
The Association between Two-Stage Tourniquet Application during Total Knee Replacement and Blood Loss: A Retrospective Cohort Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
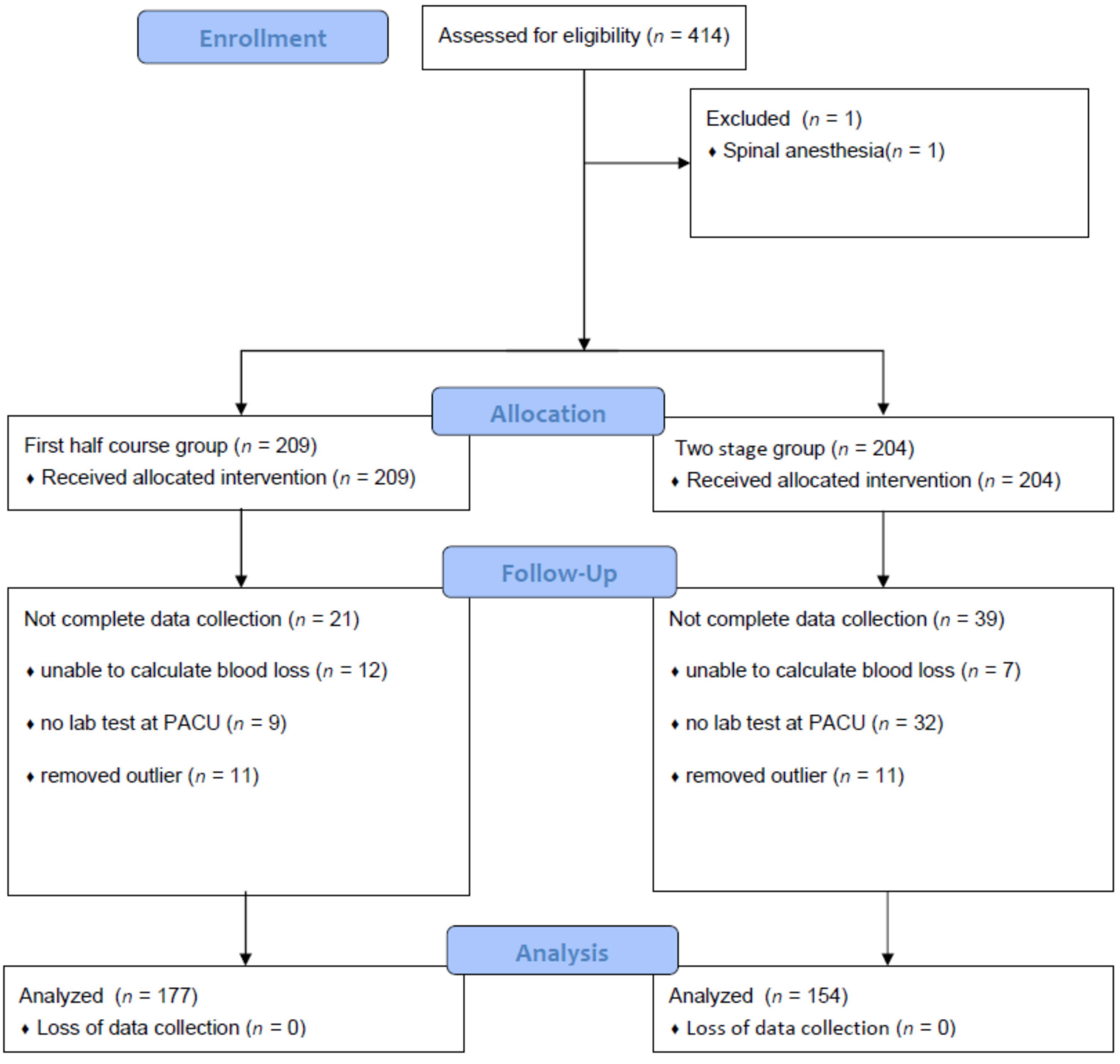
2.1. Patients
2.2. Perioperative Anesthetic Care
2.3. Outcome Variables
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zak, S.G.; Yeroushalmi, D.; Long, W.J.; Meftah, M.; Schnaser, E.; Schwarzkopf, R. Does the Use of a Tourniquet Influence Outcomes in Total Knee Arthroplasty: A Randomized Controlled Trial. J. Arthroplast. 2021, 36, 2492–2496. [Google Scholar] [CrossRef]
- Cao, Q.; He, Z.; Fan, Y.; Meng, J.; Yuan, T.; Zhao, J.; Bao, N. Effects of tourniquet application on enhanced recovery after surgery (ERAS) and ischemia-reperfusion post-total knee arthroplasty: Full- versus second half-course application. J. Orthop. Surg. 2020, 28, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Hamawandi, S.A.; Amin, H.I.; Al-Humairi, A.K. Effects of the Use of Tourniquet in Total Knee Arthroplasty on the Clinical and Functional Outcomes with 5 Years of Follow-up: A Randomized Controlled Trial. J. Knee Surg. 2021, 1. [Google Scholar] [CrossRef]
- Cai, D.F.; Fan, Q.H.; Zhong, H.H.; Peng, S.; Song, H. The effects of tourniquet use on blood loss in primary total knee arthroplasty for patients with osteoarthritis: A meta-analysis. J. Orthop. Surg. Res. 2019, 14, 348. [Google Scholar] [CrossRef] [Green Version]
- Olivecrona, C.; Blomfeldt, R.; Ponzer, S.; Stanford, B.R.; Nilsson, B.Y. Tourniquet cuff pressure and nerve injury in knee arthroplasty in a bloodless field: A neurophysiological study. Acta Orthop. 2013, 84, 159–164. [Google Scholar] [CrossRef]
- Ahmed, I.; Chawla, A.; Underwood, M.; Price, A.J.; Metcalfe, A.; Hutchinson, C.E.; Warwick, J.; Seers, K.; Parsons, H.; Wall, P.D.H. Time to reconsider the routine use of tourniquets in total knee arthroplasty surgery. Bone Jt. J. 2021, 103, 830–839. [Google Scholar] [CrossRef]
- Olivecrona, C.; Lapidus, L.J.; Benson, L.; Blomfeldt, R. Tourniquet time affects postoperative complications after knee arthroplasty. Int. Orthop. 2013, 37, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Olivecrona, C.; Ponzer, S.; Hamberg, P.; Blomfeldt, R. Lower tourniquet cuff pressure reduces postoperative wound complications after total knee arthroplasty: A randomized controlled study of 164 patients. JBJS 2012, 94, 2216–2221. [Google Scholar] [CrossRef] [Green Version]
