
Treatment of Moderate to Severe Psoriasis during the COVID-19 Pandemic: Lessons Learned and Opportunities

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification of the Research Question
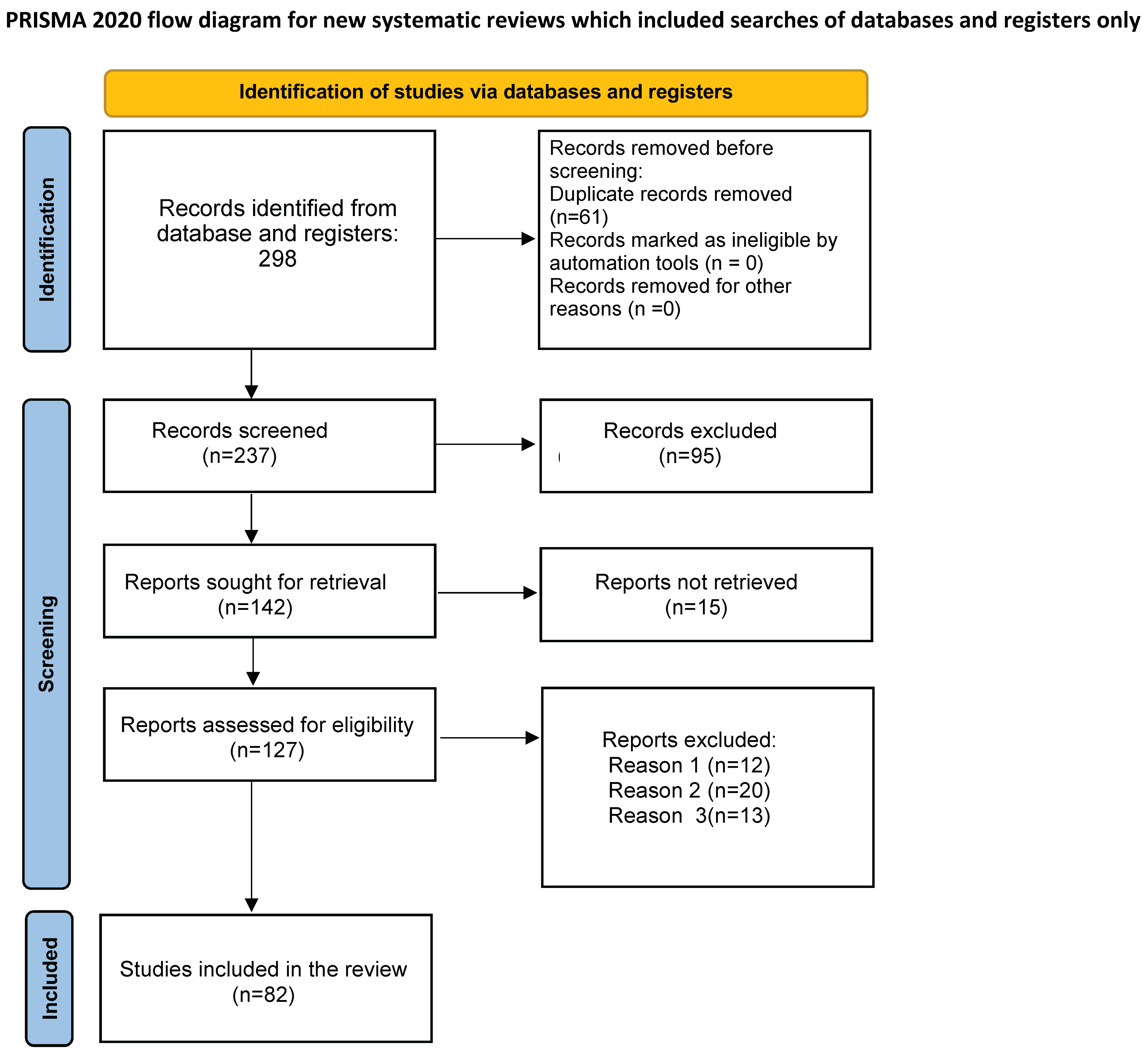
2.2. Study Selection Process
2.3. Data Extraction
3. Results
3.1. Impact of SARS-CoV-2 Infection on Psoriasis Clinical Course
3.2. Impact of Psoriasis on SARS-CoV-2 Infection
3.3. Impact of SARS-CoV-2 Infection on Systemic Treatments in Psoriatic Patients
3.3.1. TNF Alpha Inhibitors
3.3.2. IL17A/IL17R Inhibitors
3.3.3. IL-23 Inhibitors
3.3.4. Cyclosporine
3.3.5. Methotrexate
3.3.6. Apremilast
3.4. Impact of SARS-CoV-2 Vaccines on Patients with Psoriasis
3.5. Vaccinal Hesitation and Strategies to Fight It in Psoriatic Patients
3.6. Teledermatology as Emerging Assistence Paradigm in Moderate to Severe Patients
4. Discussion
- -
- Most of the existing evidence is based on spontaneous case series, and although data from literature globally indicate no significant increase of the risk for severe COVID-19 evolution in psoriasis patients, it is hard to evaluate which biological agent is safer for COVID-19. However, from the current unclassified research, biologics do not seem to have a significant impact on the COVID-19 course. Regardless of which biological agents have been used, patients in biologics treatment seem to be not at higher risk for severe COVID complications.
