
Perioperative Supplemental Oxygen and Plasma Catecholamine Concentrations after Major Abdominal Surgery—Secondary Analysis of a Randomized Clinical Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
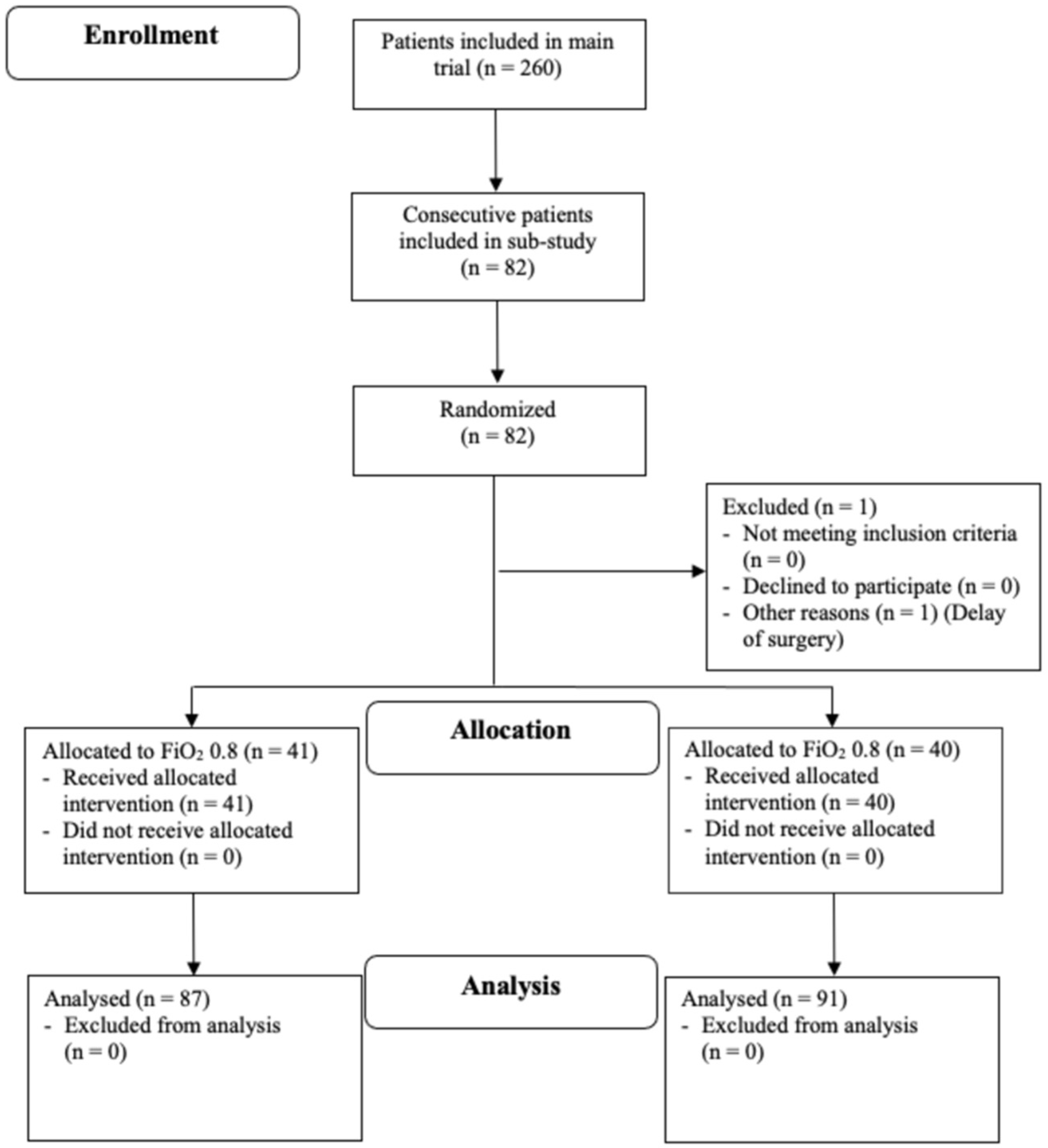
2.1. Study Design and Participants
2.2. Randomization
2.3. Measurements
2.4. Data Management
2.5. Statistical Analysis
2.6. Plasma Catecholamines
2.7. Post-Hoc Analysis
2.8. Sample Size
3. Results
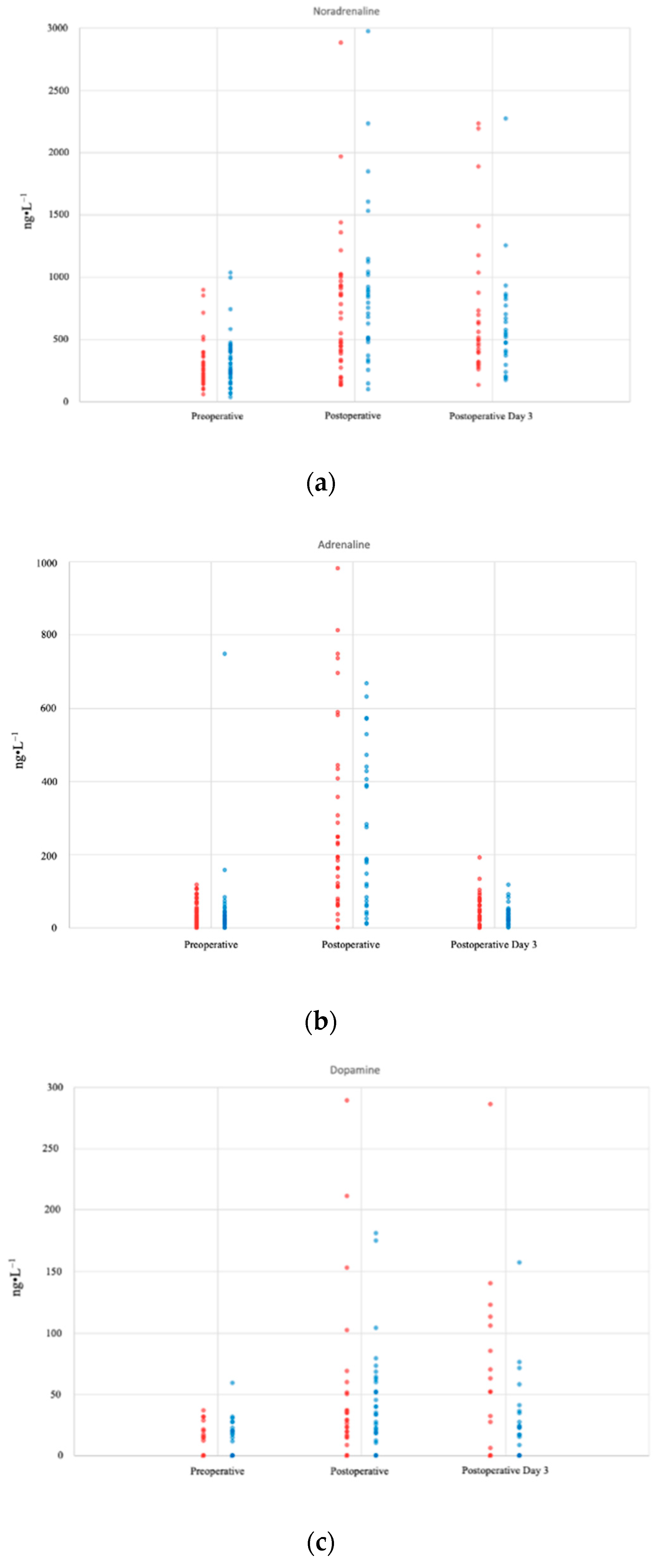
3.1. Plasma Catecholamine Concentrations
3.2. Post-Hoc Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sametz, W.; Metzler, H.; Gries, M.; Porta, S.; Sadjak, A.; Supanz, S.; Juan, H. Perioperative catecholamine changes in cardiac risk patients. Eur. J. Clin. Investig. 1999, 29, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.D.; Breslow, M.J.; Frank, S.M.; Rosenfeld, B.A.; Norris, E.J.; Christopherson, R.; Rock, P.; Gottlieb, S.O.; Raff, H.; Perler, B.A.; et al. Catecholamine and cortisol responses to lower extremity revascularization: Correlation with outcome variables. Perioperative Ischemia Randomized Anesthesia Trial Study Group. Crit. Care Med. 1995, 23, 1954–1961. [Google Scholar] [CrossRef] [PubMed]
- Devereaux, P.J.; Yang, H.; Yusuf, S.; Guyatt, G.; Leslie, K.; Villar, J.C.; Xavier, D.; Chrolavicius, S.; Greenspan, L.; Pogue, J.; et al. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): A randomised controlled trial. Lancet 2008, 371, 1839–1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devereaux, P.J.; Szczeklik, W. Myocardial injury after non-cardiac surgery: Diagnosis and management. Eur. Heart J. 2019, 41, 3083–3091. [Google Scholar] [CrossRef]
- Cohn, J.N.; Levine, T.B.; Olivari, M.T.; Garberg, V.; Lura, D.; Francis, G.S.; Simon, A.B.; Rector, T. Plasma norepinephrine as a Guide to Prognosis in Chronic Congestive Heart Failure. N. Engl. J. Med. 1984, 311, 819–823. [Google Scholar] [CrossRef] [Green Version]
- Lamba, S.; Abraham, W.T. Alterations in adrenergic receptor signaling in heart failure. Heart Fail. Rev. 2000, 5, 7–16. [Google Scholar] [CrossRef]
