
Teledermatology and Inflammatory Skin Conditions during COVID-19 Era: New Perspectives and Applications

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
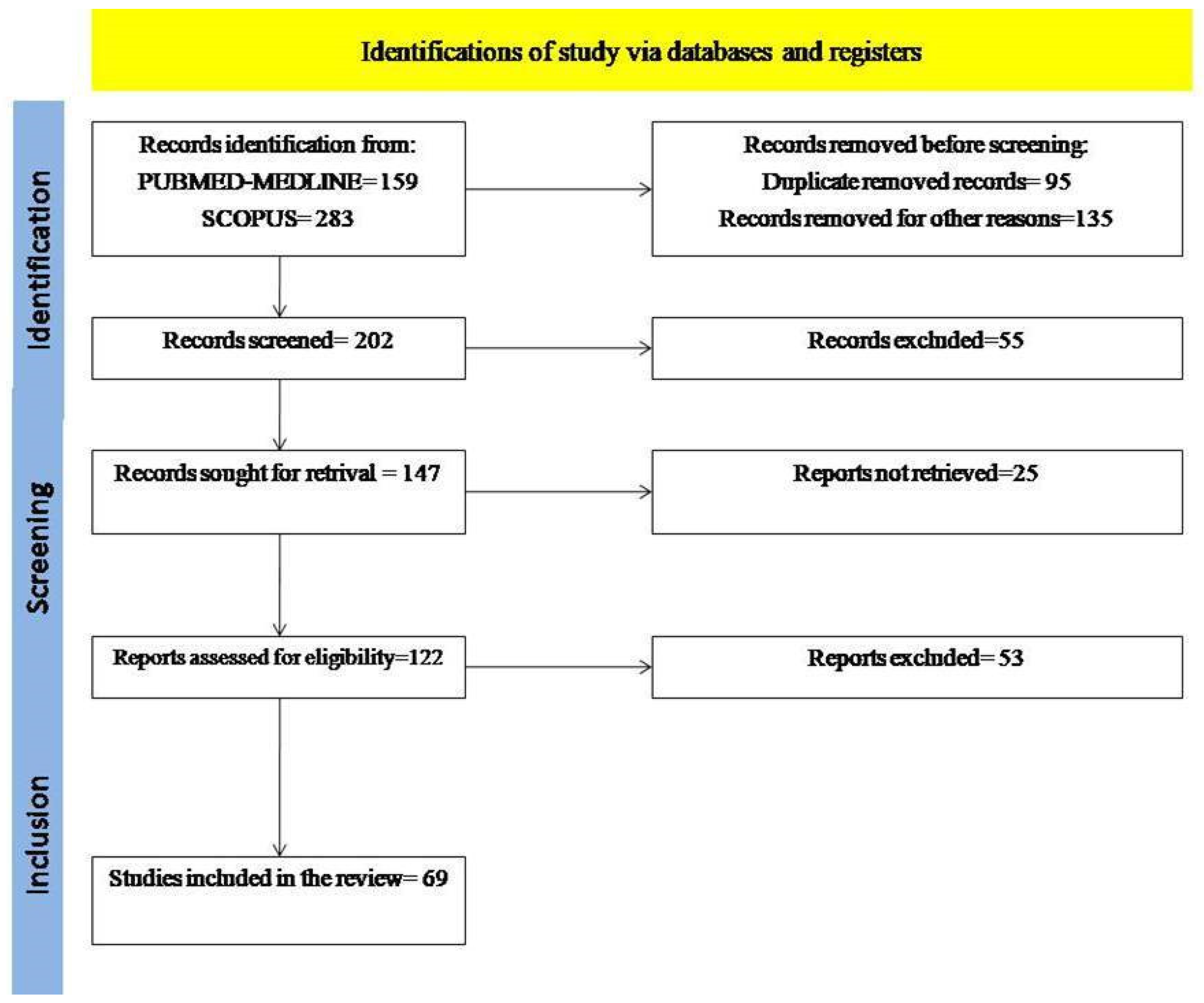
2. Materials and Methods
3. Results
3.1. Psoriasis
3.2. Acne and Hidradenitis Suppurativa
3.3. Atopic Dermatitis

{kind=link}
| Authors | Year | Country | Objectives | Main Findings |
|---|---|---|---|---|
| Dahy et al. [6] | 2020 | Egypt | To collect the evidence regarding the efficacy of telemedicine in psoriasis management. | Telemedicine (alone or in combination) had the same or higher efficacy of psoriasis management compared to usual care. |
| Muir et al. [7] | 2014 | Australia | To explore the use and potential of store-and-forward teledermatology in Australia. | The store-and-forward teledermatology increases availability and reduces time, cost, and professional isolation. Anyway, uptake is low, for lack of awareness, increased workload for referring practitioners, and lack of financial incentives. |
| Doraiswamy et al. [8] | 2020 | Qatar | To collect literature on telehealth during the COVID-19 pandemic. | Increasing literature concerning telehealth, especially from high-income countries, was reported during the first 6 months of the COVID-19 pandemic. Anyway, it should be prompted in low/middle income countries and resource-limited settings. |
| Byrom et al. [9] | 2016 | Australia | To identify the current scope of Tele-Derm, the types of dermatological complaints experienced in the rural primary care setting, and to assess the quality of patient clinical information provided to the dermatologist. | The most common dermatological complaint in rural settings was dermatitis. Children represented 1/3 of patients. The average time from submission to dermatologist’s reply was 5.5 h. Clinical photos were provided in most of the cases and displayed good quality. Management advice was provided in most cases, of which refers to the case-based learning modules on Tele-Derm was made in 21% of cases. Patient outcome was largely unknown (83%). Tele-Derm can be used as an adjunct to advice provided to rural doctors seeking advice for patient management. |
| Jemec et al. [10] | 2008 | Denmark | To show the use of telemedicine as an adjunct to conventional clinical dermatology on the Faroe Islands. | The service is based on a nurse-led dermatological clinic, and teledermatology is combined with specialist visits for more complex diagnoses or procedures. |
| Tsang et al. [11] | 2011 | USA | To characterize the conditions diagnosed through clinicopathological correlation in conjunction with photos and tissue submitted to the African Teledermatology Project. | Clinical images may not be sufficient to make a diagnosis through telemedicine consultation. Histological report of skin biopsies is an important aid for diagnosis of disease and their treatment. |
| Andersen et al. [12] | 2019 | Denmark | To review the teledermatology database of the Faroe Islands from its inauguration in 2003 to November 2018. | Teledermatology is a useful tool for dermatological conditions that do not require in-person visits in non-rural contexts; anyway, it is the only available alternative in rural areas for any kind of dermatological disease. |
| Villani et al. [13] | 2020 | Italy | To show the measures applied in the dermatologic clinic of the University of Naples Federico II, Italy, to ensure a continuous follow-up, especially for chronic skin diseases (psoriasis, acne, and hidradenitis suppurativa) during the COVID-19 pandemic. | The following services were implemented: phone consultations, video consultations through teledermatology service, and WhatsApp support group. |
| Gisondi et al. [14] | 2021 | Italy | To investigate the preference for telemedicine versus in-person visits among patients with psoriasis under biological drugs and the reported reasons behind their preferences. | About 50% of patients preferred telemedicine to an in-person visit, and the main reported reasons were saving time and safety in relation to the risk of SARS-CoV-2 infection. By contrast, the main reason to prefer in-person visits was the inability to use video-communication devices. |
| Brunasso et al. [15] | 2020 | Italy | To report the experience with teledermatologic services in smartworking using phone calls and emails for chronic skin diseases at the Department of Dermatology, Galliera Hospital, Genoa, Italy. | This real-life experience showed that remote monitoring was effective in preventing unnecessary worsening of severe chronic skin diseases and poor outcomes due to the withdrawal of current therapy. |
| Beer et al. [16] | 2021 | USA | To identify dermatological diseases that may be suitable for teledermatology versus in-person visits. | Psoriasis acne and atopic dermatitis may be managed through teledermatology. Anyway, also skin cancers may be included in the future, provided the availability of new technologies to allow the diagnosis, surveillance, and treatment. |
