
Variability of Care and Access to Transplantation for Children with Biliary Atresia Who Need a Liver Replacement

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Analysis Plan
2.2. Study Population: Inclusion and Exclusion Criteria
2.3. Data for Analysis
2.4. Data Management and Statistical Analyses
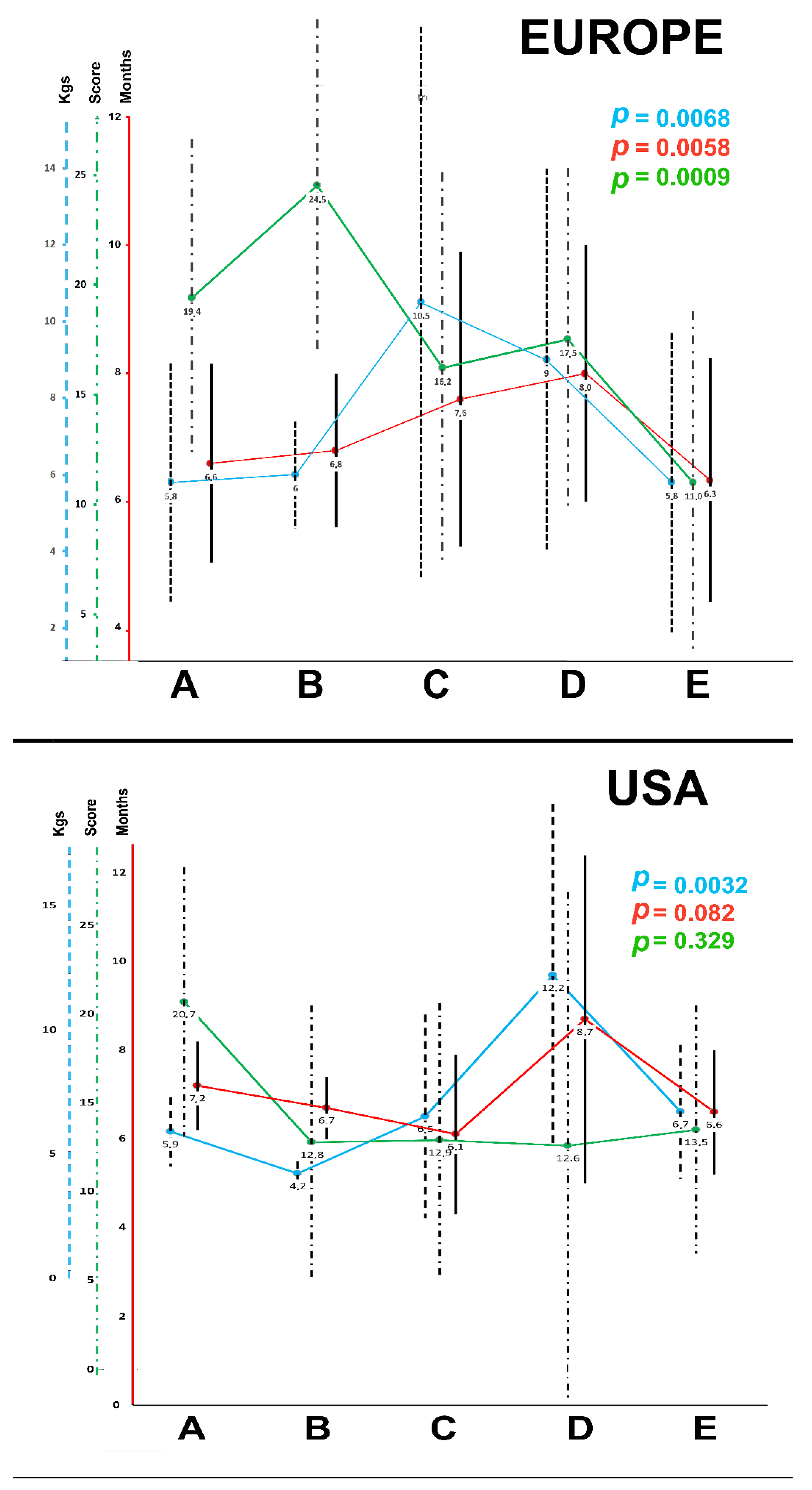
- To analyze referral pathways and their dynamic, subgroups were defined as per the type of initial BA surgery: (A) no-surgery, (B) explorative laparotomy only (no-Kasai), (C) Kasai procedure performed in non-expert liver center, (D) Kasai procedure performed in expert liver center other than the LTC and (E) Kasai procedure performed in the LTC where the transplant was performed later.
- As access to LT and waiting time for LT are very different when a candidate for LT is proposed to LD-LT, a second analysis was performed with the same subgrouping method, and comparing all patients who had living donor LT versus all others.
3. Results
3.1. Europe
3.2. USA

{kind=link}
{kind=link}
{kind=link}
| A | B | C | D | E | p | |||
|---|---|---|---|---|---|---|---|---|
| NO Surgery | Explorative Laparotomy | KASAI in Non-Liver-Expert Centre | KASAI in Liver-Expert Other Centre | KASAI and Transplant in Same Center | ||||
| N (%) | 25 (15%) | 4 (2%) | 44 (27%) | 12 (7%) | 80 (49%) | |||
| Polysplenia Syndrome | N (%) | 5 (20%) | 1 (25%) | 6 (14%) | 2 (17%) | 11 (14%) | 0.9126 | |
| Age at Kasai (if kasai) | (Days) | Mean ± SD | - | - | 62.0 ± 25 | 69.0 ± 18.7 | 58.2 ± 26.0 | 0.4499 |
| At assessment | Age (months) | Mean ± SD | 5.8 ± 3.1 | 6.0 ± 1.4 | 10.5 ± 7.2 | 9.0 ± 5.0 | 5.8 ± 3.9 | 0.0068 |
| Weight (Kgs) | Mean ± SD | 6.6 ± 1.55 | 6.8 ± 1.2 | 7.6 ±2.3 | 8.0 ± 2.0 | 6.34 ± 1.9 | 0.0058 | |
| PELD score | score | 19.4 ± 7.2 | 24.5 ± 7.55 | 16.2 ± 8.9 | 17.5 ± 7.8 | 11 ± 7.8 | 0.0009 | |
| Presence of ascites | N (%) | 20 (80%) | 3 (75%) | 27 (61%) | 8 (67%) | 47 (59%) | 0.3943 | |
| Enteral nutrition support | N (%) | 7 (28%) | 1 (25%) | 17 (39%) | 2 (17%) | 35 (44%) | 0.3079 | |
| Parenteral nutrition support | N (%) | - | - | 5 (11%) | 3 (25%) | 12 (15%) | 0.1639 | |
| At registration on list | Age (months) | Mean ± SD | 6.6 ± 3.3 | 8.25 ± 2.2 | 12.2 ± 7.5 | 11.7 ± 5.7 | 6.5 ± 4.2 | 0.0012 |
| Weight (Kgs) | Mean ± SD | 6.8 ± 1.6 | 7.2 ±0.7 | 8.1 ± 2.2 | 8.4 ± 2.8 | 6.6 ± 1.9 | 0.0005 | |
| PELD score | score | 17.8 ± 6.9 | 20.7 ± 6.8 | 15.4 ± 8.2 | 17.9 ± 8.7 | 11.5 ± 7.8 | 0.0005 | |
| Delta Peld score 1 | assessment to registration on list | delta | 1.6 ± 4.4 | 3.7 ± 2.4 | 0.8 ± 3.4 | 0.9 ± 3.2 | 1.4 ± 3.8 | 0.5916 |
| While waiting for LT | Worsening ascites | N (%) | 20 (80%) | 3 (75%) | 28 (64%) | 10 (83%) | 59 (74%) | 0.5196 |
| Albumin infusion(s) | N (%) | 15 (60%) | 2 (50%) | 26 (59%) | 10 (83%) | 45 (57%) | 0.5254 | |
| Blood transfusion(s) | N (%) | 4 (15%) | 1 (25%) | 13 (30%) | 7 (58%) | 23 (29%) | 0.1311 | |
| Enteral nutrition support | N (%) | 11 (44%) | 1 (25%) | 18 (41%) | 6 (50%) | 30 (38%) | 0.8922 | |
| parenteral nutrition support | N (%) | 3 (12%) | - | 13 (30%) | 5 (42%) | 16 (20%) | 0.1504 | |
| 1 Hospital admission < 5 days | N (%) | 3 (12%) | 1 (25%) | 6 (14%) | - | 10 (12%) | 0.6655 | |
| >1 Hospital admission < 5 days | N (%) | 5 (20%) | - | 4 (9%) | 5 (42%) | 8 (10%) | 0.0227 | |
| 1 Hospital admission > 5 days | N (%) | 14 (56%) | 1 (25%) | 19 (43%) | 8 (67%) | 43 (54%) | 0.4318 | |
| >1 Hospital admission > 5 days | N (%) | 3 (12%) | - | 2 (5%) | - | 10 (12%) | 0.3952 | |
| Recovery in ICU | N (%) | 1 (4%) | - | 1 (2%) | 4 (33%) | 16 (20%) | 0.0062 | |
| At Liver transplant | Age (months) | Mean ± SD | 9.1 ± 6.05 | 18 ± 21.4 | 14.6 ± 8.5 | 13.4 ± 7.1 | 8.9 ± 6.1 | 0.0012 |
| Weight (Kgs) | Mean ± SD | 7.5 ± 2.1 | 8.8 ± 2.9 | 9.0 ± 2.4 | 8.9 ± 3.2 | 7.6 ± 2.1 | 0.0072 | |
| PELD score | score | 21.6 ± 6.5 | 24.0 ± 12.1 | 17.7 ± 10.5 | 18.7 ± 10.0 | 14.9 ± 9.7 | 0.0184 | |
| Clinical condition at LT | Elective-Home | N (%) | 11 (44%) | 3 (75%) | 29 (66%) | 5 (42%) | 40 (50%) | 0.1300 |
| Hospital-bound | N (%) | 13 (52%) | 1 (25%) | 15 (34%) | 5 (42%) | 29 (36%) | ||
| ICU-bound | N (%) | 1 (4%) | - | - | 2 (16%) | 11 (14%) | ||
| Waiting time | Assessment to LT (Days) | Median (p25–p75) | 40 (25–72) | 34 (26–695) | 77 (45–149) | 80 (22–157) | 71 (34–121) | 0.3530 |
| Delta PELD score 2 | Assessment to LT | Mean ± SD | 3.8 ± 9.0 | 3.2 ± 5.25 | 2.4 ± 5.4 | 0.7 ± 7.4 | 3.4 ± 6.4 | 0.6658 |
| Graft type | Full-size | N (%) | 5 (20%) | - | 3 (7%) | - | 12 (15%) | 0.6108 |
| Split liver graft | N (%) | 7 (28%) | 1 (25%) | 16 (36%) | 5 (42%) | 31 (39%) | ||
| Reduced liver | N (%) | - | - | 1 (2%) | - | 4 (5%) | ||
| Living donor left lobe | N (%) | 13 (52%) | 3 (75%) | 24 (54%) | 7 (58%) | 33 (41%) | ||
| post-LT recovery | Respiratory assistance (time—days) | Median (p25–p75) | 1 (1–5) | 0 (0–2) | 1 (0–2) | 1 (0–7) | 2 (0–6) | 0.1415 |
