
Impact on Postoperative Pain and Recovery of a Regional Analgesia Strategy Based on the Surgical Approach for Lung Resection: A Prospective Observational Study

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
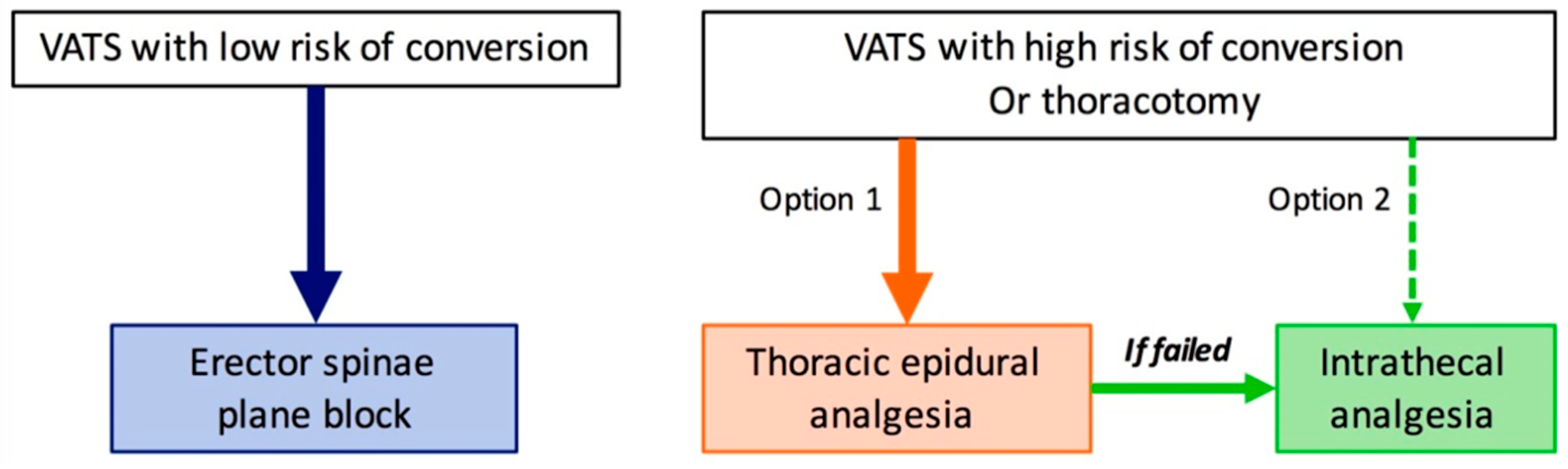
2.2. Unit Procedure for Analgesic Management
2.3. Outcome Measurements
2.4. Data Analysis
3. Results
3.1. Population Characteristics
3.2. Anesthetic and Surgical Data
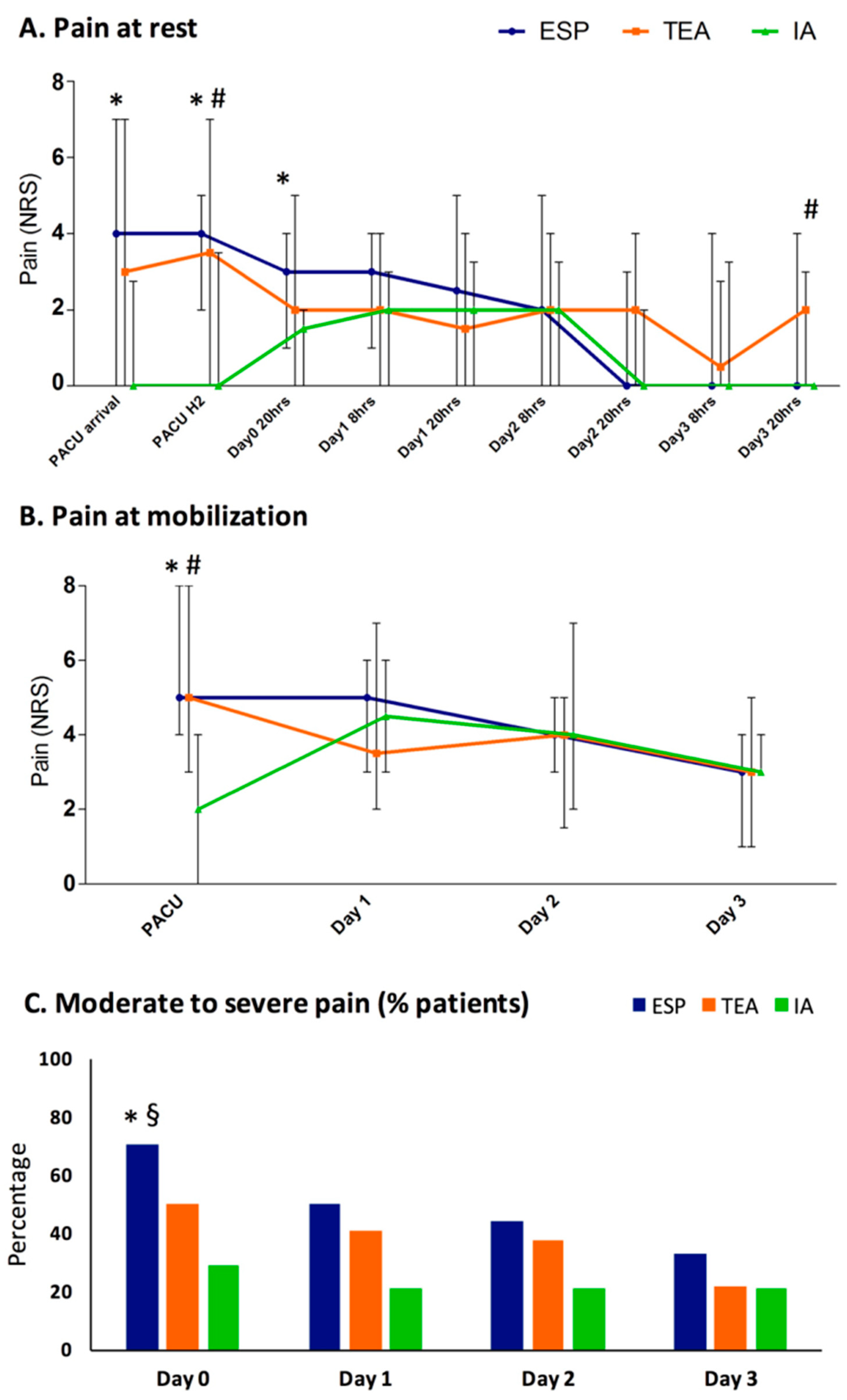
3.3. Postoperative Pain
3.4. Postoperative Recovery
3.5. Post Hoc Analysis in Patients Who Underwent a Thoracotomy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kalso, E.; Perttunen, K.; Kaasinen, S. Pain after thoracic surgery. Acta Anaesthesiol. Scand. 1992, 36, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.; Jackson, M.; Kavanagh, B.P.; Sandler, A.N. Acute Pain after Thoracic Surgery Predicts Long-Term Post-Thoracotomy Pain. Clin. J. Pain 1996, 12, 50–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lederman, D.; Easwar, J.; Feldman, J.; Shapiro, V. Anesthetic considerations for lung resection: Preoperative assessment, intraoperative challenges and postoperative analgesia. Ann. Transl. Med. 2019, 7, 356. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardio-Thorac. Surg. 2019, 55, 91–115. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H.; Rung, G.W.; Callesen, T. Postoperative opioid analgesia: Time for a reconsideration? J. Clin. Anesth. 1996, 8, 441–445. [Google Scholar] [CrossRef]
- Gottschalk, A.; Cohen, S.P.; Yang, S.; Ochroch, E.A.; Warltier, D.C. Preventing and Treating Pain after Thoracic Surgery. Anesthesiology 2006, 104, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, M.; Mori, T.; Kobayashi, H.; Iwatani, K.; Yoshimoto, K.; Terasaki, H.; Nomori, H. The efficacy of epidural analgesia after video-assisted thoracoscopic surgery: A randomized control study. Ann. Thorac. Cardiovasc. Surg. 2006, 12, 313–318. [Google Scholar] [PubMed]
- Schultz, A.-M.; Werba, A.; Ulbing, S.; Gollmann, G.; Lehofer, F. Peri-operative thoracic epidural analgesia for thoracotomy. Eur. J. Anaesthesiol. 1997, 14, 600–603. [Google Scholar] [CrossRef] [PubMed]
- Zoumprouli, A.; Chatzimichali, A.; Papadimitriou, S.; Papaioannou, A.; Xynos, E.; Askitopoulou, H. Gastrointestinal motility following thoracic surgery: The effect of thoracic epidural analgesia. A randomised controlled trial. BMC Anesthesiol. 2017, 17, 139. [Google Scholar] [CrossRef] [Green Version]
