
Primary Liver Transplantation vs. Transplant after Kasai Portoenterostomy for Infants with Biliary Atresia


Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Selection, Definitions and Data Collection
2.2. Outcomes
2.3. Statistical Analysis
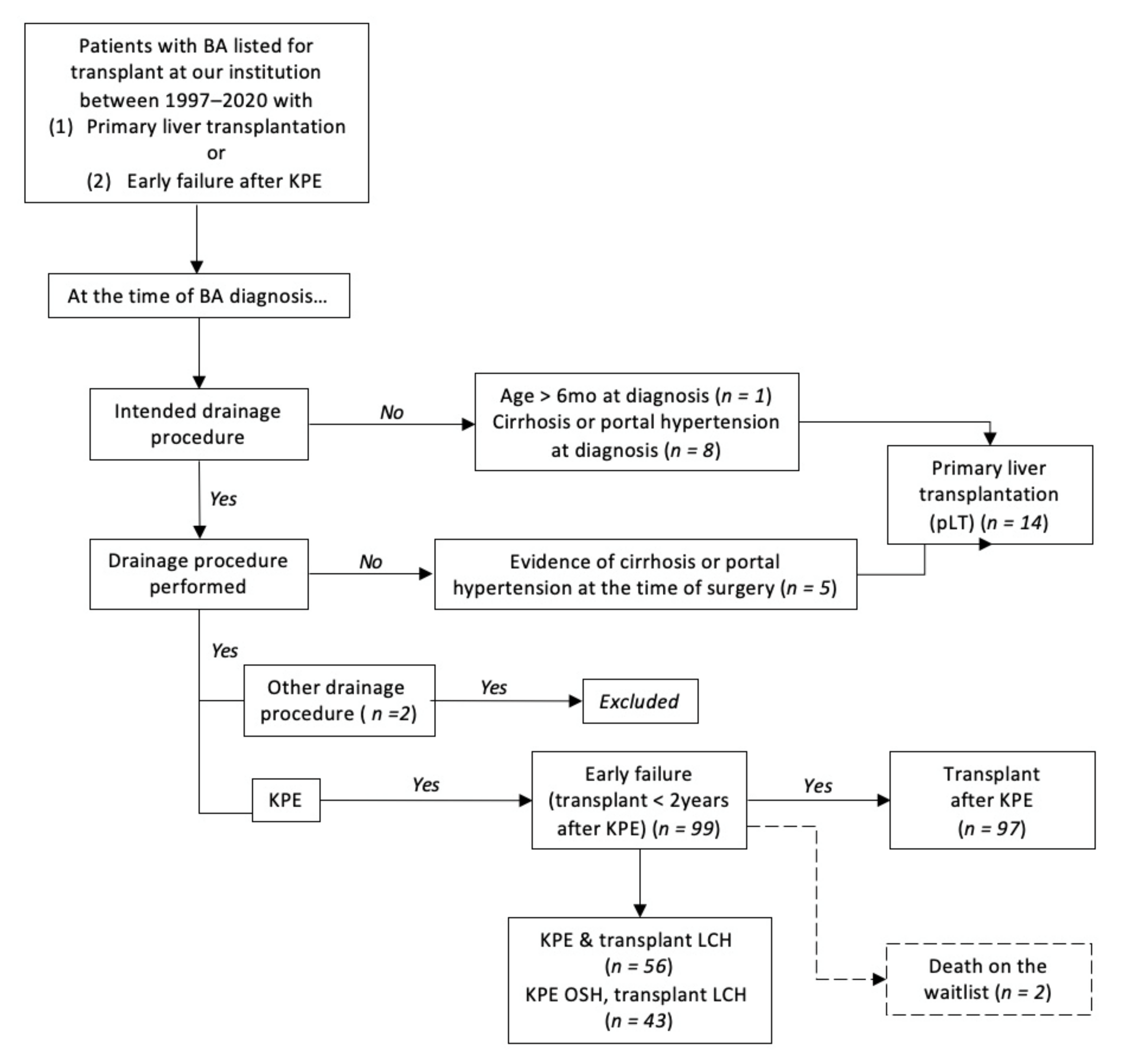
3. Results
3.1. Pre-Transplant Data: Comparison of Patients Transplanted after pLT or KPE
3.2. Transplant and Survival Data: Comparison between pLT and KPE Groups
3.3. Does the Era Make A Difference? Pre-Transplant Comparison of Patients Transplanted after KPE or pLT Based on Early Versus Modern Era
3.4. Transplant and Post-Transplant Survival Data: Comparison of Patients Transplanted after KPE or pLT Based on Era
3.5. Comparison of Patients Transplanted after KPE Based on Era
3.6. Results of pLT: Comparison of Patients Who Received A pLT Based on Era
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BA | Biliary atresia |
| CPI | Consumer price index |
| ESLD | End-stage liver disease |
| ICU | Intensive care unit |
| INR | International normalized ratio |
| IR | Interventional radiology |
| KPE | Kasai portoenterostomy |
| LDLT | Living donor liver transplantation |
| OSH | Outside hospital |
| PELD | Pediatric end-stage liver disease |
| PHIS | Pediatric Health Information System |
| pLT | Primary liver transplantation |
| pRBC | Packed red blood cells |
| USD | United States dollars |
References
- Nizery, L.; Chardot, C.; Sissaoui, S.; Capito, C.; Henrion-Caude, A.; Debray, D.; Girard, M. Biliary atresia: Clinical advances and perspectives. Clin. Res. Hepatol. Gastroenterol. 2016, 40, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Kasai, M.; Suzuki, S. A new operation for “non-correctable” biliary atresia-portoenterostomy. Shijitsu 1959, 13, 733–739. [Google Scholar]
- Shneider, B.L.; Magee, J.C.; Karpen, S.J.; Rand, E.B.; Narkewicz, M.R.; Bass, L.M.; Schwarz, K.; Whitington, P.F.; Bezerra, J.A.; Kerkar, N.; et al. Total Serum Bilirubin within 3 Months of Hepatoportoenterostomy Predicts Short-Term Outcomes in Biliary Atresia. J. Pediatr. 2016, 170, 211–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otte, J.B.; de Ville de Goyet, J.; Reding, R.; Hausleithner, V.; Sokal, E.; Chardot, C.; Debande, B. Sequential treatment of biliary atresia with Kasai portoenterostomy and liver transplantation: A review. Hepatology 1994, 20, 41S–48S. [Google Scholar] [PubMed]
- Davenport, M.; De Ville de Goyet, J.; Stringer, M.D.; Mieli-Vergani, G.; Kelly, D.A.; McClean, P.; Spitz, L. Seamless management of biliary atresia in England and Wales (1999–2002). Lancet 2004, 363, 1354–1357. [Google Scholar] [CrossRef]