| Enteral nutrition support need | N (%) | 17 (68%) | - | 26 (59%) | 8 (67%) | 71 (89%) | <0.0001 | |
| Parenteral nutrition need | N (%) | 19 (76%) | 2 (50%) | 29 (66%) | 8 (67%) | 65 (81%) | 0.2565 | |
| ITU stay (days) | Median (p25–p75) | 7 (2–11) | 2 (2–2.5) | 4.5 (2–15.5) | 4.5 (2–20) | 6 (3–12) | 0.3665 | |
| Hospital stay (days) | Median (p25–p75) | 27 (22–35) | 24.5 (16.5–32.5) | 24 (17–34) | 30 (20–44.5) | 26 (21–35) | 0.5731 | |
| Outcome | Death while waiting | N (%) | - | - | - | - | - | 0.6584 |
| Death after LT | N (%) | - | - | 1 (2%) | - | 4 (5%) | ||
| Alive and well | N (%) | 25 (100%) | 4 (100%) | 43 (98%) | 12 (100%) | 76 (95%) | ||
| Current age of survivors (months) | Mean ± SD | 47.5 ± 21.3 | 46.7 ± 5.3 | 48.4 ± 18.2 | 50.3 ± 15.7 | 38.3 ± 17.7 | 0.0157 |
| A | B | C | D | E | p | |||
|---|---|---|---|---|---|---|---|---|
| NO Surgery | Explorative Laparotomy | KASAI in Non-Liver-Expert Centre | KASAI in Liver-Expert Other Centre | KASAI and Transplant in Same Center | ||||
| N | 6 (11%) | 4 (7%) | 18 (33%) | 5 (9%) | 22 (40%) | |||
| Polysplenia Syndrome | N | 1 (17%) | - | 2 (11%) | - | 6 (27%) | 0.4409 | |
| Age at Kasai (if kasai) | (Days) | Mean ± SD | - | - | 66.8 ± 28.9 | 53.0 ± 17.3 | 55.2 ± 27.0 | 0.157 |
| At assessment | Age (months) | Mean ± SD | 5.9 ± 1.4 | 4.2 ± 0.5 | 6.5 ± 4.1 | 12.2 ± 6.9 | 6.7 ± 2.7 | 0.0032 |
| Weight (Kgs) | Mean ± SD | 7.2 ± 1.0 | 6.7 ± 0.7 | 6.1 ± 1.8 | 8.7 ± 3.7 | 6.6 ± 1.4 | 0.0821 | |
| PELD score | score | 20.7 ± 7.6 | 12.8 ± 7.7 | 12.9 ± 7.7 | 12.6 ± 14.3 | 13.5 ± 7.0 | 0.329 | |
| Presence of ascites | N (%) | 4 (67%) | 2 (50%) | 12 (67%) | 3 (60%) | 13 (59%) | 0.9682 | |
| Enteral nutrition support | N (%) | 3 (50%) | - | 10 (56%) | 2 (40%) | 13 (59%) | 0.2739 | |
| Parenteral nutrition support | N (%) | 2 (33%) | - | 6 (33%) | - | 2 (9%) | 0.1399 | |
| At registration on list | Age (months) | Mean ± SD | 5.9 ± 1.1 | 4.9 ± 0.8 | 7.2 ± 4.4 | 12.4 ± 7.3 | 7.3 ± 2.7 | 0.0264 |
| Weight (Kgs) | Mean ± SD | 7.2 ± 1.0 | 6.9 ± 0.5 | 6.4 ± 1.8 | 8.5 ± 3.9 | 6.6 ± 1.1 | 0.181 | |
| PELD score | score | 20.8 ± 8.5 | 13.5 ± 7.5 | 12.9 ± 7.7 | 14.4 ± 17.2 | 14.1 ± 7.6 | 0.459 | |
| Delta Peld score 1 | assessment to registration on list | delta | 0.2 ± 1.3 | 0.8 +/1 1.5 | 0.1 ± 0.2 | 1.8 ± 4.0 | 0.6 ± 4.3 | 0.618 |
| While waiting for LT | Worsening ascites | N (%) | 5 (83%) | 2 (50%) | 8 (44%) | 2 (40%) | 14 (64%) | 0.4201 |
| Albumin infusion(s) | N (%) | 5 (83%) | 2 (50%) | 7 (39%) | 2 (40%) | 16 (73%) | 0.135 | |
| Blood transfusion(s) | N (%) | 4 (67%) | 2 (50%) | 8 (44%) | 1 (20%) | 12 (55%) | 0.5826 | |
| Enteral nutrition support | N (%) | 3 (50%) | 4 (100%) | 5 (28%) | 2 (40%) | 9 (41%) | 0.1255 | |
| parenteral nutrition support | N (%) | 4 (67%) | 2 (50%) | 9 (50%) | - | 12 (55%) | 0.212 | |
| 1 Hospital admission < 5 days | N (%) | 1 (17%) | 1 (25%) | 5 (28%) | 3 (60%) | 5 (23%) | 0.5118 | |
| >1 Hospital admission < 5 days | N (%) | 1 (17%) | 2 (50%) | 4 (22%) | 1 (20%) | 3 (14%) | 0.574 | |
| 1 Hospital admission > 5 days | N (%) | 5 (83%) | 1 (25%) | 7 (39%) | 1 (20%) | 10 (46%) | 0.2195 | |
| >1 Hospital admission > 5 days | N (%) | 1 (17%) | 2 (50%) | 5 (28%) | - | 8 (36%) | 0.4159 | |
| Recovery in ICU | N (%) | 4 (67%) | 1 (25%) | 7 (39%) | - | 6 (27%) | 0.1787 | |
| At Liver transplant | Age (months) | Mean ± SD | 8.1 ± 1.8 | 8.9 ± 0.7 | 13.0 ± 7.2 | 16.2 ± 10.1 | 10.9 ± 4.2 | 0.0511 |
| Weight (Kgs) | Mean ± SD | 8.9 ± 1.6 | 8.2 ± 0.8 | 9.3 ± 2.6 | 8.5 ± 5.2 | 7.9 ± 1.7 | 0.559 | |
| PELD score | score | 22.0 ± 10.3 | 23.3 ± 8.3 | 12.8 ± 11.7 | 16.2 ± 16.0 | 21.5 ± 10.7 | 0.139 | |
| Clinical condition at LT | Elective-Home | N (%) | 2 (33%) | 2 (50%) | 11 (65%) | 4 (80%) | 9 (41%) | 0.4352 |
| Hospital-bound | N (%) | 2 (33%) | 1 (25%) | 4 (24%) | 1 (20%) | 11 (50%) | ||
| ICU-bound | N (%) | 2 (33%) | 1 (25%) | 2 (12%) * | - | 2 (9%) | ||
| Waiting time | Assessment to LT (Days) | Median (p25–p75) | 43 (36.8–62) | 135 (103.5–151.5) | 112 (74–303) | 117 (49–146) | 82.5 (52.3–133.3) | 0.1688 |
| Delta PELD score 2 | Assessment to LT | Mean ± SD | 1.6 ± 11.4 | 10.5 ± 5.5 | 0.2 ± 11.7 | 3.6 ± 5.5 | 8.0 ± 10.8 | 0.163 |
| Graft type | Full-size | N (%) | 2 (33%) | 3 (75%) | 16 (94%) | 3 (60%) | 6 (27%) | 0.0202 |
| Split liver graft | N (%) | 2 (33%) | 1 (25%) | - | 2 (40%) | 11 (50%) | ||
| Reduced liver | N (%) | - | - | - | - | 2 (9%) | ||
| Living donor left lobe | N (%) | 2 (33%) | - | 1 (6%) | - | 3 (14%) | ||
| post-LT recovery | Respiratory assistance (time - days) | Median (p25–p75) | 22.5 (9.3–46.3) | 16.5 (10.8–44.3) | 17 (5–30) | 2 (1–7) | 9 (5–20.3) | 0.2132 |
| Enteral nutrition support need | N (%) | 6 (100%) | 4 (100%) | 14 (82%) | 3 (60%) | 19 (91%) | 0.268 | |
| Parenteral nutrition need | N (%) | 6 (100%) | 3 (75%) | 11 (65%) | 1 (20%) | 13 (59%) | 0.0953 | |