- Priebe, H.J. Triggers of perioperative myocardial ischaemia and infarction. Br. J. Anaesth. 2004, 93, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Wu, K.K. Platelet activation mechanisms and markers in arterial thrombosis. J. Intern. Med. 1996, 239, 17–34. [Google Scholar] [CrossRef]
- Allegranzi, B.; Zayed, B.; Bischoff, P.; Kubilay, N.Z.; de Jonge, S.; de Vries, F.; Gomes, S.M.; Gans, S.; Wallert, E.D.; Wu, X.; et al. Surgical site infections 2 New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: An evidence-based global perspective. Lancet Infect. Dis. 2016, 16, e288–e303. [Google Scholar] [CrossRef]
- Reiterer, C.; Kabon, B.; Taschner, A.; von Sonnenburg, M.F.; Graf, A.; Adamowitsch, N.; Starlinger, P.; Goshin, J.; Fraunschiel, M.; Fleischmann, E. Perioperative supplemental oxygen and NT-proBNP concentrations after major abdominal surgery—A prospective randomized clinical trial. J. Clin. Anesth. 2021, 73, 110379. [Google Scholar] [CrossRef]
- Reiterer, C.; Kabon, B.; von Sonnenburg, M.F.; Starlinger, P.; Taschner, A.; Zotti, O.; Goshin, J.; Drlicek, G.; Fleischmann, E. The effect of supplemental oxygen on perioperative brain natriuretic peptide concentration in cardiac risk patients—A protocol for a prosprective randomized clinical trial. Trials 2020, 21, 400. [Google Scholar] [CrossRef] [PubMed]
- Devereaux, P.J.; Biccard, B.M.; Sigamani, A.; Xavier, D.; Chan, M.T.; Srinathan, S.K.; Walsh, M.; Abraham, V.; Pearse, R.; Wang, C.Y.; et al. Association of postoperative high-sensitivity troponin levels with myocardial injury and 30-day mortality among patients undergoing noncardiac surgery. JAMA—J. Am. Med. Assoc. 2017, 317, 1642–1651. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2011, 9, 672–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staniforth, A.D.; Kinnear, W.J.M.; Starling, R.; Hetmanski, D.J.; Cowley, A.J. Effect of oxygen on sleep quality, cognitive function and sympathetic activity in patients with chronic heart failure and Cheyn-Stokes respiration. Eur. Heart J. 1998, 19, 922–928. [Google Scholar] [CrossRef] [Green Version]
