
Psychometric Properties of the German Version of the Rivermead Post-Concussion Symptoms Questionnaire in Adolescents after Traumatic Brain Injury and Their Proxies

 ,
,  , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
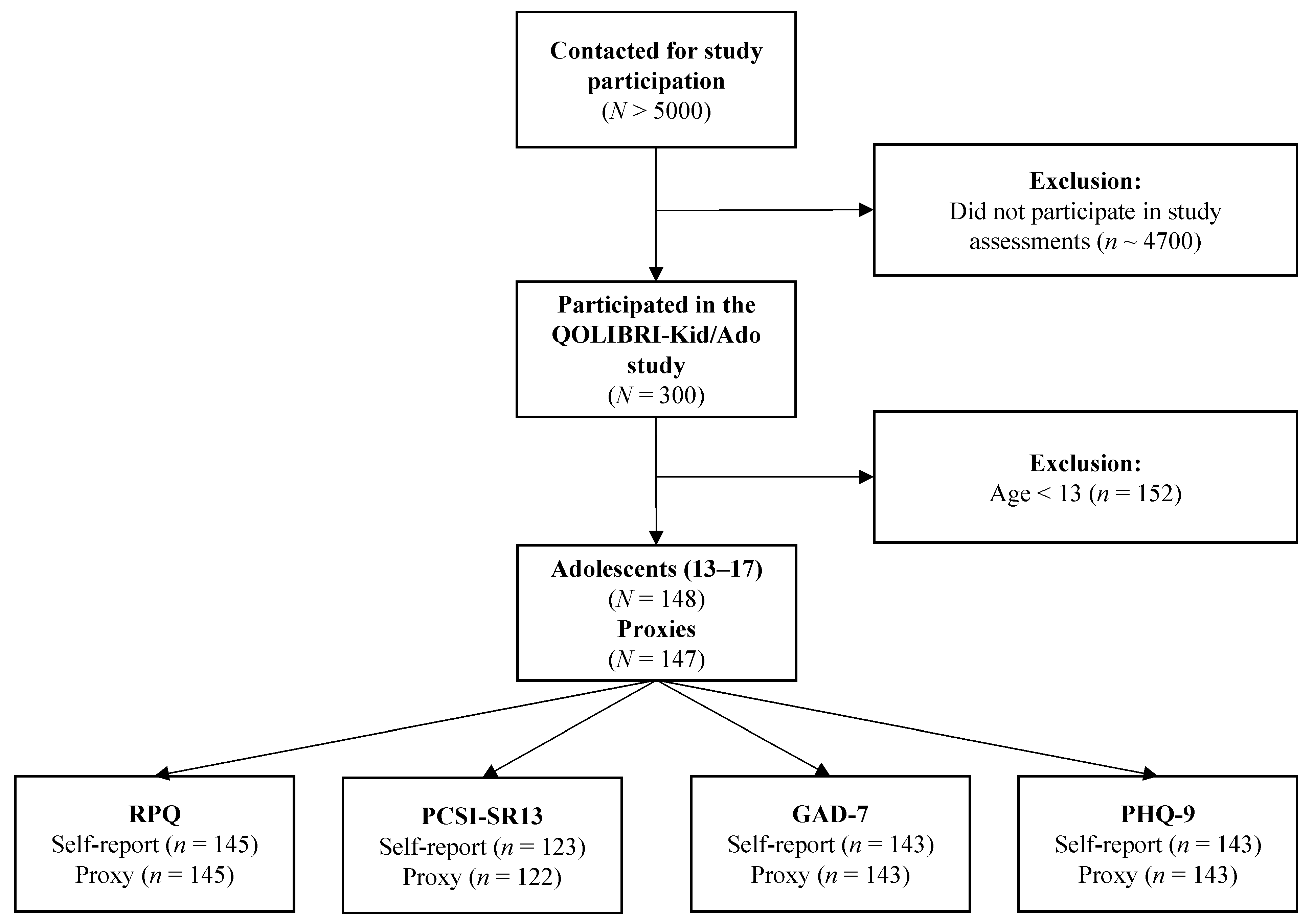
2.1. Study Sample
2.2. Ethical Approval
2.3. Sociodemographic and Injury-Related Data
2.4. Instruments
2.4.1. Rivermead Post-Concussion Symptoms Questionnaire (RPQ)
2.4.2. Post-Concussion Symptom Inventory (PCSI)
2.4.3. Generalized Anxiety Disorder Scale 7 (GAD-7)
2.4.4. Patient Health Questionnaire 9 (PHQ-9)
2.5. Statistical Analyses
2.5.1. Item Characteristics
2.5.2. Reliability
2.5.3. Factorial Validity
2.5.4. Construct Validity
2.6. Agreement between Self-Report and Proxy Assessment
3. Results
3.1. Sample Characteristics
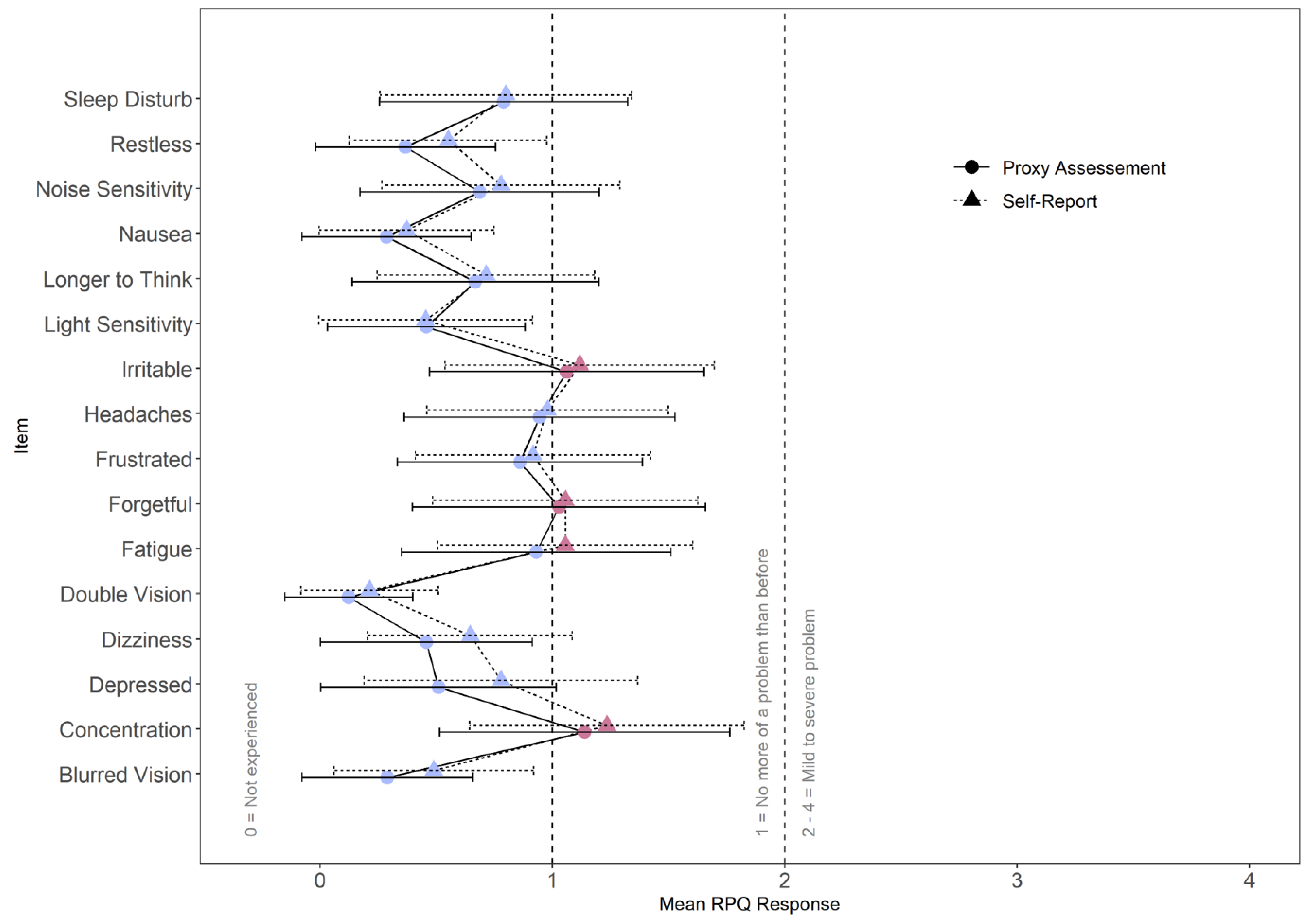
3.2. Item Characteristics
3.3. Reliability
3.4. Factorial Validity
3.5. Convergent and Divergent Validity
3.6. Agreement between Self-Report and Proxy Assessment
4. Discussion
Strengths and Limitations
5. Conclusions and Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Source | Symptom | Scale | M | SD | SK | KU | Floor | Ceiling | % Missing |
|---|---|---|---|---|---|---|---|---|---|
| Self-report | Headaches | S | 0.98 | 1.04 | 0.79 | −0.42 | 40 | 1 | 3.38 |
| Feeling of Dizziness | S | 0.65 | 0.88 | 1.23 | 0.59 | 55 | 0 | 2.70 | |
| Nausea and/or Vomiting | S | 0.37 | 0.75 | 2.36 | 5.79 | 73 | 1 | 2.03 | |
| Noise Sensitivity, easily upset by loud Noise | S | 0.78 | 1.02 | 1.14 | 0.50 | 54 | 2 | 2.03 | |
| Sleep Disturbance | S | 0.80 | 1.08 | 1.28 | 0.71 | 53 | 3 | 2.03 | |
| Fatigue, tiring more easily | S | 1.06 | 1.10 | 0.92 | 0.08 | 37 | 3 | 2.03 | |
| Being Irritable, easily angered | E | 1.12 | 1.16 | 0.87 | −0.13 | 37 | 5 | 2.03 | |
| Feeling Depressed or Tearful | E | 0.78 | 1.18 | 1.45 | 1.05 | 59 | 5 | 2.03 | |
| Feeling Frustrated or Impatient | E | 0.92 | 1.01 | 0.97 | 0.16 | 42 | 1 | 2.03 | |
| Forgetfulness, poor memory | C | 1.06 | 1.14 | 0.92 | −0.04 | 40 | 4 | 2.03 | |
| Poor Concentration | C | 1.23 | 1.18 | 0.55 | −0.88 | 34 | 3 | 2.03 | |
| Taking Longer to Think | C | 0.72 | 0.94 | 1.30 | 1.21 | 52 | 1 | 2.70 | |
| Blurred Vision | S | 0.49 | 0.86 | 1.83 | 2.76 | 68 | 1 | 2.03 | |
| Light Sensitivity, easily upset by bright light | S | 0.46 | 0.92 | 2.28 | 4.66 | 72 | 2 | 2.03 | |
| Double Vision | S | 0.21 | 0.59 | 2.91 | 8.06 | 84 | 0 | 2.03 | |
| Restlessness | E | 0.55 | 0.85 | 1.73 | 3.07 | 61 | 1 | 2.03 | |
| Proxy assessment | Headaches | S | 0.94 | 1.17 | 1.02 | −0.07 | 49 | 3 | 2.03 |
| Feeling of Dizziness | S | 0.46 | 0.91 | 1.94 | 2.70 | 72 | 1 | 4.05 | |
| Nausea and/or Vomiting | S | 0.29 | 0.73 | 3.10 | 10.37 | 79 | 1 | 3.38 | |
| Noise Sensitivity, easily upset by loud Noise | S | 0.69 | 1.03 | 1.34 | 0.74 | 60 | 1 | 2.70 | |
