
Perioperative Supplemental Oxygen and Postoperative Copeptin Concentrations in Cardiac-Risk Patients Undergoing Major Abdominal Surgery—A Secondary Analysis of a Randomized Clinical Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
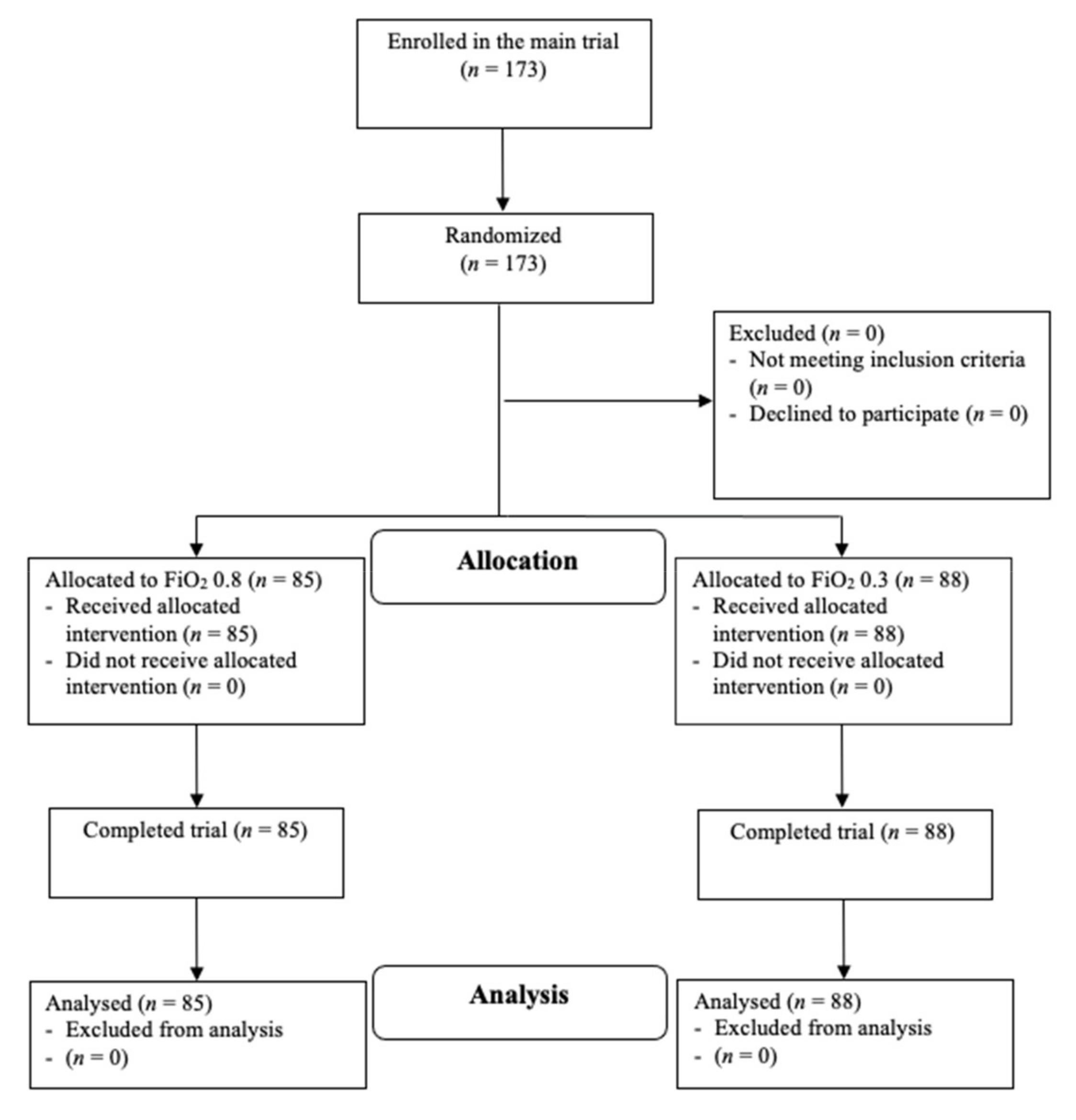
2.1. Study Design
2.2. Randomisation
2.3. Statistical Analysis
2.4. Post-Hoc Analysis
2.5. Sample Size Considerations
3. Results
3.1. Primary Outcome
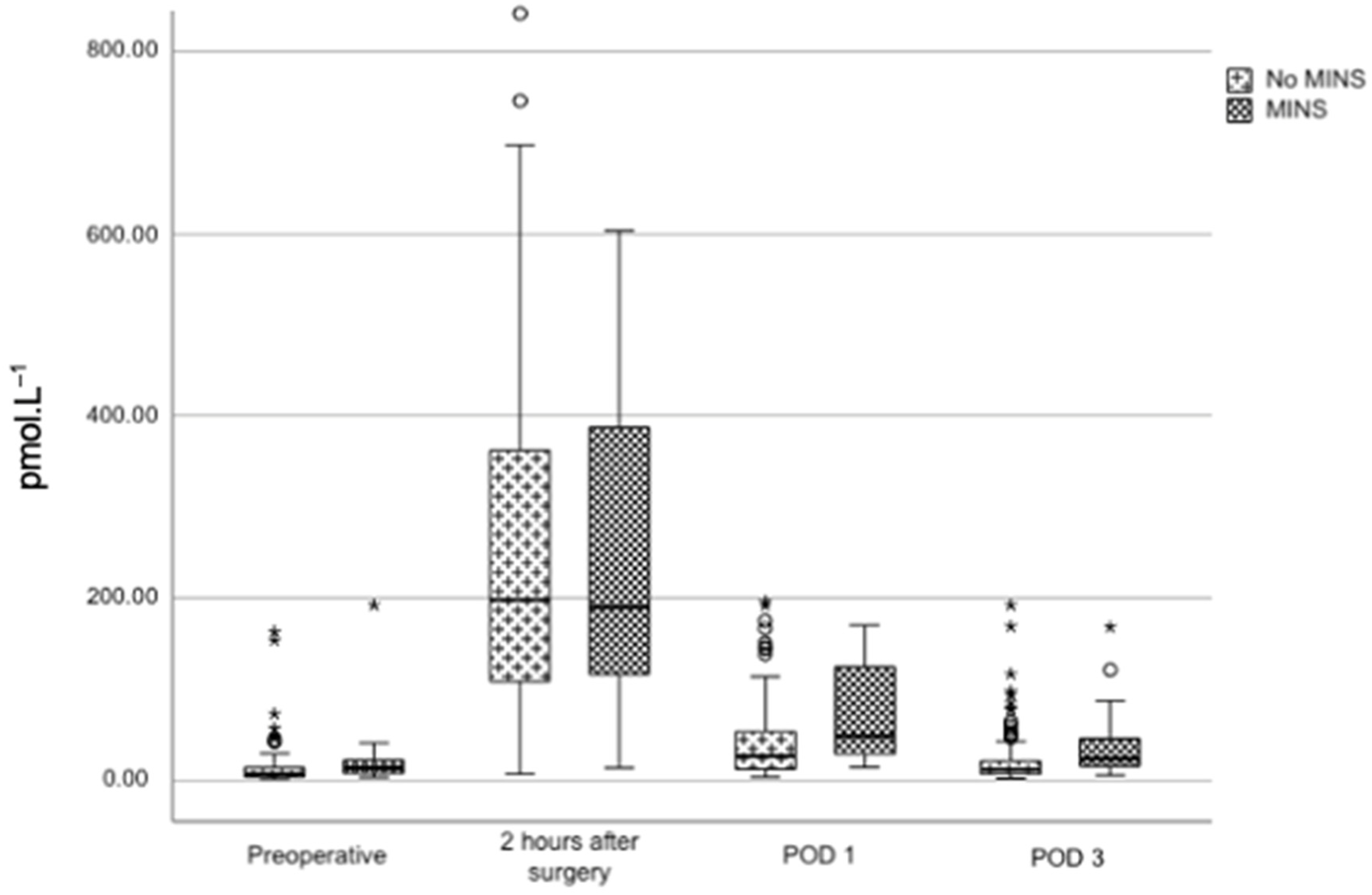
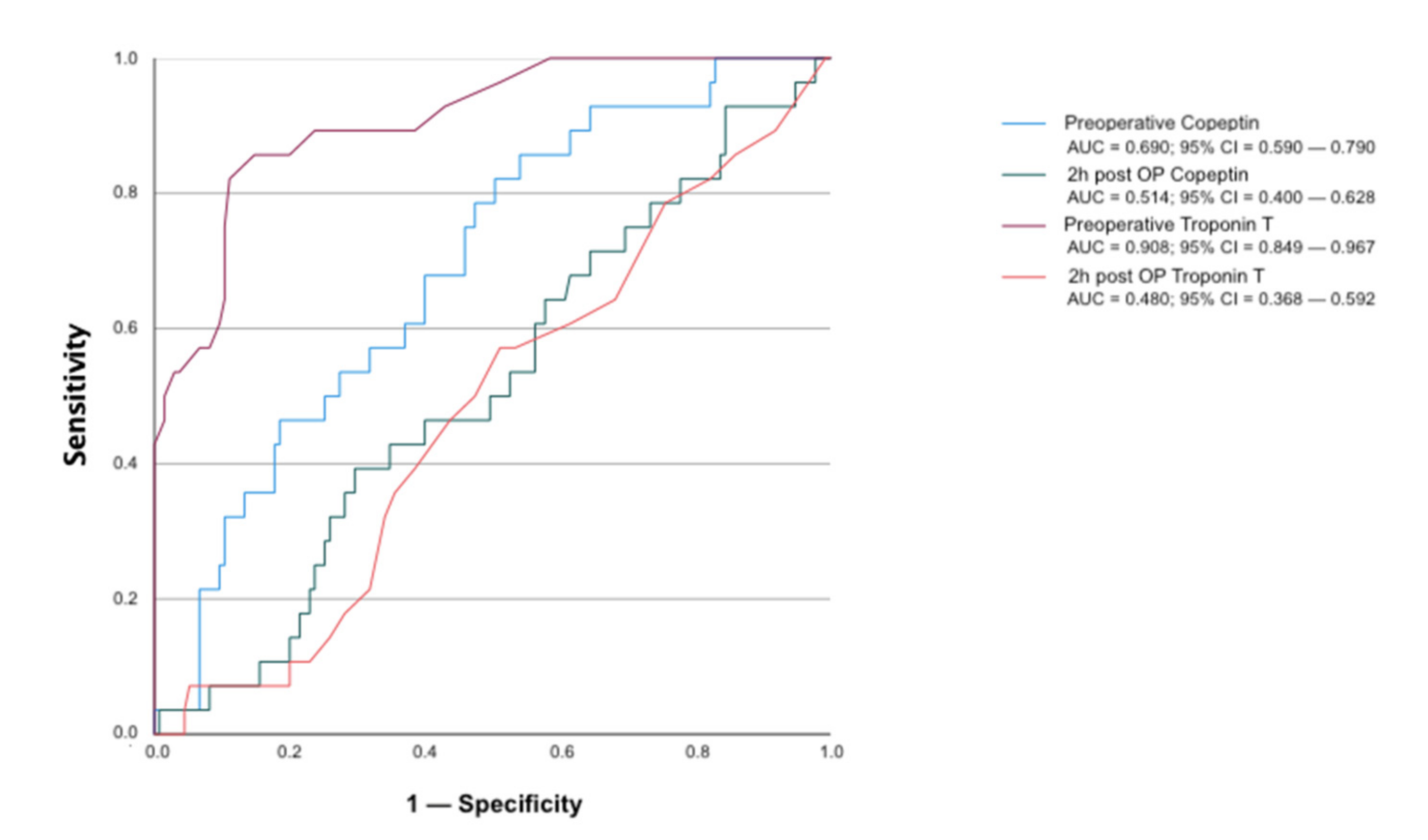
3.2. Post-Hoc Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Comparison | Effect | Lower CI | Upper CI | p-Value |
|---|---|---|---|---|---|
| Time × OP Type | Overall Interaction Test | <0.001 | |||
| Laparoscopic vs. Open: 2 h post—pre | −100.940 | −147.280 | −54.589 | <0.001 | |
| Laparoscopic vs. Open: POD 1—pre | −12.263 | −59.370 | 34.845 | 0.609 | |
| Laparoscopic vs. Open: POD 3—pre | −10.150 | −58.725 | 38.425 | 0.682 | |
| Laparoscopic vs. Open: pre | −1.973 | −37.623 | 33.676 | 0.914 | |
| Laparoscopic vs. Open: 2 h post | −102.910 | −138.100 | −67.715 | <0.001 | |
| Laparoscopic vs. Open: POD 1 | −14.236 | −50.421 | 21.949 | 0.440 | |
| Laparoscopic vs. Open: POD 3 | −12.123 | −50.204 | 25.957 | 0.532 | |
| Laparoscopic: pre vs. 2 h post | −176.100 | −213.39 | −138.810 | <0.001 | |
| Laparoscopic: pre vs. POD 1 | −27.172 | −65.203 | 10.859 | 0.161 | |
| Laparoscopic: pre vs. POD 3 | −1.508 | −41.303 | 38.287 | 0.941 | |
| Open: pre vs. 2 h post | −277.030 | −304.550 | −249.520 | <0.001 | |
| Open: pre vs. POD 1 | −39.435 | −67.232 | −11.637 | 0.006 | |
| Open: pre vs. POD 3 | −11.658 | −39.512 | 16.197 | 0.411 |



References
- Weiser, T.G.; Haynes, A.B.; Molina, G.; Lipsitz, S.R.; Esquivel, M.M.; Uribe-Leitz, T.; Fu, R.; Azad, T.; Chao, T.E.; Berry, W.R.; et al. Estimate of the global volume of surgery in 2012: An assessment supporting improved health outcomes. Lancet 2015, 385, S11. [Google Scholar] [CrossRef]
- Devereaux, P.J.; Duceppe, E.; Guyatt, G.; Tandon, V.; Rodseth, R.; Biccard, B.M.; Xavier, D.; Szczeklik, W.; Meyhoff, C.S.; Vincent, J.; et al. Association of postoperative high-sensitivity troponin levels with myocardial injury and 30-day mortality among patients undergoing noncardiac surgery. JAMA-J. Am. Med. Assoc. 2017, 317, 1642–1651. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Gupta, N.; Ramakrishna, H.; Guo, Y.; Berger, J.S.; Bangalore, S. Perioperative major adverse cardiovascular and cerebrovascular events associated with noncardiac surgery. JAMA Cardiol. 