- Shigemitsu, M.; Nishio, K.; Kusuyama, T.; Itoh, S.; Konno, N.; Katagiri, T. Nocturnal oxygen therapy prevents progress of congestive heart failure with central sleep apnea. Int. J. Cardiol. 2007, 115, 354–360. [Google Scholar] [CrossRef]
- Smit, B.; Smulders, Y.M.; van der Wouden, J.C.; Oudemans-van Straaten, H.M.; Spoelstra-de Man, A.M.E. Hemodynamic effects of acute hyperoxia: Systematic review and meta-analysis. Crit. Care 2018, 22, 40. [Google Scholar] [CrossRef] [Green Version]
- Greif, R.; Akca, O.; Horn, E.-P.; Kurz, A.; Sessler, D.I. Supplemental Perioperative Oxygen to reduce the Incidence of Surgical-Wound Infection. N. Engl. J. Med. 2000, 342, 161–167. [Google Scholar] [CrossRef]
- Bühler, F.R.; Amann, F.W.; Bolli, P.; Hulthén, L.; Kiowski, W.; Landmann, R.; Bürgisser, E. Elevated adrenaline and increased alpha-adrenoceptor-mediated vasoconstriction in essential hypertension. J. Cardiovasc. Pharmacol. 1982, 4 (Suppl. 1), S134–S138. [Google Scholar] [CrossRef]
- Møller, I.W.; Dinesen, K.; Søndergård, S.; Knigge, U.; Kehlet, H. Effect of patient-controlled analgesia on plasma catecholamine, cortisol and glucose concentrations after cholecystectomy. Br. J. Anaesth. 1988, 61, 160–164. [Google Scholar] [CrossRef]
- Devereaux, P.J.; Goldman, L.; Cook, D.J.; Gilbert, K.; Leslie, K.; Guyatt, G.H. Perioperative cardiac events in patients undergoing noncardiac surgery: A review of the magnitude of the problem, the pathophysiology of the events and methods to estimate and communicate risk. CMAJ 2005, 173, 627–634. [Google Scholar] [CrossRef] [Green Version]
- Frank, S.M.; Higgins, M.S.; Breslow, M.J.; Fleisher, L.A.; Gorman, R.B.; Sitzmann, J.V.; Raff, H.; Beattle, C. The Catecholamine, Cortisol, and Hemodynamic Responses to Mild Perioperative Hypothermia. Anesthesiology 1995, 82, 83–93. [Google Scholar] [CrossRef]