- -
- According to the recommendations of the major global dermatological associations [108,109,110], asymptomatic patients in close contact with a confirmed or probable COVID-19 case in the last 14 days can continue biologic therapy. It is advisable to discontinue or postpone biological treatment in symptomatic patients with confirmed SARS-CoV-2 infections until COVID-19 is completely resolved.
- -
- For all candidates undergoing biological treatment, it is advisable to carefully assess the balance between benefits and risks of treatment for each patient.
- -
- The National Psoriasis Foundation COVID-19 Task Force, in the last version of guidance for the management of psoriatic disease during the pandemic has reported that patients not infected with SARS-CoV-2 should continue biologics for psoriasis in most cases. Shared decision-making process between clinician and patient is recommended to guide discussions about the use of systemic therapies during the pandemic [58].
- -
- Conversely, as the impact of MTX or CsA on COVID-19 infection is still to be cleared, despite they are commonly used immunosuppressive agent for psoriasis, studies focusing on these drugs on SARS-CoV-2 infection or COVID-19 evolution in psoriasis patients under treatment are few and inconclusive. Further research in this field is warranted and needed, before giving specific recommendation on continuation of their use in psoriatic patients affected by COVID-19.
- -
- Although psoriatic patients have no increased risk of evolving toward severe forms of COVID-19 compared to the general population, they are frail subjects with respect to SARS-COV-2 infection which can favor the release of psoriasis clinically in remission, or favor its onset in predisposed patients or condition the appearance of different psoriasis phenotypes (e.g., pustular forms).
- -
- Vaccination still represents the most effective measure to prevent the development of serious form of COVID-19 in psoriasis patients who should be advised to be vaccinated without discontinuing their biological treatment. In case the patient is starting a biological treatment, he should be vaccinated in advance, as current evidence suggests that the use of immunosuppressive agents may reduce the vaccine immune response to a certain extent [41].
- -
- Dermatologists should be aware that vaccination of psoriasis patients is mandatory. They should consider the opportunity to be prompted to manage vaccination hesitancy in all patients, reassuring patients, with a clear and communicative language and informing them about the risks associated with vaccination, which are low in terms of the risk-benefit ratio [111].
- -
- Although from the beginning of the pandemic, more and more information has been collected, and dermatologists globally improved their knowledge on managing psoriasis patients, the current evidence has still certain limitations. Therefore, it is necessary to be cautious when making clinical decisions. More prospective studies with higher levels of evidence are needed to support clinical decision-making.
Author Contributions
Funding
Conflicts of Interest
References
- Diotallevi, F.; Campanati, A.; Radi, G.; Martina, E.; Rizzetto, G.; Barbadoro, P.; D’Errico, M.M.; Offidani, A. Vaccines Against SARS-CoV-2 in Psoriasis Patients on Immunosuppressive Therapy: Implications of Vaccination Nationwide Campaign on Clinical Practice in Italy. Dermatol. Ther. (Heidelb.) 2021, 11, 1889–1903. [Google Scholar] [CrossRef]
- Hilary Arksey, Lisa O’Malley Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Aram, K.; Patil, A.; Goldust, M.; Rajabi, F. COVID-19 and exacerbation of dermatological diseases: A review of the available literature. Dermatol. Ther. 2021, 34, e15113. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, R.J.; Cobb, C.B.C.; Telang, G.H.; Firoz, E.F. New-onset pustular psoriasis in the setting of severe acute respiratory syndrome coronavirus 2 infection causing coronavirus disease 2019. JAAD Case Rep. 2020, 6, 1360–1362. [Google Scholar] [CrossRef]
- Shakoei, S.; Ghanadan, A.; Hamzelou, S. Pustular psoriasis exacerbated by COVID-19 in a patient with the history of psoriasis. Dermatol. Ther. 2020, 33, e14462. [Google Scholar] [CrossRef]
- Shahidi Dadras, M.; Diab, R.; Ahadi, M.; Abdollahimajd, F. Generalized pustular psoriasis following COVID-19. Dermatol. Ther. 2021, 34, e14595. [Google Scholar] [CrossRef] [PubMed]