2017, 2, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Turan, A.; Chang, C.; Cohen, B.; Saasouh, W.; Essber, H.; Yang, D.; Ma, C.; Hovsepyan, K.; Khanna, A.K.; Vitale, J.; et al. Incidence, Severity, and Detection of Blood Pressure Perturbations after Abdominal Surgery—A prospective blinded observational study. Anesthesiology 2019, 130, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Shoemaker, W.C.; Appel, P.L.; Kram, H.B. Tissue oxygen debt as a determinant of lethal and nonlethal postoperative organ failure. Crit. Care Med. 1988, 16, 1117–1120. [Google Scholar] [CrossRef] [PubMed]
- Chernow, B.; Alexander, H.R.; Smallridge, R.C.; Thompson, W.R.; Cook, D.; Beardsley, D.; Fink, M.P.; Lake, C.R.; Fletcher, J.R. Hormonal Responses to Graded Surgical Stress. Arch. Intern. Med. 1987, 147, 1273–1278. [Google Scholar] [CrossRef]
- Parker, S.D.; Breslow, M.J.; Frank, S.M.; Rosenfeld, B.A.; Norris, E.J.; Christopherson, R.; Rock, P.; Gottlieb, S.O.; Raff, H.; Perler, B.A.; et al. Catecholamine and cortisol responses to lower extremity revascularization: Correlation with outcome variables. Perioperative Ischemia Randomized Anesthesia Trial Study Group. Crit. Care Med. 1995, 23, 1954–1961. [Google Scholar] [CrossRef]
- Devereaux, P.J.; Yang, H.; Yusuf, S.W.; Guyatt, G.H.; Leslie, K.; Villar, J.C.; Xavier, D.; Chrolavicius, S.; Greenspan, L.; Pogue, J.; et al. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): A randomised controlled trial. Lancet 2008, 371, 1839–1847. [Google Scholar] [CrossRef] [Green Version]
- Devereaux, P.J.; Szczeklik, W. Myocardial injury after non-cardiac surgery: Diagnosis and management. Eur. Heart J. 2019, 41, 3083–3091. [Google Scholar] [CrossRef]
- Gill, N.P.; Wright, B.; Reilly, C.S. Relationship between hypoxaemic and cardiac ischaemic events in the perioperative period. Br. J. Anaesth. 1992, 68, 471–473. [Google Scholar] [CrossRef]
- Mauermann, E.; Bolliger, D.; Seeberger, E.; Puelacher, C.; Corbiere, S.; Filipovic, M.; Seeberger, M.; Mueller, C.; Buse, G.L. Incremental value of preoperative copeptin for predicting myocardial injury. Anesth. Analg. 2016, 123, 1363–1371. [Google Scholar] [CrossRef] [PubMed]
- Lipinski, M.J.; Escárcega, R.O.; D’Ascenzo, F.; Magalhães, M.A.; Baker, N.C.; Torguson, R.; Chen, F.; Epstein, S.E.; Miró, O.; Llorens, P.; et al. A systematic review and collaborative meta-analysis to determine the incremental value of copeptin for rapid rule-out of acute myocardial infarction. Am. J. Cardiol. 2014, 113, 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Christ-Crain, M. Vasopressin and Copeptin in health and disease. Rev. Endocr. Metab. Disord. 2019, 20, 283–294. [Google Scholar] [CrossRef]