| Sleep Disturbance | S | 0.79 | 1.07 | 1.28 | 0.82 | 53 | 3 | 3.38 | |
| Fatigue, tiring more easily | S | 0.93 | 1.16 | 0.97 | −0.32 | 49 | 2 | 2.70 | |
| Being Irritable, easily angered | E | 1.06 | 1.18 | 1.07 | 0.25 | 39 | 6 | 2.03 | |
| Feeling Depressed or Tearful | E | 0.51 | 1.01 | 2.21 | 4.21 | 70 | 4 | 3.38 | |
| Feeling Frustrated or Impatient | E | 0.86 | 1.06 | 1.23 | 0.81 | 46 | 3 | 2.70 | |
| Forgetfulness, poor memory | C | 1.03 | 1.26 | 0.89 | −0.48 | 49 | 5 | 2.70 | |
| Poor Concentration | C | 1.14 | 1.25 | 0.72 | −0.70 | 43 | 5 | 2.70 | |
| Taking Longer to Think | C | 0.67 | 1.06 | 1.48 | 1.12 | 63 | 2 | 2.03 | |
| Blurred Vision | S | 0.29 | 0.74 | 3.03 | 9.82 | 80 | 1 | 2.03 | |
| Light Sensitivity, easily upset by bright light | S | 0.46 | 0.85 | 1.88 | 2.57 | 70 | 0 | 2.70 | |
| Double Vision | S | 0.12 | 0.55 | 5.49 | 32.81 | 91 | 1 | 2.03 | |
| Restlessness | E | 0.37 | 0.77 | 2.24 | 4.79 | 75 | 1 | 2.70 |
References
- Dewan, M.C.; Mummareddy, N.; Wellons, J.C.; Bonfield, C.M. Epidemiology of Global Pediatric Traumatic Brain Injury: Qualitative Review. World Neurosurg. 2016, 91, 497–509.e1. [Google Scholar] [CrossRef] [PubMed]
- Araki, T.; Yokota, H.; Morita, A. Pediatric Traumatic Brain Injury: Characteristic Features, Diagnosis, and Management. Neurol. Med. Chir. 2017, 57, 82–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riemann, L.; Zweckberger, K.; Unterberg, A.; El Damaty, A.; Younsi, A.; The Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) Investigators and Participants. Injury Causes and Severity in Pediatric Traumatic Brain Injury Patients Admitted to the Ward or Intensive Care Unit: A Collaborative European Neurotrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) Study. Front. Neurol. 2020, 11, 345. [Google Scholar] [CrossRef] [PubMed]
- Babikian, T.; Merkley, T.; Savage, R.C.; Giza, C.C.; Levin, H. Chronic Aspects of Pediatric Traumatic Brain Injury: Review of the Literature. J. Neurotrauma 2015, 32, 1849–1860. [Google Scholar] [CrossRef]
- Babikian, T.; Asarnow, R. Neurocognitive Outcomes and Recovery after Pediatric TBI: Meta-Analytic Review of the Literature. Neuropsychology 2009, 23, 283–296. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Liu, J. The Effect of Pediatric Traumatic Brain Injury on Behavioral Outcomes: A Systematic Review. Dev. Med. Child Neurol. 2013, 55, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Rashid, M.; Goez, H.R.; Mabood, N.; Damanhoury, S.; Yager, J.Y.; Joyce, A.S.; Newton, A.S. The Impact of Pediatric Traumatic Brain Injury (TBI) on Family Functioning: A Systematic Review. J. Pediatr. Rehabil. Med. 2014, 7, 241–254. [Google Scholar] [CrossRef]