- Gananandan, K.; Sacks, B.; Ewing, I. Guttate psoriasis secondary to COVID-19. BMJ Case Rep. 2020, 13, e237367. [Google Scholar] [CrossRef]
- Samotij, D.; Gawron, E.; Szczęch, J.; Ostańska, E.; Reich, A. Acrodermatitis Continua of Hallopeau Evolving into Generalized Pustular Psoriasis Following COVID-19: A Case Report of a Successful Treatment with Infliximab in Combination with Acitretin. Biologics 2021, 15, 107–113. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506, Erratum in Lancet 2020, 395, 496. [Google Scholar] [CrossRef] [Green Version]
- Diotallevi, F.; Campanati, A.; Bianchelli, T.; Bobyr, I.; Luchetti, M.M.; Marconi, B.; Martina, E.; Radi, G.; Offidani, A. Skin involvement in SARS-CoV-2 infection: Case series. J. Med. Virol. 2020, 92, 2332–2334. [Google Scholar] [CrossRef] [PubMed]
- Imai, Y.; Kuba, K.; Rao, S.; Huan, Y.; Guo, F.; Guan, B.; Yang, P.; Sarao, R.; Wada, T.; Leong-Poi, H.; et al. Angiotensin-converting enzyme 2 protects from severe acute lung failure. Nature 2005, 436, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Giannoni, M.; Consales, V.; Campanati, A.; Ganzetti, G.; Giuliodori, K.; Postacchini, V.; Liberati, G.; Azzaretto, L.; Vichi, S.; Guanciarossa, F.; et al. Homocysteine plasma levels in psoriasis patients: Our experience and review of the literature. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1781–1785. [Google Scholar] [CrossRef]
- Talamonti, M.; Galluzzo, M.; Chiricozzi, A.; Quaglino, P.; Fabbrocini, G.; Gisondi, P.; Marzano, A.V.; Potenza, C.; Conti, A.; Parodi, A.; et al. Characteristic of chronic plaque psoriasis patients treated with biologics in Italy during the COVID-19 Pandemic: Risk analysis from the PSO-BIO-COVID observational study. Expert Opin. Biol. Ther. 2021, 21, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Piaserico, S.; Naldi, L.; Dapavo, P.; Conti, A.; Malagoli, P.; Marzano, A.V.; Bardazzi, F.; Gasperini, M.; Cazzaniga, S.; et al. Incidence rates of hospitalization and death from COVID-19 in patients with psoriasis receiving biological treatment: A Northern Italy experience. J. Allergy Clin. Immunol. 2021, 147, 558–560.e1. [Google Scholar] [CrossRef] [PubMed]
- Costantino, F.; Bahier, L.; Tarancón, L.C.; Leboime, A.; Vidal, F.; Bessalah, L.; Breban, M.; D’Agostino, M.A. COVID-19 in French patients with chronic inflammatory rheumatic diseases: Clinical features, risk factors and treatment adherence. Jt. Bone Spine 2021, 88, 105095. [Google Scholar] [CrossRef] [PubMed]
- Montero, F.; Martínez-Barrio, J.; Serrano-Benavente, B.; González, T.; Rivera, J.; Molina Collada, J.; Castrejón, I.; Álvaro-Gracia, J. Coronavirus disease 2019 (COVID-19) in autoimmune and inflammatory conditions: Clinical characteristics of poor outcomes. Rheumatol. Int. 2020, 40, 1593–1598. [Google Scholar] [CrossRef]
- Nuño, L.; Novella Navarro, M.; Bonilla, G.; Franco-Gómez, K.; Aguado, P.; Peiteado, D.; Monjo, I.; Tornero, C.; Villalba, A.; Miranda-Carus, M.E.; et al. Clinical course, severity and mortality in a cohort of patients with COVID-19 with rheumatic diseases. Ann. Rheum. Dis. 2020, 79, 1659–1661. [Google Scholar] [CrossRef]
- Akiyama, S.; Hamdeh, S.; Micic, D.; Sakuraba, A. Prevalence and clinical outcomes of COVID-19 in patients with autoimmune diseases: A systematic review and meta-analysis. Ann. Rheum. Dis. 2020, 80, 384–391. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef]
- Zhou, Y.; Yang, Q.; Chi, J.; Dong, B.; Lv, W.; Shen, L.; Wang, Y. Comorbidities and the risk of severe or fatal outcomes associated with coronavirus disease 2019: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 99, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Shahidi-Dadras, M.; Tabary, M.; Robati, R.M.; Araghi, F.; Dadkhahfar, S. Psoriasis and risk of the COVID-19: Is there a role for angiotensin converting enzyme (ACE)? J. Dermatol. Treat. 2020, 30, 1175–1176. [Google Scholar] [CrossRef] [PubMed]
- Campanati, A.; Brisigotti, V.; Diotallevi, F.; D’Agostino, G.M.; Paolinelli, M.; Radi, G.; Rizzetto, G.; Sapigni, C.; Tagliati, C.; Offidani, A. Active implications for dermatologists in ‘SARS-CoV-2 ERA’: Personal experience and review of literature. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1626–1632. [Google Scholar] [CrossRef]