- Balanescu, S.; Kopp, P.; Gaskill, M.B.; Morgenthaler, N.G.; Schindler, C.; Rutishauser, J. Correlation of plasma copeptin and vasopressin concentrations in hypo-, iso-, and hyper-osmolar states. J. Clin. Endocrinol. Metab. 2011, 96, 1046–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolignano, D.; Cabassi, A.; Fiaccadori, E.; Ghigo, E.; Pasquali, R.; Peracino, A.; Peri, A.; Plebani, M.; Santoro, A.; Settanni, F.; et al. Copeptin (CTproAVP), a new tool for understanding the role of vasopressin in pathophysiology. Clin. Chem. Lab. Med. 2014, 52, 1447–1456. [Google Scholar] [CrossRef] [PubMed]
- Nickel, C.H.; Bingisser, R.; Morgenthaler, N.G. The role of copeptin as a diagnostic and prognostic biomarker for risk stratification in the emergency department. BMC Med. 2012, 10, 7. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.Q.; Dhillon, O.S.; O’Brien, R.J.; Struck, J.; Quinn, P.A.; Morgenthaler, N.G.; Squire, I.B.; Davies, J.E.; Bergmann, A.; Ng, L. C-terminal provasopressin (copeptin) as a novel and prognostic marker in acute myocardial infarction: Leicester acute myocardial infarction peptide (LAMP) study. Circulation 2007, 115, 2103–2110. [Google Scholar] [CrossRef] [Green Version]
- Alehagen, U.; Dahlström, U.; Rehfeld, J.F.; Goetze, J.P. Association of copeptin and N-terminal proBNP concentrations with risk of cardiovascular death in older patients with symptoms of heart failure. JAMA-J. Am. Med. Assoc. 2011, 305, 2088–2095. [Google Scholar] [CrossRef] [Green Version]
- Morgenthaler, N.G.; Müller, B.; Struck, J.; Bergmann, A.; Redl, H.; Christ-Crain, M. Copeptin, a stable peptide of the arginine vasopressin precursor, is elevated in hemorrhagic and septic shock. Shock 2007, 28, 219–226. [Google Scholar] [CrossRef]
- Reiterer, C.; Kabon, B.; Von Sonnenburg, M.F.; Starlinger, P.; Taschner, A.; Zotti, O.; Goshin, J.; Drlicek, G.; Fleischmann, E. The effect of supplemental oxygen on perioperative brain natriuretic peptide concentration in cardiac risk patients—A protocol for a prosprective randomized clinical trial. Trials 2020, 21, 400. [Google Scholar] [CrossRef]
- Reiterer, C.; Kabon, B.; Taschner, A.; von Sonnenburg, M.F.; Graf, A.; Adamowitsch, N.; Starlinger, P.; Goshin, J.; Fraunschiel, M.; Fleischmann, E. Perioperative supplemental oxygen and NT-proBNP concentrations after major abdominal surgery—A prospective randomized clinical trial. J. Clin. Anesth. 2021, 73, 110379. [Google Scholar] [CrossRef] [PubMed]