- Chu, D.K.; Kim, L.H.; Young, P.J.; Zamiri, N.; Almenawer, S.A.; Jaeschke, R.; Szczeklik, W.; Schünemann, H.J.; Neary, J.D.; Alhazzani, W. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): A systematic review and meta-analysis. Lancet 2018, 391, 1693–1705. [Google Scholar] [CrossRef]
- Meyhoff, C.S.; Wetterslev, J.; Jorgensen, L.N.; Henneberg, S.W.; Høgdall, C.; Lundvall, L.; Svendsen, P.E.; Mollerup, H.; Lunn, T.H.; Simonsen, I.; et al. Effect of High Perioperative Oxygen Fraction on Surgical Site Infection and Pulmonary Complications after Abdominal Surgery. JAMA 2009, 302, 1543–1550. [Google Scholar] [CrossRef] [PubMed]
- Kurz, A.; Kopyeva, T.; Suliman, I.; Podolyak, A.; You, J.; Lewis, B.; Vlah, C.; Khatib, R.; Keebler, A.; Reigert, R.; et al. Supplemental oxygen and surgical-site infections: An alternating intervention controlled trial. Br. J. Anaesth. 2018, 120, 117–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Patient Characteristics | ||||
|---|---|---|---|---|
| 80% Oxygen (n = 41) | 30% Oxygen (n = 40) | |||
| Age, years | 75 | (70; 78) | 73 | (69; 77) |
| Height, cm | 170 | (167; 175) | 174 | (168; 179) |
| Weight, kg | 80 | (72; 88) | 84 | (77; 92) |
| BMI, kg·m−2 | 26.8 | (24.1; 29.8) | 27.6 | (25.2; 29.9) |
| Sex, n (%) | ||||
| Women | 15 | (36.7) | 9 | (22.5) |
| Men | 26 | (63.3) | 31 | (77.5) |
| ASA physical status, n (%) | ||||
| II | 13 | (36.6) | 16 | (40) |
| III | 28 | (63.4) | 24 | (60) |
| Comorbidities, n (%) | ||||
| Hypertension | 39 | (95.1) | 36 | (90.0) |
| Coronary artery disease | 9 | (21.9) | 8 | (20.0) |
| Peripheral artery disease | 6 | (14.6) | 5 | (12.5) |
| Stroke | 5 | (12.2) | 4 | (10.0) |
| Congestive heart failure | 3 | (7.3) | 3 | (7.5) |
| Transient ischemic attack | 1 | (2.4) | 6 | (15.0) |
| Insulin use | 13 | (31.7) | 12 | (30.0) |
| Long-term medication, n (%) | ||||
| Beta blockers | 17 | (41.5) | 16 | (40.0) |
| ACI/ARB | 24 | (58.5) | 21 | (52.5) |
| Diuretics | 12 | (29.3) | 6 | (15.0) |
| Statins | 20 | (48.8) | 18 | (45.0) |
| Acetylsalicylic acid | 2 | (4.9) | 3 | (7.5) |
| Oral anticoagulant | 18 | (43.9) | 15 | (37.5) |