- Superina, R.; Magee, J.C.; Brandt, M.L.; Healey, P.J.; Tiao, G.; Ryckman, F.; Karrer, F.M.; Iyer, K.; Fecteau, A.; West, K.; et al. The anatomic pattern of biliary atresia identified at time of Kasai hepatoportoenterostomy and early postoperative clearance of jaundice are significant predictors of transplant-free survival. Ann. Surg. 2011, 254, 577–585. [Google Scholar] [CrossRef]
- Superina, R. Biliary atresia and liver transplantation: Results and thoughts for primary liver transplantation in select patients. Pediatr. Surg. Int. 2017, 33, 1297–1304. [Google Scholar] [CrossRef]
- Wang, P.; Xun, P.; He, K.; Cai, W. Comparison of liver transplantation outcomes in biliary atresia patients with and without prior portoenterostomy: A meta-analysis. Dig. Liver Dis. 2016, 48, 347–352. [Google Scholar] [CrossRef]
- Chardot, C.; Buet, C.; Serinet, M.O.; Golmard, J.L.; Lachaux, A.; Roquelaure, B.; Gottrand, F.; Broue, P.; Dabadie, A.; Gauthier, F.; et al. Improving outcomes of biliary atresia: French national series 1986–2009. J. Hepatol. 2013, 58, 1209–1217. [Google Scholar] [CrossRef]
- LeeVan, E.; Matsuoka, L.; Cao, S.; Groshen, S.; Alexopoulos, S. Biliary-Enteric Drainage vs Primary Liver Transplant as Initial Treatment for Children with Biliary Atresia. JAMA Surg. 2019, 154, 26–32. [Google Scholar] [CrossRef]
- Neto, J.S.; Feier, F.H.; Bierrenbach, A.L.; Toscano, C.M.; Fonseca, E.A.; Pugliese, R.; Candido, H.L.; Benavides, M.R.; Porta, G.; Chapchap, P. Impact of Kasai portoenterostomy on liver transplantation outcomes: A retrospective cohort study of 347 children with biliary atresia. Liver Transplant. 2015, 21, 922–927. [Google Scholar] [CrossRef] [PubMed]
- Sandler, A.D.; Azarow, K.S.; Superina, R.A. The impact of a previous Kasai procedure on liver transplantation for biliary atresia. J. Pediatr. Surg. 1997, 32, 416–419. [Google Scholar] [CrossRef]
- Davenport, M.; Ong, E.; Sharif, K.; Alizai, N.; McClean, P.; Hadzic, N.; Kelly, D.A. Biliary atresia in England and Wales: Results of centralization and new benchmark. J. Pediatr. Surg. 2011, 46, 1689–1694. [Google Scholar] [CrossRef] [PubMed]
- de Vries, W.; de Langen, Z.J.; Groen, H.; Scheenstra, R.; Peeters, P.M.; Hulscher, J.B.; Verkade, H.J.; Netherlands Study Group of Biliary Atresia and Registry. Biliary atresia in the Netherlands: Outcome of patients diagnosed between 1987 and 2008. J. Pediatr. 2012, 160, 638–644.e632. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, R.A.; Barker, C.C.; Roberts, E.A.; Martin, S.R.; Canadian Pediatric Hepatology Research Group. Biliary atresia in Canada: The effect of centre caseload experience on outcome. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Wildhaber, B.E.; Majno, P.; Mayr, J.; Zachariou, Z.; Hohlfeld, J.; Schwoebel, M.; Kistler, W.; Meuli, M.; Le Coultre, C.; Mentha, G.; et al. Biliary atresia: Swiss national study, 1994–2004. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 299–307. [Google Scholar] [CrossRef]
