
Effects of Iloprost on Oxygenation during One-Lung Ventilation in Patients with Low Diffusing Capacity for Carbon Monoxide: A Randomized Controlled Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Anesthetic Management
2.3. Study Design and Outcome Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karzai, W.; Schwarzkopf, K. Hypoxemia during one-lung ventilation: Prediction, prevention, and treatment. Anesthesiology 2009, 110, 1402–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumb, A.B.; Slinger, P. Hypoxic pulmonary vasoconstriction: Physiology and anesthetic implications. Anesthesiology 2015, 122, 932–946. [Google Scholar] [CrossRef] [PubMed]
- Campos, J.H.; Peacher, D. Application of Continuous Positive Airway Pressure During Video-Assisted Thoracoscopic Surgery. Curr. Anesth. Rep. 2021, 11, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Neder, J.A.; Berton, D.C.; Muller, P.T.; O’Donnell, D.E. Incorporating Lung Diffusing Capacity for Carbon Monoxide in Clinical Decision Making in Chest Medicine. Clin. Chest Med. 2019, 40, 285–305. [Google Scholar] [CrossRef] [PubMed]
- Cerfolio, R.J.; Bryant, A.S. Different diffusing capacity of the lung for carbon monoxide as predictors of respiratory morbidity. Ann. Thorac. Surg. 2009, 88, 405–410; discussion 401–410. [Google Scholar] [CrossRef]
- Pieretti, P.; Alifano, M.; Roche, N.; Vincenzi, M.; Forti Parri, S.N.; Zackova, M.; Boaron, M.; Zanello, M. Predictors of an appropriate admission to an ICU after a major pulmonary resection. Respiration 2006, 73, 157–165. [Google Scholar] [CrossRef]
- Ertan, C.; Tarakci, N.; Ozeke, O.; Demir, A.D. Pulmonary artery distensibility in chronic obstructive pulmonary disease. Echocardiography 2013, 30, 940–944. [Google Scholar] [CrossRef]
- Dernaika, T.A.; Beavin, M.; Kinasewitz, G.T. Iloprost improves gas exchange and exercise tolerance in patients with pulmonary hypertension and chronic obstructive pulmonary disease. Respiration 2010, 79, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Sawheny, E.; Ellis, A.L.; Kinasewitz, G.T. Iloprost improves gas exchange in patients with pulmonary hypertension and ARDS. Chest 2013, 144, 55–62. [Google Scholar] [CrossRef]
- Blanc, B. Nutritional anemias. Report of a WHO Scientific Group. WHO Tech. Rep. Ser. 1968, 405, 1–40. [Google Scholar]