- Scherer, R.; Schmutzler, M.; Giebler, R.; Erhard, J.; Stöcker, L.; Kox, W. Complications related to thoracic epidural analgesia: A prospective study in 1071 surgical patients. Acta Anaesthesiol. Scand. 1993, 37, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Manassero, A.; Bossolasco, M.; Carrega, M.; Coletta, G. Postoperative Thoracic Epidural Analgesia: Adverse Events from a Single-Center Series of 3126 Patients. Local Reg. Anesth. 2020, 13, 111–119. [Google Scholar] [CrossRef]
- Boisen, M.L.; Sardesai, M.P.; Kolarczyk, L.; Rao, V.K.; Owsiak, C.P.; Gelzinis, T.A. The Year in Thoracic Anesthesia: Selected Highlights From 2017. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1556–1569. [Google Scholar] [CrossRef]
- Okajima, H.; Tanaka, O.; Ushio, M.; Higuchi, Y.; Nagai, Y.; Iijima, K.; Horikawa, Y.; Ijichi, K. Ultrasound-guided continuous thoracic paravertebral block provides comparable analgesia and fewer episodes of hypotension than continuous epidural block after lung surgery. J. Anesth. 2015, 29, 373–378. [Google Scholar] [CrossRef]
- Yeung, J.; Gates, S.; Naidu, B.V.; A Wilson, M.J.; Smith, F.G. Paravertebral block versus thoracic epidural for patients undergoing thoracotomy. Cochrane Database Syst. Rev. 2016, 2, CD009121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogt, A.; Stieger, D.S.; Theurillat, C.; Curatolo, M. Single-injection thoracic paravertebral block for postoperative pain treatment after thoracoscopic surgery. Br. J. Anaesth. 2005, 95, 816–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marret, E.; Bazelly, B.; Taylor, G.; Lembert, N.; Deleuze, A.; Mazoit, J.-X.; Bonnet, F.J. Paravertebral Block With Ropivacaine 0.5% Versus Systemic Analgesia for Pain Relief After Thoracotomy. Ann. Thorac. Surg. 2005, 79, 2109–2113. [Google Scholar] [CrossRef] [PubMed]
- Berna, P.; Quesnel, C.; Assouad, J.; Bagan, P.; Etienne, H.; Fourdrain, A.; Le Guen, M.; Leone, M.; Lorne, E.; Nguyen, Y.-L.; et al. Guidelines on enhanced recovery after pulmonary lobectomy. Anaesth. Crit. Care Pain Med. 2021, 40, 100791. [Google Scholar] [CrossRef] [PubMed]
- Forero, M.; Adhikary, S.; Lopez, H.; Tsui, C.; Chin, K.J. The Erector Spinae Plane Block: A Novel Analgesic Technique in Thoracic Neuropathic Pain. Reg. Anesth. Pain Med. 2016, 41, 621–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsui, B.C.H.; Fonseca, A.; Munshey, F.; McFadyen, G.; Caruso, T.J. The erector spinae plane (ESP) block: A pooled review of 242 cases. J. Clin. Anesth. 