- Gan, T.J.; Sooitt, A.; Maroof, M.; El-Moalem, H.; Robertson, K.M.; Moretti, E.; Dwane, P.; Glass, P.S.A. Goal-directed intraoperative fluid administration reduces length of hospital stay after major surgery. Anesthesiology 2002, 97, 820–826. [Google Scholar] [CrossRef]
- Feldheiser, A.; Conroy, P.; Bonomo, T.; Cox, B.; Garces, T.R.; Spies, C.; Anaesthesia Working Group of the Enhanced Recovery after Surgery (ERAS®) Society. Development and feasibility study of an algorithm for intraoperative goaldirected haemodynamic management in noncardiac surgery. J. Int. Med. Res. 2012, 40, 1227–1241. [Google Scholar] [CrossRef] [PubMed]
- Spence, J.; LeManach, Y.; Chan, M.T.; Wang, C.Y.; Sigamani, A.; Xavier, D.; Pearse, R.; Alonso-Coello, P.; Garutti, I.; Srinathan, S.K.; et al. Myocardial injury after noncardiac surgery: A large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology 2014, 120, 564–578. [Google Scholar] [CrossRef]
- Kamber, F.; Mauermann, E.; Seeberger, E.; Guerke, L.; Mueller, C.; Bolliger, D.; Buse, G.A.L. Peri-operative copeptin concentrations and their association with myocardial injury after vascular surgery: A prospective observational cohort study. Eur. J. Anaesthesiol. 2018, 35, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2011, 9, 672–677. [Google Scholar] [CrossRef] [Green Version]
- Staniforth, A.D.; Kinnear, W.J.M.; Starling, R.; Hetmanski, D.J.; Cowley, A.J. Effect of oxygen on sleep quality, cognitive function and sympathetic activity in patients with chronic heart failure and Cheyn-Stokes respiration. Eur. Heart J. 1998, 19, 922–928. [Google Scholar] [CrossRef] [Green Version]
- Hafner, C.; Wu, J.; Tiboldi, A.; Hess, M.; Mitulović, G.; Kaun, C.; Krychtiuk, K.; Wojta, J.; Ullrich, R.; Tretter, E.V.; et al. Hyperoxia induces inflammation and cytotoxicity in human adult cardiac myocytes. Shock 2017, 47, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Fonnes, S.; Gögenur, I.; Søndergaard, E.S.; Siersma, V.D.; Jorgensen, L.N.; Wetterslev, J.; Meyhoff, C.S.; Søndergaard, E. Perioperative hyperoxia—Long-term impact on cardiovascular complications after abdominal surgery, a post hoc analysis of the PROXI trial. Int. J. Cardiol. 2016, 215, 238–243. [Google Scholar] [CrossRef]
- Ruetzler, K.; Cohen, B.; Leung, S.; Mascha, E.J.; Knotzer, J.; Kurz, A.; Sessler, D.I.; Turan, A. Supplemental intraoperative oxygen does not promote acute kidney injury or cardiovascular complications after noncardiac surgery: Subanalysis of an alternating intervention trial. Anesth. Analg. 2019, 130, 933–940. [Google Scholar] [CrossRef]