- Diotallevi, F.; Mazzanti, S.; Properzi, P.; Olivieri, S.; Giacometti, A.; Offidani, A. Is there a POST-COVID dermatological syndrome? The integrated dermato-infectious disease experience of a single centre. J. Eur. Acad. Dermatol. Venereol. 2021, 36, e166–e169. [Google Scholar] [CrossRef]
- Jamiolkowski, D.; Mühleisen, B.; Müller, S.; Navarini, A.A.; Tzankov, A.; Roider, E. SARS-CoV-2 PCR testing of skin for COVID-19 diagnostics: A case report. Lancet 2020, 396, 598–599. [Google Scholar] [CrossRef]
- Kolivras, A.; Dehavay, F.; Delplace, D.; Feoli, F.; Meiers, I.; Milone, L.; Olemans, C.; Sass, U.; Theunis, A.; Thompson, C.T.; et al. Coronavirus (COVID-19) infection-induced chilblains: A case report with histopathologic findings. JAAD Case Rep. 2020, 6, 489–492. [Google Scholar] [CrossRef] [PubMed]
- Abdollahimajd, F.; Niknezhad, N.; Haghighatkhah, H.R.; Namazi, N.; Niknejad, N.; Talebi, A. Angiotensin-converting enzyme and subclinical atherosclerosis in psoriasis: Is there any association? A case-control study. J. Am. Acad. Dermatol. 2020, 82, 980–981.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huskić, J.; Mulabegović, N.; Alendar, F.; Ostojić, L.; Ostojić, Z.; Simić, D.; Milicević, R.; Naletilić, M. Serum and tissue angiotensin converting enzyme in patients with psoriasis. Coll. Antropol. 2008, 32, 1215–1219. [Google Scholar]
- Lo, Y.; Tsai, T.F. Angiotensin converting enzyme and angiotensin converting enzyme inhibitors in dermatology: A narrative review. Expert Rev. Clin. Pharmacol. 2022, 15, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Patrick, M.T.; Zhang, H.; Wasikowski, R.; Prens, E.P.; Weidinger, S.; Gudjonsson, J.E.; Elder, J.T.; He, K.; Tsoi, L.C. Associations between COVID-19 and skin conditions identified through epidemiology and genomic studies. J. Allergy Clin. Immunol. 2021, 147, 857–869.e7. [Google Scholar] [CrossRef]
- Ye, L.; Lv, C.; Man, G.; Song, S.; Elias, P.M.; Man, M.Q. Abnormal epidermal barrier recovery in uninvolved skin supports the notion of an epidermal pathogenesis of psoriasis. J. Investig. Dermatol. 2014, 134, 2843–2846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehbinder, E.M.; Advocaat Endre, K.M.; Lødrup Carlsen, K.C.; Asarnoj, A.; Stensby Bains, K.E.; Berents, T.L.; Carlsen, K.H.; Gudmundsdóttir, H.K.; Haugen, G.; Hedlin, G.; et al. Predicting Skin Barrier Dysfunction and Atopic Dermatitis in Early Infancy. J. Allergy Clin. Immunol. Pract. 2020, 8, 664–673.e5. [Google Scholar] [CrossRef] [PubMed]
- Gardien, K.L.; Baas, D.C.; de Vet, H.C.; Middelkoop, E. Transepidermal water loss measured with the Tewameter TM300 in burn scars. Burns 2016, 42, 1455–1462. [Google Scholar] [CrossRef] [PubMed]
- Plichta, J.K.; Droho, S.; Curtis, B.J.; Patel, P.; Gamelli, R.L.; Radek, K.A. Local burn injury impairs epithelial permeability and antimicrobial peptide barrier function in distal unburned skin. Crit. Care Med. 2014, 42, e420–e431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, A.; Iwasaki, A. Type I and Type III Interferons—Induction, Signaling, Evasion, and Application to Combat COVID-19. Cell Host Microbe 2020, 27, 870–878. [Google Scholar] [CrossRef]
- Gisondi, P.; Bellinato, F.; Chiricozzi, A.; Girolomoni, G. The Risk of COVID-19 Pandemic in Patients with Moderate to Severe Plaque Psoriasis Receiving Systemic Treatments. Vaccines 2020, 8, 728. [Google Scholar] [CrossRef]
- McKeigue, P.M.; Weir, A.; Bishop, J.; McGurnaghan, S.J.; Kennedy, S.; McAllister, D.; Robertson, C.; Wood, R.; Lone, N.; Murray, J.; et al. Rapid Epidemiological Analysis of Comorbidities and Treatments as risk factors for COVID-19 in Scotland (REACT-SCOT): A population-based case-control study. PLoS Med. 2020, 17, e1003374. [Google Scholar] [CrossRef]
- Alqahtani, J.S.; Oyelade, T.; Aldhahir, A.M.; Alghamdi, S.M.; Almehmadi, M.; Alqahtani, A.S.; Quaderi, S.; Mandal, S.; Hurst, J.R. Prevalence, Severity and Mortality associated with COPD and Smoking in patients with COVID-19: A Rapid Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0233147. [Google Scholar] [CrossRef]
- Mahil, S.K.; Dand, N.; Mason, K.J.; Yiu, Z.Z.N.; Tsakok, T.; Meynell, F.; Coker, B.; McAteer, H.; Moorhead, L.; Mackenzie, T.; et al. Factors associated with adverse COVID-19 outcomes in patients with psoriasis-insights from a global registry-based study. J. Allergy Clin. Immunol. 2021, 147, 60–71. [Google Scholar] [CrossRef]
