

Association of Depressive and Somatic Symptoms with Heart Rate Variability in Patients with Traumatic Brain Injury

Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Beck Depression Inventory-II
2.3. The Patient Health Questionnaire-15
2.4. Heart Rate Variability
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Comparison of the HRV Parameters between Subgroups Classified by Depression Severity
3.3. Comparison of the HRV Parameters between Subgroups Classified by Somatic Symptoms Severity
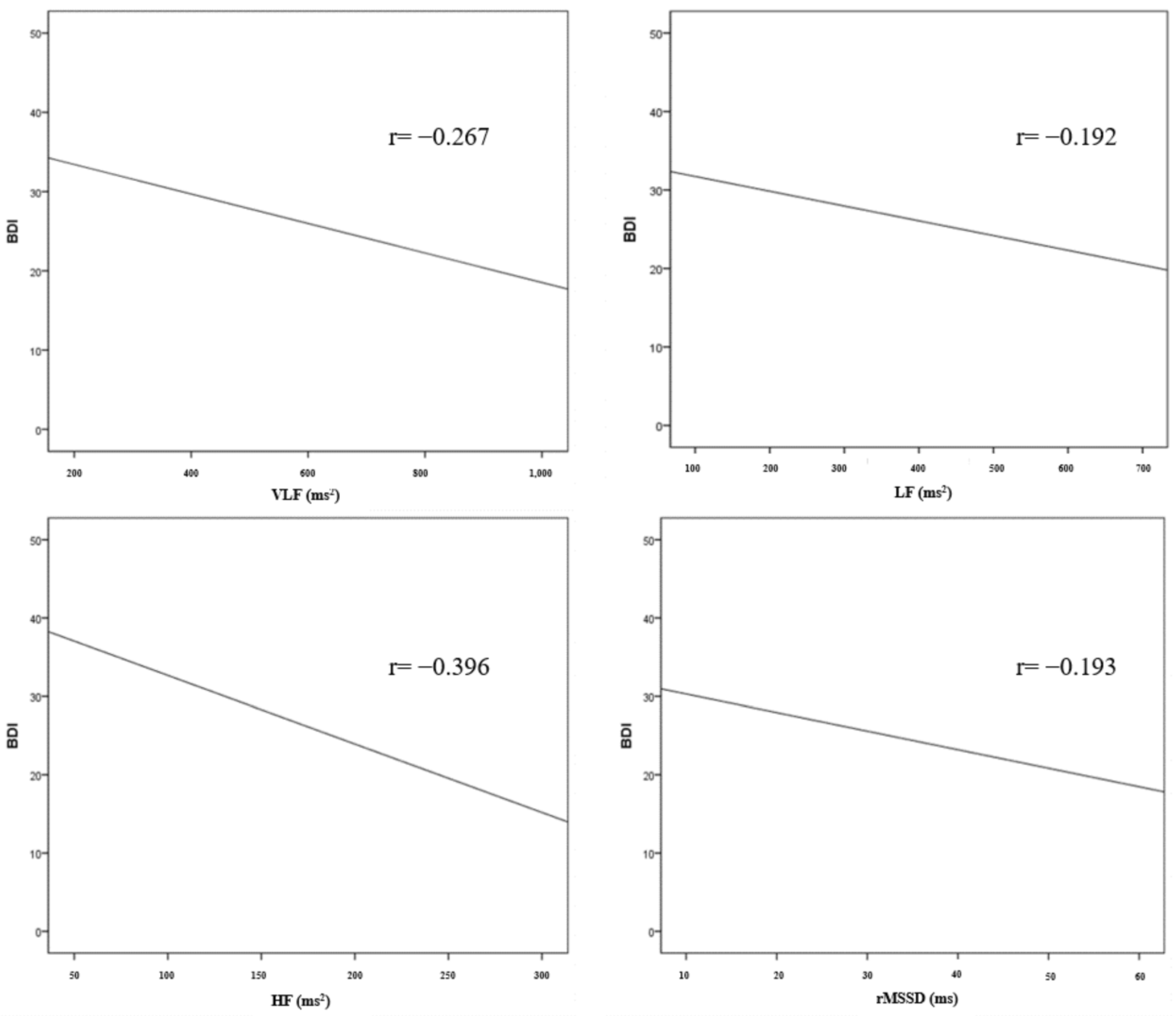
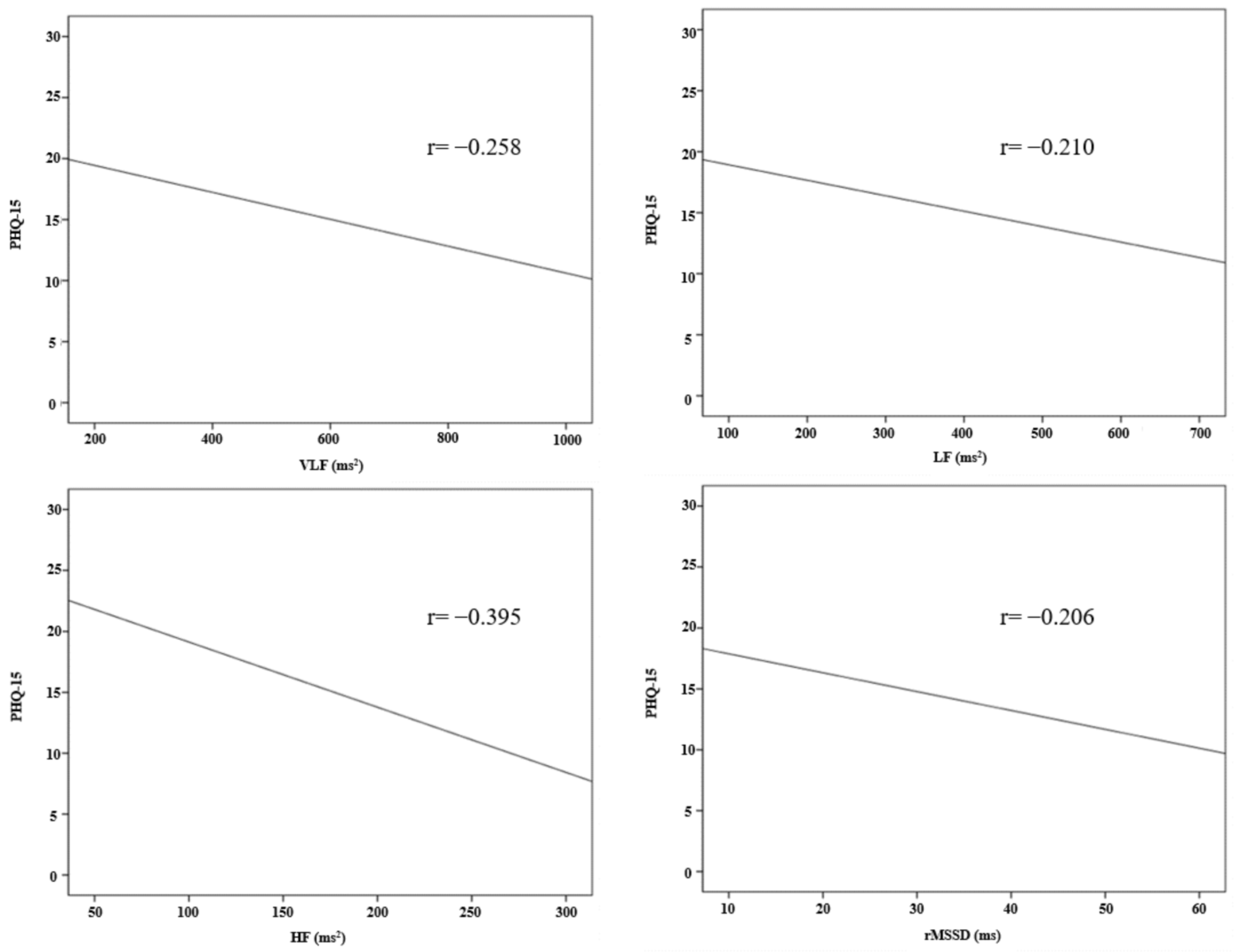
3.4. Correlation between HRV Parameters and Depression and Somatic Symptoms Severity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, R.; Mason, S.; Lecky, F.; Dawson, J. Prevalence of depression after tbi in a prospective cohort: The shefbit study. Brain Inj. 2018, 32, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Kim, E.Y.; Sun, J.; Kim, H.K.; Lee, Y.S.; Oh, B.M.; Park, H.Y.; Leigh, J.H. Incidence of depression after traumatic brain injury: A nationwide longitudinal study of 2.2 million adults. J. Neurotrauma 2022, 39, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Roy, D.; Koliatsos, V.; Vaishnavi, S.; Han, D.; Rao, V. Risk factors for new-onset depression after first-time traumatic brain injury. Psychosomatics 2018, 59, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Lallukka, T.; Mekuria, G.B.; Nummi, T.; Virtanen, P.; Virtanen, M.; Hammarström, A. Co-occurrence of depressive, anxiety, and somatic symptoms: Trajectories from adolescence to midlife using group-based joint trajectory analysis. BMC Psychiatry 2019, 19, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grauwmeijer, E.; Heijenbrok-Kal, M.H.; Peppel, L.D.; Hartjes, C.J.; Haitsma, I.K.; de Koning, I.; Ribbers, G.M. Cognition, health-related quality of life, and depression ten years after moderate to severe traumatic brain injury: A prospective cohort study. J. Neurotrauma 2018, 35, 1543–1551. [Google Scholar] [CrossRef]
- Rossom, R.C.; Peterson, E.L.; Chawa, M.S.; Prabhakar, D.; Hu, Y.; Yeh, H.H.; Owen-Smith, A.A.; Simon, G.E.; Williams, L.K.; Hubley, S.; et al. Understanding tbi as a risk factor versus a means of suicide death using electronic health record data. Arch. Suicide Res. 2022, 1–14. [Google Scholar] [CrossRef]
- Hicks, A.J.; Clay, F.J.; James, A.C.; Hopwood, M.; Ponsford, J.L. Effectiveness of pharmacotherapy for depression after adult traumatic brain injury: An umbrella review. Neuropsychol. Rev. 2022. [Google Scholar] [CrossRef]