| ITU stay (days) | Median (p25–p75) | 24.5 (10.5–40) | 19.5 (12–46.8) | 17 (8–38) | 3 (3–8) | 10 (6.3–19.8) | 0.0802 | |
| Hospital stay (days) | Median (p25–p75) | 33 (19–54.5) | 27 (24.5–70.5) | 28 (19–81) | 10 (9–11) | 19.5 (11.3–33.3) | 0.0621 | |
| Outcome | Death while waiting | N (%) | - | - | 1 (6%) | - | - | 0.8969 |
| Death after LT | N (%) | - | - | 1 (6%) | - | 2 (9%) | ||
| Alive and well | N (%) | 6 (100%) | 4 (100%) | 16 (89%) | 5 (100%) | 20 (91%) | ||
| Current age of survivors (months) | Mean ± SD | 41.6 ± 9.5 | 45.6 ± 17.6 | 37.3 ± 15.9 | 47.8 ± 21.1 | 39.8 ± 21.6 | 0.804 |
| EUROPE | p | USA | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ALL | Living Donor LT | Deceased Donor LT | ALL | Living Donor LT | Deceased Donor LT | |||||
| N | N (%) | 165 | 80 (48.5%) | 85 (51.5%) | 54 | 6 (11.1%) | 48 (88.9%) | |||
| Prematurity | N (%) | 11 (6.7%) | 7 (63.6%) | 4 (36.4%) | 0.2008 | 5 (9.3%) | - | 5 (10.4%) | 0.9339 | |
| Co-morbidity | Cardiac | N (%) | 9 (5.5%) | 6 (42.9%) | 3 (23.1%) | 0.4810 | 1 (1.9%) | - | 1 (2.1%) | 0.3916 |
| Digestive | N (%) | 10 (6.1%) | 5 (35.7%) | 5 38.5%) | 2 (3.7%) | - | 2 (4.2%) | |||
| Other | N (%) | 8 (4.8%) | 3 (21.4%) | 5 (38.5%) | 2 (3.7%) | 1 (16.7%) | 1 (2.1%) | |||
| Polysplenia Syndrome | N (%) | 25 (15.2%) | 11 (16.5%) | 14 (16.5%) | 0.6262 | 8 (14.8%) | - | 8 (16.7%) | 0.2786 | |
| Type of initial surgery for BA | NONE | N (%) | 25 (15.2%) | 13 (16.2%) | 12 (14.2%) | 0.5065 | 6 (11.1%) | 2 (33.3%) | 4 (8.3%) | 0.1587 |
| Explorative laparotomy | N (%) | 4 (2.4%) | 3 (3.7%) | 1 (1.2%) | 4 (7.4%) | - | 4 (8.3%) | |||
| Kasai | N (%) | 136 (82.4%) | 64 (80.0%) | 72 (84.7%) | 44 (81.5%) | 4 (66.7%) | 40 (83.3%) | |||
| Kasai Centre | Non-liver expert | N (%) | 44 (26.7%) | 24 (37.5%) | 20 (27.8%) | 0.2611 | 17 (38.6%) | 1 (25.0%) | 16 (40.0%) | 0.5321 |
| Liver-expert other | N (%) | 12 (7.3%) | 7 (10.9%) | 5 (6.9%) | 5 (11.4%) | - | 5 (12.5%) | |||
| Same as LT centre | N (%) | 80 (48.5%) | 33 (51.6%) | 47 (65.3%) | 22 (50.0%) | 3 (75.0%) | 19 (47.5%) | |||
| Age at Kasai (if kasai) | (months) | Mean ± SD | 60.3 ± 25.0 | 62.2 ± 24.0 | 58.5 ± 25.7 | 0.3826 | 60.0 ± 27.2 | 50.0 ± 30.3 | 60.8 ± 27.4 | 0.4594 |
| At assessment | Age (months) | Median (p25–p75) | 6 (4–8) | 6 (4–10) | 5 (4–7) | 0.0508 | 6.2 (4.1–7.7) | 6.3 (6.2–6.5) | 5.5 (4.0–7.9) | 0.6095 |
| Weight (Kgs) | Mean ± SD | 6.8 ± 2.1 | 6.59 ± 2.0 | 7.1 ± 2.0 | 0.1438 | 6.7 ± 1.8 | 6.9 ± 1.2 | 6.7 ± 1.9 | 0.8159 | |
| PELD score | Mean ± SD | 14.2 ± 8.3 | 14.7 ± 8.6 | 13.7 ± 8.0 | 0.3990 | 13.9 ± 8.1 | 18.3 ± 6.7 | 13.1 ± 8.3 | 0.1595 | |
| Presence of ascites | N (%) | 85 (51.5%) | 57 (71.2%) | 48 (56.5%) | 0.0486 | 34 (63.0%) | 5 (83.3%) | 29 (60.4%) | 0.2731 | |
| Enteral nutrition support | N (%) | 62 (37.6%) | 25 (31.2%) | 37 (43.5%) | 0.1036 | 28 (51.9%) | 3 (50.0%) | 25 (52.1%) | 0.9232 | |
| Parenteral nutrition support | N (%) | 20 (12.1%) | 9 (11.2%) | 11 (12.9%) | 0.7394 | 10 (18.5) | - | 10 (20.8) | 0.2155 | |
| At registration on list | Age (months) | Median (p25–p75) | 7 ± (4–10) | 6 (4–8) | 8 (4–11) | 0.0543 | 6.4 (5.0–8.0) | 6.8 (6.6–7.4) | 6.0 (5.0–8.4) | 0.448 |
| Weight (Kgs) | Mean ± SD | 7.2 ± 2.1 | 6.8 ± 2.0 | 7.5 ± 2.2 | 0.0283 | 6.8 ± 1.8 | 6.9 ± 1.2 | 6.8 ± 1.8 | 0.9755 | |
| While waiting for LT | Worsening ascites | N (%) | 120 (72.7%) | 69 (86.2%) | 51 (60.0%) | 0.0002 | 30 (55.6%) | 6 (100.0%) | 24 (50.0%) | 0.0201 |
| Enteral nutrition support | N (%) | 66 (40%) | 36 36.1%) | 30 (45.0%) | 0.2496 | 22 (40.7%) | 2 (33.3%) | 20 (47.7%) | 0.6953 | |
| Parenteral nutrition support | N (%) | 37 (22.4%) | 17 (21.2%) | 20 (23.8%) | 0.6951 | 26 (48.1%) | 2 (33.3%) | 24 (50.0%) | 0.4411 | |
| Albumin infusion(s) | N (%) | 98 (59.4%) | 56 (70.0%) | 42 (50.0%) | 0.0090 | 31 (57.4%) | 6 (100.0%) | 25 (52.1%) | 0.0252 | |
| Blood transfusion(s) | N (%) | 48 (29.1%) | 26 (32.5%) | 22 (25.9%) | 0.3496 | 26 (48.1%) | 3 (50.0%) | 23 (47.9%) | 0.9233 | |
| 1 Hospital admission < 5 days | N (%) | 20 (12.1%) | 9 (11.2%) | 11 (12.9%) | 0.7394 | 15 (27.8%) | 1 (16.7%) | 14 (29.2%) | 0.5192 | |
| > 1 Hospital admission < 5 days | N (%) | 21 (12.7%) | 7 (8.7%) | 15 (17.6%) | 0.0929 | 10 (18.5%) | 1 (16.7%) | 9 (18.8%) | 0.9014 | |
| 1 Hospital admission > 5 days | N (%) | 85 (51.5%) | 35 (43.7%) | 50 (58.8%) | 0.0528 | 24 (44.4%) | 5 (83.3%) | 19 (39.6%) | 0.042 | |
| > 1 Hospital admission > 5 days | N (%) | 15 (9.1%) | 8 (10.0%) | 7 (8.2%) | 0.6935 | 15 (27.8%) | 1 (16.7%) | 14 (29.2%) | 0.5192 | |
| Recovery in ICU | N (%) | 22 (13.3%) | 6 (7.5%) | 16 (18.8%) | 0.0325 | 17 (31.5%) | 3 (50.0%) | 14 (29.2%) | 0.3002 | |
| At Liver transplant | Age (months) | Median (p25–p75) | 8 (6–13) | 8 (6–10) | 10 (6–18) | 0.0294 | 9.8 (7.6–13) | 9.3 (8.3–10.5) | 10.0 (7.3–14.3) | 0.6297 |