- Zemek, R.L.; Farion, K.J.; Sampson, M.; McGahern, C. Prognosticators of Persistent Symptoms Following Pediatric Concussion: A Systematic Review. JAMA Pediatr. 2013, 167, 259. [Google Scholar] [CrossRef]
- Polinder, S.; Cnossen, M.C.; Real, R.G.L.; Covic, A.; Gorbunova, A.; Voormolen, D.C.; Master, C.L.; Haagsma, J.A.; Diaz-Arrastia, R.; von Steinbuechel, N. A Multidimensional Approach to Post-Concussion Symptoms in Mild Traumatic Brain Injury. Front. Neurol. 2018, 9, 1113. [Google Scholar] [CrossRef] [Green Version]
- Carroll, L.; Cassidy, J.D.; Peloso, P.; Borg, J.; von Holst, H.; Holm, L.; Paniak, C.; Pépin, M. Prognosis for Mild Traumatic Brain Injury: Results of the Who Collaborating Centre Task Force on Mild Traumatic Brain Injury. J. Rehabil. Med. 2004, 36, 84–105. [Google Scholar] [CrossRef]
- Ewing-Cobbs, L.; Cox, C.S., Jr.; Clark, A.E.; Holubkov, R.; Keenan, H.T. Persistent Postconcussion Symptoms After Injury. Pediatrics 2018, 142, e20180939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novak, Z.; Aglipay, M.; Barrowman, N.; Yeates, K.O.; Beauchamp, M.H.; Gravel, J.; Freedman, S.B.; Gagnon, I.; Gioia, G.; Boutis, K.; et al. Association of Persistent Postconcussion Symptoms With Pediatric Quality of Life. JAMA Pediatr. 2016, 170, e162900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alla, S.; Sullivan, S.J.; Hale, L.; McCrory, P. Self-Report Scales/Checklists for the Measurement of Concussion Symptoms: A Systematic Review. Br. J. Sport. Med. 2009, 43, i3–i12. [Google Scholar] [CrossRef] [PubMed]
- King, N.S.; Crawford, S.; Wenden, F.J.; Moss, N.E.; Wade, D.T. The Rivermead Post Concussion Symptoms Questionnaire: A Measure of Symptoms Commonly Experienced after Head Injury and Its Reliability. J. Neurol. 1995, 242, 587–592. [Google Scholar] [CrossRef]
- Iverson, G.L.; Gaetz, M. Practical Considerations for Interpreting Change Following Brain Injury. In Traumatic Brain Injury in Sports; Taylor & Francis: London, UK, 2004; pp. 323–356. ISBN 978-0-367-81053-5. [Google Scholar]
- Wilde, E.A.; McCauley, S.R.; Hunter, J.V.; Bigler, E.D.; Chu, Z.; Wang, Z.J.; Hanten, G.R.; Troyanskaya, M.; Yallampalli, R.; Li, X.; et al. Diffusion Tensor Imaging of Acute Mild Traumatic Brain Injury in Adolescents. Neurology 2008, 70, 948–955. [Google Scholar] [CrossRef]
- Gioia, G.A.; Schneider, J.C.; Vaughan, C.G.; Isquith, P.K. Which Symptom Assessments and Approaches Are Uniquely Appropriate for Paediatric Concussion? Br. J. Sport. Med. 2009, 43, i13–i22. [Google Scholar] [CrossRef] [Green Version]
- Barlow, K.M.; Crawford, S.; Stevenson, A.; Sandhu, S.S.; Belanger, F.; Dewey, D. Epidemiology of Postconcussion Syndrome in Pediatric Mild Traumatic Brain Injury. Pediatrics 2010, 126, e374–e381. [Google Scholar] [CrossRef]
- NINDS Project Overview. Available online: https://www.commondataelements.ninds.nih.gov (accessed on 29 March 2022).