- Hardman, J.G.; Aitkenhead, A.R. Estimation of alveolar deadspace fraction using arterial and end-tidal CO2: A factor analysis using a physiological simulation. Anaesth. Intensive Care 1999, 27, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, R.H.; Wallace, W.D.; Nouraie, S.M.; Chan, S.Y.; Risbano, M.G. Lower DLco% identifies exercise pulmonary hypertension in patients with parenchymal lung disease referred for dyspnea. Pulm. Circ. 2020, 10, 2045894019891912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farha, S.; Asosingh, K.; Xu, W.; Sharp, J.; George, D.; Comhair, S.; Park, M.; Tang, W.H.; Loyd, J.E.; Theil, K.; et al. Hypoxia-inducible factors in human pulmonary arterial hypertension: A link to the intrinsic myeloid abnormalities. Blood 2011, 117, 3485–3493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macintyre, N.; Crapo, R.O.; Viegi, G.; Johnson, D.C.; van der Grinten, C.P.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Enright, P.; et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur. Respir J. 2005, 26, 720–735. [Google Scholar] [CrossRef] [PubMed]
- van Heerden, P.V.; Barden, A.; Michalopoulos, N.; Bulsara, M.K.; Roberts, B.L. Dose-response to inhaled aerosolized prostacyclin for hypoxemia due to ARDS. Chest 2000, 117, 819–827. [Google Scholar] [CrossRef]
- Choi, H.; Jeon, J.; Huh, J.; Koo, J.; Yang, S.; Hwang, W. The Effects of Iloprost on Oxygenation During One-Lung Ventilation for Lung Surgery: A Randomized Controlled Trial. J. Clin. Med. 2019, 8, 982. [Google Scholar] [CrossRef] [Green Version]
- Boeck, L.; Tamm, M.; Grendelmeier, P.; Stolz, D. Acute effects of aerosolized iloprost in COPD related pulmonary hypertension—A randomized controlled crossover trial. PLoS ONE 2012, 7, e52248. [Google Scholar] [CrossRef]
- Wang, L.; Jin, Y.Z.; Zhao, Q.H.; Jiang, R.; Wu, W.H.; Gong, S.G.; He, J.; Liu, J.M.; Jing, Z.C. Hemodynamic and gas exchange effects of inhaled iloprost in patients with COPD and pulmonary hypertension. Int. J. Chronic. Obstr. Pulm. Dis. 2017, 12, 3353–3360. [Google Scholar] [CrossRef] [Green Version]
- Aren, C.; Blomstrand, C.; Wikkelso, C.; Radegran, K. Hypotension induced by prostacyclin treatment during cardiopulmonary bypass does not increase the risk of cerebral complications. J. Thorac. Cardiovasc. Surg. 1984, 88, 748–753. [Google Scholar] [CrossRef]
- Wang, J.S. Relationship of carbon monoxide pulmonary diffusing capacity to postoperative cardiopulmonary complications in patients undergoing pneumonectomy. Kaohsiung J. Med. Sci 2003, 19, 437–446. [Google Scholar] [CrossRef] [Green Version]
