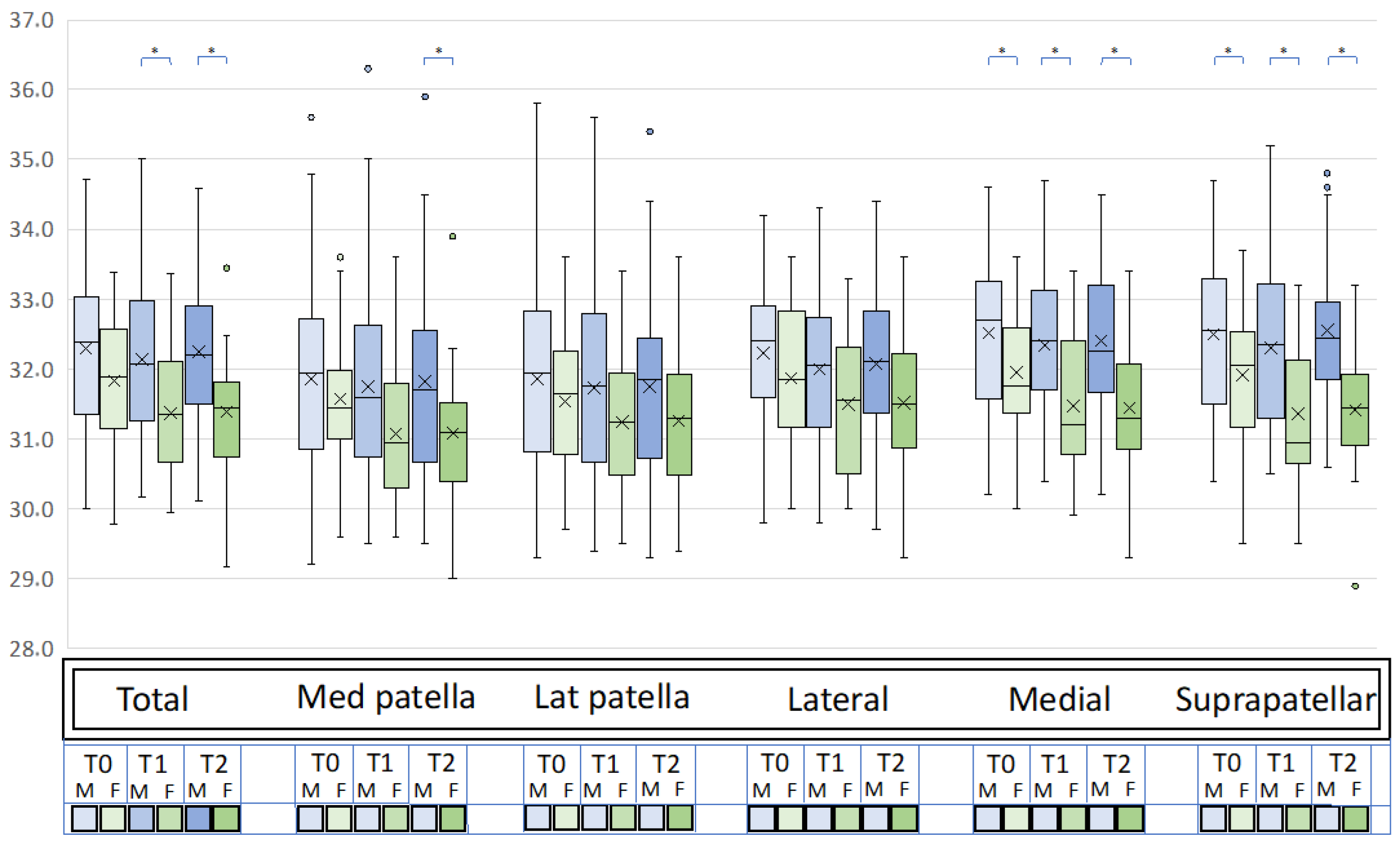
3.2. Influences of Demographic Variables
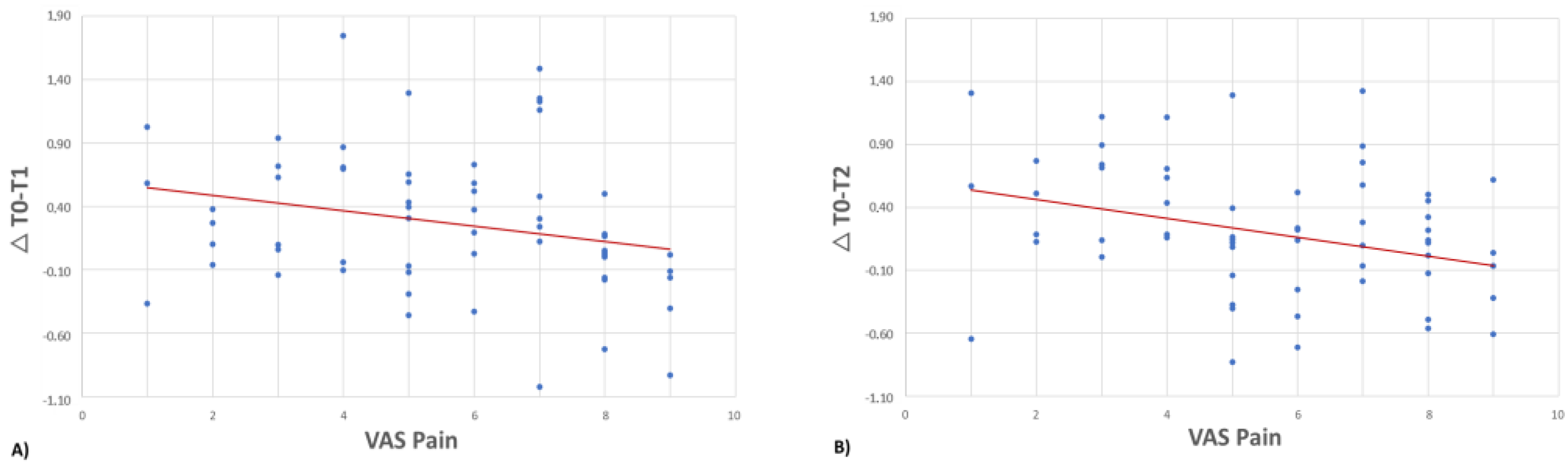
3.3. Influence of Clinical Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hildebrandt, C.; Raschner, C.; Ammer, K. An Overview of Recent Application of Medical Infrared Thermography in Sports Medicine in Austria. Sensors 2010, 10, 4700–4715. [Google Scholar] [CrossRef] [PubMed]
- Ring, F. Thermal Imaging Today and Its Relevance to Diabetes. J. Diabetes Sci. Technol. 2010, 4, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Tattersall, G.J. Infrared Thermography: A Non-Invasive Window into Thermal Physiology. Comp. Biochem. Physiol. A Mol. Integr. Physiol. 2016, 202, 78–98. [Google Scholar] [CrossRef] [PubMed]
- Schiavon, G.; Capone, G.; Frize, M.; Zaffagnini, S.; Candrian, C.; Filardo, G. Infrared Thermography for the Evaluation of Inflammatory and Degenerative Joint Diseases: A Systematic Review. Cartilage 2021, 13, 1790S–1801S. [Google Scholar] [CrossRef]
- Khan, A.A.; Arora, A.S. Thermography as an Economical Alternative Modality to Mammography for Early Detection of Breast Cancer. J. Healthc. Eng. 2021, 2021, 5543101. [Google Scholar] [CrossRef]
- Nakagami, G.; Sanada, H.; Iizaka, S.; Kadono, T.; Higashino, T.; Koyanagi, H.; Haga, N. Predicting Delayed Pressure Ulcer Healing Using Thermography: A Prospective Cohort Study. J. Wound Care 2010, 19, 465–466, 468, 470. [Google Scholar] [CrossRef]