| Weight (Kgs) | Med ± SD | 8.1 ± 2.3 | 7.4 ± 2.0 | 8.7 ± 2.5 | 0.0007 | 8.5 ± 2.4 | 8.4 ± 1.7 | 8.6 ± 2.5 | 0.8853 | |
| PELD score | Med ± SD | 17.2 ± 9.8 | 18.8 ± 9.8 | 15.6 ± 9.6 | 0.0395 | 18.5 ± 11.8 | 18.2 ± 12.7 | 18.5 ± 11.8 | 0.9421 | |
| Clinical condition at LT | Elective-Home | N (%) | 88 (53.3%) | 47 (58.7%) | 41 (48.2%) | 0.1990 | 28 (51.9%) | 1 (16.7%) | 27 (56.2%) | 0.1666 |
| Hospital-bound | N (%) | 63 (38.2%) | 29 (36.2%) | 34 (40.0%) | 19 (35.2%) | 4 (66.7%) | 15 (31.2%) | |||
| ICU-bound | N (%) | 14 (8.5%) | 4 (5.0%) | 10 (11.8%) | 7 (13.0%) | 1 (16.7%) | 6 (12.5%) | |||
| Waiting time | Assessment to LT (Days) | Median (p25–p75) | 63 (33–124) | 55 (33–98) | 82 (32–180) | 0.0717 | 90 (49.3–148.8) | 95.5 (56.3–128.8) | 90.5 (49.8–152.3) | 0.7726 |
| Delta PELD score | Assessment to LT | Med ± SD | 3.0 ± 6.6 | 4.0 ± 6.0 | 2.0 ± 7.0 | 0.0470 | 4.6 ± 10.9 | -0.2 ± 15.3 | 5.2 ± 10.3 | 0.2575 |
| Graft type | Full-size | N (%) | 20 (12.1%) | - | 20 (23.5%) | 30 (55.6%) | - | 30 (62.5%) | ||
| Split liver graft | N (%) | 60 (36.4%) | - | 60 (70.6%) | 16 (29.6%) | - | 16 (33.3%) | |||
| Reduced liver | N (%) | 5 (3%) | - | 5 (5.9%) | 2 (3.7%) | - | 2 (4.2%) | |||
| Living donor left lobe | N (%) | 80 (48.5%) | 80 (100%) | - | 6 (11.1%) | 6 (100.0%) | - | |||
| LT recovery | Respiratory assistance (time - days) | Median (p25–p75) | 1.0 (0–5) | 0.0 (0.0–3.5) | 3.0 (1.0–6.0) | <0.0001 | 10 (5–24.5) | 9 (6.5–16.8) | 10.5 (4.3–25.8) | 0.7726 |
| Enteral nutrition support need | N (%) | 122 (74%) | 49 (61.2%) | 73 (85.9%) | 0.0003 | 46 (86.8%) | 6 (100.0%) | 40 (85.1%) | 0.3103 | |
| Parenteral nutrition need | N (%) | 123 (74%) | 61 (76.2%) | 62 (72.9%) | 0.6258 | 34 (63.0%) | 5 (83.3%) | 29 (60.4%) | 0.2731 | |
| ITU stay (days) | Median (p25–p75) | 6 (2–12) | 3.5 (2–8.5) | 8.0 (4–15) | 0.0002 | 12 (6.3–27.0) | 10.5 (7.5–18) | 12.5 (7.5–18.0) | 0.9341 | |
| Hospital stay (days) | Median (p25–p75) | 26 (21–35) | 24.5 (17–31.5) | 27 (21–38) | 0.0312 | 23 (11.3–38) | 28.5 (20.5–33.5) | 22.0 (11.0–39.8) | 0.6794 | |
| Death after LT | N (%) | 5 (3%) | 2 (2.5%) | 3 (3.5%) | 0.6999 | 3 (5.6%) | - | 3 (6.3%) | 0.529 | |
| Alive and well | N (%) | 160 (97.0%) | 78 (97.5%) | 82 (96.5%) | 51 (94.4%) | 6 (100.0%) | 45 (93.8%) | |||
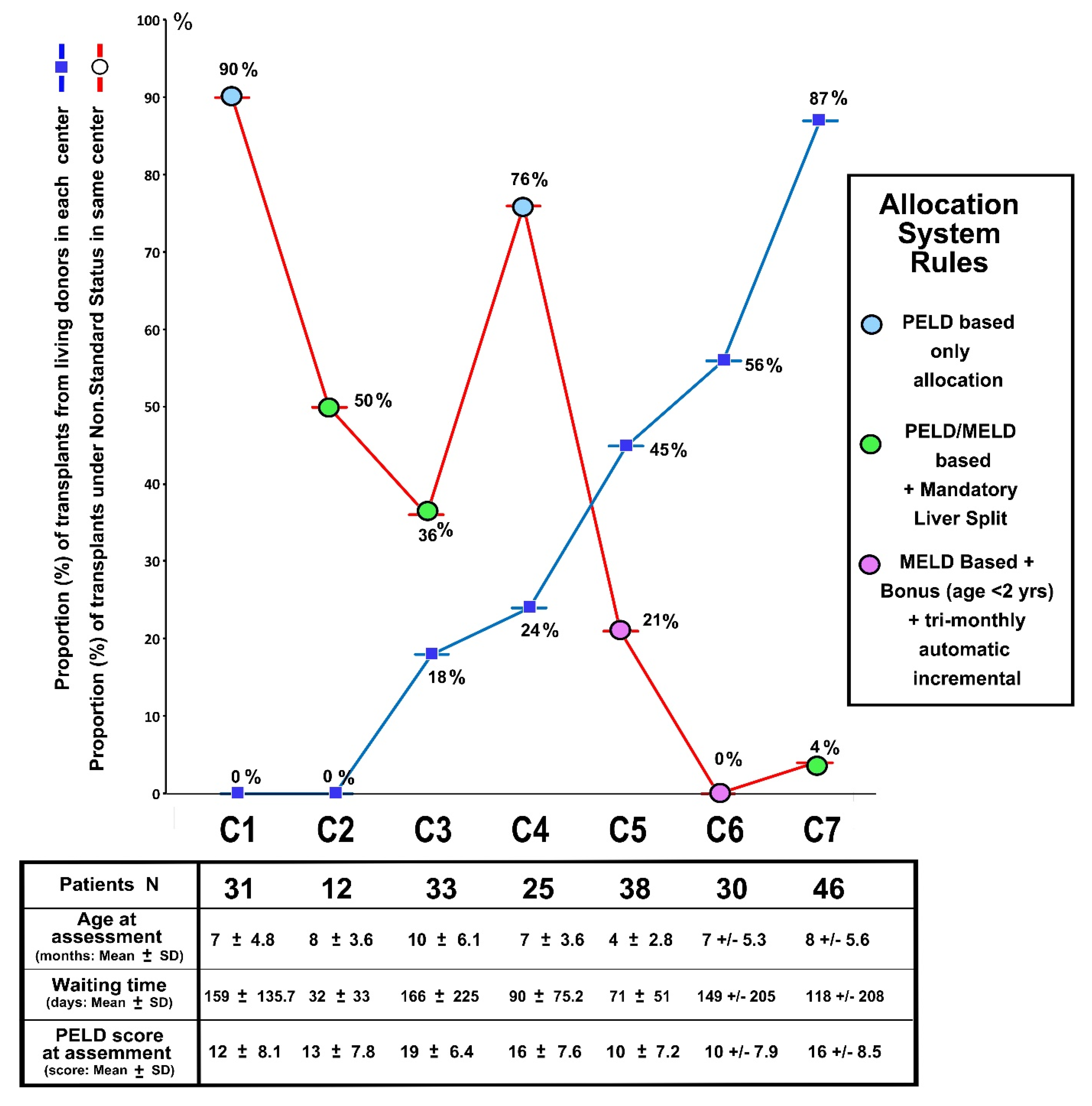
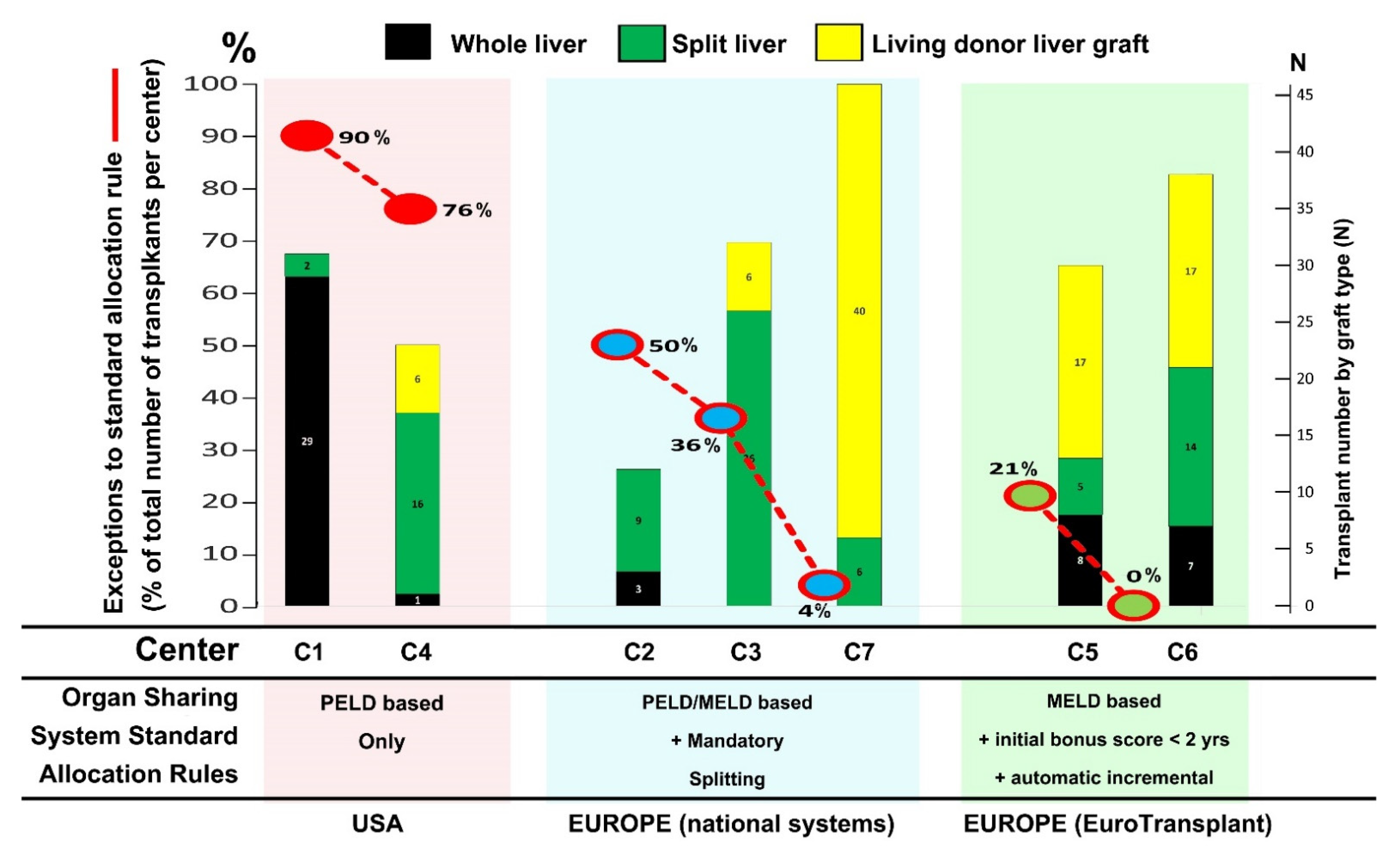
3.3. Center’s Waiting List Dynamics in Relation to Regional Allocation Rules
4. Discussion
4.1. Advanced Liver Disease at Registration on Waiting List
4.2. Variability of Timing in Registration on Waiting List
4.3. Burden of Care While Waiting for LT
4.4. Steadily Increasing Prioritization Requests
4.5. Paradigm Shift in Caring for BA and Roadmap for Future Management
4.6. More than Ever, Room for Technical Solutions
4.7. Study Limits and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ERN RARE-LIVER | European reference network for pediatric hepatological diseases. |
| BARD | Biliary Atresia and Related Diseases (multi-purpose online platform for study of biliary atresia and related diseases: http://www.bard-online.com, accessed on 10 March 2022) |
| BA | Biliary atresia |
| LT | Liver transplantation |
| PELD | Pediatric End-Stage Liver score |
| ICU | Intensive care unit |
| LD | Living donor |
| LTC | Pediatric liver transplant center |
| PN | Parenteral nutrition |
References
- De Ville de Goyet, J.; Baumann, U.; Karam, V.; Adam, R.; Nadalin, S.; Heaton, N.; Reding, R.; Branchereau, S.; Mirza, D.; Klempnauer, J.L.; et al. European Liver Transplant Registry: Donor and transplant surgery aspects of 16,641 liver transplantations in children. Hepatology 2022, 75, 634–645. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.; Goyet, J.D.V.D.; Stringer, M.; Mieli-Vergani, G.; Kelly, D.; McClean, P.; Spitz, L. Seamless management of biliary atresia in England and Wales (1999–2002). Lancet 2004, 363, 1354–1357. [Google Scholar] [CrossRef]
- Kasahara, M.; Umeshita, K.; Sakamoto, S.; Fukuda, A.; Furukawa, H.; Uemoto, S. Liver transplantation for biliary atresia: A systematic review. Pediatr. Surg. Int. 2017, 33, 1289–1295. [Google Scholar] [CrossRef]
- Chardot, C.; Buet, C.; Serinet, M.-O.; Golmard, J.-L.; Lachaux, A.; Roquelaure, B.; Gottrand, F.; Broué, P.; Dabadie, A.; Gauthier, F.; et al. Improving outcomes of biliary atresia: French national series 1986–2009. J. Hepatol. 2013, 58, 1209–1217. [Google Scholar] [CrossRef] [PubMed]
- Malenicka, S.; Ericzon, B.; Jørgensen, M.H.; Isoniemi, H.; Karlsen, T.H.; Krantz, M.; Naeser, V.; Olausson, M.; Rasmussen, A.; Rönnholm, K.; et al. Impaired intention-to-treat survival after listing for liver transplantation in children with biliary atresia compared to other chronic liver diseases: 20 years’ experience from the Nordic countries. Pediatr. Transplant. 2017, 21, e12851. [Google Scholar] [CrossRef] [PubMed]