- Datta, D.; Lahiri, B. Preoperative evaluation of patients undergoing lung resection surgery. Chest 2003, 123, 2096–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Battaglini, D.; Ball, L.; Wittenstein, J.; Cohen, E.; Gama, D.E.A.M.; Pelosi, P. PEEP in thoracic anesthesia: Pros and cons. Minerva Anestesiol. 2021, 87, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Turnaoglu, S.; Tugrul, M.; Camci, E.; Cakar, N.; Akinci, O.; Ergin, P. Clinical applicability of the substitution of mixed venous oxygen saturation with central venous oxygen saturation. J. Cardiothorac. Vasc. Anesth. 2001, 15, 574–579. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
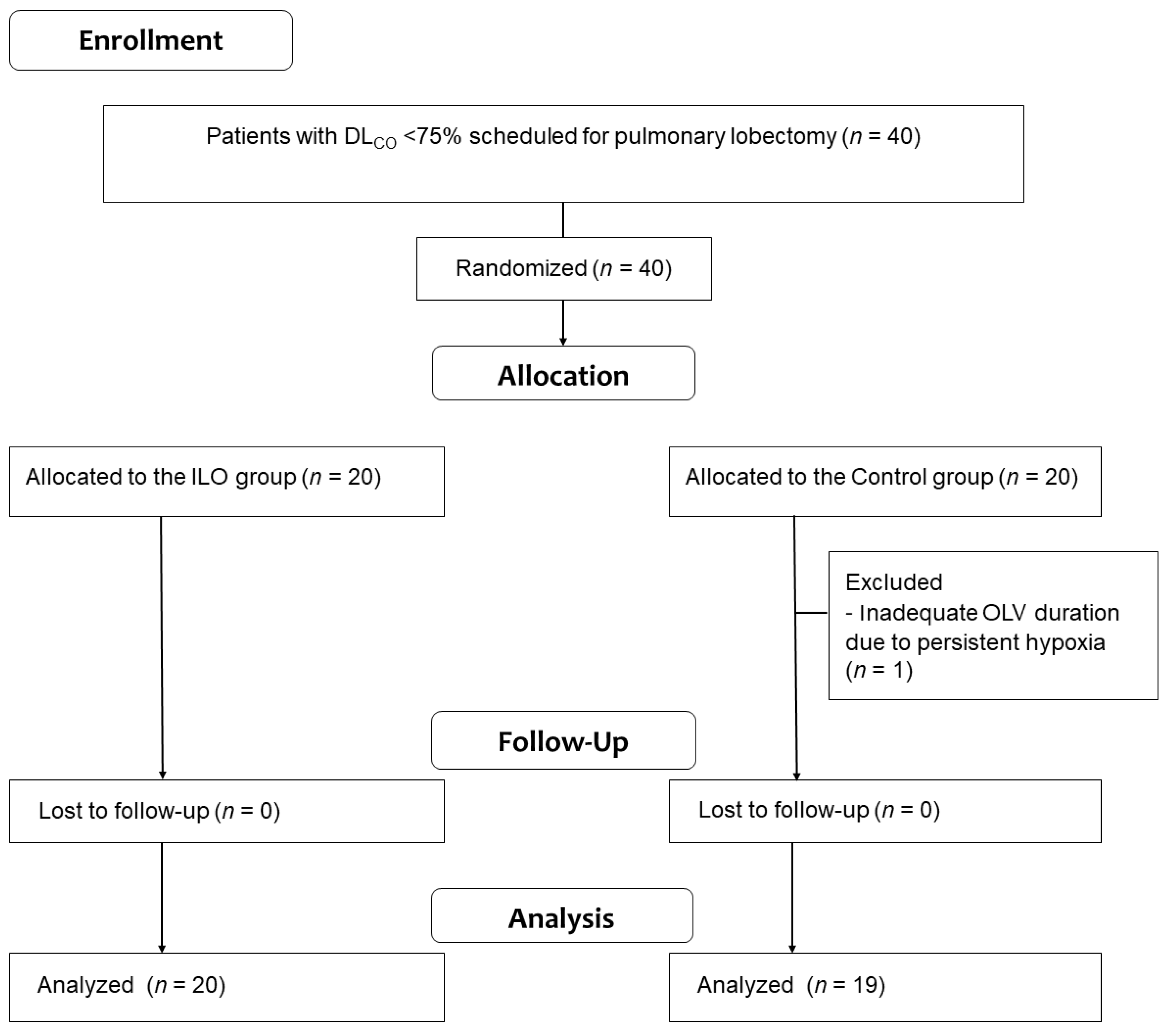
| ILO Group (n = 20) | Control Group (n = 19) | p-Value | |
|---|---|---|---|
| Age (years) | 68 ± 9 | 63 ± 10 | 0.173 |
| Women (n) | 10 (50) | 6 (31.6) | 0.242 |
| Height (cm) | 159.3 ± 10.4 | 164.2 ± 9.5 | 0.125 |
| Weight (kg) | 63.8 ± 11.9 | 68.1 ± 12.8 | 0.280 |
| Body mass index (kg/m2) | 24.7 ± 4.4 | 25.0 ± 3.6 | 0.674 |
| ASA classification 2/3 (n) | 11 (55)/9 (45) | 9 (47.4)/10 (52.6) | 0.634 |
| Hypertension (n) | 6 (30) | 7 (37) | 0.651 |
| Diabetes mellitus (n) | 4 (20) | 4 (21) | 0.935 |
| Smoking history | 0.113 | ||
| Ex-smoker or current smoker (n) | 11 (55) | 15 (78.9) | |
| Nonsmoker (n) | 9 (45) | 4 (21.1) | |
| Smoking index (pack × years) | 10 (0–50) | 31 (3–41) | 0.398 |
| Preoperative chest CT | |||
| Atelectasis (n) | 2 (10) | 0 (0) | 0.157 |
| Bronchiectasis (n) | 2 (10) | 0 (0) | 0.157 |
| Pleural effusion (n) | 1 (5) | 2 (11) | 0.517 |
| Emphysema (n) | 10 (50) | 7 (36.8) | 0.408 |
| Interstitial lung disease (n) | 3 (15) | 5 (26.3) | 0.382 |
| Preoperative spirometry | |||
| FEV1 (L) | 1.9 ± 0.6 | 2.6 ± 2.3 | 0.173 |
| FEV1 (% predicted) | 88.9 ± 20.7 | 83.3 ± 17.7 | 0.368 |
| FVC (L) | 2.8 ± 0.9 | 3.1 ± 1.0 | 0.320 |
| FVC (% predicted) | 89.5 ± 15.6 | 84.7 ± 19.0 | 0.388 |
| FEV1/FVC (%) | 69.6 ± 11.1 | 71.5 ± 13.6 | 0.517 |
| DLCO (% predicted) | 65.5 ± 6.1 | 61.1 ± 10.6 | 0.117 |
| ILO Group (n = 20) | Control Group (n = 19) | p-Value | |
|---|---|---|---|
| Initial SpO2 at room air (%) | 98 (97–99) | 96.0 (95–99) | 0.918 |
| Lobectomy (right/left) (n) | 11 (55)/9 (45) | 9 (47)/10 (53) | 0.634 |
| Anesthesia time (min) | 200 (180–225) | 183 (151–233) | 0.473 |
| Operation time (min) | 138 (120–161) | 118 (100–175) | 0.336 |
| OLV time (min) | 115 (95–135) | 103 (81–149) | 0.603 |