- Leonhardt, J.; Kuebler, J.F.; Leute, P.J.; Turowski, C.; Becker, T.; Pfister, E.D.; Ure, B.; Petersen, C. Biliary atresia: Lessons learned from the voluntary German registry. Eur. J. Pediatr. Surg. 2011, 21, 82–87. [Google Scholar] [CrossRef]
- Alexopoulos, S.P.; Merrill, M.; Kin, C.; Matsuoka, L.; Dorey, F.; Concepcion, W.; Esquivel, C.; Bonham, A. The impact of hepatic portoenterostomy on liver transplantation for the treatment of biliary atresia: Early failure adversely affects outcome. Pediatr. Transplant. 2012, 16, 373–378. [Google Scholar] [CrossRef]
- Nio, M.; Ohi, R.; Miyano, T.; Saeki, M.; Shiraki, K.; Tanaka, K.; Japanese Biliary Atresia Registry. Five- and 10-year survival rates after surgery for biliary atresia: A report from the Japanese Biliary Atresia Registry. J. Pediatr. Surg. 2003, 38, 997–1000. [Google Scholar] [CrossRef]
- Uto, K.; Inomata, Y.; Sakamoto, S.; Hibi, T.; Sasaki, H.; Nio, M. A multicenter study of primary liver transplantation for biliary atresia in Japan. Pediatr. Surg. Int. 2019, 35, 1223–1229. [Google Scholar] [CrossRef]
- Millis, J.M.; Brems, J.J.; Hiatt, J.R.; Klein, A.S.; Ashizawa, T.; Ramming, K.P.; Quinones-Baldrich, W.J.; Busuttil, R.W. Orthotopic liver transplantation for biliary atresia. Evolution of management. Arch. Surg. 1988, 123, 1237–1239. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.P.; Langnas, A.N.; Stratta, R.J.; Pillen, T.J.; Williams, L.; Lindsay, S.; Meiergerd, D.; Shaw, B.W., Jr. Optimal therapy for patients with biliary atresia: Portoenterostomy (“Kasai” procedures) versus primary transplantation. J. Pediatr. Surg. 1990, 25, 153–160. [Google Scholar] [CrossRef]
- Chang, C.H.; Bryce, C.L.; Shneider, B.L.; Yabes, J.G.; Ren, Y.; Zenarosa, G.L.; Tomko, H.; Donnell, D.M.; Squires, R.H.; Roberts, M.S. Accuracy of the Pediatric End-stage Liver Disease Score in Estimating Pretransplant Mortality among Pediatric Liver Transplant Candidates. JAMA Pediatr. 2018, 172, 1070–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S.A.; Venkat, V.; Arnon, R.; Gopalareddy, V.V.; Rosenthal, P.; Erinjeri, J.; Anand, R.; Daniel, J.F.; Society of Pediatric Liver Transplantation. Improved Outcomes for Liver Transplantation in Patients with Biliary Atresia Since Pediatric End-Stage Liver Disease Implementation: Analysis of the Society of Pediatric Liver Transplantation Registry. J. Pediatr. 2020, 219, 89–97. [Google Scholar] [CrossRef]