| Chamber et al. [17] | 2012 | USA | To compare the clinical equivalence of a novel patient-centered online health care delivery model with standard in-office care for follow-up treatment of patients with psoriasis. | PASI, DLQI, IGA improved in both online and in-office groups without significant differences. Hence, a patient-centered online model may be an effective alternative to in-office care for follow-up management of psoriasis. |
| Pearlman et al. [18] | 2021 | USA | To evaluate patients’ attitudes toward synchronous teledermatology. | Included patients were familiar with social media platforms (Facebook, hardware platforms, and apple device). About 90% of patients were satisfied with synchronous teledermatology and did not find any technical difficulty during the consult. Anyway, the majority preferred in-person visits. Thus, synchronous teledermatology allows patients to access specialty consultation. It is well-received and appreciated by patients despite technical barriers, especially during a global health crisis. |
| Frühauf et al. [19] | 2012 | Austria | To evaluate the acceptance of mobile teledermatology for the home monitoring of high-need patients with psoriasis. | Mobile teledermatology is a precious tool for the home monitoring of patients with psoriasis. Moreover, it is well accepted by both patients and physicians. |
| Yi et al. [20] | 2021 | USA | To evaluate a new practice model represented by a hybrid model of in-person and teledermatology visits at a 90% to 10% ratio, to identify trends in access to and quality of teledermatology services. | With in-person visits halted for the COVID-19 pandemic, there was a decrease in elderly and non-English-speaking patients seeking teleconsultations in dermatology, so they may experience unequal access to care. |
| Ferwerda et al. [21] | 2013 | Netherlands | To evaluate perspectives of patients with psoriasis and rheumatoid arthritis towards internet-based cognitive-behavioral treatments (CBT). | Patients appreciated the CBT as time-saving and easy to use. Anyway, the inability to use a computer and the lack of face-to-face interaction with the therapist may be a disadvantage. Hence, from the patients’ perspective, internet-based CBT is a promising health care development. |
| Adam et al. [22] | 2019 | USA | To evaluate the impact of an online, collaborative connected-health (CCH) model on psoriasis management on access to specialty care. | The CCH model resulted in less distance traveled and transportation as well as in-office waiting time compared to in-person care. Both patients and providers were highly satisfied with CCH. The CCH model resulted in increased access to specialty care and enabled patient-centered, safe, and effective management of psoriasis patients. |
| Armstrong et al. [23] | 2018 | USA | To determine if an online, collaborative connected-health model results in equivalent clinical improvements in psoriasis compared with in-person care. | The online, collaborative connected-health model was as effective as in-person management in improving clinical outcomes among patients with psoriasis. |
| Frühauf et al. [24] | 2015 | Austria | To evaluate the feasibility of teledermatology services for high-need patients with psoriasis. | The patient-driven mobile home monitoring system was feasible for high-need patients with psoriasis and actively involved them in their treatment process. Moreover, there was a strong correlation between psoriasis severity measurements and therapeutic management obtained during online and in-person visits. |
| Balato et al. [25] | 2013 | Italy | To evaluate the use of text message (TM) in improving treatment adherence and patient outcomes, such as quality of life, disease severity, patient-perceived disease severity, and the patient-physician relationship. | TM increases patients’ adherence to treatment and improves self-care and patient-physician relationships, allowing improved clinical outcomes and better control of the disease. |
| Singh et al. [26] | 2011 | Australia | To assess the feasibility of the remote determination of PASI scores by comparing the results of face-to-face with digital image assessment. | PASI scores can be determined with moderate-to-good accuracy by dermatologists using standardized digital images. Thus, the implementation of a tele-PASI service may act as an adjunct to the care of patients with severe psoriasis that are unavailable for face-to-face consultations. |
| Wu et al. [27] | 2021 | Australia | To develop and validate a model for estimating total PASI score for assessment in teledermatology (Tele-PASI). | A strong correlation between the tele-PASI scores and the original total PASI scores at baseline and during treatment was reported. Hence, a tele-PASI score may be useful in determining psoriasis severity in teledermatology settings. |
| Koller et al. [28] | 2011 | Austria | To investigate the applicability of a mobile phone-based teledermatological system for monitoring psoriasis patients on biologic therapy. | The mobile phone-based teledermatological system is useful for the long-term monitoring of patients with psoriasis under systemic therapies, such as biological drugs. |