- Wallace, I.J.; Worthington, S.; Felson, D.T.; Jurmain, R.D.; Wren, K.T.; Maijanen, H.; Woods, R.J.; Lieberman, D.E. Knee Osteoarthritis Has Doubled in Prevalence since the Mid-20th Century. Proc. Natl. Acad. Sci. USA 2017, 114, 9332–9336. [Google Scholar] [CrossRef]
- Sanchez-Lopez, E.; Coras, R.; Torres, A.; Lane, N.E.; Guma, M. Synovial Inflammation in Osteoarthritis Progression. Nat. Rev. Rheumatol. 2022, 18, 258–275. [Google Scholar] [CrossRef]
- Boffa, A.; Merli, G.; Andriolo, L.; Lattermann, C.; Salzmann, G.M.; Filardo, G. Synovial Fluid Biomarkers in Knee Osteoarthritis: A Systematic Review and Quantitative Evaluation Using BIPEDs Criteria. Cartilage 2021, 13, 82S–103S. [Google Scholar] [CrossRef]
- Nanus, D.E.; Badoume, A.; Wijesinghe, S.N.; Halsey, A.M.; Hurley, P.; Ahmed, Z.; Botchu, R.; Davis, E.T.; Lindsay, M.A.; Jones, S.W. Synovial Tissue from Sites of Joint Pain in Knee Osteoarthritis Patients Exhibits a Differential Phenotype with Distinct Fibroblast Subsets. EBioMedicine 2021, 72, 103618. [Google Scholar] [CrossRef]
- de Silva, M.; Kyle, V.; Hazleman, B.; Salisbury, R.; Page Thomas, P.; Wraight, P. Assessment of Inflammation in the Rheumatoid Knee Joint: Correlation between Clinical, Radioisotopic, and Thermographic Methods. Ann. Rheum. Dis. 1986, 45, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Varjú, G.; Pieper, C.F.; Renner, J.B.; Kraus, V.B. Assessment of Hand Osteoarthritis: Correlation between Thermographic and Radiographic Methods. Rheumatology 2004, 43, 915–919. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.M.; Chun, J.H.; Hong, S.; Lee, C.-K.; Yoo, B.; Oh, J.S.; Kim, Y.