- Cowles, R.A.; Lobritto, S.J.; Ventura, K.A.; Harren, P.A.; Gelbard, R.; Emond, J.C.; Altman, R.P.; Jan, D.M. Timing of liver transplantation in biliary atresia-results in 71 children managed by a multidisciplinary team. J. Pediatr. Surg. 2008, 43, 1605–1609. [Google Scholar] [CrossRef]
- Tiao, M.M.; Yang, C.Y.; Tsai, S.S.; Chen, C.L.; Kuo, H.W. Liver transplantation for biliary atresia in Taiwan: A national study. Transplant. Proc. 2008, 40, 3569–3570. [Google Scholar] [CrossRef]
- Kim, H.B.; Elisofon, S.A. Biliary Atresia: Biliary-Enteric Drainage or Primary Liver Transplant? Hepatology 2020, 71, 751–752. [Google Scholar] [CrossRef]
- Azarow, K.S.; Phillips, M.J.; Sandler, A.D.; Hagerstrand, I.; Superina, R.A. Biliary atresia: Should all patients undergo a portoenterostomy? J. Pediatr. Surg. 1997, 32, 168–172, discussion 172–164. [Google Scholar] [CrossRef]
- Kwong, A.J.; Kim, W.R.; Lake, J.R.; Smith, J.M.; Schladt, D.P.; Skeans, M.A.; Noreen, S.M.; Foutz, J.; Booker, S.E.; Cafarella, M.; et al. OPTN/SRTR 2019 Annual Data Report: Liver. Am. J. Transplant. 2021, 21 (Suppl. 2), 208–315. [Google Scholar] [CrossRef]
- Battula, N.R.; Platto, M.; Anbarasan, R.; Perera, M.T.; Ong, E.; Roll, G.R.; Ferraz Neto, B.H.; Mergental, H.; Isaac, J.; Muiesan, P.; et al. Intention to Split Policy: A Successful Strategy in a Combined Pediatric and Adult Liver Transplant Center. Ann. Surg. 2017, 265, 1009–1015. [Google Scholar] [CrossRef]
- Ebel, N.H.; Hsu, E.K.; Dick, A.A.S.; Shaffer, M.L.; Carlin, K.; Horslen, S.P. Decreased Incidence of Hepatic Artery Thrombosis in Pediatric Liver Transplantation Using Technical Variant Grafts: Report of the Society of Pediatric Liver Transplantation Experience. J. Pediatr. 2020, 226, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Egawa, H.; Oike, F.; Buhler, L.; Shapiro, A.M.; Minamiguchi, S.; Haga, H.; Uryuhara, K.; Kiuchi, T.; Kaihara, S.; Tanaka, K. Impact of recipient age on outcome of ABO-incompatible living-donor liver transplantation. Transplantation 2004, 77, 403–411. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | KPE (n = 99) | pLT (n = 14) | p Value |
|---|---|---|---|
| Age at KPE or diagnosis BA (days) (mean ± sd) | 67.1 ± 25.5 | 141.5 ± 46.0 | <0.001 * |
| Time to listing (days) (mean ± sd) | 140.8 ± 102.8 | 44.5 ± 44.7 | 0.001 * |
| Waitlist time (days) (mean ± sd) | 105.6 ± 102.8 | 90.8 ± 66.5 | 0.6 |
| Hospital admissions while on waitlist (n, mean ± sd) | 3.2 ± 3.3 | 2.6 ± 2.4 | 0.58 |
| Days admitted while on waitlist (mean ± sd) | 24.9 ± 31.2 | 22.4 ± 17.6 | 0.78 |
| Adjusted cost of hospital admissions on the waitlist ‡ (median (IQR)) | 425,090.00 (285,282.83, 566,405.40) | 253,004.10 (95,640.49, 431,530.70) | 0.07 |