2019, 53, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Pirsaharkhiz, N.; Comolli, K.; Fujiwara, W.; Stasiewicz, S.; Boyer, J.M.; Begin, E.V.; Rubinstein, A.J.; Henderson, H.R.; Lazar, J.F.; Watson, T.J.; et al. Utility of erector spinae plane block in thoracic surgery. J. Cardiothorac. Surg. 2020, 15, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Forero, M.; Rajarathinam, M.; Adhikary, S.; Chin, K.J. Erector spinae plane (ESP) block in the management of post thoracotomy pain syndrome: A case series. Scand. J. Pain 2017, 17, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Kuhlman, G.; Dalibon, N.; Moutafis, M.; Levron, J.-C.; Fischler, M. A Randomized, Double-Blinded Comparison of Intrathecal Morphine, Sufentanil and their Combination versus IV Morphine Patient-Controlled Analgesia for Postthoracotomy Pain. Anesth. Analg. 2001, 92, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Madi-Jebara, S.; Adaimé, C.; Yazigi, A.; Haddad, F.; Hayek, G.; Sleilaty, G.; Antakly, M.-C. Thoracic epidural and intrathecal analgesia have similar effects on pain relief and respiratory function after thoracic surgery. Can. J. Anaesth. 2005, 52, 710–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, N.; Gondret, R.; Junca, A.; Bonnet, F. Intrathecal sufentanil and morphine for post-thoracotomy pain relief. Br. J. Anaesth. 2001, 86, 236–240. [Google Scholar] [CrossRef] [Green Version]
- Meylan, N.; Elia, N.; Lysakowski, C.; Tramèr, M.R. Benefit and risk of intrathecal morphine without local anaesthetic in patients undergoing major surgery: Meta-analysis of randomized trials. Br. J. Anaesth. 2009, 102, 156–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Block, B.M.; Liu, S.S.; Rowlingson, A.J.; Cowan, A.R.; Cowan, J.J.A.; Wu, C.L. Efficacy of Postoperative Epidural Analgesia: A meta-analysis. JAMA 2003, 290, 2455–2463. [Google Scholar] [CrossRef] [PubMed]
- Pöpping, D.M.; Elia, N.; Marret, E.; Remy, C.; Tramèr, M.R. Protective Effects of Epidural Analgesia on Pulmonary Complications After Abdominal and Thoracic Surgery: A meta-analysis. Arch. Surg. Chic. Ill 2008, 143, 990–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bendixen, M.; Jørgensen, O.D.; Kronborg, C.; Andersen, C.; Licht, P.B. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: A randomised controlled trial. Lancet Oncol. 2016, 17, 836–844. [Google Scholar] [CrossRef]
- Chin, K.J. Thoracic wall blocks: From paravertebral to retrolaminar to serratus to erector spinae and back again – A review of evidence. Best Pract. Res. Clin. Anaesthesiol. 2019, 33, 67–77. [Google Scholar] [CrossRef]