- Juengst, S.B.; Kumar, R.G.; Wagner, A.K. A narrative literature review of depression following traumatic brain injury: Prevalence, impact, and management challenges. Psychol. Res. Behav. Manag. 2017, 10, 175–186. [Google Scholar] [CrossRef] [Green Version]
- Mostafa Alim, S.; Ahmed, M.N.; Mullick, M.S.I.; Chowdhury, N.F.; Akhter, F.; Alam, M.S. Validation of the bangla version of beck depression inventory-ii. Brain Behav. 2020, 10, e01563. [Google Scholar] [CrossRef] [Green Version]
- van Driel, T.J.W.; Hilderink, P.H.; Hanssen, D.J.C.; de Boer, P.; Rosmalen, J.G.M.; Oude Voshaar, R.C. Assessment of somatization and medically unexplained symptoms in later life. Assessment 2018, 25, 374–393. [Google Scholar] [CrossRef]
- Weil, Z.M.; White, B.; Whitehead, B.; Karelina, K. The role of the stress system in recovery after traumatic brain injury: A tribute to bruce s. Mcewen. Neurobiol. Stress 2022, 19, 100467. [Google Scholar] [CrossRef] [PubMed]
- Green, K.; Cairncross, M.; Panenka, W.J.; Stubbs, J.L.; Silverberg, N.D. History of functional somatic syndromes and persistent symptoms after mild traumatic brain injury. J. Neuropsychiatry Clin. Neurosci. 2021, 33, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Toussaint, A.; Hüsing, P.; Kohlmann, S.; Löwe, B. Detecting dsm-5 somatic symptom disorder: Criterion validity of the patient health questionnaire-15 (phq-15) and the somatic symptom scale-8 (sss-8) in combination with the somatic symptom disorder—B criteria scale (ssd-12). Psychol. Med. 2020, 50, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Leonhart, R.; de Vroege, L.; Zhang, L.; Liu, Y.; Dong, Z.; Schaefert, R.; Nolte, S.; Fischer, F.; Fritzsche, K.; van der Feltz-Cornelis, C.M. Comparison of the factor structure of the patient health questionnaire for somatic symptoms (phq-15) in germany, the netherlands, and china. A transcultural structural equation modeling (sem) study. Front. Psychiatry 2018, 9, 240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenza, G.; Citi, L.; Saul, J.P.; Barbieri, R. Measures of sympathetic and parasympathetic autonomic outflow from heartbeat dynamics. J. Appl. Physiol. 2018, 125, 19–39. [Google Scholar] [CrossRef] [PubMed]
- Chuangchai, W.; Pothisiri, W.; Chanbenjapipu, P. Variation of autonomic nervous system function by age and gender in thai ischemic stroke patients. Brain Sci. 2021, 11, 380. [Google Scholar] [CrossRef]