- Lovell, M.R.; Iverson, G.L.; Collins, M.W.; Podell, K.; Johnston, K.M.; Pardini, D.; Pardini, J.; Norwig, J.; Maroon, J.C. Measurement of Symptoms Following Sports-Related Concussion: Reliability and Normative Data for the Post-Concussion Scale. Appl. Neuropsychol. 2006, 13, 166–174. [Google Scholar] [CrossRef]
- Sady, M.D.; Vaughan, C.G.; Gioia, G.A. Psychometric Characteristics of the Postconcussion Symptom Inventory in Children and Adolescents. Arch. Clin. Neuropsychol. 2014, 29, 348–363. [Google Scholar] [CrossRef] [Green Version]
- Preiss-Farzanegan, S.J.; Chapman, B.; Wong, T.M.; Wu, J.; Bazarian, J.J. The Relationship Between Gender and Postconcussion Symptoms After Sport-Related Mild Traumatic Brain Injury. PMR 2009, 1, 245–253. [Google Scholar] [CrossRef]
- Steinbuechel, N.; Rauen, K.; Bockhop, F.; Covic, A.; Krenz, U.; Plass, A.; Cunitz, K.; Polinder, S.; Wilson, L.; Steyerberg, E.; et al. Psychometric Characteristics of the Patient-Reported Outcome Measures Applied in the CENTER-TBI Study. J. Clin. Med. 2021, 10, 2396. [Google Scholar] [CrossRef] [PubMed]
- Plass, A.M.; Van Praag, D.; Covic, A.; Gorbunova, A.; Real, R.; Von Steinbüchel, N. The Psychometric Validation of the Dutch Version of the Rivermead Post-Concussion Symptoms Questionnaire (RPQ) after Traumatic Brain Injury (TBI); Scientific Communication and Education: Francisco, CA, USA, 2018. [Google Scholar]
- Teasdale, G.; Jennett, B. Assessment of Coma and Impaired Consciousness. A Practical Scale. Lancet Lond. Engl. 1974, 2, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Mundfrom, D.J.; Shaw, D.G.; Ke, T.L. Minimum Sample Size Recommendations for Conducting Factor Analyses. Int. J. Test. 2005, 5, 159–168. [Google Scholar] [CrossRef]
- Crouchman, M. A Practical Outcome Scale for Paediatric Head Injury. Arch. Dis. Child. 2001, 84, 120–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith-Seemiller, L.; Fow, N.R.; Kant, R.; Franzen, M.D. Presence of Post-Concussion Syndrome Symptoms in Patients with Chronic Pain vs Mild Traumatic Brain Injury. Brain Inj. 2003, 17, 199–206. [Google Scholar] [CrossRef]
- Potter, S.; Leigh, E.; Wade, D.; Fleminger, S. The Rivermead Post Concussion Symptoms Questionnaire: A Confirmatory Factor Analysis. J. Neurol. 2006, 253, 1603–1614. [Google Scholar] [CrossRef]
- Eyres, S.; Carey, A.; Gilworth, G.; Neumann, V.; Tennant, A. Construct Validity and Reliability of the Rivermead Post-Concussion Symptoms Questionnaire. Clin. Rehabil. 2005, 19, 878–887. [Google Scholar] [CrossRef]
- Herrmann, N.; Rapoport, M.J.; Rajaram, R.D.; Chan, F.; Kiss, A.; Ma, A.K.; Feinstein, A.; Mc Cullagh, S.; Lanctôt, K.L. Factor Analysis of the Rivermead Post-Concussion Symptoms Questionnaire in Mild-to-Moderate Traumatic Brain Injury Patients. J. Neuropsychiatry Clin. Neurosci. 2009, 21, 181–188. [Google Scholar] [CrossRef]
- Lannsjö, M.; Borg, J.; Björklund, G.; af Geijerstam, L.; Lundgren-Nilsson, Å. Internal Construct Validity of the Rivermead Post-Concussion Symptoms Questionnaire. J. Rehabil. Med. 2011, 43, 997–1002. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.; Skilbeck, C.; Cannan, P.; Slatyer, M. The Structure of the Rivermead Post-Concussion Symptoms Questionnaire in Australian Adults with Traumatic Brain Injury. Brain Impair. 2018, 19, 166–182. [Google Scholar] [CrossRef]
- Agtarap, S.; Kramer, M.D.; Campbell-Sills, L.; Yuh, E.; Mukherjee, P.; Manley, G.T.; McCrea, M.A.; Dikmen, S.; Giacino, J.T.; Stein, M.B.; et al. Invariance of the Bifactor Structure of Mild Traumatic Brain Injury (MTBI) Symptoms on the Rivermead Postconcussion Symptoms Questionnaire Across Time, Demographic Characteristics, and Clinical Groups: A TRACK-TBI Study. Assessment 2021, 28, 1656–1670. [Google Scholar] [CrossRef] [PubMed]
- Zeldovich, M.; Bockhop, F.; Plass, A.M.; Covic, A.; Mueller, I.; Polinder, S.; Mikolic, A.; van der Vlegel, M.; Steinbuechel, N.; CENTER-TBI participants and investigators. Comparability of the Six Rivermead Post-Concussion Symptoms Questionnaire Translations: Results from the CENTER-TBI Study. PLoS ONE, 2022; in press. [Google Scholar]
- Rivera, D.; Greving, S.; Arango-Lasprilla, J.C. Comparability of (Post-Concussion) Symptoms across Time in Individuals after Traumatic Brain Injury: Results from the Center-Tbi Study. J. Clin. Med. 2022, 11, 4090. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guze, S.B. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Sun, J.; Liang, K.; Chi, X.; Chen, S. Psychometric Properties of the Generalized Anxiety Disorder Scale-7 Item (GAD-7) in a Large Sample of Chinese Adolescents. Healthcare 2021, 9, 1709. [Google Scholar] [CrossRef]
- Tiirikainen, K.; Haravuori, H.; Ranta, K.; Kaltiala-Heino, R.; Marttunen, M. Psychometric Properties of the 7-Item Generalized Anxiety Disorder Scale (GAD-7) in a Large Representative Sample of Finnish Adolescents. Psychiatry Res. 2019, 272, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Gillie, B.L.; Fazio-Sumrok, V.; Eagle, S.R.; Kegel, N.; Trbovich, A.M.; Collins, M.W.; Kontos, A.P. Clinical Predictors of Post-Injury Anxiety in Adolescent Patients Following Concussion. Appl. Neuropsychol. Child 2022, 11, 253–259. [Google Scholar] [CrossRef]