| Alpha 2 agonist | 1 | (2.4) | 2 | (5.0) |
| Type of Surgery, (%) | ||||
| Hepatobiliary | 8 | (19.5) | 7 | (17.5) |
| Colorectal | 9 | (22.0) | 8 | (20.0) |
| Pancreatic | 6 | (14.6) | 3 | (7.5) |
| Urological | 12 | (29.3) | 19 | (47.5) |
| Other | 6 | (14.6) | 3 | (7.5) |
| Laboratory parameters | ||||
| CRP, mg·dL−1 | 0.33 | (0.19; 1.43) | 0.26 | (0.12; 0.58) |
| Creatinine, mg·dL−1 | 0.9 | (0.8; 1.0) | 0.9 | (0.8; 1.1) |
| Leukocytes, G·L−1 | 6.61 | (5.42; 8.60) | 6.58 | (5.03; 8.07) |
| NT-proBNP, pg·mL−1 | 280 | (97; 533) | 128 | (69; 391) |
| Troponin T, ng·L−1 | 14 | (11; 22) | 15 | (9; 22) |
| Perioperative Variables | |||||
|---|---|---|---|---|---|
| 80% Oxygen (n = 41) | 30% Oxygen (n = 40) | p-Value | |||
| Intraoperative | |||||
| Duration of anesthesia, min | 264 | (191; 403) | 215 | (177; 287) | 0.06 |
| Duration of surgery, min | 207 | (134; 329) | 152 | (129; 233) | 0.17 |
| Fluid management | |||||
| Crystalloid, mL | 2237 | (1262; 3538) | 1936 | (1396; 2696) | 0.41 |
| Blood loss, mL | 200 | (0; 500) | 200 | (0; 500) | 0.78 |
| Urine output, mL | 245 | (150; 400) | 225 | (285; 400) | 0.83 |
| Anesthesia management | |||||
| Fentanyl, mcg | 1100 | (863; 1488) | 1050 | (800; 1500) | 0.60 |
| Propofol, mg | 145 | (70; 160) | 150 | (100; 200) | 0.15 |
| Phenylephrine, mg | 0.25 | (0.10; 0.58) | 0.20 | (0.08; 0.52) | 0.56 |
| Noradrenaline, mg | 0.0 | (0.0; 1.0) | 0.0 | (0.0; 0.3) | 0.10 |
| etSevo, % | 1.3 | (1.0; 1.5) | 1.2 | (0.7; 1.4) | 0.18 |
| FiO2, % | 81 | (80; 81) | 32 | (31; 68) | |
| etCO2, mmHg | 35 | (34; 36) | 34 | (32; 36) | 0.18 |
| Core temp, °C | 36.2 | (35.9; 36.8) | 36.4 | (36.2; 36.9) | 0.55 |
| Hemodynamic Parameters | |||||
| HR, beats·min−1 | 62 | (58; 69) | 73 | (62; 84) | 0.59 |
| MAP, mmHg | 79 | (74; 90) | 91 | (85; 95) | 0.42 |
| SV, mL | 77 | (55; 81) | 52 | (30; 67) | 0.22 |
| CO, L·min−1 | 4.7 | (3.7; 5.4) | 3.3 | (1.9; 4.5) | 0.12 |
| CVP, mmHg | 12 | (8; 15) | 11 | (8; 20) | 0.69 |
| Arterial Blood Gas Analysis | |||||