- Holse, C.; Aasvang, E.K.; Vester-Andersen, M.; Rasmussen, L.S.; Wetterslev, J.; Christensen, R.; Jorgensen, L.N.; Pedersen, S.S.; Loft, F.C.; Troensegaard, H.; et al. Hyperoxia and Antioxidants for Myocardial Injury in Noncardiac Surgery: A 2 × 2 Factorial, Blinded, Randomized Clinical Trial. Anesthesiology 2022, 136, 408–419. [Google Scholar] [CrossRef] [PubMed]
- Sametz, W.; Metzler, H.; Gries, M.; Porta, S.; Sadjak, A.; Supanz, S.; Juan, H. Perioperative catecholamine changes in cardiac risk patients. Eur. J. Clin. Investig. 1999, 29, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Devereaux, P.J.; Duceppe, E.; Guyatt, G.; Tandon, V.; Rodseth, R.; Biccard, B.M.; Xavier, D.; Szczeklik, W.; Meyhoff, C.; Vincent, J.; et al. Dabigatran in patients with myocardial injury after non-cardiac surgery (MANAGE): An international, randomised, placebo-controlled trial. Lancet 2018, 391, 2325–2334. [Google Scholar] [CrossRef]
- Rodseth, R.N.; Biccard, B.M.; Chu, R.; Buse, G.A.L.; Thabane, L.; Bakhai, A.; Bolliger, D.; Cagini, L.; Cahill, T.J.; Cardinale, D.; et al. Postoperative B-type natriuretic peptide for prediction of major cardiac events in patients undergoing noncardiac surgery: Systematic review and individual patient meta-analysis. Anesthesiology 2013, 119, 271–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiterer, C.; Kabon, B.; Taschner, A.; Zotti, O.; Kurz, A.; Fleischmann, E. A comparison of intraoperative goal-directed intravenous administration of crystalloid versus colloid solutions on the postoperative maximum N-terminal pro brain natriuretic peptide in patients undergoing moderate- To high-risk noncardiac surgery. BMC Anesthesiol. 2020, 20, 192. [Google Scholar] [CrossRef] [PubMed]
- Devereaux, P.J.; Sessler, D.I. Cardiac complications in patients undergoing major noncardiac surgery. N. Engl. J. Med. 2015, 373, 2258–2269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solomon, M.J.; Young, C.J.; Eyers, A.A.; Roberts, R.A. Randomized clinical trial of laparoscopic versus open abdominal rectopexy for rectal prolapse. Br. J. Surg. 2002, 89, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Arsalani-Zadeh, R.; Ullah, S.; Khan, S.; MacFie, J. Oxidative stress in laparoscopic versus open abdominal surgery: A systematic review. J. Surg. Res. 2011, 169, e59–e68. [Google Scholar] [CrossRef]
- Obradovic, M.; Kurz, A.; Kabon, B.; Roth, G.; Kimberger, O.; Zotti, O.; Bayoumi, A.; Reiterer, C.; Stift, A.; Fleischmann, E. The effect of intraoperative goal-directed crystalloid versus colloid administration on perioperative inflammatory markers- Asubstudy of a randomized controlled trial. BMC Anesthesiol. 2020, 20, 210. [Google Scholar] [CrossRef]