- Lees, T.; Shad-Kaneez, F.; Simpson, A.M.; Nassif, N.T.; Lin, Y.; Lal, S. Heart rate variability as a biomarker for predicting stroke, post-stroke complications and functionality. Biomark. Insights 2018, 13, 1177271918786931. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.S.; El Ghormli, L.; Vajravelu, M.E.; Bacha, F.; Farrell, R.M.; Gidding, S.S.; Levitt Katz, L.E.; Tryggestad, J.B.; White, N.H.; Urbina, E.M. Heart rate variability and cardiac autonomic dysfunction: Prevalence, risk factors, and relationship to arterial stiffness in the treatment options for type 2 diabetes in adolescents and youth (today) study. Diabetes Care 2019, 42, 2143–2150. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Yu, Y.; Zou, W.; Zhang, M.; Wang, Y.; Gu, Y. Association between cardiac autonomic nervous dysfunction and the severity of coronary lesions in patients with stable coronary artery disease. J. Int. Med. Res. 2018, 46, 3729–3740. [Google Scholar] [CrossRef] [Green Version]
- Sessa, F.; Anna, V.; Messina, G.; Cibelli, G.; Monda, V.; Marsala, G.; Ruberto, M.; Biondi, A.; Cascio, O.; Bertozzi, G.; et al. Heart rate variability as predictive factor for sudden cardiac death. Aging 2018, 10, 166–177. [Google Scholar] [CrossRef]
- Chang, Y.M.; Huang, Y.T.; Chen, I.L.; Yang, C.L.; Leu, S.C.; Su, H.L.; Kao, J.L.; Tsai, S.C.; Jhen, R.N.; Shiao, C.C. Heart rate variability as an independent predictor for 8-year mortality among chronic hemodialysis patients. Sci. Rep. 2020, 10, 881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherbakov, N.; Barkhudaryan, A.; Ebner, N.; von Haehling, S.; Anker, S.D.; Joebges, M.; Doehner, W. Early rehabilitation after stroke: Relationship between the heart rate variability and functional outcome. ESC Heart Fail. 2020, 7, 2983–2991. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.Y.; Huang, A.P.; Kuo, L.T. Prognostic value of variables derived from heart rate variability in patients with traumatic brain injury after decompressive surgery. PLoS ONE 2021, 16, e0245792. [Google Scholar] [CrossRef] [PubMed]
- Leipzig, T.J.; Lowensohn, R.I. Heart rate variability in neurosurgical patients. Neurosurgery 1986, 19, 356–362. [Google Scholar] [CrossRef]
- Hartmann, R.; Schmidt, F.M.; Sander, C.; Hegerl, U. Heart rate variability as indicator of clinical state in depression. Front. Psychiatry 2018, 9, 735. [Google Scholar] [CrossRef] [Green Version]