- De Ville de Goyet, J.; Grimaldi, C.; Tuzzolino, F.; Di Francesco, F. A paradigm shift in the intention-to-transplant children with biliary atresia: Outcomes of 101 cases and a review of the literature. Pediatr. Transplant. 2019, 23, e13569. [Google Scholar] [CrossRef] [PubMed]
- Van der Doef, H.P.J.; van Rheenen, P.F.; van Rosmalen, M.; Rogiers, X.; Verkade, H.J. Wait-list mortality of young patients with Biliary atresia: Competing risk analysis of a eurotransplant regis-try-based cohort. Liver Transplant. 2018, 24, 810–819. [Google Scholar] [CrossRef] [Green Version]
- Leung, D.H.; Narang, A.; Minard, C.G.; Hiremath, G.; Goss, J.A.; Shepherd, R. A 10-Year united network for organ sharing review of mortality and risk factors in young children awaiting liver transplantation. Liver Transplant. 2016, 22, 1584–1592. [Google Scholar] [CrossRef] [Green Version]
- De Vries, W.; de Langen, Z.J.; Aronson, D.C.; Hulscher, J.B.; Peeters, P.M.; Jansen-Kalma, P.; Verkade, H.J. Mortality of biliary atresia in children not undergoing liver transplantation in The Netherlands. Pediatr. Transplant. 2011, 15, 176–183. [Google Scholar] [CrossRef]
- D’Souza, R.; Grammatikopoulos, T.; Pradhan, A.; Sutton, H.; Douiri, A.; Davenport, M.; Verma, A.; Dhawan, A. Acute-on-chronic liver failure in children with biliary atresia awaiting liver transplantation. Pediatr. Transplant. 2019, 23, e13339. [Google Scholar] [CrossRef]
- Tessier, M.E.M.; Harpavat, S.; Shepherd, R.W.; Hiremath, G.S.; Brandt, M.L.; Fisher, A.; Goss, J.A. Beyond the Pediatric end-stage liver disease system: Solutions for infants with biliary atresia requiring liver transplant. World J. Gastroenterol. 2014, 20, 11062–11068. [Google Scholar] [CrossRef] [PubMed]
- Hsu, E.; Mazariegos, G.V. Global lessons in graft type and pediatric liver allocation: A path toward improving outcomes and eliminating wait-list mortality. Liver Transplant. 2017, 23, 86–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischler, B.; Baumann, U.; D’Agostino, D.; D’Antiga, L.; Dezsofi, A.; Debray, D.; Durmaz, O.; Evans, H.; Frauca, E.; Hadzic, N.; et al. Similarities and Differences in Allocation Policies for Pediatric Liver Transplantation Across the World. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 700–705. [Google Scholar] [CrossRef] [Green Version]
- Kasahara, M.; Umeshita, K.; Sakamoto, S.; Fukuda, A.; Furukawa, H.; Sakisaka, S.; Kobayashi, E.; Tanaka, E.; Inomata, Y.; Kawasaki, S.; et al. Living donor liver transplantation for biliary atresia: An analysis of 2085 cases in the registry of the Japanese Liver Transplantation Society. Am. J. Transplant. 2018, 18, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, S.S.; Mack, C.L.; Feldman, A.G.; Sokol, R.J. Biliary atresia: Indications and timing of liver transplantation and optimization of pretransplant care. Liver Transplant. 2017, 23, 96–109. [Google Scholar] [CrossRef] [Green Version]
- Bondec, A.; Bucuvalas, J. The tip of the iceberg: Outcomes after liver transplantation for very young infants. Pediatr. Transplant. 2016, 20, 880–881. [Google Scholar] [CrossRef]
- Rana, A.; Kueht, M.; Desai, M.; Lam, F.; Miloh, T.; Moffett, J.; Galvan, N.T.N.; Cotton, R.; O’Mahony, C.; Goss, J. No Child Left Behind: Liver Transplantation in Critically Ill Children. J. Am. Coll. Surg. 2017, 224, 671–677. [Google Scholar] [CrossRef]
- Ziogas, I.A.; Ye, F.; Zhao, Z.; Cao, S.; Rauf, M.A.; Izzy, M.; Matsuoka, L.K.; Gillis, L.A.; Alexopoulos, S.P. Mortality Determinants in Children with Biliary Atresia Awaiting Liver Transplantation. J. Pediatr. 2021, 228, 177–182. [Google Scholar] [CrossRef]
- Pugliese, R.; Fonseca, E.A.; Porta, G.; Danesi, V.; Guimaraes, T.; Porta, A.; Miura, I.K.; Borges, C.; Candido, H.; Benavides, M.; et al. Ascites and serum sodium are markers of increased waiting list mortality in children with chronic liver failure. Hepatology 2014, 59, 1964–1971. [Google Scholar] [CrossRef]
- Kohaut, J.; Guérin, F.; Fouquet, V.; Gonzales, E.; de Lambert, G.; Martelli, H.; Jacquemin, E.; Branchereau, S. First liver transplantation for biliary atresia in children: The hidden effects of non-centralization. Pediatr. Transplant. 2018, 22, e13232. [Google Scholar] [CrossRef]
- Karakoyun, M.; Baran, M.; Turan, C.; Kilic, M.; Ergun, O.; Aydogdu, S. Infants with extrahepatic biliary atresia: Effect of follow-up on the survival rate at Ege University Medical School transplantation center. Turk. J. Gastroenterol. 2017, 28, 298–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lampela, H.; Ritvanen, A.; Kosola, S.; Koivusalo, A.; Rintala, R.; Jalanko, H.; Pakarinen, M. National centralization of biliary atresia care to an assigned multidisciplinary team provides high-quality outcomes. Scand. J. Gastroenterol. 2012, 47, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Tessitore, M.; Sorrentino, E.; Di Cola, G.S.; Colucci, A.; Vajro, P.; Mandato, C. Malnutrition in Pediatric Chronic Cholestatic Disease: An Up-to-Date Overview. Nutrients 2021, 13, 2785. [Google Scholar] [CrossRef] [PubMed]