- Reiterer, C.; Fleischmann, E.; Taschner, A.; Adamowitsch, N.; von Sonnenburg, M.F.; Graf, A.; Fraunschiel, M.; Starlinger, P.; Goschin, J.; Kabon, B. Perioperative supplemental oxygen and oxidative stress in patients undergoing moderate- to high-risk major abdominal surgery—A subanalysis of randomized clinical trial. J. Clin. Anesth. 2022, 77, 110614. [Google Scholar] [CrossRef]
- Stagos, D.; Goutzourelas, N.; Ntontou, A.M.; Kafantaris, I.; Deli, C.K.; Poulios, A.; Jamurtas, A.Z.; Bar-Or, D.; Kouretas, D. Assessment of eccentric exercise-induced oxidative stress using oxidation-reduction potential markers. Oxid. Med. Cell. Longev. 2015, 2015, 204615. [Google Scholar] [CrossRef] [PubMed]


| 80% Oxygen (n = 85) | 30% Oxygen (n = 88) | |
|---|---|---|
| Age, years | 73 (70; 78) | 74 (70; 79) |
| Height, cm | 172 (165; 176) | 172 (167; 178) |
| Weight, kg | 80 (67; 93) | 75 (67; 90) |
| BMI, kg·m−2 | 26.6 (23.8; 30.7) | 24.9 (23.2; 27.7) |
| Sex, n (%) | ||
| Women | 31 (36.5) | 28 (31.8) |
| Men | 54 (63.5) | 60 (68.2) |
| ASA physical status, n (%) | ||
| II | 16 (18.8) | 30 (34.1) |
| III | 67 (78.8) | 58 (65.9) |
| IV | 2 (2.4) | 0 (0) |
| Comorbidities, n (%) | ||
| Hypertension | 79 (92.9) | 82 (93.2) |
| Coronary artery disease | 24 (28.2) | 23 (26.1) |
| Peripheral artery disease | 13 (15.3) | 15 (17.0) |
| Stroke | 7 (8.2) | 5 (5.7) |
| Congestive heart failure | 5 (5.9) | 6 (6.8) |
| Transient ischemic attack | 2 (2.4) | 2 (2.3) |
| Diabetes | 26 (30.6) | 19 (21.6) |
| Insulin use | 7 (8.2) | 2 (2.3) |
| Long-term medication, n (%) | ||
| Beta blockers | 44 (51.8) | 47 (53.4) |
| ACI/ARB | 45 (52.9) | 50 (56.8) |
| Diuretics | 31 (36.5) | 26 (29.5) |
| Statins | 33 (38.8) | 38 (43.2) |
| Acetylsalicylic acid | 24 (28.2) | 30 (34.1) |
| Oral anticoagulant | 31 (36.5) | 21 (23.9) |
| Alpha 2 agonist | 3 (3.5) | 3 (3.4) |
| Type of Surgery, (%) | ||
| Hepatobiliary | 6 (7.1) | 6 (6.8) |
| Colorectal | 18 (21.2) | 18 (20.5) |
| Pancreatic | 11 (12.9) | 14 (15.9) |
| Urological | 37 (42.1) | 34 (40.0) |
| Gynaecological | 6 (7.1) | 3 (3.4) |
| Other | 10 (11.8) | 10 (11.6) |
| Open vs. Laparoscopic Surgery, (%) | ||
| Open | 51 (60.0) | 53 (60.2) |
| Laparoscopic | 30 (35.3) | 30 (34.1) |
| Both 1 | 4 (4.7) | 5 (5.7) |
| Laboratory parameters | ||
| CRP, mg·dL−1 | 0.33 (0.10; 0.82) | 0.27 (0.10; 0.91) |
| Creatinine, mg·dL−1 | 0.9 (0.7; 1.1) | 0.9 (0.8; 1.1) |
| Hemoglobin, g·dL−1 | 12.2 (10.7; 13.2) | 12.6 (10.8; 13.9) |
| Leukocytes, G·L−1 | 5.96 (5.03; 7.72) | 5.73 (4.85; 7.76) |
| NT-proBNP, pg·ml−1 | 205 (88; 486) | 218 (102; 796) |