- Ying-Chih, C.; Yu-Chen, H.; Wei-Lieh, H. Heart rate variability in patients with somatic symptom disorders and functional somatic syndromes: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2020, 112, 336–344. [Google Scholar] [CrossRef]
- Solem, S.; Kennair, L.E.O.; Hagen, R.; Havnen, A.; Nordahl, H.M.; Wells, A.; Hjemdal, O. Metacognitive therapy for depression: A 3-year follow-up study assessing recovery, relapse, work force participation, and quality of life. Front. Psychol. 2019, 10, 2908. [Google Scholar] [CrossRef] [Green Version]
- Parrish, J.M.; Jenkins, N.W.; Massel, D.H.; Rush, A.J., 3rd; Parrish, M.S.; Hrynewycz, N.M.; Brundage, T.S.; Van Horn, R.; Singh, K. The perioperative symptom severity of higher patient health questionnaire-9 scores between genders in single-level lumbar fusion. Int. J. Spine Surg. 2021, 15, 62–73. [Google Scholar] [CrossRef]
- García-Batista, Z.E.; Guerra-Peña, K.; Cano-Vindel, A.; Herrera-Martínez, S.X.; Medrano, L.A. Validity and reliability of the beck depression inventory (bdi-ii) in general and hospital population of dominican republic. PLoS ONE 2018, 13, e0199750. [Google Scholar] [CrossRef]
- Meyfroidt, G.; Baguley, I.J.; Menon, D.K. Paroxysmal sympathetic hyperactivity: The storm after acute brain injury. Lancet. Neurol. 2017, 16, 721–729. [Google Scholar] [CrossRef]
- Lee, H.; Jeon, S.B.; Lee, K.S. Continuous heart rate variability and electroencephalography monitoring in severe acute brain injury: A preliminary study. Acute Crit. Care 2021, 36, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Fedriga, M.; Czigler, A.; Nasr, N.; Zeiler, F.A.; Park, S.; Donnelly, J.; Papaioannou, V.; Frisvold, S.K.; Wolf, S.; Rasulo, F.; et al. Autonomic nervous system activity during refractory rise in intracranial pressure. J. Neurotrauma 2021, 38, 1662–1669. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.I.; Ropper, A.H.; Zuñiga, G. Acute intracranial lesions and respiratory sinus arrhythmia. Arch Neurol. 1992, 49, 1200–1203. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.J. The cardiac autonomic nervous system: An introduction. Herzschrittmachertherapie Elektrophysiologie 2021, 32, 295–301. [Google Scholar] [CrossRef]
- Li, Y.L. Stellate ganglia and cardiac sympathetic overactivation in heart failure. Int. J. Mol. Sci. 2022, 23, 13311. [Google Scholar] [CrossRef]