-G. The Value of Thermal Imaging for Knee Arthritis: A Single-Center Observational Study. Yonsei Med. J. 2022, 63, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Romanò, C.L.; Logoluso, N.; Dell’Oro, F.; Elia, A.; Drago, L. Telethermographic Findings after Uncomplicated and Septic Total Knee Replacement. Knee 2012, 19, 193–197. [Google Scholar] [CrossRef]
- Brito, C.J.; Miarka, B.; García-Pastor, T.; Pérez, D.I.V.; Marins, J.C.B.; Sillero-Quintana, M. Osteoarthritis Subjects Have Differentiated Lower Extremity Thermal Skin Response after the Concurrent Acute Training Session. J. Therm. Anal. Calorim. 2021, 145, 2467–2475. [Google Scholar] [CrossRef]
- Arfaoui, A.; Bouzid, M.A.; Pron, H.; Taiar, R.; Polidori, G. Application of Infrared Thermography as a Diagnostic Tool of Knee Osteoarthritis. J. Therm. Sci. Technol. 2012, 7, 227–235. [Google Scholar] [CrossRef]
- Moreira, D.G.; Costello, J.T.; Brito, C.J.; Adamczyk, J.G.; Ammer, K.; Bach, A.J.E.; Costa, C.M.A.; Eglin, C.; Fernandes, A.A.; Fernández-Cuevas, I.; et al. Thermographic Imaging in Sports and Exercise Medicine: A Delphi Study and Consensus Statement on the Measurement of Human Skin Temperature. J. Therm. Biol. 2017, 69, 155–162. [Google Scholar] [CrossRef]
- Schwartz, R.G.; Getson, P.; O’Young, B.; Bernton, T.; Brioschi, M.; Schakaraschwilli, G.; Terzella, M.; Habibi, B.; Zhang, H.-Y. Guidelines for Neuro-Musculoskeletal Infrared Medical Thermology & Sympathetic Skin Response (SSR) Studies. Pan Am. J. Med. Thermol. 2021, 1–13. Available online: https://aathermology.org/wp-content/uploads/2018/04/AAT-NMSK-Guidelines-2021.pdf (accessed on 23 January 2023).