| Klotz et al. [29] | 2005 | Canada | To investigate the use of telemedicine in the monitoring of phototherapy of psoriasis patients living in a Nova Scotia region with no dermatologist. | Telemedicine provided an excellent way to monitor patients receiving phototherapy in a region without dermatologists. Overall, patient care improved. More patients were treated effectively, with better outcomes and fewer side effects. |
| Svendsen et al. [30] | 2018 | Denmark | To review randomized controlled trials (RCTs) testing eHealth interventions designed to improve adherence to topical antipsoriatic agents and to review applications for smartphones (apps) incorporating the word psoriasis. | An improvement in medical adherence and reduction in the severity of psoriasis was reported. A total of 184 apps contained the word psoriasis. |
| Rompoti et al. [31] | 2019 | Greece | Primary endpoint was the percentage of patients who achieved a PASIreduction of 75% (PASI75) at Week 16. | An improvement in the PASI index. |
| Li et al. [32] | 2020 | To assess through phone calls the consequences of infliximab interruption in psoriatic patients during the COVID-19 pandemic. | The majority of patients had lesions exacerbation and anxiety, so it is recommended to administer common drugs for psoriasis at home. Telemedicine should be advocated as a main medical visit mode during the outbreak of COVID-19. | |
| Young et al. [33] | 2019 | USA | To evaluate how a novel online health model that facilitates physician-patient collaboration compares with in-person care for improving psoriasis patients’ functional status and mental health. | The online health model was equivalent to in-person care for reducing functional impairment and depressive symptoms in psoriasis patients. |
| Beytout et al. [34] | 2021 | France | To investigate the impact of the COVID-19 pandemic on children with psoriasis. | This study demonstrates the impact of the COVID-19 pandemic on children with psoriasis. Overall, psoriasis worsening, visit cancellation and fear to attend visits were reported. Moreover, patients felt that their psoriasis did not allow them to respect the hygiene measures, such as using an alcoholic solution, wearing the mask, and hand washing. Teleconsultations played a key role in patient management as regards patient monitoring, provision of information, and renewal of treatments. |
| Mazzuoccolo et al. [35] | 2019 | Argentina | To evaluate the implementation of a WhatsApp discussion group in Project ECHO (Extension for Community Health care Outcomes) Psoriasis in Argentina. | The Project ECHO Psoriasis was shown to be promising in reducing the gap of knowledge, promoting better clinical decisions through the empowerment of physicians working in remote areas. |
| Frühauf et al. [39] | 2015 | Austria | To examine the superiority in terms of effectiveness, safety, and patient compliance of mobile teledermatology in the care of patients with high-need facial acne in comparison to outpatient services. | Teledermatology is a useful tool among patients with high-need acne. It could be a valuable adjunct to outpatient care services. |
| Loh et al. [40] | 2021 | Singapore | To evaluate the implementation of teledermatology. | Teledermatology is an excellent tool for dermatoses management during the COVID-19 pandemic. |
| Kazi et al. [41] | 2021 | USA | To show quantitative data about the use of teledermatology. | The use of asynchronous teledermatology was preferred for acne management, whereas synchronous teledermatology was preferable to providers for complex medical dermatology. |
| Gu et al. [42] | 2021 | USA | To evaluate the features of acne visits during the pandemic. | Even if face-to-face visits were permitted, the majority of systemic acne management and about half of acne visits were conducted in telemedicine. |
| Marasca et al. [43] | 2020 | Italy | Evaluate the effectiveness of short message service to follow-up some patients. | The SMS group, who received the daily medical support by text, showed an increased treatment adherence. |
| Ruggiero et al. [44] | 2020 | Italy | To evaluate patients’ experience of teledermatology visits | Most of the patients (92.3%) appreciated the visits and the treatment received. |
| Villani et al. [45] | 2020 | Italy | To show the experience about the use of teledermatology for patients affected by acne disease. | Even if telemedicine is related to video or images quality, and to patients’ compliance, it could be an important supportive tool. |
| Lee, M. al. [46] | 2020 | To show the experience about the use of teledermatology for patients affected by acne disease | Even if teledermatology is a promising tool to extend dermatologic care with earlier access to follow-up., it could be useful in acne patients | |
| Khosravi et al. [47] | 2020 | USA | To compare the rate and duration of follow-up between acne patients initially evaluated by teledermatology to in-person outpatient consultation. | Even if teledermatology is a promising tool to extend dermatologic care with earlier access to follow-up., follow-up education needs to be improved to improve follow-up care. |