| Hypotension (n) | 8 (40.0) | 12 (63.2) | 0.206 |
| Hypoxia (n) | 1 (5.0) * | 6 (31.6) | 0.031 |
| Intake fluid (mL) | 1315.8 ± 316.9 | 1454.0 ± 581.3 | 0.356 |
| Urine output (mL) | 241.3 ± 161.1 | 256.4 ± 152.3 | 0.768 |
| Estimated blood loss (mL) | 102.5 ± 63.8 | 136.0 ± 110.6 | 0.248 |
| ILO Group (n = 20) | Control Group (n = 19) | p-Value | |
|---|---|---|---|
| FiO2 | 0.157 | ||
| T1 | 0.6 (0.6–0.9) | 0.6 (0.6–0.7) | |
| T2 | 0.6 (0.6–0.8) | 0.8 (0.6–0.8) | |
| PaO2/FiO2 ratio (mmHg) | 0.025 | ||
| T1 | 125.9 (100.1–222.0) | 138.3 (110.0–191.7) | |
| T2 | 141.4 (120.8–247.7) *† | 128.3 (100.0–161.8) | |
| PaO2 (mmHg) | 0.044 | ||
| T1 | 84.8 (70.3–139.7) | 83.0 (74.0–116.0) | |
| T2 | 104.7 (82.3–148.6) *† | 81.0 (81.0–110.3) | |
| SaO2 (%) | 0.026 | ||
| T1 | 95.0 (92.8–98.5) | 94.2 (92.8–97.3) | |
| T2 | 97.1 (95.5–99.8) *† | 95.3 (92.2–97.3) | |
| Pulmonary shunt (%) | 0.027 | ||
| T1 | 27.0 ± 17.9 | 25.1 ± 17.8 | |
| T2 | 18.4 ± 11.8 * | 26.6 ± 14.4 | |
| Alveolar dead space | 0.042 | ||
| T1 | 16.4 ± 5.0 | 19.2 ± 11.6 | |
| T2 | 10.8 ± 7.3 *† | 19.2 ± 11.0 | |
| Dynamic compliance (mL/cm H2O) | 0.055 | ||
| T1 | 20.0 ± 5.3 | 21.4 ± 4.7 | |
| T2 | 21.5 ± 7.9 | 20.2 ± 4.5 |
| ILO Group (n = 20) | Control Group (n = 19) | p-Value | |
|---|---|---|---|
| Hospital days | 6 (5–8) | 7 (4–9) | 0.540 |
| Postoperative complications | 3 (15.0) | 6 (31.6) | 0.219 |
| Air leak | 1 (5.0) | 3 (15.8) | 0.267 |
| Pneumonia | 2 (10.0) | 4 (21.1) | 0.339 |
| In-hospital mortality | 1 (5.0) | 2 (5.3) | 0.970 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.; Oh, Y.J.; Kim, M.; Song, S.H.; Kim, N. Effects of Iloprost on Oxygenation during One-Lung Ventilation in Patients with Low Diffusing Capacity for Carbon Monoxide: A Randomized Controlled Study. J. Clin. Med. 2022, 11, 1542. https://doi.org/10.3390/jcm11061542
Lee K, Oh YJ, Kim M, Song SH, Kim N. Effects of Iloprost on Oxygenation during One-Lung Ventilation in Patients with Low Diffusing Capacity for Carbon Monoxide: A Randomized Controlled Study. Journal of Clinical Medicine. 2022; 11(6):1542. https://doi.org/10.3390/jcm11061542
Chicago/Turabian StyleLee, Kyuho, Young Jun Oh, Mina Kim, Sei Han Song, and Namo Kim. 2022. "Effects of Iloprost on Oxygenation during One-Lung Ventilation in Patients with Low Diffusing Capacity for Carbon Monoxide: A Randomized Controlled Study" Journal of Clinical Medicine 11, no. 6: 1542. https://doi.org/10.3390/jcm11061542