- Triggs, N.D.; Beer, S.; Mokha, S.; Hosek, K.; Guffey, D.; Minard, C.G.; Munoz, F.M.; Himes, R.W. Central line-associated bloodstream infection among children with biliary atresia listed for liver transplantation. World J. Hepatol. 2019, 11, 208–216. [Google Scholar] [CrossRef]
- Samyn, M.; Davenport, M.; Jain, V.; Hadzic, N.; Joshi, D.; Heneghan, M.; Dhawan, A.; Heaton, N. Young People with Biliary Atresia Requiring Liver Transplantation: A Distinct Population Requiring Specialist Care. Transplantation 2019, 103, e99–e107. [Google Scholar] [CrossRef]
- Mohammad, S.; Alonso, E.M. Approach to Optimizing Growth, Rehabilitation, and Neurodevelopmental Outcomes in Children After Solid-organ Transplantation. Pediatr. Clin. N. Am. 2010, 57, 539–557. [Google Scholar] [CrossRef]
- Ng, V.L.; Mazariegos, G.V.; Kelly, B.; Horslen, S.; McDiarmid, S.V.; Magee, J.C.; Loomes, K.M.; Fischer, R.; Sundaram, S.S.; Lai, J.C.; et al. Barriers to ideal outcomes after pediatric liver transplantation. Pediatr. Transplant. 2019, 23, e13537. [Google Scholar] [CrossRef]
- Sun, Y.; Jia, L.; Yu, H.; Zhu, M.; Sheng, M.; Yu, W. The Effect of Pediatric Living Donor Liver Transplantation on Neurocognitive Outcomes in Children. Ann. Transplant. 2019, 24, 446–453. [Google Scholar] [CrossRef]
- Parmar, A.; VanDriel, S.M.; Ng, V.L. Health-related quality of life after pediatric liver transplantation: A systematic review. Liver Transplant. 2017, 23, 361–374. [Google Scholar] [CrossRef]
- Vimalesvaran, S.; Souza, L.N.; Deheragoda, M.; Samyn, M.; Day, J.; Verma, A.; Vilca-Melendez, H.; Rela, M.; Heaton, N.; Dhawan, A. Outcomes of adults who received liver transplant as young children. eClinicalMedicine 2021, 38, 100987. [Google Scholar] [CrossRef]
- Angelico, R.; Trapani, S.; Spada, M.; Colledan, M.; De Goyet, J.V.; Salizzoni, M.; De Carlis, L.; Andorno, E.; Gruttadauria, S.; Ettorre, G.M.; et al. A national mandatory-split liver policy: A report from the Italian experience. Am. J. Transplant. 2019, 19, 2029–2043. [Google Scholar] [CrossRef]
- Kitajima, T.; Sakamoto, S.; Sasaki, K.; Narumoto, S.; Kazemi, K.; Hirata, Y.; Fukuda, A.; Imai, R.; Miyazaki, O.; Irie, R.; et al. Impact of graft thickness reduction of left lateral segment on outcomes following pediatric living donor liver transplantation. Am. J. Transplant. 2018, 18, 2208–2219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourdeaux, C.; Darwish, A.; Jamart, J.; Tri, T.T.; Janssen, M.; Lerut, J.; Otte, J.B.; Sokal, E.; de Ville de Goyet, J.; Reding, R. Liv-ing-Related Versus Deceased Donor Pediatric Liver Transplantation: A Multivariate Analysis of Technical and Immunological Complications in 235 Recipients. Am. J. Transplant. 2007, 7, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Montenovo, M.I.; Bambha, K.; Reyes, J.; Dick, A.; Perkins, J.; Healey, P. Living liver donation improves patient and graft survival in the pediatric population. Pediatr. Transplant. 2019, 23, e13318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, M.T.; Feurer, I.D.; Chari, R.S.; Gorden, D.L.; Wright, J.K.; Pinson, C.W. Survival after pediatric liver transplantation: Why does living donation offer an advantage? Arch. Surg. 2005, 140, 465–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehar, M.; Parekh, R.S.; Stunguris, J.; De Angelis, M.; Van Roestel, K.; Ghanekar, A.; Cattral, M.; Fecteau, A.; Ling, S.; Kamath, B.M.; et al. Superior Outcomes and Reduced Wait Times in Pediatric Recipients of Living Donor Liver Transplantation. Transplant. Direct 2019, 5, e430. [Google Scholar] [CrossRef]
- Barbetta, A.; Butler, C.; Barhouma, S.; Hogen, R.; Rocque, B.; Goldbeck, C.; Schilperoort, H.; Meeberg, G.; Shapiro, J.; Kwon, Y.K.; et al. Living Donor Versus Deceased Donor Pediatric Liver Transplantation: A Systematic Review and Meta-analysis. Transplant. Direct 2021, 7, e767. [Google Scholar] [CrossRef]
- Wildhaber, B.E.; Majno, P.; Mayr, J.; Zachariou, Z.; Hohlfeld, J.; Schwoebel, M.; Kistler, W.; Meuli, M.; Le Coultre, C.; Mentha, G.; et al. Biliary Atresia: Swiss National Study, 1994–2004. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 299–307. [Google Scholar] [CrossRef]
- Elisofon, S.A.; Magee, J.C.; Ng, V.L.; Horslen, S.P.; Fioravanti, V.; Economides, J.; Erinjeri, J.; Anand, R.; Mazariegos, G.V.; Dunn, S.; et al. Society of pediatric liver transplantation: Current registry status 2011–2018. Pediatr. Transplant. 2020, 24, e13605. [Google Scholar] [CrossRef]
- Kwong, A.J.; Kim, W.R.; Lake, J.R.; Smith, J.M.; Schladt, D.P.; Skeans, M.A.; Noreen, S.M.; Foutz, J.; Booker, S.E.; Cafarella, M.; et al. OPTN/SRTR 2019 Annual Data Report: Liver. Am. J. Transplant. 2021, 21 (Suppl. 2), 208–315. [Google Scholar] [CrossRef]