- Gisondi, P.; Cazzaniga, S.; Chimenti, S.; Maccarone, M.; Picardo, M.; Girolomoni, G.; Naldi, L.; Psocare Study Group. Latent tuberculosis infection in patients with chronic plaque psoriasis: Evidence from the Italian Psocare Registry. Br. J. Dermatol. 2015, 172, 1613–1620. [Google Scholar] [CrossRef]
- Zeng, H.; Wang, S.; Chen, L.; Shen, Z. Biologics for Psoriasis During the COVID-19 Pandemic. Front. Med. (Lausanne) 2021, 8, 759568. [Google Scholar] [CrossRef] [PubMed]
- Kartal, S.P.; Çelik, G.; Yılmaz, O.; Öksüm Solak, E.; Demirbağ Gül, B.; Üstünbaş, T.K.; Gönülal, M.; Baysak, S.; Yüksel, E.İ.; Ünlü, B.; et al. The impact of COVID-19 pandemic on psoriasis patients, and their immunosuppressive treatment: A cross-sectional multicenter study from Turkey. J. Dermatol. Treat. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, P.; Panda, P.; Ostwal, V.; Ramaswamy, A. Repurposing valproate to prevent acute respiratory distress syndrome/acute lung injury in COVID-19: A review of immunomodulatory action. Cancer Res. Stat. Treat. 2020, 3, 65–70. [Google Scholar] [CrossRef]
- Ghazavi, A.; Ganji, A.; Keshavarzian, N.; Rabiemajd, S.; Mosayebi, G. Cytokine profile and disease severity in patients with COVID-19. Cytokine 2021, 137, 155323. [Google Scholar] [CrossRef]
- Kridin, K.; Schonmann, Y.; Damiani, G.; Peretz, A.; Onn, E.; Bitan, D.T.; Cohen, A.D. Tumor necrosis factor inhibitors are associated with a decreased risk of COVID-19-associated hospitalization in patients with psoriasis-A population-based cohort study. Dermatol. Ther. 2021, 34, e15003. [Google Scholar] [CrossRef]
- Wang, J.; Jiang, M.; Chen, X.; Montaner, L.J. Cytokine storm and leukocyte changes in mild versus severe SARS-CoV-2 infection: Review of 3939 COVID-19 patients in China and emerging pathogenesis and therapy concepts. J. Leukoc. Biol. 2020, 108, 17–41. [Google Scholar] [CrossRef]
- Liu, P.; Huang, Z.; Yin, M.; Liu, C.; Chen, X.; Pan, P.; Kuang, Y. Safety and Efficacy of Ixekizumab and Antiviral Treatment for Patients with COVID-19: A structured summary of a study protocol for a Pilot Randomized Controlled Trial. Trials 2020, 21, 999. [Google Scholar] [CrossRef]
- Lebwohl, M.; Rivera-Oyola, R.; Murrell, D.F. Should biologics for psoriasis be interrupted in the era of COVID-19? J. Am. Acad. Dermatol. 2020, 82, 1217–1218. [Google Scholar] [CrossRef]
- Balestri, R.; Rech, G.; Girardelli, C.R. SARS-CoV-2 infection in a psoriatic patient treated with IL-17 inhibitor. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e357–e358. [Google Scholar] [CrossRef]
- Mugheddu, C.; Sanna, S.; Atzori, L.; Rongioletti, F. Safety of secukinumab treatment in COVID-19 affected psoriatic patients. Dermatol. Ther. 2021, 34, e14710. [Google Scholar] [CrossRef]
- Di Lernia, V.; Bombonato, C.; Motolese, A. COVID-19 in an elderly patient treated with secukinumab. Dermatol. Ther. 2020, 33, e13580. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.; Gooderham, M. Asymptomatic SARS-CoV2 infection in a patient receiving risankizumab, an inhibitor of interleukin 23. JAAD Case Rep. 2021, 7, 60–61. [Google Scholar] [CrossRef] [PubMed]
- Di Lernia, V. Antipsoriatic treatments during COVID-19 outbreak. Dermatol. Ther. 2020, 33, e13345. [Google Scholar] [CrossRef]
- Rudnicka, L.; Glowacka, P.; Goldust, M.; Sikora, M.; Sar-Pomian, M.; Rakowska, A.; Samochocki, Z.; Olszewska, M. Cyclosporine therapy during the COVID-19 pandemic. J. Am. Acad. Dermatol. 2020, 83, e151–e152. [Google Scholar] [CrossRef] [PubMed]
- Di Lernia, V.; Goldust, M.; Feliciani, C. Covid-19 infection in psoriasis patients treated with cyclosporin. Dermatol. Ther. 2020, 33, e13739. [Google Scholar] [CrossRef] [PubMed]
- Lima, X.T.; Cueva, M.A.; Lopes, E.M.; Alora, M.B. Severe COVID-19 outcomes in patients with psoriasis. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e776–e778. [Google Scholar] [CrossRef]
- Keating, G.M. Apremilast: A Review in Psoriasis and Psoriatic Arthritis. Drugs 2017, 77, 459–472. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Armstrong, A.W.; Bell, S.; Anesi, G.L.; Blauvelt, A.; Calabrese, C.; Dommasch, E.D.; Feldman, S.R.; Gladman, D.; Kircik, L.; et al. National Psoriasis Foundation COVID-19 Task Force guidance for management of psoriatic disease during the pandemic: Version 2-Advances in psoriatic disease management, COVID-19 vaccines, and COVID-19 treatments. J. Am. Acad. Dermatol. 2021, 84, 1254–1268. [Google Scholar] [CrossRef] [PubMed]