- Júnior, A.d.P.J.; Erdmann, T.R.; dos Santos, T.V.; Brunharo, G.M.; Filho, C.T.B.; Losso, M.J.; Filho, G.R.D.O. Comparison between Continuous Thoracic Epidural and Paravertebral Blocks for Postoperative Analgesia in Patients Undergoing Thoracotomy: Systematic Review. Braz. J. Anesthesiol. 2013, 63, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Hill, S.E.; Keller, R.A.; Stafford-Smith, M.; Grichnik, K.; White, W.D.; D’Amico, T.A.; Newman, M.F. Efficacy of Single-dose, Multilevel Paravertebral Nerve Blockade for Analgesia after Thoracoscopic Procedures. Anesthesiology 2006, 104, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Park, M.H.; Kim, J.A.; Ahn, H.J.; Yang, M.K.; Son, H.J.; Seong, B.G. A randomised trial of serratus anterior plane block for analgesia after thoracoscopic surgery. Anaesthesia 2018, 73, 1260–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, B.; Wang, Z.; Huang, X. Ultrasound-guided preoperative single-dose erector spinae plane block provides comparable analgesia to thoracic paravertebral block following thoracotomy: A single center randomized controlled double-blind study. Ann. Transl. Med. 2019, 7, 174. [Google Scholar] [CrossRef]
- Van Der Ploeg, A.P.T.; Ayez, N.; Akkersdijk, G.P.; Van Rossem, C.C.; De Rooij, P.D. Postoperative pain after lobectomy: Robot-assisted, video-assisted and open thoracic surgery. J. Robot. Surg. 2020, 14, 131–136. [Google Scholar] [CrossRef]
- Pitre, L.; Garbee, D.; Tipton, J.; Schiavo, J.; Pitt, A. Effect of intrathecal morphine plus patient-controlled analgesia with morphine versus patient-controlled analgesia with morphine alone on total morphine dosage 24 hours after surgery: A systematic review. JBI Evid. Synth. 2020. [Google Scholar] [CrossRef]
- Helander, E.M.; Webb, M.P.; Kendrick, J.; Montet, T.; Kaye, A.J.; Cornett, E.M.; Kaye, A.D. PECS, serratus plane, erector spinae, and paravertebral blocks: A comprehensive review. Best Pract. Res. Clin. Anaesthesiol. 2019, 33, 573–581. [Google Scholar] [CrossRef]
- Dango, S.; Harris, S.; Offner, K.; Hennings, E.; Priebe, H.-J.; Buerkle, H.; Passlick, B.; Loop, T. Combined paravertebral and intrathecal vs thoracic epidural analgesia for post-thoracotomy pain relief. Br. J. Anaesth. 2012, 110, 443–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciftci, B.; Ekinci, M.; Celik, E.C.; Tukac, I.C.; Bayrak, Y.; Atalay, Y.O. Efficacy of an Ultrasound-Guided Erector Spinae Plane Block for Postoperative Analgesia Management After Video-Assisted Thoracic Surgery: A Prospective Randomized Study. J. Cardiothorac. Vasc. Anaesth. 2020, 34, 444–449. [Google Scholar] [CrossRef]