| Admission on the waitlist (n, %): Cholangitis | 31 (31.3) | 0 | 0.014 * |
| Admission on the waitlist (n, %): Infections (other than cholangitis) | 41 (41.4) | 6 (42.9) | 0.92 |
| Admission on the waitlist (n, %): Gastrointestinal bleeding | 20 (20.2) | 2 (14.3) | 0.6 |
| Admission on the waitlist (n, %): Ascites or Spontaneous bacterial peritonitis | 25 (25.3) | 5 (35.7) | 0.41 |
| Admission on the waitlist (n, %): Malnutrition | 24 (24.2) | 4 (28.6) | 0.73 |
| Death on the waitlist (yes) (n, %) | 2 (2.0) | 0 | 0.59 |
| Variables | KPE (n = 97) | pLT (n = 14) | p Value |
|---|---|---|---|
| Age at transplant (days) (mean ± sd) | 311.4 ± 144.0 | 287.0 ± 82.7 | 0.54 |
| Calculated PELD score at transplant (mean ± sd) | 22 ± 11 | 27 ± 8 | 0.15 |
| Type of donor (LDLT) (n, %) | 39 (40.2) | 4 (28.6) | 0.4 |
| Transplant surgery duration (minutes) (mean ± sd) | 443.9 ± 98.6 | 423.1 ± 70.0 | 0.39 |
| Intraoperative pRBC transfusion (cc/kg) (mean ± sd) | 143.9 ± 122.3 | 136.1 ± 137.2 | 0.83 |
| Duration of mechanical ventilation (days) (mean ± sd) | 7.5 ± 6.6 | 9.8 ± 9.1 | 0.27 |
| Length of ICU stay (days) (mean ± sd) | 14.2 ± 25.6 | 14.2 ± 10.5 | 1 |
| Length of hospital stay (days) (mean ± sd) | 31.8 ± 36.0 | 32.8 ± 15.2 | 0.92 |
| Return to ICU after transplant (n, %) | 15 (15.5) | 5 (35.7) | 0.065 |
| Surgical take back post-transplant (mean ± sd) | 0.7 ± 1.1 | 1.0 ± 1.0 | 0.31 |
| Adjusted cost of transplant admission (median (IQR)) | 588,887.00 (466,829.20, 902,360.70) | 932,675.30 (668,937.90, 1,120,433.90) | 0.098 |
| Retransplant (yes) (n, %) | 8 (8.2) | 2 (14.3) | 0.46 |
| 1-year patient survival from list date (n, %) | 93 (93.9) | 14 (100.0) | 0.35 |
| 1-year post-transplant patient survival (n, %) | 91 (93.8) | 14 (100.0) | 0.35 |
| 3-year post-transplant patient survival (n, %) | 88 (90.7) | 13 (92.9) | 0.8 |
| 1-year post-transplant graft survival (n, %) | 88 (90.7) | 13 (92.9) | 0.78 |
| 3-year post-transplant graft survival (n, %) | 86 (88.7) | 12 (85.7) | 0.78 |
| Early Era (1997–2008) | Modern Era (2009–2020) | |||||
|---|---|---|---|---|---|---|
| Variables | KPE (n = 51) | pLT (n = 5) | p value | KPE (n = 48) | pLT (n = 9) | p Value |
| Age at KPE or diagnosis BA (days) (mean ± sd) | 67.9 ± 23.3 | 139.4 ± 71.7 | <0.001 * | 66.1 ± 27.9 | 127.9 ± 37.2 | <0.001 * |
| Time to listing (days) (mean ± sd) | 112.1 ± 95.6 | 63.8 ± 69.3 | 0.28 | 171.5 ± 110.7 | 48.6 ± 40.3 | 0.002 * |
| Waitlist time (days) (mean ± sd) | 117.8 ± 121.9 | 130.0 ± 83.1 | 0.83 | 92.6 ± 76.7 | 69.0 ± 47.4 | 0.38 |
| Number of hospital admissions while on waitlist (n, mean ± sd) | 2.8 ± 3.3 | 2.0 ± 2.0 | 0.61 | 3.6 ± 3.4 | 3 ± 2.4 | 0.62 |