- Wright, B.; Wilmoth, K.; Juengst, S.B.; Didehbani, N.; Maize, R.; Cullum, C.M. Perceived Recovery and Self-Reported Functioning in Adolescents with Mild Traumatic Brain Injury: The Role of Sleep, Mood, and Physical Symptoms. Dev. Neurorehabilit. 2021, 24, 237–243. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A New Depression Diagnostic and Severity Measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Ganguly, S.; Samanta, M.; Roy, P.; Chatterjee, S.; Kaplan, D.W.; Basu, B. Patient Health Questionnaire-9 as an Effective Tool for Screening of Depression Among Indian Adolescents. J. Adolesc. Health 2013, 52, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Tsai, F.-J.; Huang, Y.-H.; Liu, H.-C.; Huang, K.-Y.; Huang, Y.-H.; Liu, S.-I. Patient Health Questionnaire for School-Based Depression Screening Among Chinese Adolescents. Pediatrics 2014, 133, e402–e409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durish, C.L.; Pereverseff, R.S.; Yeates, K.O. Depression and Depressive Symptoms in Pediatric Traumatic Brain Injury: A Scoping Review. J. Head Trauma Rehabil. 2018, 33, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.M.; McCarty, C.A.; Marcynyszyn, L.A.; Zatzick, D.F.; Chrisman, S.P.; Rivara, F.P. Child- Compared with Parent-Report Ratings on Psychosocial Measures Following a Mild Traumatic Brain Injury among Youth with Persistent Post-Concussion Symptoms. Brain Inj. 2021, 35, 574–586. [Google Scholar] [CrossRef] [PubMed]
- Bulmer, M.G. Principles of Statistics; Dover Publications: New York, NY, USA, 1979; ISBN 978-0-486-63760-0. [Google Scholar]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality Criteria Were Proposed for Measurement Properties of Health Status Questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Feißt, M.; Hennigs, A.; Heil, J.; Moosbrugger, H.; Kelava, A.; Stolpner, I.; Kieser, M.; Rauch, G. Refining Scores Based on Patient Reported Outcomes—Statistical and Medical Perspectives. BMC Med. Res. Methodol. 2019, 19, 167. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research. In Methodology in the Social Sciences, 2nd ed.; The Guilford Press: New York, NY, USA; London, UK, 2015; ISBN 978-1-4625-1779-4. [Google Scholar]
- Steiger, J.H. Statistically Based Tests for the Number of Common Factors. In Proceedings of the Annual Meeting of the Psychometric Society, Iowa City, IA, USA, 28 May 1980; 1980. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. Online 2003, 8, 23–27. [Google Scholar]
- Tanveer, S.; Zecavati, N.; Delasobera, E.B.; Oyegbile, T.O. Gender Differences in Concussion and Postinjury Cognitive Findings in an Older and Younger Pediatric Population. Pediatr. Neurol. 2017, 70, 44–49. [Google Scholar] [CrossRef]
- Sigurdardottir, S.; Andelic, N.; Roe, C.; Jerstad, T.; Schanke, A.-K. Post-Concussion Symptoms after Traumatic Brain Injury at 3 and 12 Months Post-Injury: A Prospective Study. Brain Inj. 2009, 23, 489–497. [Google Scholar] [CrossRef]
- Pickering, A.; Grundy, K.; Clarke, A.; Townend, W. A Cohort Study of Outcomes Following Head Injury among Children and Young Adults in Full-Time Education. Emerg. Med. J. 2012, 29, 451–454. [Google Scholar] [CrossRef]
- Brooks, B.L.; Plourde, V.; Beauchamp, M.H.; Tang, K.; Yeates, K.O.; Keightley, M.; Anderson, P.; Désiré, N.; Barrowman, N.; Zemek, R.; et al. Predicting Psychological Distress after Pediatric Concussion. J. Neurotrauma 2019, 36, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Vargha, A.; Delaney, H.D. A Critique and Improvement of the CL Common Language Effect Size Statistics of McGraw and Wong. J. Educ. Behav. Stat. 2000, 25, 101–132. [Google Scholar] [CrossRef]
- Cicchetti, D.V. Guidelines, Criteria, and Rules of Thumb for Evaluating Normed and Standardized Assessment Instruments in Psychology. Psychol. Assess. 1994, 6, 284. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Revelle, W. Psych: Procedures for Personality and Psychological Research. 2019. Available online: https://www.scholars.northwestern.edu/en/publications/psych-procedures-for-personality-and-psychological-research (accessed on 22 December 2022).
- Kirkwood, M.W.; Peterson, R.L.; Connery, A.K.; Baker, D.A.; Grubenhoff, J.A. Postconcussive Symptom Exaggeration After Pediatric Mild Traumatic Brain Injury. Pediatrics 2014, 133, 643–650. [Google Scholar] [CrossRef]
- Sroufe, N.S.; Fuller, D.S.; West, B.T.; Singal, B.M.; Warschausky, S.A.; Maio, R.F. Postconcussive Symptoms and Neurocognitive Function After Mild Traumatic Brain Injury in Children. Pediatrics 2010, 125, e1331–e1339. [Google Scholar] [CrossRef]