| Patel et al. [48] | 2021 | UK | To evaluate the effectiveness of teledermatology on the care of patients with HS during the pandemic. | Face-to-face consultations should be preferred, as HS patients should be handled sensitively, given the propensity of the disease to affect intimate body areas and the possibility of anxiety and depression in these patients. |
| Price et al. [49] | 2021 | USA | To evaluate the impact of COVID-19 on HS care. | Teledermatology is a useful tool for HS management. However, an improvement of this strategy is needed to optimize care for HS patients. |
| Kang et al. [50] | 2020 | Canada | To examine teledermatology management strategies and treatment outcomes. | Patients affected by HS need special strategies in telemedicine. Support group should be considered. More data is needed to improve HS management in telemedicine. |
| Foolad et al. [52] | 2017 | USA | To assess the difference in acne grading and treatment recommendations among an international group of dermatologists evaluating photographs. | The study suggests the effectiveness of the use of mobile phone-based photography and cloud-based image sharing for acne assessment. |
| Ariens et al. [56] | 2017 | Netherlands | To assess opinions of the most important stakeholders influencing the implementation and use of eHealth services in daily dermatology practice | Health care professionals and patients acknowledge the benefits arising from the implementation and use of eHealth services in daily dermatology practice. |
| Matricardi et al. [57] | 2019 | EAACI Task force | To evaluate the current and future potential of mHealth for specific areas of allergology, including allergic rhinitis, aerobiology, allergen immunotherapy, asthma, dermatological diseases, food allergies, anaphylaxis, insect venom, and drug allergy. | The perspectives of health care professionals and allergic patients are discussed, underlining the need for thorough investigation for an effective design of mHealth technologies as auxiliary tools to improve the quality of care. |
| Bergmo et al. [58] | 2009 | Norway | To analyze how web-based consultations for parents of children with atopic dermatitis affect self-management behaviour, health outcome, health resource use, and family costs. | No effect of supplementing traditional treatment for childhood dermatitis with web-based consultations was found, however, the intervention group tended to have fewer visits to practitioners. |
| Schopf et al. [59] | 2012 | Norway | To investigate whether an interactive Web-based course, including personal guidance via email or cellular phone texting, may be used to improve practice behavior of general practitioners in the management of atopic dermatitis. | A Web-based educational intervention aimed at general practitioners combined with personal support can reduce the number of atopic dermatitis patient referrals to specialists. |
| Giavina-Bianchi et al. [60] | 2020 | Brazil | To evaluate the proportion of atopic dermatitis patients who could be managed with the support of telemedicine and its accuracy. To assess the frequency of atopic dermatitis, demographics, clinical features, and therapies dispensed in relation to the disease. | Telemedicine was an accurate method and helped primary care physicians to treat 72% of the atopic dermatitis lesions, optimizing in-person appointments with dermatologists for more severe cases. |
| van Os-Medendorp et al. [61] | 2012 | Netherlands | To determine the cost-effectiveness of individualized e-health compared with usual face-to-face care for children and adults with AD. | E-health during follow-up of patients with AD is just as effective as usual face-to-face care with regard to the quality of life and severity of disease, with the advantage of cost-saving. |
| Kornmehl et al. [62] | 2017 | USA | To evaluate the quality of life in AD patients managed through a direct-access online model. | Adult and pediatric AD patients receiving direct-access online care had an equivalent quality of life outcomes as those seen in-person. The direct-access online model has the potential to increase access to care for patients with chronic skin diseases. |
| Santer et al. [63] | 2014 | United Kingdom | To develop and test a Web-based intervention to support families of children with eczema, and to explore whether support from a health care professional (HCP) is necessary to engage participants with the intervention | This trial demonstrates the potential for greater improvements in POEM scores in website intervention groups. Moreover, HCP support was not strongly valued by participants and did not lead to better outcomes. |
| Armstrong et al. [64] | 2015 | USA | To compare the effectiveness of a direct-access online model for follow-up dermatologic care in pediatric and adult patients with atopic dermatitis with that of in-person office visits. | The direct-access online model results in equivalent improvements in atopic dermatitis clinical outcomes as in-person care. |
| Schmid-Grendelmeier et al. [65] | 2019 | Africa | To identify research and intervention priorities in Africa and initiate African-led projects for AD. | AD is one of the most prevalent chronic inflammatory skin diseases in SSA. The potential applications of telemedicine could improve the diagnosis and therapeutic management of AD. |