| pO2, mmHg | 158 | (112; 195) | 91 | (75; 155) | <0.05 |
| pCO2, mmHg | 43 | (39; 52) | 49 | (46; 60) | 0.50 |
| SpO2, % | 100 | (99; 100) | 98 | (97; 99) | <0.001 |
| pH | 7.34 | (7.28; 7.38) | 7.31 | (7.25; 7.34) | 0.33 |
| BE | −1.9 | (−4.6; −0.7) | −1.2 | (−3.3; −0.1) | 0.25 |
| Hb, g·dL−1 | 11.8 | (10.4; 12.5) | 13.4 | (11.1; 13.9) | 0.31 |
| Lactate, mmol·L−1 | 0.8 | (0.6; 1.0) | 1.6 | (0.9; 2.3) | 0.53 |
| Glucose, mg·dL−1 | 163 | (150; 184) | 155 | (123; 175) | 0.31 |
| 2 h postoperative | |||||
| Hemodynamic Parameters | |||||
| HR, beats·min−1 | 75 | (60; 88) | 82 | (64; 90) | 0.41 |
| MAP, mmHg | 86 | (75; 103) | 109 | (98; 122) | <0.001 |
| SpO2, % | 99 | (97; 99) | 98 | (97; 99) | 0.11 |
| VAS | 2 | (0; 4) | 2 | (0; 4) | 0.88 |
| PONV | |||||
| Dexamethasone, n (%) | 29 | (70.7) | 35 | (87.5) | 0.10 |
| PONV, n (%) | 4 | (9.8) | 5 | (12.5) | 0.74 |
| Ondansetron, n (%) | 10 | (24.4) | 12 | (30.0) | 0.62 |
| Amount per capita, mg | 4 | (4; 5) | 4 | (4; 5) | 0.84 |
| Droperidol, n (%) | 2 | (4.9) | 3 | (7.5) | 0.68 |
| Amount per capita, mg | 1.25 | (1.25; 1.25) | 1.25 | (1.25; 1.25) | 1.00 |
| 72 h postoperative | |||||
| Fluid, mL (a) | 10,400 | (7417; 12,525) | 9471 | (7013; 11,526) | 0.58 |
| Piritramide, mg (b) | 12.0 | (4.5; 22.0) | 8.3 | (3.0; 21.8) | 0.65 |
| Plasma Catecholamine Concentrations | |||||
|---|---|---|---|---|---|
| 80% Oxygen (n = 41) | 30% Oxygen (n = 40) | p-Value | |||
| Noradrenaline, ng·L−1 | |||||
| Baseline | 247 | (147; 443) | 259 | (170; 369) | 0.20 |
| 2 h postoperative | 757 | (447; 1240) | 494 | (318; 864) | 0.13 |
| Postoperative day 3 | 560 | (384; 827) | 493 | (313; 730) | 0.89 |
| Adrenaline, ng·L−1 | |||||
| Baseline | 27 | (16; 43) | 25 | (14; 69) | 0.59 |
| 2 h postoperative | 187 | (70; 539) | 193 | (74; 444) | 0.86 |
| Postoperative day 3 | 36 | (18; 49) | 43 | (23; 75) | 0.17 |
| Dopamine, ng·L−1 | |||||
| Baseline | 0 | (0; 19) | 0 | (0; 15) | 0.66 |
| 2 h postoperative | 34 | (19; 52) | 19 | (0; 35) | 0.10 |
| Postoperative day 3 | 23 | (0; 37) | 0 | (0; 85) | 0.92 |