- Channappanavar, R.; Perlman, S. Pathogenic human coronavirus infections: Causes and consequences of cytokine storm and immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef]
- Ren, X.; Wen, W.; Fan, X.; Hou, W.; Su, B.; Cai, P.; Li, J.; Liu, Y.; Tang, F.; Zhang, F.; et al. COVID-19 immune features revealed by a large-scale single-cell transcriptome atlas. Cell 2021, 184, 1895–1913.e19, Erratum in Cell 2021, 184, 5838. [Google Scholar] [CrossRef]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.C.; Uhl, S.; Hoagland, D.; Møller, R.; Jordan, T.X.; Oishi, K.; Panis, M.; Sachs, D.; et al. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 2020, 181, 1036–1045.e9. [Google Scholar] [CrossRef] [PubMed]
- Ganzetti, G.; Campanati, A.; Santarelli, A.; Pozzi, V.; Molinelli, E.; Minnetti, I.; Brisigotti, V.; Procaccini, M.; Emanuelli, M.; Offidani, A. Involvement of the oral cavity in psoriasis: Results of a clinical study. Br. J. Dermatol. 2015, 172, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, J.E.; Chan, T.C.; Krueger, J.G. Psoriasis pathogenesis and the development of novel targeted immune therapies. J. Allergy Clin. Immunol. 2017, 140, 645–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dávila-Seijo, P.; Dauden, E.; Descalzo, M.A.; Carretero, G.; Carrascosa, J.M.; Vanaclocha, F.; Gómez-García, F.J.; De la Cueva-Dobao, P.; Herrera-Ceballos, E.; Belinchón, I.; et al. Infections in Moderate to Severe Psoriasis Patients Treated with Biological Drugs Compared to Classic Systemic Drugs: Findings from the BIOBADADERM Registry. J. Investig. Dermatol. 2017, 137, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Campanati, A.; Ganzetti, G.; Giuliodori, K.; Molinelli, E.; Offidani, A. Biologic Therapy in Psoriasis: Safety Profile. Curr. Drug Saf. 2016, 11, 4–11. [Google Scholar] [CrossRef]
- Bardazzi, F.; Magnano, M.; Campanati, A.; Loconsole, F.; Carpentieri, A.; Potenza, C.; Bernardini, N.; Di Lernia, V.; Carrera, C.; Raone, B.; et al. Biologic Therapies in HIV-infected Patients with Psoriasis: An Italian Experience. Acta Dermato Venereol. 2017, 97, 989–990. [Google Scholar] [CrossRef] [Green Version]
- Ladda, M.; Lynde, C.; Fleming, P. Severe Acute Respiratory Syndrome Coronavirus 2 and the Use of Biologics in Patients with Psoriasis. J. Cutan. Med. Surg. 2020, 24, 625–632. [Google Scholar] [CrossRef]
- Piaserico, S.; Gisondi, P.; Cazzaniga, S.; Naldi, L. Lack of Evidence for an Increased Risk of Severe COVID-19 in Psoriasis Patients on Biologics: A Cohort Study from Northeast Italy. Am. J. Clin. Dermatol. 2020, 21, 749–751. [Google Scholar] [CrossRef]
- Campanati, A.; Moroncini, G.; Ganzetti, G.; Pozniak, K.N.; Goteri, G.; Giuliano, A.; Martina, E.; Liberati, G.; Ricotti, F.; Gabrielli, A.; et al. Adalimumab modulates angiogenesis in psoriatic skin. Eur. J. Inflamm. 2013, 11, 489–498. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Galluzzo, M.; Tofani, L.; Bianchi, L.; Talamonti, M. Status of a real-life cohort of patients with moderate-to-severe plaque psoriasis treated with secukinumab and considerations on the use of biological agents in the Covid-19 era. Expert Opin. Biol. Ther. 2020, 20, 829–830. [Google Scholar] [CrossRef] [PubMed]
- Conti, A.; Lasagni, C.; Bigi, L.; Pellacani, G. Evolution of COVID-19 infection in four psoriatic patients treated with biological drugs. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e360–e361. [Google Scholar] [CrossRef] [PubMed]
- Messina, F.; Piaserico, S. SARS-CoV-2 infection in a psoriatic patient treated with IL-23 inhibitor. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e254–e255. [Google Scholar] [CrossRef] [Green Version]
- Benhadou, F.; Del Marmol, V. Improvement of SARS-CoV-2 symptoms following Guselkumab injection in a psoriatic patient. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e363–e364. [Google Scholar] [CrossRef] [PubMed]
- de Wilde, A.H.; Pham, U.; Posthuma, C.C.; Snijder, E.J. Cyclophilins and cyclophilin inhibitors in nidovirus replication. Virology 2018, 522, 46–55. [Google Scholar] [CrossRef] [PubMed]