| Number of days admitted while on waitlist (mean ± sd) | 23.1 ± 34.0 | 22.8 ± 23.9 | 0.99 | 26.1 ± 28.3 | 19.7 ± 16.0 | 0.53 |
| Admission on the waitlist (n, %): Cholangitis | 15 (29.4) | 0 | 0.16 | 16 (33.3) | 0 | 0.041 * |
| Admission on the waitlist (n, %): Infections (other than cholangitis) | 20 (39.2) | 3 (60.0) | 0.37 | 21 (43.8) | 3 (33.3) | 0.56 |
| Admission on the waitlist (n, %): Gastrointestinal bleeding | 11 (21.6) | 0 (0) | 0.25 | 9 (18.8) | 3 (33.3) | 0.81 |
| Admission on the waitlist (n, %): Ascites or Spontaneous bacterial peritonitis | 10 (19.6) | 1 (20.0) | 0.98 | 14 (29.2) | 4 (44.4) | 0.37 |
| Admission on the waitlist (n, %): Malnutrition | 5 (9.8) | 0 (0) | 0.46 | 19 (39.6) | 4 (44.4) | 0.79 |
| Death on the waitlist (n, %) | 0 (0) | 0 | — | 2 (4.2) | 0 | 0.53 |
| Early Era (1997–2008) | Modern Era (2009–2020) | |||||
|---|---|---|---|---|---|---|
| Variables | KPE (n = 51) | pLT (n = 5) | p Value | KPE (n = 46) | pLT (n = 9) | p Value |
| Age at transplant (days) (mean ± sd) | 297.9 ± 144.0 | 333.2 ± 98.6 | 0.6 | 326.4 ± 144.2 | 261.3 ± 64.6 | 0.19 |
| Calculated PELD score at transplant (mean ± sd) | 17 ± 9 | 18 ± 0 | 0.78 | 16 ± 8 | 23 ± 8 | 0.022 * |
| Type of donor (LDLT) (n, %) | 25 (49.0) | 1 (20.0) | 0.21 | 14 (30.4) | 3 (33.3) | 0.86 |
| OR duration (minutes) (mean ± sd) | 467.8 ± 89.3 | 451.2 ± 76.9 | 0.69 | 417.4 ± 74.7 | 407.4 ± 64.3 | 0.71 |
| Intraoperative pRBC transfusion (cc/kg) (mean ± sd) | 162.7 ± 142.1 | 156.7 ± 176.4 | 0.93 | 123.1 ± 92.9 | 124.7 ± 120.9 | 0.96 |
| Days on the ventilator (days) (mean ± sd) | 7.3 ± 6.4 | 2.0 ± 2.0 | 0.64 | 7.7 ± 6.8 | 12.3 ± 9.2 | 0.085 |
| Length of ICU stay (days) (mean ± sd) | 15.0 ± 34.1 | 7.0 ± 2.3 | 0.67 | 13.3 ± 10.2 | 17.6 ± 11.1 | 0.27 |
| Length of hospital stay (days) (mean ± sd) | 32.9 ± 40.1 | 24.3 ± 18.1 | 0.1 | 30.7 ± 31.5 | 34.7 ± 13.9 | 0.32 |
| Return to ICU after transplant (n, %) | 8 (15.7) | 3 (60.0) | 0.017 * | 7 (15.2) | 3 (33.3) | 0.2 |
| Retransplant (n, %) | 8 (15.7) | 2 (40.0) | 0.18 | 1 (2.2) | 0 (0) | 0.66 |
| 1-year patient survival from list date (n, %) | 48 (94.1) | 5 (100.0) | 0.58 | 45 (93.8) | 9 (100.0) | 0.45 |
| 1-year post-transplant patient survival (n, %) | 46 (90.2) | 5 (100.0) | 0.48 | 45 (97.8) | 9 (100.0) | 0.66 |
| 3-year post-transplant patient survival (n, %) | 44 (86.3) | 5 (100.0) | 0.39 | 44 (95.7) | 8 (88.9) | 0.4 |
| 1-year post-transplant graft survival (n, %) | 43 (84.3) | 4 (80.0) | 0.86 | 45 (97.8) | 9 (100.0) | 0.66 |
| 3-year post-transplant graft survival (n, %) | 42 (82.4) | 4 (80.0) | 0.94 | 44 (95.7) | 8 (88.9) | 0.4 |
| KPE | |||
|---|---|---|---|