- Cattaneo, L.A.; Franquillo, A.C.; Grecucci, A.; Beccia, L.; Caretti, V.; Dadomo, H. Is low heart rate variability associated with emotional dysregulation, psychopathological dimensions, and prefrontal dysfunctions? An integrative view. J. Pers. Med. 2021, 11, 872. [Google Scholar] [CrossRef]
- Pinter, A.; Szatmari, S., Jr.; Horvath, T.; Penzlin, A.I.; Barlinn, K.; Siepmann, M.; Siepmann, T. Cardiac dysautonomia in depression—Heart rate variability biofeedback as a potential add-on therapy. Neuropsychiatr. Dis. Treat. 2019, 15, 1287–1310. [Google Scholar] [CrossRef] [Green Version]
- Kemp, A.H.; Koenig, J.; Thayer, J.F. From psychological moments to mortality: A multidisciplinary synthesis on heart rate variability spanning the continuum of time. Neurosci. Biobehav. Rev. 2017, 83, 547–567. [Google Scholar] [CrossRef] [Green Version]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart rate variability and cardiac vagal tone in psychophysiological research—Recommendations for experiment planning, data analysis, and data reporting. Front. Psychol. 2017, 8, 213. [Google Scholar] [CrossRef] [Green Version]
- O’Reardon, J.P.; Cristancho, P.; Peshek, A.D. Vagus nerve stimulation (vns) and treatment of depression: To the brainstem and beyond. Psychiatry 2006, 3, 54–63. [Google Scholar]
- Austelle, C.W.; O’Leary, G.H.; Thompson, S.; Gruber, E.; Kahn, A.; Manett, A.J.; Short, B.; Badran, B.W. A comprehensive review of vagus nerve stimulation for depression. Neuromodulation J. Int. Neuromodulation Soc. 2022, 25, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Shah, A.; Su, S.; Goldberg, J.; Lampert, R.J.; Levantsevych, O.M.; Shallenberger, L.; Pimple, P.; Bremner, J.D.; Vaccarino, V. Association of depressive symptoms and heart rate variability in vietnam war-era twins: A longitudinal twin difference study. JAMA Psychiatry 2018, 75, 705–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okur Güney, Z.E.; Sattel, H.; Witthöft, M.; Henningsen, P. Emotion regulation in patients with somatic symptom and related disorders: A systematic review. PLoS ONE 2019, 14, e0217277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, W.-L.; Liao, S.-C.; Yang, C.C.H.; Kuo, T.B.J.; Chen, T.-T.; Chen, I.-M.; Gau, S.S.-F. Measures of heart rate variability in individuals with somatic symptom disorder. Psychosom. Med. 2017, 79, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Marinkovic, I.; Isokuortti, H.; Huovinen, A.; Trpeska Marinkovic, D.; Mäki, K.; Nybo, T.; Korvenoja, A.; Rahul, R.; Vataja, R.; Melkas, S. Prognosis after mild traumatic brain injury: Influence of psychiatric disorders. Brain Sci. 2020, 10, 916. [Google Scholar] [CrossRef]