- West, J.; Ogston, S.; Foerster, J. Safety and Efficacy of Methotrexate in Psoriasis: A Meta-Analysis of Published Trials. PLoS ONE 2016, 11, e0153740, Erratum in PLoS ONE 2016, 11, e0158928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kridin, K.; Schonmann, Y.; Tzur Bitan, D.; Damiani, G.; Peretz, A.; Weinstein, O.; Cohen, A.D. Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization and Mortality in Patients with Psoriasis: A Population-Based Study. Am. J. Clin. Dermatol. 2021, 22, 709–718. [Google Scholar] [CrossRef]
- Veenstra, J.; Buechler, C.R.; Robinson, G.; Chapman, S.; Adelman, M.; Tisack, A.; Dimitrion, P.; Todter, E.; Kohen, L.; Lim, H.W. Antecedent immunosuppressive therapy for immune-mediated inflammatory diseases in the setting of a COVID-19 outbreak. J. Am. Acad. Dermatol. 2020, 83, 1696–1703. [Google Scholar] [CrossRef]
- Olisova, O.Y.; Anpilogova, E.M.; Svistunova, D.A. Apremilast as a potential treatment option for COVID-19: No symptoms of infection in a psoriatic patient. Dermatol. Ther. 2020, 33, e13668. [Google Scholar] [CrossRef]
- Lytvyn, Y.; Georgakopoulos, J.R.; Mufti, A.; Devani, A.R.; Gooderham, M.J.; Jain, V.; Lansang, P.; Vender, R.; Prajapati, V.H.; Yeung, J. Incidence and prognosis of COVID-19 in patients with psoriasis on apremilast: A multicentre retrospective cohort study. J. Eur. Acad. Dermatol. Venereol. 2021, 36, e94–e95. [Google Scholar] [CrossRef]
- Yalcin, A.D.; Yalcin, A.N. Future perspective: Biologic agents in patients with severe COVID-19. Immunopharmacol. Immunotoxicol. 2021, 43, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mugheddu, C.; Pizzatti, L.; Sanna, S.; Atzori, L.; Rongioletti, F. COVID-19 pulmonary infection in erythrodermic psoriatic patient with oligodendroglioma: Safety and compatibility of apremilast with critical intensive care management. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e376–e378. [Google Scholar] [CrossRef]
- Sun, Q.; Fathy, R.; McMahon, D.E.; Freeman, E.E. COVID-19 Vaccines and the Skin: The Landscape of Cutaneous Vaccine Reactions Worldwide. Dermatol. Clin. 2021, 39, 653–673. [Google Scholar] [CrossRef]
- Sotiriou, E.; Tsentemeidou, A.; Bakirtzi, K.; Lallas, A.; Ioannides, D.; Vakirlis, E. Psoriasis exacerbation after COVID-19 vaccination: A report of 14 cases from a single centre. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e857–e859. [Google Scholar] [CrossRef] [PubMed]
- Priebe, G.P.; Walsh, R.L.; Cederroth, T.A.; Kamei, A.; Coutinho-Sledge, Y.S.; Goldberg, J.B.; Pier, G.B. IL-17 is a critical component of vaccine-induced protection against lung infection by lipopolysaccharide-heterologous strains of Pseudomonas aeruginosa. J. Immunol. 2008, 181, 4965–4975. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Slight, S.R.; Khader, S.A. Th17 cytokines and vaccine-induced immunity. Semin. Immunopathol. 2010, 32, 79–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Megna, M.; Potestio, L.; Gallo, L.; Caiazzo, G.; Ruggiero, A.; Fabbrocini, G. Reply to “Psoriasis exacerbation after COVID-19 vaccination: Report of 14 cases from a single centre” by Sotiriou E et al. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e11–e13. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, M.L.; Caruso, G.; Trecarichi, A.C.; Micali, G. Safety of SARS-CoV-2 vaccines in psoriatic patients treated with biologics: A real life experience. Dermatol. Ther. 2021, 26, e15177. [Google Scholar] [CrossRef] [PubMed]
- Bostan, E.; Elmas, L.; Yel, B.; Yalici-Armagan, B. Exacerbation of plaque psoriasis after inactivated and BNT162b2 mRNA COVID-19 vaccines: A report of two cases. Dermatol. Ther. 2021, 34, e15110. [Google Scholar] [CrossRef] [PubMed]
- Onsun, N.; Kaya, G.; Işık, B.G.; Güneş, B. A generalized pustular psoriasis flare after CoronaVac COVID-19 vaccination: Case report. Health Promot. Perspect. 2021, 11, 261–262. [Google Scholar] [CrossRef]
- Lehmann, M.; Schorno, P.; Hunger, R.E.; Heidemeyer, K.; Feldmeyer, L.; Yawalkar, N. New onset of mainly guttate psoriasis after COVID-19 vaccination: A case report. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e752–e755. [Google Scholar] [CrossRef] [PubMed]
- Krajewski, P.K.; Matusiak, Ł.; Szepietowski, J.C. Psoriasis flare-up associated with second dose of Pfizer-BioNTech BNT16B2b2 COVID-19 mRNA vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e632–e634. [Google Scholar] [CrossRef] [PubMed]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Campanati, A.; Martina, E.; Diotallevi, F.; Radi, G.; Kontochristopoulos, G.; Rigopoulos, D.; Gregoriou, S.; Offidani, A. How to fight SARS-COV-2 vaccine hesitancy in patients suffering from chronic and immune-mediated skin disease: Four general rules. Hum. Vaccin Immunother. 2021, 17, 1–3. [Google Scholar] [CrossRef]