| Variables | Early Era (1997–2008) (n = 51) | Modern Era (2009–2020) (n = 48) | p Value |
| Age at KPE (days) (mean ± sd) | 67.9 ± 23.3 | 66.1 ± 27.9 | 0.73 |
| Time to listing (days) (mean ± sd) | 112.1 ± 95.6 | 171.5 ± 110.7 | 0.005 * |
| Waitlist time (days) (mean ± sd) | 117.8 ± 121.9 | 92.6 ± 76.7 | 0.22 |
| Number of hospital admissions while on waitlist (mean ± sd) | 2.7 ± 3.3 | 2.0 ± 2.0 | 0.17 |
| Number of days admitted while on waitlist (mean ± sd) | 23.1 ± 34.0 | 26.1 ± 28.3 | 0.64 |
| Admission on the waitlist (n, %): Cholangitis | 15 (29.4) | 16 (33.3) | 0.67 |
| Admission on the waitlist (n, %): Infections (other than cholangitis) | 20 (39.2) | 21 (43.8) | 0.65 |
| Admission on the waitlist (n, %): Gastrointestinal bleeding | 11 (21.6) | 9 (18.8) | 0.73 |
| Admission on the waitlist (n, %): Ascites or Spontaneous bacterial peritonitis | 10 (19.6) | 14 (29.2) | 0.27 |
| Admission on the waitlist (n, %): Malnutrition | 5 (9.8) | 19 (39.6) | 0.001 * |
| Death on the waitlist (n, %) | 0 (0) | 2 (4.2) | 0.14 |
| KPE | |||
|---|---|---|---|
| Variables | Early Era (1997–2008) (n = 51) | Modern Era (2009–2020) (n = 46) | p Value |
| Age at transplant (days) (mean ± sd) | 297.9 ± 144.0 | 326.4 ± 144.2 | 0.21 |
| Calculated PELD score at transplant (mean ± sd) | 17 ± 9 | 16 ± 8 | 0.46 |
| Type of donor (LDLT) (n, %) | 25 (49.0) | 14 (30.4) | 0.06 |
| OR duration (minutes) (mean ± sd) | 467.8 ± 89.3 | 417.4 ± 74.7 | 0.005 * |
| Intraoperative pRBC transfusion (cc/kg) (mean ± sd) | 162.7 ± 142.1 | 123.1 ± 92.9 | 0.11 |
| Days on the ventilator (days) (mean ± sd) | 7.3 ± 6.4 | 7.7 ± 6.8 | 0.84 |
| Length of ICU stay (days) (mean ± sd) | 15.0 ± 34.1 | 13.3 ± 10.2 | 0.73 |
| Length of hospital stay (days) (mean ± sd) | 32.9 ± 40.1 | 30.7 ± 31.5 | 0.73 |
| Return to ICU after transplant (n, %) | 8 (15.7) | 7 (15.2) | 0.95 |
| Retransplant (n, %) | 8 (15.7) | 1 (2.2) | 0.022 * |
| 1-year patient survival from list date (n, %) | 48 (94.1) | 45 (93.8) | 0.94 |
| 1-year post-transplant patient survival (n, %) | 46 (90.2) | 45 (97.8) | 0.13 |
| 3-year post-transplant patient survival (n, %) | 44 (86.3) | 44 (95.7) | 0.13 |
| 1-year graft survival (n, %) | 43 (84.3) | 45 (97.8) | 0.025 * |
| 3-year graft survival (n, %) | 42 (82.4) | 44 (95.7) | 0.044 * |
| pLT | |||
|---|---|---|---|
| Variables | Early Era (1997–2008) (n = 5) | Modern Era (2009–2020) (n = 9) | p Value |
| Age at diagnosis BA (days) (mean ± sd) | 139.4 ± 71.7 | 127.9 ± 37.2 | 0.70 |
| Time to listing (days) (mean ± sd) | 63.8 ± 69.3 | 48.6 ± 40.3 | 0.61 |
| Waitlist time (days) (mean ± sd) | 130.0 ± 83.1 | 69.0 ± 47.4 | 0.10 |
| Number of hospital admissions while on waitlist (mean ± sd) | 3.6 ± 3.4 | 3 ± 2.4 | 0.45 |