- Migliorini, F.; Maffulli, N.; Aretini, P.; Trivellas, A.; Tingart, M.; Eschweiler, J.; Baroncini, A. Impact of tourniquet during knee arthroplasty: A bayesian network meta-analysis of peri-operative outcomes. Arch. Orthop. Trauma Surg. 2021, 141, 1007–1023. [Google Scholar] [CrossRef]
- Kim, K.S.; Min, H.K.; Youn, H.J.; Cheong, M.A.; Jun, J.H. The Hemodynamic Effects of a Tourniquet Application during Knee Surgery in Elderly Patients with Hypertension. Korean J. Anesth. 2006, 51, 695–700. [Google Scholar] [CrossRef]
- Girardis, M.; Milesi, S.; Donato, S.; Raffaelli, M.; Spasiano, A.; Antonutto, G.; Pasqualucci, A.; Pasetto, A. The Hemodynamic and Metabolic Effects of Tourniquet Application during Knee Surgery. Anesth. Analg. 2000, 91, 727–731. [Google Scholar] [CrossRef]
- Song, I.; Kim, D.Y.; Kim, Y.J. The effect of tourniquet deflation on hemodynamics and regional cerebral oxygen saturation in aged patients undergoing total knee replacement surgery. Korean J. Anesthesiol. 2012, 63, 425–430. [Google Scholar] [CrossRef]
- Huh, I.Y.; Kim, D.-Y.; Lee, J.-H.; Shin, S.J.; Cho, Y.W.; Park, S.E. Relation between preoperative autonomic function and blood pressure change after tourniquet deflation during total knee replacement arthroplasty. Korean J. Anesthesiol. 2012, 62, 154–160. [Google Scholar] [CrossRef]
- Pinsornsak, P.; Pinitchanon, P.; Boontanapibul, K. Effect of Different Tourniquet Pressure on Postoperative Pain and Complications After Total Knee Arthroplasty: A Prospective, Randomized Controlled Trial. J. Arthroplast. 2021, 36, 1638–1644. [Google Scholar] [CrossRef]
- Horlocker, T.T.; Hebl, J.R.; Gali, B.; Jankowski, C.J.; Burkle, C.M.; Berry, D.J.; Zepeda, F.A.; Stevens, S.R.; Schroeder, D.R. Anesthetic, Patient, and Surgical Risk Factors for Neurologic Complications After Prolonged Total Tourniquet Time during Total Knee Arthroplasty. Anesth. Analg. 2006, 102, 950–955. [Google Scholar] [CrossRef]
- Vaishya, R.; Agarwal, A.K.; Vijay, V.; Tiwari, M.K. Short term outcomes of long duration versus short duration tourniquet in primary total knee arthroplasty: A randomized controlled trial. J. Clin. Orthop. Trauma 2018, 9, 46–50. [Google Scholar] [CrossRef]