- Merla, A.; Mattei, P.A.; Di Donato, L.; Romani, G.L. Thermal Imaging of Cutaneous Temperature Modifications in Runners during Graded Exercise. Ann. Biomed. Eng. 2010, 38, 158–163. [Google Scholar] [CrossRef]
- Ring, E.F.J.; Ammer, K. The Technique of Infrared Imaging in Medicine. In Infrared Imaging: A Casebook in Clinical Medicin; IoP Publishing: Bristol, UK, 2015; pp. 1-1–1-10. [Google Scholar]
- Marins, J.C.B.; Moreira, D.G.; Cano, S.P.; Quintana, M.S.; Soares, D.D.; de Andrade Fernandes, A.; da Silva, F.S.; Costa, C.M.A.; dos Santos Amorim, P.R. Time Required to Stabilize Thermographic Images at Rest. Infrared Phys. Technol. 2014, 65, 30–35. [Google Scholar] [CrossRef]
- Danko, M.; Hudak, R.; Foffová, P.; Zivcak, J. An Importance of Camera—Subject Distance and Angle in Musculoskeletal Application of Medical Thermography. Acta Electrotech. Inf. 2010, 10, 57–59. [Google Scholar]
- De Marziani, L.; Boffa, A.; Angelelli, L.; Andriolo, L.; Di Martino, A.; Zaffagnini, S.; Filardo, G. Infrared Thermography in Symptomatic Knee Osteoarthritis: Joint Temperature Differs Based on Patient and Pain Characteristics. J. Clin. Med. 2023, 12, 2319. [Google Scholar] [CrossRef] [PubMed]
- Denoble, A.E.; Hall, N.; Pieper, C.F.; Kraus, V.B. Patellar Skin Surface Temperature by Thermography Reflects Knee Osteoarthritis Severity. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2010, 3, 69–75. [Google Scholar] [CrossRef] [PubMed]
- de Lacerda, A.P.D.; de Andrade, P.R.; Kamonseki, D.H.; Parizotto, N.A.; da Silva, A.S.A.; de Medeiros, L.B.; de Almeida Ferreira, J.J. Accuracy of Infrared Thermography in Detecting Tendinopathy: A Systematic Review with Meta-Analysis. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2022, 58, 117–125. [Google Scholar] [CrossRef]
- Kumar, P.; Gaurav, A.; Rajnish, R.K.; Sharma, S.; Kumar, V.; Aggarwal, S.; Patel, S. Applications of Thermal Imaging with Infrared Thermography in Orthopaedics. J. Clin. Orthop. Trauma 2022, 24, 101722. [Google Scholar] [CrossRef]
- Calin, M.A.; Mologhianu, G.; Savastru, R.; Calin, M.R.; Brailescu, C.M. A Review of the Effectiveness of Thermal Infrared Imaging in the Diagnosis and Monitoring of Knee Diseases. Infrared Phys. Technol. 2015, 69, 19–25. [Google Scholar] [CrossRef]
- Lohchab, V.; Rathod, P.; Mahapatra, P.K.; Bachhal, V.; Hooda, A. Non-invasive Assessment of Knee Osteoarthritis Patients Using Thermal Imaging. IET Sci. Meas. Technol. 2022, 16, 242–249. [Google Scholar] [CrossRef]
- Formenti, D.; Ludwig, N.; Gargano, M.; Gondola, M.; Dellerma, N.; Caumo, A.; Alberti, G. Thermal Imaging of Exercise-Associated Skin Temperature Changes in Trained and Untrained Female Subjects. Ann. Biomed. Eng. 2013, 41, 863–871. [Google Scholar] [CrossRef]
- Merla, A.; Iodice, P.; Tangherlini, A.; De Michele, G.; Di Romualdo, S.; Saggini, R.; Romani, G. Monitoring Skin Temperature in Trained and Untrained Subjects throughout Thermal Video. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 1684–1686. [Google Scholar] [CrossRef]
- Hillen, B.; Pfirrmann, D.; Nägele, M.; Simon, P. Infrared Thermography in Exercise Physiology: The Dawning of Exercise Radiomics. Sport. Med. Auckl. NZ 2020, 50, 263–282. [Google Scholar] [CrossRef]