| Number of days admitted while on waitlist (mean ± sd) | 22.8 ± 23.9 | 19.8 ± 16.0 | 0.79 |
| Admission on the waitlist (n, %): Cholangitis | 0 | 0 | — |
| Admission on the waitlist (n, %): Infections (other than cholangitis) | 3 (60.0) | 3 (33.3) | 0.33 |
| Admission on the waitlist (n, %): Gastrointestinal bleeding | 0 (0) | 3 (33.3) | 0.15 |
| Admission on the waitlist (n, %): Ascites or Spontaneous bacterial peritonitis | 1 (20.0) | 4 (44.4) | 0.36 |
| Admission on the waitlist (n, %): Malnutrition | 0 (0) | 4 (44.4) | 0.078 |
| Death on the waitlist (n, %) | 0 | 0 | — |
| pLT | |||
|---|---|---|---|
| Variables | Early Era (1997–2008) (n = 5) | Modern Era (2009–2020) (n = 9) | p Value |
| Age at transplant (days) (mean ± sd) | 333.2 ± 98.6 | 261.3 ± 64.6 | 0.12 |
| Calculated PELD score at transplant (mean ± sd) | 18 ± 0 | 23 ± 8 | 0.18 |
| Type of donor (LDLT) (n, %) | 1 (20.0) | 3 (33.3) | 0.60 |
| OR duration (minutes) (mean ± sd) | 451.2 ± 76.9 | 407.4 ± 64.3 | 0.28 |
| Intraoperative pRBC transfusion (cc/kg) (mean ± sd) | 156.7 ± 176.4 | 124.7 ± 120.8 | 0.69 |
| Days on the ventilator (days) (mean ± sd) | 2.0 ± 2.0 | 12.3 ± 9.2 | 0.099 |
| Length of ICU stay (days) (mean ± sd) | 7.0 ± 2.3 | 17.6 ± 11.1 | 0.12 |
| Length of hospital stay (days) (mean ± sd) | 24.3 ± 18.1 | 34.7 ± 13.9 | 0.28 |
| Return to ICU after transplant (n, %) | 3 (60.0) | 3 (33.3) | 0.33 |
| Retransplant (n, %) | 2 (40.0) | 0 (0) | 0.04 * |
| 1-year patient survival from list date (n, %) | 5 (100.0) | 9 (100.0) | – |
| 1-year post-transplant patient survival (n, %) | 5 (100.0) | 9 (100.0) | – |
| 3-year post-transplant patient survival (n, %) | 5 (100.0) | 8 (88.9) | 0.40 |
| 1-year post-transplant graft survival (n, %) | 4 (80.0) | 9 (100.0) | 0.18 |
| 3-year post-transplant graft survival (n, %) | 4 (80.0) | 8 (88.9) | 0.68 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lemoine, C.P.; LeShock, J.P.; Brandt, K.A.; Superina, R. Primary Liver Transplantation vs. Transplant after Kasai Portoenterostomy for Infants with Biliary Atresia. J. Clin. Med. 2022, 11, 3012. https://doi.org/10.3390/jcm11113012
Lemoine CP, LeShock JP, Brandt KA, Superina R. Primary Liver Transplantation vs. Transplant after Kasai Portoenterostomy for Infants with Biliary Atresia. Journal of Clinical Medicine. 2022; 11(11):3012. https://doi.org/10.3390/jcm11113012
Chicago/Turabian StyleLemoine, Caroline P., John P. LeShock, Katherine A. Brandt, and Riccardo Superina. 2022. "Primary Liver Transplantation vs. Transplant after Kasai Portoenterostomy for Infants with Biliary Atresia" Journal of Clinical Medicine 11, no. 11: 3012. https://doi.org/10.3390/jcm11113012