- Barker-Collo, S.; Theadom, A.; Starkey, N.; Kahan, M.; Jones, K.; Feigin, V. Factor Structure of the Rivermead Post-Concussion Symptoms Questionnaire over the First Year Following Mild Traumatic Brain Injury. Brain Inj. 2018, 32, 453–458. [Google Scholar] [CrossRef]
- Lundin, A.; de Boussard, C.; Edman, G.; Borg, J. Symptoms and Disability until 3 Months after Mild TBI. Brain Inj. 2006, 20, 799–806. [Google Scholar] [CrossRef]
- Lovell, M.R.; Collins, M.W. Neuropsychological Assessment of the College Football Player. J. Head Trauma Rehabil. 1998, 13, 9–26. [Google Scholar] [CrossRef]
- Broshek, D.K.; Marco, A.P.D.; Freeman, J.R. A Review of Post-Concussion Syndrome and Psychological Factors Associated with Concussion. Brain Inj. 2015, 29, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Styrke, J.; Sojka, P.; Björnstig, U.; Bylund, P.; Stålnacke, B. Sex-Differences in Symptoms, Disability, and Life Satisfaction Three Years after Mild Traumatic Brain Injury: A Population-Based Cohort Study. J. Rehabil. Med. 2013, 45, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Mikolic, A.; Groeniger, J.O.; Zeldovich, M.; Wilson, L.; van Lennep, J.R.; van Klaveren, D.; Polinder, S.; Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) Participants and Investigators; Åkerlund, C.; Amrein, K.; et al. Explaining Outcome Differences between Men and Women Following Mild Traumatic Brain Injury. J. Neurotrauma 2021, 38, 3315–3331. [Google Scholar] [CrossRef] [PubMed]
- Dikmen, S.S.; Corrigan, J.D.; Levin, H.S.; Machamer, J.; Stiers, W.; Weisskopf, M.G. Cognitive Outcome Following Traumatic Brain Injury. J. Head Trauma Rehabil. 2009, 24, 430–438. [Google Scholar] [CrossRef]
- Ponsford, J.; Nguyen, S.; Downing, M.; Bosch, M.; McKenzie, J.; Turner, S.; Chau, M.; Mortimer, D.; Gruen, R.; Knott, J.; et al. Factors Associated with Persistent Post-Concussion Symptoms Following Mild Traumatic Brain Injury in Adults. J. Rehabil. Med. 2019, 51, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.; Mason, S.; Lecky, F.; Dawson, J. Prevalence of Depression after TBI in a Prospective Cohort: The SHEFBIT Study. Brain Inj. 2018, 32, 84–90. [Google Scholar] [CrossRef]
- Di Battista, A.; Soo, C.; Catroppa, C.; Anderson, V. Quality of Life in Children and Adolescents Post-TBI: A Systematic Review and Meta-Analysis. J. Neurotrauma 2012, 29, 1717–1727. [Google Scholar] [CrossRef]
- Kim, C.; Choi, H.; Ko, H.; Park, C.G. Agreement Between Parent Proxy Reports and Self-Reports of Adolescent Emotional Distress. J. Sch. Nurs. 2020, 36, 104–111. [Google Scholar] [CrossRef]
- Erickson, S.J.; Krapf, E.M.; Gerstle, M. Adolescent Cancer Survivors’ Posttraumatic Stress Symptoms: Concordance between Self-Report and Maternal-Proxy Report. J. Health Psychol. 2017, 22, 1789–1798. [Google Scholar] [CrossRef]
- Green, L.; Godfrey, C.; Soo, C.; Anderson, V.; Catroppa, C. Agreement between Parent-adolescent Ratings on Psychosocial Outcome and Quality-of-life Following Childhood Traumatic Brain Injury. Dev. Neurorehabilit. 2012, 15, 105–113. [Google Scholar] [CrossRef]
- Cohen, L.L.; Vowles, K.E.; Eccleston, C. Adolescent Chronic Pain-Related Functioning: Concordance and Discordance of Mother-Proxy and Self-Report Ratings. Eur. J. Pain Lond. Engl. 2010, 14, 882–886. [Google Scholar] [CrossRef] [PubMed]
- Hajek, C.A.; Yeates, K.O.; Taylor, H.G.; Bangert, B.; Dietrich, A.; Nuss, K.E.; Rusin, J.; Wright, M. Agreement between Parents and Children on Ratings of Post-Concussive Symptoms Following Mild Traumatic Brain Injury. Child Neuropsychol. 2010, 17, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Mollayeva, T.; Kendzerska, T.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A.; Cassidy, J.D. A Systematic Review of Fatigue in Patients with Traumatic Brain Injury: The Course, Predictors and Consequences. Neurosci. Biobehav. Rev. 2014, 47, 684–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blinman, T.A.; Houseknecht, E.; Snyder, C.; Wiebe, D.J.; Nance, M.L. Postconcussive Symptoms in Hospitalized Pediatric Patients after Mild Traumatic Brain Injury. J. Pediatr. Surg. 2009, 44, 1223–1228. [Google Scholar] [CrossRef] [PubMed]
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and Cognitive Impairment in Post-COVID-19 Syndrome: A Systematic Review and Meta-Analysis. Brain. Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef] [PubMed]
- Lynn Snow, A.; Cook, K.F.; Lin, P.-S.; Morgan, R.O.; Magaziner, J. Proxies and Other External Raters: Methodological Considerations. Health Serv. Res. 2005, 40, 1676–1693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapin, B.; Thompson, N.; Schuster, A.; Katzan, I.L. Optimal Methods for Reducing Proxy-Introduced Bias on Patient-Reported Outcome Measurements for Group-Level Analyses. Circ. Cardiovasc. Qual. Outcomes 2021, 14, e007960. [Google Scholar] [CrossRef]
- Barry, A.E.; Chaney, B.; Piazza-Gardner, A.K.; Chavarria, E.A. Validity and Reliability Reporting Practices in the Field of Health Education and Behavior: A Review of Seven Journals. Health Educ. Behav. 2014, 41, 12–18. [Google Scholar] [CrossRef]