- Ma, S.; Yang, J.; Yang, B.; Kang, L.; Wang, P.; Zhang, N.; Wang, W.; Zong, X.; Wang, Y.; Bai, H.; et al. The patient health questionnaire-9 vs. The hamilton rating scale for depression in assessing major depressive disorder. Front. Psychiatry 2021, 12, 747139. [Google Scholar] [CrossRef]
- Saracino, R.M.; Weinberger, M.I.; Roth, A.J.; Hurria, A.; Nelson, C.J. Assessing depression in a geriatric cancer population. Psycho-oncology 2017, 26, 1484–1490. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.M.; Hwang, K.S.; Lee, S.Y.; Seo, J.S.; Jang, S.H. Reliability and validity of the korean version of somatic symptom scale-8. Psychiatry Investig. 2020, 17, 814–821. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Sociodemographics | |
| Age (years) | 60.60 ± 12.46 |
| Male | 66 (48.50) |
| Female | 70 (51.50) |
| Lifestyle | |
| BMI (kg/m2) | 21.66 ± 2.06 |
| Smoking | 278 (65.30) |
| Regular alcohol use | 148 (34.70) |
| Comorbidities | |
| Hypertension | 83 (61.00) |
| Arrhythmia | 18 (13.20) |
| Diabetes mellitus | 74 (54.40) |
| Dyslipidemia | 67 (49.30) |
| Coronary artery disease | 7 (5.10) |
| Heart failure | 29 (21.30) |
| Medication | |
| Beta blocker | 33 (24.30) |
| Calcium channel blocker | 87 (64.00) |
| ACE-i/ARB | 82 (60.30) |
| Diuretics | 67 (49.30) |
| MMSE | 23.43 ± 3.32 |
| MBI | 39.18 ± 18.13 |
| HRV parameter (frequency domain) | |
| VLF (ms2) | 584.62 ± 222.04 |
| LF (ms2) | 432.46 ± 159.42 |
| HF (ms2) | 168.54 ± 71.57 |
| LF/HF ratio | 5.34 ± 2.75 |
| HRV parameter (time domain) | |
| SDNN (ms) | 98.90 ± 29.57 |
| SDANN (ms) | 98.20 ± 29.63 |
| ASDNN (ms) | 49.38 ± 11.12 |
| rMSSD (ms) | 26.21 ± 6.32 |
| pNN50 (%) | 45.06 ± 24.33 |
| Glasgow Coma Scale | |
| 13–15 | 134 (98.53) |
| 9–12 | 2 (1.47) |
| 3–8 | 0 (0.00) |
| Post-traumatic amnesia | |
| <24 h | 56 (41.18) |
| 1–7 days | 3 (2.20) |
| >7 days | 0 (0.00) |
| No post-traumatic amnesia | 77 (56.62) |
| Loss of consciousness | |
| <30 min | 47 (34.56) |
| 30 min–24 h | 5 (3.68) |
| >24 h | 0 (0.00) |
| No loss of consciousness | 84 (61.76) |
| Cause of injury | |
| Falls | 75 (55.15) |
| Traffic accidents | 38 (27.94) |
| Violence | 16 (11.76) |
| Sports | 7 (5.15) |
| Skull fracture at injury | 32 (23.53) |
| BDI | 25.59 ± 14.79 |
| PHQ-15 | 14.79 ± 9.08 |