- Wang, C.; Zhou, C.; Qu, H.; Yan, S.; Pan, Z. Comparison of tourniquet application only during cementation and long-duration tourniquet application in total knee arthroplasty: A meta-analysis. J. Orthop. Surg. Res. 2018, 13, 1–10. [Google Scholar] [CrossRef]
- Gao, F.Q.; Li, Z.J.; Zhang, K.; Sun, W.; Zhang, H. Four methods for calculating blood-loss after total knee arthroplasty. Chin. Med. J. 2015, 128, 2856–2860. [Google Scholar] [CrossRef]
- Zhang, W.; Li, N.; Chen, S.; Tan, Y.; Al-Aidaros, M.; Chen, L. The effects of a tourniquet used in total knee arthroplasty: A meta-analysis. J. Orthop. Surg. Res. 2014, 9, 13. [Google Scholar] [CrossRef] [Green Version]
- Sahu, S.; Hemlata; Verma, A. Adverse events related to blood transfusion. Indian J. Anaesth. 2014, 58, 543–551. [Google Scholar] [CrossRef]
- Monk, T.G.; Saini, V.; Weldon, B.C.; Sigl, J.C. Anesthetic Management and One-Year Mortality after Noncardiac Surgery. Anesth. Analg. 2005, 100, 4–10. [Google Scholar] [CrossRef]
- Kim, E.; Cho, M.R.; Byun, S.H.; Lim, J.A.; Chae, S.; Choi, W.K.; Kim, I.; Kim, J. Sympathetic predominance before tourniquet deflation is associated with a reduction in arterial blood pressure after tourniquet deflation during total knee arthroplasty. Physiol. Res. 2021, 70, 401–412. [Google Scholar] [CrossRef]
- Aubrun, F.; Langeron, O.; Quesnel, C.; Coriat, P.; Riou, B. Relationships between Measurement of Pain Using Visual Analog Score and Morphine Requirements during Postoperative Intravenous Morphine Titration. Anesthesiology 2003, 98, 1415–1421. [Google Scholar] [CrossRef]


{kind=link}
| Variables | FH Group | TS Group | p-Value |
|---|---|---|---|
| (n = 177) | (n = 154) | ||
| Patient Characteristics | |||
| Age | 69.5 ± 8.3 | 69.9 ± 7.2 | 0.622 |
| Height (cm) | 155.1 ± 6.4 | 154.9 ± 7.7 | 0.756 |
| Weight (kg) | 62.0 ± 9.7 | 62.1 ± 9.2 | 0.899 |
| Disease characteristics | |||
| Hypertension | 97 | 103 | 0.025 |
| Diabetes Mellitus | 39 | 35 | 0.880 |
| Stroke | 6 | 1 | 0.084 |
| Chronic kidney disease | 6 | 6 | 0.806 |
| Angina, myocardial infarction | 7 | 13 | 0.087 |
| Taking anticoagulants | 42 | 45 | 0.258 |
| Pre-operative hemoglobin (g/dL) | 12.9 ± 1.2 | 13.0 ± 1.1 | 0.589 |
| Estimated Blood Loss | FH Group | TS Group |
|---|---|---|