| Troponin T, ng·L−1 | 13 (8; 19) | 13 (9; 21) |
| 80% Oxygen (n = 85) | 30% Oxygen (n = 88) | p-Value | |
|---|---|---|---|
| Intraoperative | |||
| Duration of anesthesia, min | 272 (186; 355) | 259 (205; 352) | 0.622 |
| Duration of surgery, min | 221 (141; 307) | 200 (142; 292) | 0.711 |
| Fluid management | |||
| Crystalloid, mL | 2160 (1508; 3386) | 2578 (1683; 3339) | 0.304 |
| Blood loss, mL | 300 (0; 600) | 275 (0; 725) | 0.610 |
| Urine output, mL | 300 (150; 475) | 300 (200; 500) | 0.417 |
| Anesthesia management | |||
| Fentanyl, mcg | 1013 (800; 1463) | 1100 (838; 1513) | 0.459 |
| Propofol, mg | 120 (93; 150) | 125 (50; 200) | 0.536 |
| Phenylephrine, mg | 0.28 (0.09; 0.46) | 0.21 (0.08; 0.42) | 0.717 |
| Noradrenaline, mg | 0.25 (0.00; 0.60) | 0.20 (0.00; 0.08) | 0.491 |
| etSevo, % | 1.3 (1.0; 1.3) | 1.2 (1.0; 1.3) | 0.556 |
| FiO2, % | 80 (80; 80) | 31 (30; 32) | |
| etCO2, mmHg | 34 (32; 36) | 34 (31; 35) | 0.531 |
| Core temp, °C | 36.5 (36.1; 36.8) | 36.5 (36.2; 36.9) | 0.210 |
| Hemodynamic Parameters | |||
| HR, beats·min−1 | 70 (58; 86) | 65 (56; 73) | 0.845 |
| MAP, mmHg | 80 (76; 84) | 81 (76; 88) | 0.549 |
| SV, mL | 71 (63; 84) | 66 (57; 83) | 0.821 |
| CO, L·min−1 | 4.1 (3.7; 5.6) | 4.6 (3.7; 5.3) | 0.615 |
| CVP, mmHg | 12 (10; 15) | 10 (9; 12) | 0.086 |
| Arterial Blood Gas Analysis | |||
| pO2, mmHg | 314 (270; 361) | 131 (109; 158) | <0.001 |
| pCO2, mmHg | 42 (40; 44) | 41 (39; 43) | 0.015 |
| pH | 7.38 (7.35; 7.41) | 7.39 (7.35; 7.42) | 0.169 |
| BE | −0.6 (−1.9; 0.9) | −0.3 (−1.9; 0.9) | 0.765 |
| Hemoglobin, g·dL−1 | 11.7 (9.9; 12.8) | 11.7 (10.2; 12.9) | 0.745 |
| Lactate, mmol·L−1 | 0.9 (0.7; 1.2) | 0.9 (0.7; 1.1) | 0.745 |
| Glucose, mmol·L−1 | 7.3 (6.4; 8.9) | 7.0 (6.2; 8.1) | 0.071 |
| 2 h postoperative | |||
| Hemodynamic Parameters | |||
| HR, beats·min−1 | 75 (61; 91) | 69 (63; 77) | 0.450 |
| MAP, mmHg | 82 (76; 100) | 81 (77; 100) | 0.431 |
| 72 h postoperative | |||
| Fluid, mL a | 9852 (6845; 11,989) | 9506 (7200; 12,137) | 0.900 |
| Piritramide, mg b | 8.0 (3.0; 20.3) | 10.0 (3.0; 21.0) | 0.903 |
| Variable | Comparison | Effect | Lower CI | Upper CI | p-Value |
|---|---|---|---|---|---|
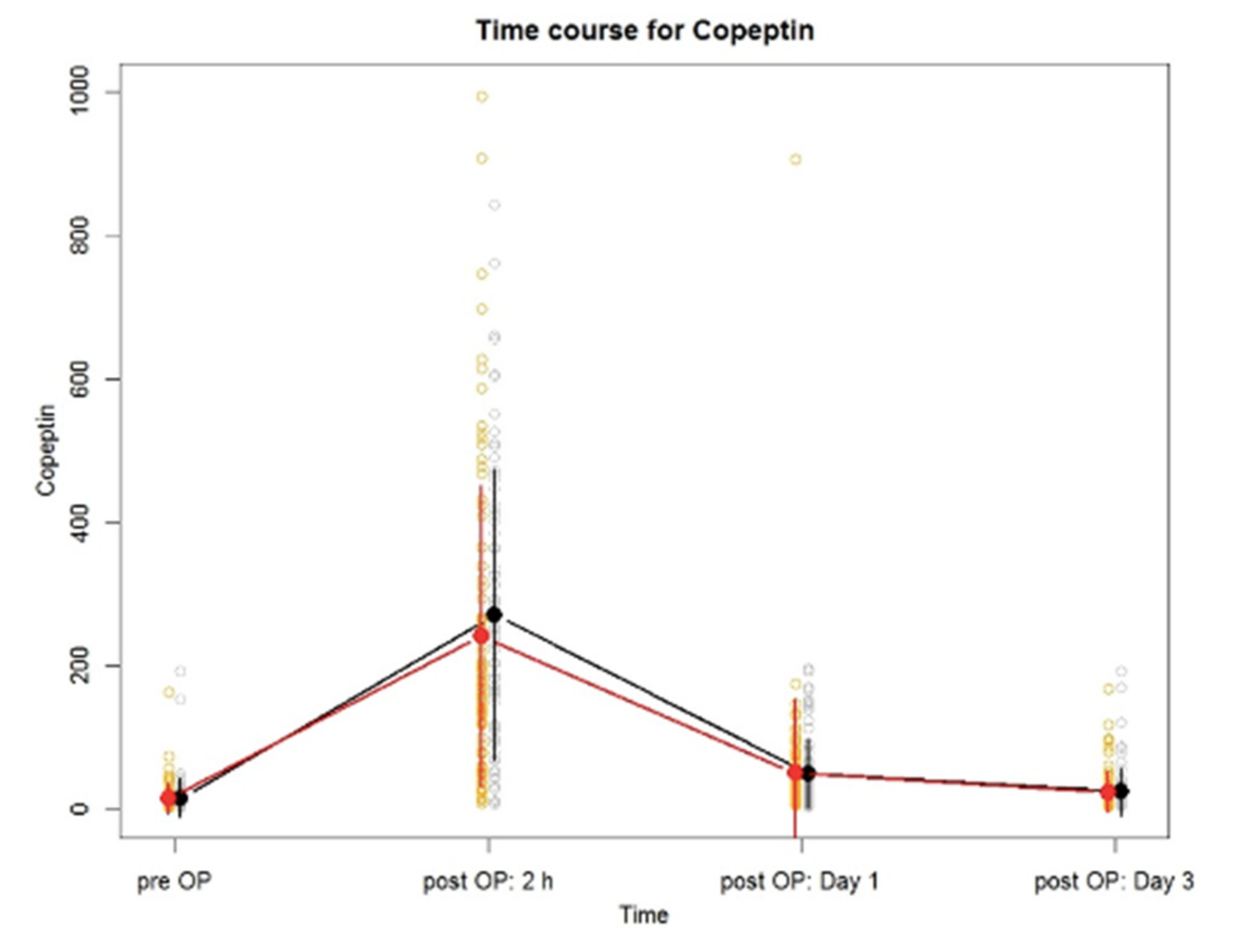
| Time | pre vs. 2 h post | −241.740 | −264.440 | −219.050 | <0.001 |
| pre vs. POD 1 | −35.206 | −58.245 | −12.168 | 0.003 | |
| pre vs. POD 3 | −7.976 | −31.470 | 15.519 | 0.505 | |
| Time × Group | Group 30% vs. 80% pre | −0.087 | −35.119 | 34.944 | 0.996 |
| Group 30% vs. 80% 2 h post | 29.838 | −4.614 | 64.291 | 0.090 | |
| Group 30% vs. 80% POD 1 | −1.453 | −36.794 | 33.888 | 0.936 | |