- Yoeli, D.; Goss, M.; Galván, N.T.N.; Desai, M.S.; Miloh, T.A.; Rana, A. Trends in pediatric liver transplant donors and deceased donor circumstance of death in the United States, 2002–2015. Pediatr. Transplant. 2018, 22, e13156. [Google Scholar] [CrossRef] [PubMed]
- Saidi, R.F.; Jabbour, N.; Li, Y.; Shah, S.A.; Bozorgzadeh, A. Outcomes in partial liver transplantation: Deceased donor split-liver vs. live donor liver transplantation. HPB 2011, 13, 797–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cauley, R.P.; Vakili, K.; Potanos, K.; Fullington, N.; Graham, D.A.; Finkelstein, J.A.; Kim, H.B. Deceased donor liver transplantation in infants and small children: Are partial grafts riskier than whole organs? Liver Transpl. 2013, 19, 721–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mogul, D.B.; Luo, X.; Bowring, M.G.; Chow, E.; Massie, A.B.; Schwarz, K.B.; Cameron, A.M.; Bridges, J.F.; Segev, D.L. Fifteen-Year Trends in Pediatric Liver Transplants: Split, Whole Deceased, and Living Donor Grafts. J. Pediatr. 2018, 196, 148–153.e2. [Google Scholar] [CrossRef] [PubMed]
- Perito, E.R.; Roll, G.; Dodge, J.L.; Rhee, S.; Roberts, J.P. Split Liver Transplantation and Pediatric Waitlist Mortality in the United States: Potential for Improvement. Transplantation 2019, 103, 552–557. [Google Scholar] [CrossRef]
- Valentino, P.L.; Emre, S.; Geliang, G.; Li, L.; Deng, Y.; Mulligan, D.; I Rodriguez-Davalos, M. Frequency of whole-organ in lieu of split-liver transplantation over the last decade: Children experienced increased wait time and death. Am. J. Transplant. 2019, 19, 3114–3123. [Google Scholar] [CrossRef]
- Davenport, M.; Ong, E.; Sharif, K.; Alizai, N.; McClean, P.; Hadzic, N.; Kelly, D.A. Biliary atresia in England and Wales: Results of centralization and new benchmark. J. Pediatr. Surg. 2011, 46, 1689–1694. [Google Scholar] [CrossRef]
- Stringer, M.D. Biliary atresia: Service delivery and outcomes. Semin. Pediatr. Surg. 2008, 17, 116–122. [Google Scholar] [CrossRef]
- Verkade, H.J.; Bezerra, J.A.; Davenport, M.; Schreiber, R.A.; Mieli-Vergani, G.; Hulscher, J.B.; Sokol, R.J.; Kelly, D.A.; Ure, B.; Whitington, P.F.; et al. Biliary atresia and other cholestatic childhood diseases: Advances and future challenges. J. Hepatol. 2016, 65, 631–642. [Google Scholar] [CrossRef] [Green Version]
- Shneider, B.L.; Magee, J.C.; Karpen, S.J.; Rand, E.B.; Narkewicz, M.R.; Bass, L.M.; Schwarz, K.; Whitington, P.F.; Bezerra, J.A.; Kerkar, N.; et al. Total Serum Bilirubin within 3 Months of Hepatoportoenterostomy Predicts Short-Term Outcomes in Biliary Atresia. J. Pediatr. 2016, 170, 211–217.e2. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, H.; Koga, H.; Okawada, M.; Nakamura, H.; Lane, G.J.; Yamataka, A. Does time taken to achieve jaundice-clearance influence survival of the native liver in post-Kasai biliary atresia? World J. Pediatr. 2018, 14, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, S.; Stormon, M.O.; O’Loughlin, E.V.; Shun, A.; Thomas, G.; Benchimol, E.I.; Day, A.S.; Adams, S.; Shi, E.; Ooi, C.Y.; et al. Early Posthepatoportoenterostomy Predictors of Native Liver Survival in Biliary Atresia. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Serinet, M.-O.; Broué, P.; Jacquemin, E.; Lachaux, A.; Sarles, J.; Gottrand, F.; Gauthier, F.; Chardot, C. Management of patients with biliary atresia in France: Results of a decentralized policy 1986–2002. Hepatology 2006, 44, 75–84. [Google Scholar] [CrossRef]
- Hukkinen, M.; Kerola, A.; Lohi, J.; Heikkilä, P.; Merras-Salmio, L.; Jahnukainen, T.; Koivusalo, A.; Jalanko, H.; Pakarinen, M.P. Treatment Policy and Liver Histopathology Predict Biliary Atresia Outcomes: Results after National Centralization and Protocol Biopsies. J. Am. Coll. Surg. 2018, 226, 46–57. [Google Scholar] [CrossRef] [Green Version]
- Wong, Z.H.; Davenport, M. What Happens after Kasai for Biliary Atresia? A European Multicenter Survey. Eur. J. Pediatr. Surg. 2019, 29, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexopoulos, S.P.; Merrill, M.; Kin, C.; Matsuoka, L.; Dorey, F.; Concepcion, W.; Esquivel, C.; Bonham, A. The impact of hepatic portoenterostomy on liver transplantation for the treatment of biliary atresia: Early failure adversely affects outcome. Pediatr. Transplant. 2012, 16, 373–378. [Google Scholar] [CrossRef]
- Superina, R. Biliary atresia and liver transplantation: Results and thoughts for primary liver transplantation in select patients. Pediatr. Surg. Int. 2017, 33, 1297–1304. [Google Scholar] [CrossRef]
- Kim, H.B.; Elisofon, S.A. Biliary Atresia: Biliary-Enteric Drainage or Primary Liver Transplant? Hepatology 2020, 71, 751–752. [Google Scholar] [CrossRef]
- Goda, S.S.; Khedr, M.A.; Elshenawy, S.Z.; Ibrahim, T.M.; El-Araby, H.A.; Sira, M.M. Preoperative Serum IL-12p40 Is a Potential Predictor of Kasai Portoenterostomy Outcome in Infants with Biliary Atresia. Gastroenterol. Res. Pract. 2017, 2017, 9089068. [Google Scholar] [CrossRef]