| Davis et al. [66] | 2021 | USA | To describe current evidence regarding health disparities within allergy/immunology in racial and ethnic underserved populations. | Health disparities affect all aspects of health care, especially with regard to access, delivery, and outcomes. Telemedicine could improve access to health care in AD patients, |
| Shaker et al. [67] | 2020 | USA and Canada | To provide useful strategies for the correct diagnostic and therapeutic management of patients referring to allergy/immunological clinics during the COVID-19 pandemic. | Telehealth and virtual patient encounters can be central to delivering allergy services within a risk-stratified context of the SARS-CoV-2 pandemic, thanks to the ability to integrate telecommunications, information systems, and patient care. |
| Napolitano et al. [68] | 2020 | Italy | To provide monitoring strategies for patients with atopic dermatitis treated with dupilumab, during the COVID-19 pandemic. | Telephone consultations with adult AD patients treated with dupilumab prevent patients from leaving their homes and crowding the hospital and to continue monitoring their condition. |
| Malipiero et al. [69] | 2020 | To evaluate the reorganization of work in allergy clinics to fight the COVID-19 pandemic | Telemedicine and digital medicine services can be helpful to reduce the risk of viral spreading while delivering up-to-date personalized care |
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Armstrong, A.W.; Read, C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA 2020, 323, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Goldburg, S.R.; Strober, B.E.; Payette, M.J. Hidradenitis suppurativa: Epidemiology, clinical presentation, and pathogenesis. J. Am. Acad. Dermatol. 2020, 82, 1045–1058. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Bhate, K. A global perspective on the epidemiology of acne. Br. J. Dermatol. 2015, 172, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Nutten, S. Atopic dermatitis: Global epidemiology and risk factors. Ann. Nutr. Metab. 2015, 66 (Suppl. 1), 8–16. [Google Scholar] [CrossRef] [PubMed]
- Marasca, C.; Ruggiero, A.; Napolitano, M.; Fabbrocini, G.; Megna, M. May COVID-19 outbreaks lead to a worsening of skin chronic inflammatory conditions? Med. Hypotheses 2020, 143, 109853. [Google Scholar] [CrossRef]
- Dahy, A.; El-Qushayri, A.E.; Mahmoud, A.R.; Al-Kelany, T.A.; Salman, S. Telemedicine approach for psoriasis management, time for application? A systematic review of published studies. Dermatol. Ther. 2020, 33, e13908. [Google Scholar] [CrossRef] [PubMed]
- Muir, J. Telehealth: The specialist perspective. Aust. Fam. Physician 2014, 43, 828–830. [Google Scholar] [PubMed]
- Doraiswamy, S.; Abraham, A.; Mamtani, R.; Cheema, S. Use of Telehealth During the COVID-19 Pandemic: Scoping Review. J. Med. Internet Res. 2020, 22, e24087. [Google Scholar] [CrossRef] [PubMed]
- Byrom, L.; Lucas, L.; Sheedy, V.; Madison, K.; McIver, L.; Castrisos, G.; Alfonzo, C.; Chiu, F.P.-C.; Muir, J. Tele-Derm National: A decade of teledermatology in rural and remote Australia. Aust. J. Rural Health 2016, 24, 193–199. [Google Scholar] [CrossRef]
- Jemec, G.B.E.; Heidenheim, M.; Dam, T.N.; Vang, E. Teledermatology on the Faroe Islands. Int. J. Dermatol. 2008, 47, 891–893. [Google Scholar] [CrossRef]
- Tsang, M.W.; Kovarik, C.L. The role of dermatopathology in conjunction with teledermatology in resource-limited settings: Lessons from the African Teledermatology Project. Int. J. Dermatol. 2011, 50, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, R.K.; Jemec, G.B.E. Teledermatology management of difficult-to-treat dermatoses in the Faroe Islands. Acta Dermatovenerol. Alp. Pannonica Adriat. 2019, 28, 103–105. [Google Scholar]
- Villani, A.; Megna, M.; Scalvenzi, M.; Fabbrocini, G.; Ruggiero, A. Teledermatology and chronic skin diseases: Real life experience in a Southern Italian Dermatologic Centre. Dermatol. Ther. 2020, 33, e13839. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Bellinato, F.; Piaserico, S.; Di Leo, S.; Cazzaniga, S.; Naldi, L. Preference for Telemedicine Versus In-Person Visit Among Patients with Psoriasis Receiving Biological Drugs. Dermatol. Ther. 2021, 11, 1333–1343. [Google Scholar] [CrossRef] [PubMed]
- Brunasso, A.M.G.; Massone, C. Teledermatologic monitoring for chronic cutaneous autoimmune diseases with smartworking during COVID-19 emergency in a tertiary center in Italy. Dermatol. Ther. 2020, 33, e13495. [Google Scholar] [CrossRef]
- Beer, J.; Hadeler, E.; Calume, A.; Gitlow, H.; Nouri, K. Teledermatology: Current indications and considerations for future use. Arch. Dermatol. Res. 2021, 313, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Chambers, C.J.; Parsi, K.K.; Schupp, C.; Armstrong, A.W. Patient-centered online management of psoriasis: A randomized controlled equivalency trial. J. Am. Acad. Dermatol. 2012, 66, 948–953. [Google Scholar] [CrossRef] [Green Version]