| Statistic | p-Value | |
|---|---|---|
| BDI | 0.075 | 0.051 |
| PHQ-15 | 0.064 | 0.200 |
| VLF | 0.076 | 0.050 |
| LF | 0.074 | 0.052 |
| HF | 0.066 | 0.200 |
| LF/HF ratio | 0.058 | 0.200 |
| SDNN | 0.072 | 0.060 |
| SDANN | 0.054 | 0.200 |
| ASDNN | 0.059 | 0.200 |
| rMSSD | 0.071 | 0.061 |
| pNN50 | 0.050 | 0.200 |
| Group A (n = 28) | Group B (n = 19) | Group C (n = 32) | Group D (n = 57) | F | p-Value | Post Hoc | |
|---|---|---|---|---|---|---|---|
| Frequency domain | |||||||
| VLF (ms2) | 668.60 | 762.92 | 619.59 | 550.36 | 6.002 | 0.001 * | B > D |
| ±230.58 | ±30.15 | ±139.29 | ±242.85 | ||||
| LF (ms2) | 419.46 | 505.10 | 448.73 | 389.57 | 3.276 | 0.023 * | B > D |
| ±164.01 | ±142.19 | ±106.64 | ±158.56 | ||||
| HF (ms2) | 214.75 | 215.82 | 176.58 | 155.27 | 8.005 | <0.001 ** | A, B > D |
| ±57.96 | ±14.50 | ±69.57 | ±69.16 | ||||
| LF/HF ratio | 5.29 | 7.33 | 5.34 | 5.24 | 3.961 | 0.010 * | A > B > C, D |
| ±2.42 | ±0.52 | ±2.43 | ±2.74 | ||||
| Time domain | |||||||
| SDNN (ms) | 103.08 | 109.59 | 104.17 | 98.60 | 0.806 | 0.493 | |
| ±26.60 | ±27.01 | ±26.99 | ±29.86 | ||||
| SDANN (ms) | 106.38 | 111.13 | 92.78 | 97.09 | 2.606 | 0.054 | |
| ±29.06 | ±19.37 | ±23.69 | ±29.38 | ||||
| ASDNN (ms) | 49.41 | 50.70 | 47.08 | 48.21 | 0.611 | 0.609 | |
| ±11.04 | ±8.01 | ±9.40 | ±10.38 | ||||
| rMSSD (ms) | 27.71 | 38.57 | 33.10 | 26.26 | 6.863 | <0.001 ** | A > B, C > D |
| ±7.65 | ±16.83 | ±14.16 | ±8.49 | ||||
| pNN50 (%) | 49.13 | 55.65 | 54.27 | 47.12 | 1.229 | 0.302 | |
| ±20.81 | ±13.49 | ±21.90 | ±23.00 |
| Group E (n = 28) | Group F (n = 19) | Group G (n = 32) | Group H (n = 57) | F | p-Value | Post Hoc | |
|---|---|---|---|---|---|---|---|
| Frequency domain | |||||||
| VLF (ms2) | 650.71 | 763.87 | 609.11 | 564.34 | 5.600 | 0.001 * | F > G, H |
| ±241.70 | ±76.49 | ±114.96 | ±235.47 | ||||
| LF (ms2) | 431.62 | 471.19 | 464.39 | 390.55 | 2.796 | 0.043 * | G > H |
| ±165.00 | ±161.30 | ±118.62 | ±146.29 | ||||
| HF (ms2) | 214.90 | 217.40 | 196.04 | 154.19 | 9.747 | <0.001 ** | E, F > H |
| ±61.93 | ±21.34 | ±68.92 | ±65.72 | ||||
| LF/HF ratio | 5.15 | 7.06 | 5.80 | 5.19 | 3.659 | 0.014 * | E > F > H |
| ±2.49 | ±1.21 | ±2.67 | ±2.56 | ||||
| Time domain | |||||||
| SDNN (ms) | 102.37 | 108.05 | 109.57 | 97.31 | 1.559 | 0.203 | |
| ±28.94 | ±25.44 | ±26.09 | ±28.56 | ||||
| SDANN (ms) | 105.97 | 110.41 | 97.44 | 92.02 | 2.328 | 0.078 | |
| ±26.60 | ±25.81 | ±23.46 | ±28.64 | ||||