- Jensen, M.P. Questionnaire Validation: A Brief Guide for Readers of the Research Literature. Clin. J. Pain 2003, 19, 345–352. [Google Scholar] [CrossRef]
- Rosema, S.; Crowe, L.; Anderson, V. Social Function in Children and Adolescents after Traumatic Brain Injury: A Systematic Review 1989–2011. J. Neurotrauma 2012, 29, 1277–1291. [Google Scholar] [CrossRef]
- Yeates, K.O. Mild Traumatic Brain Injury and Postconcussive Symptoms in Children and Adolescents. J. Int. Neuropsychol. Soc. 2010, 16, 953–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helsel, W.J.; Matson, J.L. The Assessment of Depression in Children: The Internal Structure of the Child Depression Inventory (CDI). Behav. Res. Ther. 1984, 22, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Chorpita, B.F.; Tracey, S.A.; Brown, T.A.; Collica, T.J.; Barlow, D.H. Assessment of Worry in Children and Adolescents: An Adaptation of the Penn State Worry Questionnaire. Behav. Res. Ther. 1997, 35, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Ferdinand, R.F. Validity of the CBCL/YSR DSM-IV Scales Anxiety Problems and Affective Problems. J. Anxiety Disord. 2008, 22, 126–134. [Google Scholar] [CrossRef]
- Upton, P.; Lawford, J.; Eiser, C. Parent–Child Agreement across Child Health-Related Quality of Life Instruments: A Review of the Literature. Qual. Life Res. 2008, 17, 895–913. [Google Scholar] [CrossRef] [PubMed]
- Iverson, G.L.; Lange, R.T. Examination of “Postconcussion-Like” Symptoms in a Healthy Sample. Appl. Neuropsychol. 2003, 10, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Voormolen, D.C.; Cnossen, M.C.; Polinder, S.; Gravesteijn, B.Y.; Von Steinbuechel, N.; Real, R.G.L.; Haagsma, J.A. Prevalence of Post-Concussion-like Symptoms in the General Population in Italy, The Netherlands and the United Kingdom. Brain Inj. 2019, 33, 1078–1086. [Google Scholar] [CrossRef] [Green Version]
- Cnossen, M.C.; Winkler, E.A.; Yue, J.K.; Okonkwo, D.O.; Valadka, A.B.; Steyerberg, E.W.; Lingsma, H.F.; Manley, G.T.; The TRACK-TBI Investigators. Development of a Prediction Model for Post-Concussive Symptoms Following Mild Traumatic Brain Injury: A TRACK-TBI Pilot Study. J. Neurotrauma 2017, 34, 2396–2409. [Google Scholar] [CrossRef]
- Matza, L.S.; Swensen, A.R.; Flood, E.M.; Secnik, K.; Leidy, N.K. Assessment of Health-Related Quality of Life in Children: A Review of Conceptual, Methodological, and Regulatory Issues. Value Health 2004, 7, 79–92. [Google Scholar] [CrossRef] [Green Version]
- Starkey, N.J.; Jones, K.; Case, R.; Theadom, A.; Barker-Collo, S.; Feigin, V. Post-Concussive Symptoms after a Mild Traumatic Brain Injury during Childhood and Adolescence. Brain Inj. 2018, 32, 617–626. [Google Scholar] [CrossRef]


| Variable | Group/Values | Adolescents (n = 148) | Proxies (n =147) |
|---|---|---|---|
| Gender † | Female | 62 (42%) | 121 (82%) |
| Male | 85 (57%) | 26 (18%) | |
| Diverse | 1 (1%) | 0 (0%) | |
| Missing | 0 (0%) | 1 (1%) | |
| Age | M (SD) | 15.24 (1.47) | 47.97 (5.64) |
| Min–Max | 13.00–17.92 | 35.00–70.00 | |
| TBI severity † | Mild | 109 (74%) | - |
| Moderate | 9 (6%) | - | |
| Severe | 30 (20%) | - | |
| Presence of lesions † | No lesions | 100 (68%) | - |
| At least one lesion | 43 (29%) | - | |
| Missing | 5 (3%) | - | |
| Years since injury † | <1 | 3 (2%) | - |
| 1–<2 | 20 (14%) | - | |
| 2–<4 | 36 (24%) | - | |
| 4–10 | 88 (59%) | - | |
| Missing | 1 (13%) | - | |
| KOSCHI Score † | 3a (lower severe disability) | 0 (0%) | - |
| 3b | 0 (0%) | - | |
| 4a | 5 (3%) | - | |
| 4b | 18 (12%) | - | |
| 5a | 25 (17%) | - | |
| 5b (full recovery) | 100 (68%) | - |
| Source | RPQ | PCSI-SR13 | GAD-7 | PHQ-9 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C | S | E | Total | C | P | E | F | Total | Total | Total | ||
| Self-report | n | 145 | 145 | 145 | 145 | 123 | 123 | 123 | 123 | 123 | 143 | 143 |
| M | 2.13 | 3.79 | 2.25 | 8.17 | 5.63 | 6.18 | 5.02 | 3.22 | 16.82 | 3.43 | 4.7 | |
| SD | 3.03 | 5.22 | 3.43 | 9.96 | 5.47 | 6.66 | 5.52 | 3.52 | 15.39 | 3.57 | 4.19 | |
| Mdn | 0 | 2 | 0 | 4 | 4 | 4 | 3 | 3 | 12 | 2 | 4 | |
| W | 0.74 | 0.75 | 0.71 | 0.80 | 0.85 | 0.82 | 0.83 | 0.82 | 0.86 | 0.82 | 0.88 | |
| Proxy assessment | n | 145 | 145 | 145 | 145 | 122 | 122 | 122 | 121 | 122 | 143 | 143 |
| M | 2.29 | 3.57 | 1.84 | 7.7 | 3.3 | 3.75 | 3.34 | 2.04 | 10.38 | 3.44 | 4.71 | |
| SD | 3.29 | 5.49 | 3.31 | 10.25 | 5.07 | 5.88 | 4.8 | 3.44 | 13.55 | 3.58 | 4.22 | |
| Mdn | 0 | 0 | 0 | 2 | 1 | 2 | 1 | 0 | 6 | 2 | 4 | |
| W | 0.73 | 0.70 | 0.63 | 0.77 | 0.70 | 0.69 | 0.73 | 0.65 | 0.76 | 0.82 | 0.88 | |
| Source | Scale | Cronbach’s α | Cronbach’s α When Item Omitted | McDonald’s ω | Corrected Item-Total Correlation Range | Correlations | ||
|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | ||||||
| Self-report | (1) Cognitive | 0.84 | 0.74–0.83 | 0.84 | 0.70–0.81 | 1 | – | – |
| (2) Somatic | 0.82 | 0.79–0.83 | 0.82 | 0.34–0.73 | 0.57 | 1 | – | |