- Pearlman, R.L.; Le, P.B.; Brodell, R.T.; Nahar, V.K. Evaluation of patient attitudes towards the technical experience of synchronous teledermatology in the era of COVID-19. Arch. Dermatol. Res. 2021, 313, 769–772. [Google Scholar] [CrossRef]
- Frühauf, J.; Schwantzer, G.; Ambros-Rudolph, C.M.; Weger, W.; Ahlgrimm-Siess, V.; Salmhofer, W.; Hofmann-Wellenhof, R. Pilot study on the acceptance of mobile teledermatology for the home monitoring of high-need patients with psoriasis. Australas. J. Dermatol. 2012, 53, 41–46. [Google Scholar] [CrossRef]
- Julie, Z.Y.; Reynolds, R.V.; Olbricht, S.M.; McGee, J.S. Moving forward with teledermatology: Operational challenges of a hybrid in-person and virtual practice. Clin. Dermatol. 2021, 39, 707–709. [Google Scholar]
- Ferwerda, M.; Van Beugen, S.; Van Burik, A.; Van Middendorp, H.; De Jong, E.M.G.J.; Van De Kerkhof, P.C.M.; Van Riel, P.L.C.M.; Evers, A.W.M. What patients think about E-health: Patients’ perspective on internet-based cognitive behavioral treatment for patients with rheumatoid arthritis and psoriasis. Clin. Rheumatol. 2013, 32, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.R.; Gibbons, C.M.; Torres, J.; Kornmehl, H.A.; Singh, S.; Young, P.M.; Chambers, C.J.; Maverakis, E.; Dunnick, C.A.; Armstrong, A.W. Access to Dermatological Care with an Innovative Online Model for Psoriasis Management:Results from a Randomized Controlled Trial. Telemed. e-Health 2019, 25, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Chambers, C.J.; Maverakis, E.; Cheng, M.Y.; Dunnick, C.A.; Chren, M.M.; Gelfand, J.M.; Wong, D.J.; Gibbons, B.M.; Gibbons, C.M.; et al. Effectiveness of Online vs In-Person Care for Adults with Psoriasis: A Randomized Clinical Trial. JAMA Netw. Open 2018, 1, e183062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frühauf, J.; Schwantzer, G.; Ambros-Rudolph, C.M.; Weger, W.; Ahlgrimm-Siess, V.; Salmhofer, W.; Hofmann-Wellenhof, R. Pilot Study Using Teledermatology to Manage High-Need Patients with Psoriasis. Arch. Dermatol. 2015, 146, 200–201. [Google Scholar] [CrossRef] [PubMed]
- Balato, N.; Megna, M.; Di Costanzo, L.; Balato, A.; Ayala, F. Educational and motivational support service: A pilot study for mobile-phone-based interventions in patients with psoriasis. Br. J. Dermatol. 2013, 168, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Soyer, H.P.; Wu, J.; Salmhofer, W.; Gilmore, S. Tele-assessment of Psoriasis Area and Severity Index: A study of the accuracy of digital image capture. Australas. J. Dermatol. 2011, 52, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Petto, H.; Dutronc, Y.; Burkhardt, N.; Gebauer, K.; Gooderham, M. Development and validation of a new method for potential use of Psoriasis Area and Severity Index in teledermatology. Australas. J. Dermatol. 2021, 62, e114–e117. [Google Scholar] [CrossRef] [PubMed]
- Koller, S.; Hofmann-Wellenhof, R.; Hayn, D.; Weger, W.; Kastner, P.; Schreier, G.; Salmhofer, W. Teledermatological monitoring of psoriasis patients on biologic therapy. Acta Derm. Venereol. 2011, 91, 680–685. [Google Scholar] [CrossRef] [Green Version]
- Klotz, J.; Muir, L.; Cameron, C.; Delaney, L. Monitoring a remote phototherapy unit via telemedicine. J. Cutan. Med. Surg. 2005, 9, 47–53. [Google Scholar] [CrossRef]
- Svendsen, M.T.; Andersen, F.; Andersen, K.E. eHealth Technologies as an intervention to improve adherence to topical antipsoriatics: A systematic review. J. Dermatol. Treat. 2018, 29, 123–128. [Google Scholar] [CrossRef]
- Rompoti, N.; Katsimbri, P.; Kokkalis, G.; Boumpas, D.; Ikonomidis, I.; Theodoropoulos, K.; Rigopoulos, D.; Papadavid, E. Real world data from the use of secukinumab in the treatment of moderate-to-severe psoriasis, including scalp and palmoplantar psoriasis: A 104-week clinical study. Dermatol. Ther. 2019, 32, e13006. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhang, S.; Wu, R.; Su, Y. COVID-19 and psoriasis: Recommendation for patients on regular infliximab therapy. Dermatol. Ther. 2020, 33, e14472. [Google Scholar] [CrossRef] [PubMed]
- Young, P.M.; Chen, A.Y.; Ford, A.; Cheng, M.Y.; Lane, C.J.; Armstrong, A.W. Effects of Online Care on Functional and Psychological Outcomes in Patients with Psoriasis: A Randomized Controlled Trial. J. Am. Acad. Dermatol. 2019; in press. [Google Scholar]
- Beytout, Q.; Pepiot, J.; Maruani, A.; Devulder, D.; Aubert, R.; Beylot-Barry, M.; Amici, J.-M.; Jullien, D.; Mahé, E. Impact of the COVID-19 pandemic on children with psoriasis. Ann. Dermatol. Vénéréologie 2020, 148, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Mazzuoccolo, L.D.; Esposito, M.N.; Luna, P.C.; Seiref, S.; Dominguez, M.; Echeverría, C.M. WhatsApp: A Real-Time Tool to Reduce the Knowledge Gap and Share the Best Clinical Practices in Psoriasis. Telemed. e-Health 2019, 25, 294–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knutsen-Larson, S.; Dawson, A.L.; Dunnick, C.A.; Dellavalle, R.P. Acne vulgaris: Pathogenesis, treatment, and needs assessment. Dermatol. Clin. 2012, 30, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Saunte, D.M.L.; Jemec, G.B.E. Hidradenitis Suppurativa: Advances in Diagnosis and Treatment. JAMA 2017, 318, 2019–2032. [Google Scholar] [CrossRef] [PubMed]