| Post-Hoc Analysis | |||||
|---|---|---|---|---|---|
| MINS (n = 26) | No MINS (n = 55) | p-Value | |||
| Noradrenaline, ng·L−1 | |||||
| Baseline | 233 | (121; 415) | 259 | (166; 380) | |
| 2 h postoperative | 672 | (365; 990) | 501 | (349; 927) | |
| Postoperative day 3 | 505 | (400; 809) | 531 | (311; 795) | |
| Maximum | 782 | (508; 1040) | 855 | (597; 1164) | 0.48 |
| Adrenaline, ng·L−1 | |||||
| Baseline | 31 | (16; 48) | 21 | (15; 56) | |
| 2 h postoperative | 164 | (83; 585) | 193 | (67; 442) | |
| Postoperative day 3 | 38 | (18; 87) | 40 | (22; 66) | |
| Maximum | 171 | (113; 571) | 211 | (75; 438) | 0.72 |
| Dopamine, ng·L−1 | |||||
| Baseline | 0 | (0; 19) | 0 | (0; 0) | |
| 2 h postoperative | 31 | (0; 61) | 23 | (15; 36) | |
| Postoperative day 3 | 16 | (0; 53) | 22 | (0; 67) | |
| Maximum | 39 | (11; 68) | 36 | (17; 71) | 0.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taschner, A.; Kabon, B.; Falkner von Sonnenburg, M.; Graf, A.; Adamowitsch, N.; Fraunschiel, M.; Fleischmann, E.; Reiterer, C. Perioperative Supplemental Oxygen and Plasma Catecholamine Concentrations after Major Abdominal Surgery—Secondary Analysis of a Randomized Clinical Trial. J. Clin. Med. 2022, 11, 1767. https://doi.org/10.3390/jcm11071767
Taschner A, Kabon B, Falkner von Sonnenburg M, Graf A, Adamowitsch N, Fraunschiel M, Fleischmann E, Reiterer C. Perioperative Supplemental Oxygen and Plasma Catecholamine Concentrations after Major Abdominal Surgery—Secondary Analysis of a Randomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(7):1767. https://doi.org/10.3390/jcm11071767
Chicago/Turabian StyleTaschner, Alexander, Barbara Kabon, Markus Falkner von Sonnenburg, Alexandra Graf, Nikolas Adamowitsch, Melanie Fraunschiel, Edith Fleischmann, and Christian Reiterer. 2022. "Perioperative Supplemental Oxygen and Plasma Catecholamine Concentrations after Major Abdominal Surgery—Secondary Analysis of a Randomized Clinical Trial" Journal of Clinical Medicine 11, no. 7: 1767. https://doi.org/10.3390/jcm11071767