- Vainer, B.G. FPA-Based Infrared Thermography as Applied to the Study of Cutaneous Perspiration and Stimulated Vascular Response in Humans. Phys. Med. Biol. 2005, 50, R63–R94. [Google Scholar] [CrossRef]
- Formenti, D.; Ludwig, N.; Trecroci, A.; Gargano, M.; Michielon, G.; Caumo, A.; Alberti, G. Dynamics of Thermographic Skin Temperature Response during Squat Exercise at Two Different Speeds. J. Therm. Biol. 2016, 59, 58–63. [Google Scholar] [CrossRef]
- Kenney, W.L.; Armstrong, C.G. Reflex Peripheral Vasoconstriction Is Diminished in Older Men. J. Appl. Physiol. 1996, 80, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Holowatz, L.A.; Kenney, W.L. Peripheral Mechanisms of Thermoregulatory Control of Skin Blood Flow in Aged Humans. J. Appl. Physiol. 2010, 109, 1538–1544. [Google Scholar] [CrossRef] [PubMed]
- Kalliokoski, K.K.; Knuuti, J.; Nuutila, P. Relationship between Muscle Blood Flow and Oxygen Uptake during Exercise in Endurance-Trained and Untrained Men. J. Appl. Physiol. 2005, 98, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.E.; Losina, E.; Nevitt, M.C.; Roemer, F.W.; Guermazi, A.; Lynch, J.A.; Katz, J.N.; Kent Kwoh, C.; Kraus, V.B.; Hunter, D.J. Semiquantitative Imaging Biomarkers of Knee Osteoarthritis Progression: Data from the Foundation for the National Institutes of Health Osteoarthritis Biomarkers Consortium. Arthritis Rheumatol. 2016, 68, 2422–2431. [Google Scholar] [CrossRef]
- Riis, R.G.C.; Gudbergsen, H.; Henriksen, M.; Ballegaard, C.; Bandak, E.; Röttger, D.; Bliddal, H.; Hansen, B.B.; Hangaard, S.; Boesen, M. Synovitis Assessed on Static and Dynamic Contrast-Enhanced Magnetic Resonance Imaging and Its Association with Pain in Knee Osteoarthritis: A Cross-Sectional Study. Eur. J. Radiol. 2016, 85, 1099–1108. [Google Scholar] [CrossRef]
- Moss, P.; Benson, H.A.E.; Will, R.; Wright, A. Patients with Knee Osteoarthritis Who Score Highly on the PainDETECT Questionnaire Present with Multimodality Hyperalgesia, Increased Pain, and Impaired Physical Function. Clin. J. Pain 2018, 34, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tölle, T.R. PainDETECT: A New Screening Questionnaire to Identify Neuropathic Components in Patients with Back Pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef]
- Moreton, B.J.; Tew, V.; das Nair, R.; Wheeler, M.; Walsh, D.A.; Lincoln, N.B. Pain Phenotype in Patients with Knee Osteoarthritis: Classification and Measurement Properties of PainDETECT and Self-Report Leeds Assessment of Neuropathic Symptoms and Signs Scale in a Cross-Sectional Study. Arthritis Care Res. 2015, 67, 519–528. [Google Scholar] [CrossRef]
- Bonnet, C.S.; Walsh, D.A. Osteoarthritis, Angiogenesis and Inflammation. Rheumatology 2005, 44, 7–16. [Google Scholar] [CrossRef]
- French, H.P.; Smart, K.M.; Doyle, F. Prevalence of Neuropathic Pain in Knee or Hip Osteoarthritis: A Systematic Review and Meta-Analysis. Semin. Arthritis Rheum. 2017, 47, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cracowski, J.-L.; Roustit, M. Human Skin Microcirculation. Compr. Physiol. 2020, 10, 1105–1154. [Google Scholar] [CrossRef] [PubMed]
- Minson, C.T.; Berry, L.T.; Joyner, M.J. Nitric Oxide and Neurally Mediated Regulation of Skin Blood Flow during Local Heating. J. Appl. Physiol. 2001, 91, 1619–1626. [Google Scholar] [CrossRef]