| (3) Emotional | 0.81 | 0.72–0.79 | 0.82 | 0.67–0.80 | 0.62 | 0.64 | 1 | |
| (4) Total score | 0.90 | 0.89–0.90 | 0.93 | 0.40–0.76 | 0.80 | 0.91 | 0.86 | |
| (1) | (2) | (3) | ||||||
| Proxy assessment | (1) Cognitive | 0.90 | 0.82–0.92 | 0.91 | 0.77–0.91 | 1 | – | – |
| (2) Somatic | 0.86 | 0.83–0.87 | 0.86 | 0.37–0.76 | 0.56 | 1 | – | |
| (3) Emotional | 0.83 | 0.71–0.84 | 0.84 | 0.59–0.89 | 0.60 | 0.61 | 1 | |
| (4) Total score | 0.91 | 0.90–0.92 | 0.95 | 0.30–0.76 | 0.80 | 0.91 | 0.83 | |
| Confirmatory Factor Analyses (CFA) | Model Comparison | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Source | Model | χ2 | df | χ2/df | p | CFI | TLI | RMSEA | CI90% | SRMR | ∆χ2 (∆df) | p |
| Self-report | One factor | 225.89 | 104 | 2.50 | <0.001 | 0.98 | 0.98 | 0.09 | [0.07, 0.11] | 0.1 | 49.05 (3) | <0.001 |
| Three factors | 141.04 | 101 | 1.86 | 0.005 | 0.99 | 1.00 | 0.05 | [0.03, 0.07] | 0.09 | – | – | |
| Proxy assessment | One factor | 475.72 | 104 | 4.14 | <0.001 | 0.96 | 0.96 | 0.16 | [0.14, 0.17] | 0.16 | 89.68 (3) | <0.001 |
| Three factors | 209.72 | 101 | 2.40 | <0.001 | 0.99 | 0.99 | 0.08 | [0.07, 0.10] | 0.12 | – | – | |
| Source | n | Total (RPQ, PCSI) | Somatic (RPQ), Physical (PCSI) | Emotional (RPQ, PCSI) | Cognitive (RPQ, PCSI) |
|---|---|---|---|---|---|
| Self-report | 123 | 0.80 | 0.70 | 0.70 | 0.71 |
| Proxy assessment | 121 | 0.75 | 0.57 | 0.64 | 0.71 |
| Source | PROM | Total | Somatic | Emotional | Cognitive |
|---|---|---|---|---|---|
| Self-report | GAD-7 | 0.36 | 0.34 | 0.38 | 0.25 |
| PHQ-9 | 0.35 | 0.31 | 0.33 | 0.30 | |
| Proxy assessment | GAD-7 | 0.53 | 0.37 | 0.59 | 0.42 |
| PHQ-9 | 0.62 | 0.48 | 0.57 | 0.52 |
| Variable | Scale | Group | n | M | Md | Cliff’s δ | W | p |
|---|---|---|---|---|---|---|---|---|
| Sex | Total score | Male | 83 | 6.41 | 3 | −0.19 | 2044 | 0.022 |
| Female | 61 | 10.54 | 8 | |||||
| Cognitive | Male | 83 | 1.82 | 0 | −0.13 | 2214.5 | 0.077 ☨ | |
| Female | 61 | 2.59 | 0 | |||||
| Emotional | Male | 83 | 1.55 | 0 | −0.23 | 1953 | 0.005☨ | |
| Female | 61 | 3.23 | 2 | |||||
| Somatic | Male | 83 | 3.04 | 2 | −0.15 | 2156.5 | 0.055 ☨ | |
| Female | 61 | 4.72 | 2 | |||||
| TBI severity | Total score | Mild | 107 | 7.80 | 4 | −0.12 | 1795 | 0.137 |
| Moderate—Severe | 38 | 9.18 | 6 | |||||
| Cognitive | Mild | 107 | 1.69 | 0 | −0.28 | 1473.5 | 0.003☨ | |
| Moderate—Severe | 38 | 3.37 | 3 | |||||
| Emotional | Mild | 107 | 2.24 | 0 | −0.02 | 1994 | 0.424 ☨ | |
| Moderate—Severe | 38 | 2.26 | 0 | |||||
| Somatic | Mild | 107 | 3.87 | 2 | −0.04 | 1961 | 0.368 ☨ | |
| Moderate—Severe | 38 | 3.55 | 2 | |||||
| KOSCHI score | Total score | 5b | 123 | 5.09 | 4 | −1.02 | 1534.5 | <0.001 |
| <5b | 22 | 13.15 | 12.5 | |||||
| Cognitive | 5b | 123 | 1.48 | 0 | −1.15 | 1703 | 0.002☨ | |
| <5b | 22 | 3.98 | 3.5 | |||||
| Emotional | 5b | 123 | 1.26 | 0 | −0.60 | 1718.5 | 0.003☨ | |
| <5b | 22 | 3.06 | 2.5 | |||||
| Somatic | 5b | 123 | 2.36 | 2 | −0.83 | 1505.5 | <0.001☨ | |
| <5b | 22 | 6.11 | 3.5 | |||||
| GAD-7 | Total score | <5 | 110 | 5.57 | 2 | −1.10 | 1034.5 | <0.001 |
| ≥5 | 37 | 15.26 | 14 | |||||
| Cognitive | <5 | 110 | 1.45 | 0 | −0.97 | 1120.5 | <0.001☨ | |
| ≥5 | 37 | 4.17 | 5 | |||||
| Emotional | <5 | 110 | 1.44 | 0 | −1.00 | 1090 | <0.001☨ | |
| ≥5 | 37 | 4.54 | 3 | |||||
| Somatic | <5 | 110 | 2.68 | 0 | −0.82 | 1180.5 | <0.001☨ | |
| ≥5 | 37 | 6.54 | 5 | |||||
| PHQ-9 | Total score | <5 | 89 | 5.45 | 2 | −0.69 | 1619 | <0.001 |
| ≥5 | 58 | 11.82 | 9 | |||||
| Cognitive | <5 | 89 | 1.38 | 0 | −0.65 | 1769 | 0.001☨ | |
| ≥5 | 58 | 3.27 | 2 | |||||
| Emotional | <5 | 89 | 1.41 | 0 | −0.62 | 1651 | <0.001☨ | |
| ≥5 | 58 | 3.43 | 2 | |||||
| Somatic | <5 | 89 | 2.66 | 0 | −0.51 | 1785.5 | 0.002☨ | |
| ≥5 | 58 | 5.12 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bockhop, F.; Zeldovich, M.; Greving, S.; Krenz, U.; Cunitz, K.; Timmermann, D.; Bonke, E.M.; Bonfert, M.V.; Koerte, I.K.; Kieslich, M.; et al. Psychometric Properties of the German Version of the Rivermead Post-Concussion Symptoms Questionnaire in Adolescents after Traumatic Brain Injury and Their Proxies. J. Clin. Med. 2023, 12, 319. https://doi.org/10.3390/jcm12010319
Bockhop F, Zeldovich M, Greving S, Krenz U, Cunitz K, Timmermann D, Bonke EM, Bonfert MV, Koerte IK, Kieslich M, et al. Psychometric Properties of the German Version of the Rivermead Post-Concussion Symptoms Questionnaire in Adolescents after Traumatic Brain Injury and Their Proxies. Journal of Clinical Medicine. 2023; 12(1):319. https://doi.org/10.3390/jcm12010319
Chicago/Turabian StyleBockhop, Fabian, Marina Zeldovich, Sven Greving, Ugne Krenz, Katrin Cunitz, Dagmar Timmermann, Elena M. Bonke, Michaela V. Bonfert, Inga K. Koerte, Matthias Kieslich, and et al. 2023. "Psychometric Properties of the German Version of the Rivermead Post-Concussion Symptoms Questionnaire in Adolescents after Traumatic Brain Injury and Their Proxies" Journal of Clinical Medicine 12, no. 1: 319. https://doi.org/10.3390/jcm12010319