| Volume (mL) | 542.90 ± 274.77 | 514.66 ± 228.54 |
| Medications | FH Group (n = 177) | TS Group (n = 154) | p-Value |
|---|---|---|---|
| Type of Drugs | |||
| Antihypertensive drug 1 | 38 | 26 | 0.292 |
| Vasopressor 2 | 28 | 21 | 0.577 |
| Transfused Blood (Number of Patients) | FH Group | TS Group | p-Value |
|---|---|---|---|
| Intra-operatively | 0(149) | 0(151) | 0.000 |
| 1(26) | 1(3) | ||
| 2(2) | 2(0) | ||
| In the post-anesthesia care unit | 0(174) | 0(153) | 0.385 |
| 1(3) | 1(1) | ||
| In the ward post-operatively | 0(153) | 0(140) | 0.108 |
| 1(12) | 1(11) | ||
| 2(12) | 2(3) |
| Hemoglobin Values (g/dL) | FH Group | TS Group | p-Value |
|---|---|---|---|
| Intra-operatively (initial) | 11.8 ± 1.1 | 11.8 ± 1.0 | 0.435 |
| Intra-operatively (last) | 10.5 ± 1.0 | 10.4 ± 1.0 | 0.403 |
| In the post-anesthesia care unit | 11.3 ± 1.0 | 11.2 ± 1.0 | 0.246 |
| Hemoglobin Values (g/dL) | Non-Transfused Group (n = 300) | Transfused Group (n = 31) | p-Value |
|---|---|---|---|
| Pre-operative | 13.1 ± 1.0 | 11.7 ± 1.0 | 0.000 |
| Intra-operatively (initial) | 11.9 ± 1.0 | 10.5 ± 0.8 | 0.000 |
| Opioid Use (µg) | FH Group | TS Group |
|---|---|---|
| Fentanyl | 76.2 ± 43.9 | 84.4 ± 56.1 |
| Equivalent |
| Time (min) | FH Group (n = 177) | TS Group (n = 154) | p-Value |
|---|---|---|---|
| Tourniquet applied | |||
| 1st | 89.0 ± 17.2 | 89.6 ± 16.6 | 0.747 |
| 2nd | - | 25.4 ± 8.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, M.S.; Kim, J.-Y.; Kim, C.L.; Koh, S.R.; Jung, Y.; Kim, N.Y.; Jeong, M.A. The Association between Two-Stage Tourniquet Application during Total Knee Replacement and Blood Loss: A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 1682. https://doi.org/10.3390/jcm11061682
Oh MS, Kim J-Y, Kim CL, Koh SR, Jung Y, Kim NY, Jeong MA. The Association between Two-Stage Tourniquet Application during Total Knee Replacement and Blood Loss: A Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(6):1682. https://doi.org/10.3390/jcm11061682
Chicago/Turabian StyleOh, Min Seok, Ji-Yoon Kim, Cho Long Kim, Su Rim Koh, Yundo Jung, Na Yeon Kim, and Mi Ae Jeong. 2022. "The Association between Two-Stage Tourniquet Application during Total Knee Replacement and Blood Loss: A Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 6: 1682. https://doi.org/10.3390/jcm11061682