- Blaak, E. Gender Differences in Fat Metabolism. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Ansdell, P.; Thomas, K.; Hicks, K.M.; Hunter, S.K.; Howatson, G.; Goodall, S. Physiological Sex Differences Affect the Integrative Response to Exercise: Acute and Chronic Implications. Exp. Physiol. 2020, 105, 2007–2021. [Google Scholar] [CrossRef]
- Roepstorff, C.; Thiele, M.; Hillig, T.; Pilegaard, H.; Richter, E.A.; Wojtaszewski, J.F.P.; Kiens, B. Higher Skeletal Muscle Alpha2AMPK Activation and Lower Energy Charge and Fat Oxidation in Men than in Women during Submaximal Exercise. J. Physiol. 2006, 574, 125–138. [Google Scholar] [CrossRef]
- Hill, E.C.; Housh, T.J.; Smith, C.M.; Schmidt, R.J.; Johnson, G.O. Gender- and Muscle-Specific Responses During Fatiguing Exercise. J. Strength Cond. Res. 2018, 32, 1471–1478. [Google Scholar] [CrossRef]
- Parker, B.A.; Smithmyer, S.L.; Pelberg, J.A.; Mishkin, A.D.; Herr, M.D.; Proctor, D.N. Sex Differences in Leg Vasodilation during Graded Knee Extensor Exercise in Young Adults. J. Appl. Physiol. 2007, 103, 1583–1591. [Google Scholar] [CrossRef]
- Kaciuba-Uscilko, H.; Grucza, R. Gender Differences in Thermoregulation. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 533–536. [Google Scholar] [CrossRef]
- Alizadeh, S.; Rayner, M.; Mahmoud, M.M.I.; Behm, D.G. Push-Ups vs. Bench Press Differences in Repetitions and Muscle Activation between Sexes. J. Sport. Sci. Med. 2020, 19, 289–297. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex, M/W | 38/22 |
| Age, years | 61.4 ± 9.2 (43–75) |
| BMI, kg/m2 | 25.4 ± 3.0 (19.5–33.8) |
| Side | Right: 33—Left: 27 |
| Symptom duration, months | 108.3 ± 99.3 (18–372) |
| Symptom onset | Acute: 14—Chronic: 46 |
| Previous knee surgery, yes/no | 31/29 |
| Smoker, yes/no | 13/47 |
| Kellgren–Lawrence grade | Grade 2: 30 |
| Grade 3: 21 | |
| Grade 4: 9 | |
| VAS pain | 5.6 ± 2.3 (1–9) |
| IKDC subjective score | 41.3 ± 14.2 (9.2–81.6) |
| IKDC objective score | Grade 1: 8 |
| Grade 2: 29 | |
| Grade 3: 10 | |
| Grade 4: 13 | |
| KOOS pain | 59.8 ± 18.9 (2–94) |
| KOOS symptoms | 60.4 ± 19.7 (18–100) |
| KOOS ADL | 69.5 ± 18.4 (6–100) |
| KOOS QoL | 34.5 ± 16.2 (0–75) |
| KOOS Sport/Rec | 43.8 ± 17.7 (20–90) |
| Tegner score pre-treatment | 2.2 ± 1.2 (1–5) |
| PainDETECT questionnaire | 8.7 ± 5.5 (0–25) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Marziani, L.; Boffa, A.; Orazi, S.; Andriolo, L.; Di Martino, A.; Zaffagnini, S.; Filardo, G. Joint Response to Exercise Is Affected by Knee Osteoarthritis: An Infrared Thermography Analysis. J. Clin. Med. 2023, 12, 3399. https://doi.org/10.3390/jcm12103399
De Marziani L, Boffa A, Orazi S, Andriolo L, Di Martino A, Zaffagnini S, Filardo G. Joint Response to Exercise Is Affected by Knee Osteoarthritis: An Infrared Thermography Analysis. Journal of Clinical Medicine. 2023; 12(10):3399. https://doi.org/10.3390/jcm12103399
Chicago/Turabian StyleDe Marziani, Luca, Angelo Boffa, Simone Orazi, Luca Andriolo, Alessandro Di Martino, Stefano Zaffagnini, and Giuseppe Filardo. 2023. "Joint Response to Exercise Is Affected by Knee Osteoarthritis: An Infrared Thermography Analysis" Journal of Clinical Medicine 12, no. 10: 3399. https://doi.org/10.3390/jcm12103399