- Yassin, N.; El-Tagy, G.; Abdelhakeem, O.N.; Asem, N.; El-Karaksy, H. Predictors of Short-Term Outcome of Kasai Portoenterostomy for Biliary Atresia in Infants: A Single-Center Study. Pediatr. Gastroenterol. Hepatol. Nutr. 2020, 23, 266–275. [Google Scholar] [CrossRef]
- Caruso, M.; Ricciardi, C.; Paoli, G.D.; Di Dato, F.; Donisi, L.; Romeo, V.; Petretta, M.; Iorio, R.; Cesarelli, G.; Brunetti, A.; et al. Machine Learning Evaluation of Biliary Atresia Patients to Predict Long-Term Outcome after the Kasai Procedure. Bioengineering 2021, 8, 152. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.; Lai, J.C. Split-Liver Allocation: An Underused Opportunity to Expand Access to Liver Transplantation. Liver Transplant. 2019, 25, 690–691. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.; Perito, E.R.; Bucuvalas, J.; Gilroy, R.; Hsu, E.K.; Roberts, J.P.; Lai, J.C. Split liver transplantation is utilized infrequently and concentrated at few transplant centers in the United States. Am. J. Transplant. 2020, 20, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Godown, J.; McKane, M.; Wujcik, K.; Mettler, B.A.; Dodd, D.A. Expanding the donor pool: Regional variation in pediatric organ donation rates. Pediatr. Transplant. 2016, 20, 1093–1097. [Google Scholar] [CrossRef]
- Battula, N.R.; Platto, M.; Anbarasan, R.; Perera, M.T.; Ong, E.; Roll, G.R.; Ferraz Neto, B.H.; Mergental, H.; Isaac, J.; Muiesan, P. Intention to split policy: A successful strategy in a combined pediatric and adult liver transplant center. Ann. Surg. 2017, 265, 1009–1015. [Google Scholar] [CrossRef]
- Patroniti, N.; Zangrillo, A.; Pappalardo, F.; Peris, A.; Cianchi, G.; Braschi, A.; Iotti, G.A.; Arcadipane, A.; Panarello, G.; Ranieri, V.M.; et al. The Italian ECMO network experience during the 2009 influenza A(H1N1) pandemic: Preparation for severe respiratory emergency outbreaks. Intensive Care Med. 2011, 37, 1447–1457. [Google Scholar] [CrossRef] [PubMed]
- Benson, C.; Judson, I. Role of expert centres in the management of sarcomas—A UK perspective. Eur. J. Cancer 2014, 50, 1951–1956. [Google Scholar] [CrossRef]
- Congiu, M.E. The Italian National Plan for Rare Diseases. Blood Transfus. 2014, 12, s614–s616. [Google Scholar] [CrossRef]
- Gatta, G.; Botta, L.; Comber, H.; Dimitrova, N.; Leinonen, M.; Pritchard-Jones, K.; Siesling, S.; Trama, A.; Van Eycken, L.; van der Zwan, J.; et al. The European study on centralisation of childhood cancer treatment. Eur. J. Cancer 2019, 115, 120–127. [Google Scholar] [CrossRef]
 ) and a request for a PELD exception or similar priority score (red line) (values in % of all transplants in each center). Center organ sharing/allocation system type (see legend on the right side) are referred to as per the color spot in the figure (blue, green and purple).
) and a request for a PELD exception or similar priority score (red line) (values in % of all transplants in each center). Center organ sharing/allocation system type (see legend on the right side) are referred to as per the color spot in the figure (blue, green and purple).
) and a request for a PELD exception or similar priority score (red line) (values in % of all transplants in each center). Center organ sharing/allocation system type (see legend on the right side) are referred to as per the color spot in the figure (blue, green and purple).
) and a request for a PELD exception or similar priority score (red line) (values in % of all transplants in each center). Center organ sharing/allocation system type (see legend on the right side) are referred to as per the color spot in the figure (blue, green and purple).


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Ville de Goyet, J.; Illhardt, T.; Chardot, C.; Dike, P.N.; Baumann, U.; Brandt, K.; Wildhaber, B.E.; Pakarinen, M.; di Francesco, F.; Sturm, E.; et al. Variability of Care and Access to Transplantation for Children with Biliary Atresia Who Need a Liver Replacement. J. Clin. Med. 2022, 11, 2142. https://doi.org/10.3390/jcm11082142
de Ville de Goyet J, Illhardt T, Chardot C, Dike PN, Baumann U, Brandt K, Wildhaber BE, Pakarinen M, di Francesco F, Sturm E, et al. Variability of Care and Access to Transplantation for Children with Biliary Atresia Who Need a Liver Replacement. Journal of Clinical Medicine. 2022; 11(8):2142. https://doi.org/10.3390/jcm11082142
Chicago/Turabian Stylede Ville de Goyet, Jean, Toni Illhardt, Christophe Chardot, Peace N. Dike, Ulrich Baumann, Katherine Brandt, Barbara E. Wildhaber, Mikko Pakarinen, Fabrizio di Francesco, Ekkehard Sturm, and et al. 2022. "Variability of Care and Access to Transplantation for Children with Biliary Atresia Who Need a Liver Replacement" Journal of Clinical Medicine 11, no. 8: 2142. https://doi.org/10.3390/jcm11082142