| Group 30% vs. 80% POD 3 | −1.514 | −38.053 | 35.025 | 0.935 | |
| Group 30% pre vs. 2 h post | −256.380 | −288.210 | −224.550 | <0.001 | |
| Group 30% pre vs. POD 1 | −34.513 | −66.983 | −2.042 | 0.037 | |
| Group 30% pre vs. POD 3 | −7.259 | −40.295 | 25.778 | 0.666 | |
| Group 80% pre vs. 2 h post | −226.450 | −258.820 | −194.080 | <0.001 | |
| Group 80% pre vs. POD 1 | −35.878 | −68.582 | −3.175 | 0.032 | |
| Group 80% pre vs. POD 3 | −8.685 | −42.115 | 24.744 | 0.610 | |
| Type of surgery | Laparoscopic vs. Open | −31.164 | −55.866 | −6.463 | 0.014 |
| Time × Type of surgery | Overall Interaction | <0.001 | |||
| Age | 0.559 | −0.937 | 2.055 | 0.464 | |
| BMI | 0.194 | −2.136 | 2.523 | 0.871 | |
| Sex | Female vs. Male | 15.426 | −9.309 | 40.161 | 0.221 |
| ASA | III, IV vs. I, II | −3.227 | −29.836 | 23.383 | 0.812 |
| Coronary Artery Disease | Yes vs. No | 5.535 | −20.697 | 31.767 | 0.679 |
| Peripheral Artery Disease | Yes vs. No | 19.548 | −12.763 | 51.859 | 0.235 |
| Stroke | Yes vs. No | 1.759 | −44.601 | 48.118 | 0.941 |
| Heart Failure | Yes vs. No | 22.391 | −24.925 | 69.707 | 0.353 |
| Diabetes | Yes vs. No | −1.582 | −28.143 | 24.980 | 0.907 |
| Hypertension | Yes vs. No | −4.915 | −51.273 | 41.443 | 0.835 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taschner, A.; Kabon, B.; Graf, A.; Adamowitsch, N.; Falkner von Sonnenburg, M.; Fraunschiel, M.; Horvath, K.; Fleischmann, E.; Reiterer, C. Perioperative Supplemental Oxygen and Postoperative Copeptin Concentrations in Cardiac-Risk Patients Undergoing Major Abdominal Surgery—A Secondary Analysis of a Randomized Clinical Trial. J. Clin. Med. 2022, 11, 2085. https://doi.org/10.3390/jcm11082085
Taschner A, Kabon B, Graf A, Adamowitsch N, Falkner von Sonnenburg M, Fraunschiel M, Horvath K, Fleischmann E, Reiterer C. Perioperative Supplemental Oxygen and Postoperative Copeptin Concentrations in Cardiac-Risk Patients Undergoing Major Abdominal Surgery—A Secondary Analysis of a Randomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(8):2085. https://doi.org/10.3390/jcm11082085
Chicago/Turabian StyleTaschner, Alexander, Barbara Kabon, Alexandra Graf, Nikolas Adamowitsch, Markus Falkner von Sonnenburg, Melanie Fraunschiel, Katharina Horvath, Edith Fleischmann, and Christian Reiterer. 2022. "Perioperative Supplemental Oxygen and Postoperative Copeptin Concentrations in Cardiac-Risk Patients Undergoing Major Abdominal Surgery—A Secondary Analysis of a Randomized Clinical Trial" Journal of Clinical Medicine 11, no. 8: 2085. https://doi.org/10.3390/jcm11082085