| ASDNN (ms) | 50.35 | 48.94 | 47.71 | 46.31 | 0.324 | 0.808 | |
| ±11.18 | ±8.76 | ±9.90 | ±9.95 | ||||
| rMSSD (ms) | 27.20 | 35.05 | 35.00 | 27.48 | 4.271 | 0.007 * | F, G > H |
| ±7.64 | ±15.19 | ±16.13 | ±9.47 | ||||
| pNN50 (%) | 47.11 | 57.25 | 56.31 | 47.05 | 2.141 | 0.098 | |
| ±21.84 | ±13.77 | ±22.01 | ±22.34 |
| Pearson Correlation Coefficient (r) | p-Value | |
|---|---|---|
| Frequency domain | ||
| VLF (ms2) | −0.267 | 0.002 * |
| LF (ms2) | −0.192 | 0.025 * |
| HF (ms2) | −0.396 | <0.001 ** |
| LF/HF ratio | −0.086 | 0.316 |
| Time domain | ||
| SDNN (ms) | −0.077 | 0.370 |
| SDANN (ms) | −0.128 | 0.137 |
| ASDNN (ms) | −0.043 | 0.618 |
| rMSSD (ms) | −0.193 | 0.025 * |
| pNN50 (%) | −0.092 | 0.285 |
| Pearson Correlation Coefficient (r) | p-Value | |
|---|---|---|
| Frequency domain | ||
| VLF (ms2) | −0.258 | 0.002 * |
| LF (ms2) | −0.210 | 0.014 * |
| HF (ms2) | −0.395 | <0.001 ** |
| LF/HF ratio | −0.091 | 0.294 |
| Time domain | ||
| SDNN (ms) | −0.084 | 0.331 |
| SDANN (ms) | −0.106 | 0.221 |
| ASDNN (ms) | −0.033 | 0.706 |
| rMSSD (ms) | −0.206 | 0.016 * |
| pNN50 (%) | −0.107 | 0.214 |
| Dependent Variable | Independent Variable | Standardized β | B | 95% CI | p-Value | VIF | Adjusted R2 |
|---|---|---|---|---|---|---|---|
| BDI | Constant | 56.505 | 0.217 | ||||
| HF | −0.364 | −0.080 | (−0.114, −0.047) | <0.001 ** | 1.014 | ||
| VLF | −0.229 | −0.016 | (−0.027, −0.005) | 0.003 * | 1.009 | ||
| LF | −0.155 | −0.015 | (−0.030, −0.001) | 0.045 * | 1.007 | ||
| PHQ-15 | Constant | 33.962 | 0.219 | ||||
| HF | −0.362 | −0.049 | (−0.070. −0.029) | <0.001 ** | 1.014 | ||
| VLF | −0.219 | −0.009 | (−0.016, −0.003) | 0.005 * | 1.009 | ||
| LF | −0.174 | −0.010 | (−0.020, −0.001) | 0.025 * | 1.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, S.D.; Park, E.J. Association of Depressive and Somatic Symptoms with Heart Rate Variability in Patients with Traumatic Brain Injury. J. Clin. Med. 2023, 12, 104. https://doi.org/10.3390/jcm12010104
Yoo SD, Park EJ. Association of Depressive and Somatic Symptoms with Heart Rate Variability in Patients with Traumatic Brain Injury. Journal of Clinical Medicine. 2023; 12(1):104. https://doi.org/10.3390/jcm12010104
Chicago/Turabian StyleYoo, Seung Don, and Eo Jin Park. 2023. "Association of Depressive and Somatic Symptoms with Heart Rate Variability in Patients with Traumatic Brain Injury" Journal of Clinical Medicine 12, no. 1: 104. https://doi.org/10.3390/jcm12010104