- Zhao, H.; Xin, L.; Feng, Y. The effect of preoperative erector spinae plane vs. paravertebral blocks on patient-controlled oxycodone consumption after video-assisted thoracic surgery: A prospective randomized, blinded, non-inferiority study. J. Clin. Anaesth. 2020, 62, 109737. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All Patients (n = 116) | ESP Group (n = 70) | TEA Group (n = 32) | IA Group (n = 14) | p | |
|---|---|---|---|---|---|
| Patients’ characteristics | |||||
| Age (years) | 64 (11) | 64 (11) | 63 (10) | 66 (12) | 0.48 |
| Male | 73 (63%) | 41 (59%) | 21 (66%) | 11 (79%) | 0.32 |
| Height (cm) | 169 (9) | 169 (9) | 169 (8) | 170 (10) | 0.76 |
| Weight (kg) | 72 (17) | 70 (16) | 72 (18) | 81 (22) | 0.16 |
| ASA status | |||||
| I | 5 (4%) | 2 (3%) | 2 (6%) | 1 (7%) | 0.64 |
| II | 47 (41%) | 28 (40%) | 14 (44%) | 5 (36%) | 0.87 |
| III | 63 (54%) | 39 (56%) | 16 (50%) | 8 (57%) | 0.84 |
| IV | 1 (9%) | 1 (1%) | 0 | 0 | 0.72 |
| Medical history | |||||
| COPD | 39 (34%) | 19 (27%) | 16 (50%) | 4 (29%) | 0.08 |
| Active smokers | 27 (23%) | 16 (23%) | 7 (22%) | 4 (29%) | 0.88 |
| Previous thoracic surgery | 24 (21%) | 13 (19%) | 8 (25%) | 3 (21%) | 0.76 |
| Previous thoracic radiotherapy | 10 (9%) | 6 (9%) | 3 (9%) | 1 (7%) | 0.97 |
| Diabetes | 18 (16%) | 12 (17%) | 5 (16%) | 1 (7%) | 0.59 |
| Chronic alcoholism | 15 (13%) | 10 (14%) | 4 (12%) | 1 (7%) | 0.74 |
| Psychiatric disease | 8 (7%) | 4 (6%) | 3 (9%) | 1 (7%) | 0.80 |
| Chronic pain | 24 (21%) | 16 (23%) | 5 (16%) | 3 (21%) | 0.69 |
| Preoperative respiratory function | |||||
| FEV1 (L) | 2.4 (1.9–2.9) | 2.5 (1.9–3.0) | 2.4 (1.8–2.8) | 2.0 (1.8–3.1) | 0.36 |
| Tiffeneau index | 71 (61–79) | 71 (63–80) | 66 (57–78) | 69 (60–78) | 0.28 |
| Surgical indication | |||||
| Diagnostic biopsy | 5 (4%) | 4 (6%) | 0 | 1 (7%) | 0.36 |
| Lung infection | 2 (2%) | 1 (1%) | 0 | 1 (7%) | 0.22 |
| Tumour resection | 107 (92%) | 65 (93%) | 30 (93%) | 12 (86%) | 0.62 |
| Other | 2 (2%) | 0 | 2 (6%) | 0 | 0.07 |
| All Patients (n = 116) | ESP Group (n = 70) | TEA Group (n = 32) | IA Group (n = 14) | ESP vs. TEA p Value | ESP vs. IA p Value | TEA vs. IA p Value | |
|---|---|---|---|---|---|---|---|
| Intravenous anesthesia | |||||||
| Remifentanil (mg) | 1.6 (1.0–2.0) | 1.5 (0.9–1.9) | 1.8 (1.4–2.6) | 2.0 (1.5–2.6) | <0.01 | 0.01 | 0.74 |