- Marasca, C.; De Rosa, A.; Fabbrocini, G.; Cantelli, M.; Patrì, A.; Vastarella, M.; Gallo, L.; Di Vico, F.; Poggi, S.; Ruggiero, A. Psychological teleconsultations in patients suffering from chronic skin diseases during the COVID-19 era: A service to improve patients’ quality of life. J. Dermatol. Treat. 2020, 12, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Frühauf, J.; Kröck, S.; Quehenberger, F.; Kopera, D.; Fink-Puches, R.; Komericki, P.; Pucher, S.; Arzberger, E.; Hofmann-Wellenhof, R. Mobile teledermatology helping patients control high-need acne: A randomized controlled trial. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Loh, C.H.; Tam, S.Y.C.; Oh, C.C. Teledermatology in the COVID-19 pandemic: A systematic review. JAAD Int. 2021, 5, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Kazi, R.; Evankovich, M.R.; Liu, R.; Liu, A.; Moorhead, A.; Ferris, L.K.; Falo, L.D.; English, J.C. Utilization of asynchronous and synchronous teledermatology in a large health care system during the COVID-19 pandemic. Telemed. e-Health 2021, 27, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Gu, L.; Diaz, S.M.; Lipner, S.R. Retrospective study of acne telemedicine and in-person visits at an academic center during the COVID-19. Cosmet. Dermatol. 2021, 21, 36–38. [Google Scholar] [CrossRef] [PubMed]
- Marasca, C.; Ruggiero, A.; Fontanella, G.; Ferrillo, M.; Fabbrocini, G.; Villani, A. Telemedicine and support groups could be used to improve adherence to treatment and health-related quality of life in patients affected by inflammatory skin conditions during the COVID-19 pandemic. Clin. Exp. Dermatol. 2020, 45, 749. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Megna, M.; Annunziata, M.C.; Abategiovanni, L.; Scalvenzi, M.; Tajani, A.; Fabbrocini, G.; Villani, A. Teledermatology for acne during COVID-19: High patients’ satisfaction in spite of the emergency. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e662–e663. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.; Annunziata, M.C.; Abategiovanni, L.; Fabbrocini, G. Teledermatology for acne patients: How to reduce face-to-face visits during COVID-19 pandemic. J. Cosmet. Dermatol. 2020, 19, 1828. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Kassamali, B.; Shah, N.; LaChance, A.; Nambudiri, V.E. Differences in virtual care utilization for acne by vulnerable populations during the COVID-19 pandemic: A retrospective review. J. Am. Acad. Dermatol. 2021, 85, 718–719. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, H.; Zhang, S.; Siripong, N.; Moorhead, A.; Iii, J.C.E. Comparing acne follow-up: Teledermatology versus outpatient dermatology visits. Dermatol. Online J. 2020, 26, 13030/qt1424r02m. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.P. Remote consultations for patients with hidradenitis suppurativa during the COVID-19 pandemic: A single-centre experience. Clin. Exp. Dermatol. 2021, 46, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Price, K.N.; Collier, E.K.; Grogan, T.R.; Hsiao, J.L.; Shi, V.Y. Hidradenitis suppurativa patient perspectives during the COVID-19 pandemic. Dermatol. Online J. 2021, 27, 13030/qt42g0634s. [Google Scholar] [CrossRef] [PubMed]
- Kang, N.C.; Hsiao, J.; Shi, V.; Naik, H.B.; Lowes, M.A.; Alavi, A. Remote management of hidradenitis suppurativa in a pandemic era of COVID-19. Int. J. Dermatol. 2020, 59, e318–e320. [Google Scholar] [CrossRef] [PubMed]
- Okeke, C.A.V.; Shipman, W.D.; Perry, J.D.; Kerns, M.L.; Okoye, G.A.; Byrd, A.S. Treating hidradenitis suppurativa during the COVID-19 pandemic: Teledermatology exams of sensitive body areas. J Dermatol. Treat. 2020. [Google Scholar] [CrossRef] [PubMed]
- Foolad, N.; Ornelas, J.N.; Bs, A.K.C.; Ali, I.; Sharon, V.R.; Al Mubarak, L.; Lopez, A.; Alikhan, A.; Al Dabagh, B.; Firooz, A.; et al. International inter-rater agreement in scoring acne severity utilizing cloud-based image sharing of mobile phone photographs. Int. J. Dermatol. 2017, 56, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Weidinger, S.; Novak, N. Atopic dermatitis. Lancet 2016, 12, 1109–1122. [Google Scholar] [CrossRef]
- Tsai, T.; Rajagopalan, M.; Chu, C.-Y.; Encarnacion, L.; Gerber, R.A.; Santos-Estrella, P.; Llamado, L.J.Q.; Tallman, A.M. Burden of atopic dermatitis in Asia. J. Dermatol. 2019, 46, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Deckers, I.A.G.; Mclean, S.; Linssen, S.; Mommers, M.; Van Schayck, C.P.; Sheikh, A. Investigating international time trends in the incidence and prevalence of atopic eczema 1990–2010: A systematic review of epidemiological studies. PLoS ONE 2012, 7, e39803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ariens, L.F.; Schussler-Raymakers, F.M.; Frima, C.; Flinterman, A.; Hamminga, E.; Arents, B.W.; Bruijnzeel-Koomen, C.A.; De Bruin-Weller, M.S.; Van Os-Medendorp, H. Barriers and Facilitators to eHealth Use in Daily Practice: Perspectives of Patients and Professionals in Dermatology. J. Med. Internet Res. 2017, 19, e300. [Google Scholar] [CrossRef] [PubMed]