| Propofol (g) | 1.7 (1.4–2.4) | 1.6 (1.3–2.3) | 1.9 (1.5–2.5) | 2.2 (1.6–3.2) | 0.07 | 0.01 | 0.24 |
| IV morphine equivalent (mg) | 4 (4–5) | 4 (4–5) | 4 (4–5) | 5 (3.75–5.25) | 0.57 | 0.9 | 0.69 |
| Paracetamol | 113 (97%) | 69 (98%) | 30 (94%) | 14 (100%) | 0.23 | 1 | 1 |
| Nefopam | 70 (60%) | 43 (61%) | 19 (59%) | 8 (57%) | 1 | 0.77 | 1 |
| NSAIDs | 22 (19%) | 18 (26%) | 2 (6%) | 2 (14%) | 0.03 | 0.5 | 0.57 |
| Ketamine | 78 (67%) | 52 (74%) | 23 (72%) | 3 (21%) | 0.81 | <0.01 | <0.01 |
| Surgical incision | |||||||
| Primary thoracotomy | 38 (33%) | 3 (4%) | 27 (84%) | 8 (57%) | <0.01 | <0.01 | 0.24 |
| Converted VATS | 8 (7%) | 3 (4%) | 0 | 1 (%) | 0.55 | 0.52 | 0.3 |
| Not converted VATS | 70 (60%) | 64 (91%) | 5 (16%) | 5 (%) | <0.01 | <0.01 | 0.24 |
| Type of resection | |||||||
| Lobectomy | 69 (59%) | 37 (53%) | 23 (72%) | 9 (64%) | <0.01 | 0.24 | 0.17 |
| Pneumonectomy | 7 (6%) | 0 | 6 (19%) | 1 (7%) | <0.01 | 0.16 | 0.65 |
| Segmentectomy | 7 (6%) | 7 (10%) | 0 | 0 | 0.33 | 1 | 0.41 |
| Wedge | 32 (28%) | 26 (37%) | 2 (6%) | 4 (29%) | 0.26 | 1 | 0.49 |
| Biopsy | 1 (8%) | 0 | 1 (3%) | 0 | <0.01 | 0.02 | 0.4 |
| Curage | 80 (69%) | 43 (61%) | 26 (81%) | 11 (79%) | 0.06 | 0.3 | 1 |
| Drains | 1 (1–2) | 1 (1–1) | 2 (1–2) | 1.5 (1–2) | <0.01 | 0.01 | 0.57 |
| Rib fractures | 4 (3%) | 1 (1%) | 3 (9%) | 0 | 0.09 | 1 | 0.54 |
| Operating room time (min) | 173 (134–210) | 170 (129–204) | 191 (143–238) | 170 (150–219) | 0.03 | 0.44 | 0.42 |
| PACU time (min) | 131 (114–169) | 132 (120–165) | 120 (84–256) | 131 (67–195) | 0.39 | 0.7 | 0.88 |
| All Patients (n = 116) | ESP Group (n = 70) | TEA Group (n = 32) | IA Group (n = 14) | ESP vs. TEA p Value | ESP vs. IA p Value | TEA vs. IA p Value | |
|---|---|---|---|---|---|---|---|
| IV or oral opioid use | |||||||
| Day 0 | 115 (99%) | 70 (100%) | 31 (97%) | 14 (100%) | 0.31 | 1 | 1 |
| Day 1 | 95 (82%) | 64 (91%) | 19 (59%) | 12 (86%) | <0.01 | 0.61 | 0.09 |
| Day 2 | 84 (72%) | 50 (71%) | 24 (75%) | 10 (71%) | 0.81 | 1 | 1.0 |
| Day 3 | 69 (59%) | 38 (54%) | 23 (71%) | 8 (57%) | 0.12 | 1 | 0.49 |
| IV morphine equivalent (for oral or IV opioids) (mg) | |||||||
| H2 | 3 (0–7) | 5 (0–8) | 0 (0–3.5) | 0 (0–4.5) | <0.01 | 0.03 | 0.97 |
| Day 0 | 14 (5–25) | 16 (7–25) | 10 (0–27) | 16 (5–33) | 0.16 | 0.94 | 0.46 |
| Day 1 | 12.3 (2.5–23.3) | 12 (6.5–22) | 6.5 (0–35) | 16 (6–24.5) | 0.31 | 0.6 | 0.49 |
| Day 2 | 10 (0–14.1) | 8.8 (0–12.5) | 11 (0.3–29.5) | 7.5 (0–16.3) | 0.05 | 0.69 | 0.28 |
| Day 3 | 5 (0–10) | 5 (0–10) | 10 (0–18) | 2.75 (0–10) | <0.01 | 0.9 | 0.049 |
| Total | 44 (28.9–73.3) | 44 (28.9–73.3) | 41 (18–94.9) | 57 (19.1–77.1) | 0.96 | 0.80 | 0.86 |
| All Patients (n = 116) | ESP Group (n = 70) | TEA Group (n = 32) | IA Group (n = 14) | ESP vs. TEA p Value | ESP vs. IA p Value | TEA vs. IA p Value | |
|---|---|---|---|---|---|---|---|
| First time setting in the chair (days) | 1 (1–1) | 1 (1–1) | 1 (1–1) | 1 (1–1) | 0.02 | 0.18 | 0.49 |
| First standing up (days) | 1 (1–1) | 1 (1–1) | 1 (1–2) | 1 (1–2) | <0.01 | 0.01 | 0.94 |
| Drain removal ≤ Day 3 | 68 59%) | 52 (74%) | 9 (28%) | 7 (50%) | <0.01 | 0.1 | 0.18 |
| Urinary catheter removal ≤ Day 3 | 76 (66%) | 39 (93%) | 25 (78%) | 12 (92%) | 0.09 | 1 | 0.4 |
| PEF (% theoretical value) | |||||||
| Day 1 | 35 (25–46) | 37 (27–47) | 35 (27–43) | 25 (21–47) | 0.62 | 0.37 | 0.44 |
| Day 2 | 30 (24–38) | 28 (24–40) | 31 (21–35) | 31 (24–38) | 0.8 | 0.8 | 0.6 |
| Day 3 | 37 (27–46) | 41 (29–46) | 31 (17–54) | 34 (29–53) | 0.19 | 0.7 | 0.42 |
| Postoperative admission to ICU (vs. ward) | 93 (80%) | 47 (67%) | 32 (100%) | 14 (100%) | <0.01 | <0.01 | 1 |
| Length of ICU stay (days) | 2 (1–4) | 1 (0–2) | 4 (3–6) | 1 (1–2.5) | <0.01 | <0.01 | <0.01 |
| Length of hospital stay (days) | 5 (3–9) | 4 (3–5) | 10 (6–15) | 6 (4–11) | <0.01 | 0.07 | 0.046 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trouillard, M.; Dupuis, W.; Siaudeau, H.; Denou, F.; Longeau, E.; Léger, M.; Ammi, M.; Sargentini, C.; Lasocki, S.; Rineau, E. Impact on Postoperative Pain and Recovery of a Regional Analgesia Strategy Based on the Surgical Approach for Lung Resection: A Prospective Observational Study. J. Clin. Med. 2022, 11, 1376. https://doi.org/10.3390/jcm11051376
Trouillard M, Dupuis W, Siaudeau H, Denou F, Longeau E, Léger M, Ammi M, Sargentini C, Lasocki S, Rineau E. Impact on Postoperative Pain and Recovery of a Regional Analgesia Strategy Based on the Surgical Approach for Lung Resection: A Prospective Observational Study. Journal of Clinical Medicine. 2022; 11(5):1376. https://doi.org/10.3390/jcm11051376
Chicago/Turabian StyleTrouillard, Marion, William Dupuis, Hélène Siaudeau, Florian Denou, Emmanuelle Longeau, Maxime Léger, Myriam Ammi, Cyril Sargentini, Sigismond Lasocki, and Emmanuel Rineau. 2022. "Impact on Postoperative Pain and Recovery of a Regional Analgesia Strategy Based on the Surgical Approach for Lung Resection: A Prospective Observational Study" Journal of Clinical Medicine 11, no. 5: 1376. https://doi.org/10.3390/jcm11051376