- Matricardi, P.M.; Dramburg, S.; Alvarez-Perea, A.; Antolín-Amérigo, D.; Apfelbacher, C.; Atanaskovic-Markovic, M.; Berger, U.; Blaiss, M.S.; Blank, S.; Boni, E.; et al. The role of mobile health technologies in allergy care: An EAACI position paper. Allergy 2020, 75, 259–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergmo, T.S.; Wangberg, S.; Schopf, T.R.G.; Solvoll, T. Web-based consultations for parents of children with atopic dermatitis: Results of a randomized controlled trial. Acta Paediatr. 2009, 98, 316–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schopf, T.; Flytkjaer, V. Impact of interactive web-based education with mobile and email-based support of general practitioners on treatment and referral patterns of patients with atopic dermatitis: Randomized controlled trial. J. Med. Internet Res. 2012, 14, e2359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giavina-Bianchi, M.; Giavina-Bianchi, P.; Santos, A.P.; Rizzo, L.V.; Cordioli, E. Accuracy and efficiency of telemedicine in atopic dermatitis. JAAD Int. 2020, 1, 175–181. [Google Scholar] [CrossRef] [PubMed]
- van Os-Medendorp, H.; Koffijberg, H.; Eland-de Kok, P.C.M.; Van der Zalm, A.; de Bruin-Weller, M.S.; Pasmans, S.G.M.A.; Ros, W.J.G.; Thio, H.B.; Knol, M.J.; Bruijnzeel-Koomen, C.A.F.M. E-health in caring for patients with atopic dermatitis: A randomized controlled cost-effectiveness study of internet-guided monitoring and online self-management training. Br. J. Dermatol. 2012, 166, 1060–1068. [Google Scholar] [CrossRef]
- Kornmehl, H.; Singh, S.; Johnson, M.A.; Armstrong, A.W. Direct-Access Online Care for the Management of Atopic Dermatitis: A Randomized Clinical Trial Examining Patient Quality of Life. Telemed. e-Health 2017, 23, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Santer, M.; Müller, I.; Yardley, L.; Burgess, H.; Selinger, H.; Stuart, B.L.; Little, P.; Van Os-Medendorp, H.; Schopf, T. Supporting self-care for families of children with eczema with a Web-based intervention plus health care professional support: Pilot randomized controlled trial. J. Med. Internet Res. 2014, 16, e70. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Johnson, M.A.; Lin, S.; Maverakis, E.; Fazel, N.; Liu, F.T. Patient-centered, direct-access online care for management of atopic dermatitis: A randomized clinical trial. JAMA Dermatol. 2015, 151, 154–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid-Grendelmeier, P.; Takaoka, R.; Ahogo, K.; Belachew, W.; Brown, S.; Correia, J.C.; Correia, M.; Degboe, B.; Dorizy-Vuong, V.; Faye, O.; et al. Position Statement on Atopic Dermatitis in Sub-Saharan Africa: Current status and roadmap. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2019–2028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, C.M.; Apter, A.J.; Casillas, A.; Foggs, M.B.; Louisias, M.; Morris, E.C.; Nanda, A.; Nelson, M.R.; Ogbogu, P.U.; Walker-McGill, C.L.; et al. Health disparities in allergic and immunologic conditions in racial and ethnic underserved populations: A Work Group Report of the AAAAI Committee on the Underserved. J. Allergy Clin. Immunol. 2021, 147, 1579–1593. [Google Scholar] [CrossRef] [PubMed]
- Shaker, M.S.; Oppenheimer, J.; Grayson, M.; Stukus, D.; Hartog, N.; Hsieh, E.W.; Rider, N.; Dutmer, C.M.; Vander Leek, T.K.; Kim, H.; et al. COVID-19: Pandemic Contingency Planning for the Allergy and Immunology Clinic. J. Allergy Clin. Immunol. Pract. 2020, 8, 1477–1488.e5. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Patruno, C.; Ruggiero, A.; Nocerino, M.; Fabbrocini, G. Safety of dupilumab in atopic patients during COVID-19 outbreak. J. Dermatol. Treat. 2020, 33, 600–601. [Google Scholar] [CrossRef] [PubMed]
- Malipiero, G.; Heffler, E.; Pelaia, C.; Puggioni, F.; Racca, F.; Ferri, S.; Spinello, L.; Merigo, M.; Lamacchia, D.; Cataldo, G.; et al. Allergy clinics in times of the SARS-CoV-2 pandemic: An integrated model. Clin. Transl. Allergy. 2020, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Scalvini, S.; Vitacca, M.; Paletta, L.; Giordano, A.; Balbi, B. Telemedicine: A new frontier for effective healthcare services. Monaldi Arch. Chest Dis. 2004, 61, 226–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marasca, C.; Annunziata, M.C.; Camela, E.; Di Guida, A.; Fornaro, L.; Megna, M.; Napolitano, M.; Patruno, C.; Potestio, L.; Fabbrocini, G. Teledermatology and Inflammatory Skin Conditions during COVID-19 Era: New Perspectives and Applications. J. Clin. Med. 2022, 11, 1511. https://doi.org/10.3390/jcm11061511
Marasca C, Annunziata MC, Camela E, Di Guida A, Fornaro L, Megna M, Napolitano M, Patruno C, Potestio L, Fabbrocini G. Teledermatology and Inflammatory Skin Conditions during COVID-19 Era: New Perspectives and Applications. Journal of Clinical Medicine. 2022; 11(6):1511. https://doi.org/10.3390/jcm11061511
Chicago/Turabian StyleMarasca, Claudio, Maria Carmela Annunziata, Elisa Camela, Adriana Di Guida, Luigi Fornaro, Matteo Megna, Maddalena Napolitano, Cataldo Patruno, Luca Potestio, and Gabriella Fabbrocini. 2022. "Teledermatology and Inflammatory Skin Conditions during COVID-19 Era: New Perspectives and Applications" Journal of Clinical Medicine 11, no. 6: 1511. https://doi.org/10.3390/jcm11061511