- Loewenstein, G.; Sunstein, C.R.; Golman, R. Disclosure: Psychology changes everything. Annu. Rev. Econ. 2014, 6, 391–419. [Google Scholar] [CrossRef]
- Bavel, J.J.V.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Habersaat, K.B.; Betsch, C.; Danchin, M.; Sunstein, C.R.; Böhm, R.; Falk, A.; Brewer, N.T.; Omer, S.B.; Scherzer, M.; Sah, S.; et al. Ten considerations for effectively managing the COVID-19 transition. Nat. Hum. Behav. 2020, 4, 677–687. [Google Scholar] [CrossRef]
- Toppenberg-Pejcic, D.; Noyes, J.; Allen, T.; Alexander, N.; Vanderford, M.; Gamhewage, G. Emergency Risk Communication: Lessons Learned from a Rapid Review of Recent Gray Literature on Ebola, Zika, and Yellow Fever. Health Commun. 2019, 34, 437–455. [Google Scholar] [CrossRef]
- Diotallevi, F.; Campanati, A.; Radi, G.; Martina, E.; Rizzetto, G.; Barbadoro, P.; D’Errico, M.M.; Offidani, A. Vaccination against SARS-CoV-2 and psoriasis: The three things every dermatologist should know. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e428–e430. [Google Scholar] [CrossRef]
- Hollander, J.E.; Carr, B.G. Virtually Perfect? Telemedicine for COVID-19. N. Engl. J. Med 2020, 382, 1679–1681. [Google Scholar] [CrossRef]
- Lee, C.H.; Huang, C.C.; Huang, J.T.; Wang, C.C.; Fan, S.; Wang, P.S.; Lan, K.C. Live-interactive teledermatology program in Taiwan: One-year experience serving a district hospital in rural Taitung County. J. Formos. Med. Assoc. 2021, 120 Pt 2, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Brunasso, A.M.G.; Massone, C. Teledermatologic monitoring for chronic cutaneous autoimmune diseases with smartworking during COVID-19 emergency in a tertiary center in Italy. Dermatol. Ther. 2020, 33, e13495. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Bellinato, F.; Piaserico, S.; Di Leo, S.; Cazzaniga, S.; Naldi, L. Preference for Telemedicine Versus In-Person Visit Among Patients with Psoriasis Receiving Biological Drugs. Dermatol. Ther. (Heidelb.) 2021, 11, 1333–1343. [Google Scholar] [CrossRef]
- Uscher-Pines, L.; Malsberger, R.; Burgette, L.; Mulcahy, A.; Mehrotra, A. Effect of teledermatology on access to dermatology care among medicaid enrollees. JAMA Dermatol. 2016, 152, 905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linggonegoro, D.W.; Sanchez-Flores, X.; Huang, J.T. How telemedicine may exacerbate disparities in patients with limited English proficiency. J. Am. Acad. Dermatol. 2021, 84, E289–E290. [Google Scholar] [CrossRef]
- Trettel, A.; Eissing, L.; Augustin, M. Telemedicine in dermatology: Findings and experiences world- wide—a systematic literature review. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.Z.; Reynolds, R.V.; Olbricht, S.M.; McGee, J.S. Moving forward with teledermatology: Operational challenges of a hybrid in-person and virtual practice. Clin. Dermatol. 2021, 39, 707–709. [Google Scholar] [CrossRef]
- Ciechanowicz, P.; Dopytalska, K.; Mikucka-Wituszyńska, A.; Dźwigała, M.; Wiszniewski, K.; Herniczek, W.; Szymańska, E.; Walecka, I. The prevalence of SARS-CoV-2 infection and the severity of the course of COVID-19 in patients with psoriasis treated with biologic therapy. J. Dermatol. Treat. 2020, 1–4. [Google Scholar] [CrossRef]
- Gadarowski, M.B.; Balogh, E.A.; Bashyam, A.M.; Feldman, S.R. Examining recommendations for the use of biologics and other systemic therapies during COVID-19: A review and comparison of available dermatology guidelines and patient registries. J. Dermatol. Treat. 2020, 30, 1–5. [Google Scholar] [CrossRef]
- Kearns, D.G.; Uppal, S.; Chat, V.S.; Wu, J.J. Use of systemic therapies for psoriasis in the COVID-19 era. J. Dermatol. Treat. 2021, 33, 622–625. [Google Scholar] [CrossRef]
- Radi, G.; Diotallevi, F.; Campanati, A.; Offidani, A. Global coronavirus pandemic (2019-nCOV): Implication for an Italian medium size dermatological clinic of a II level hospital. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e213–e214. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Type of Study [Reference] | Outcomes | Number of Patients | Results |
|---|---|---|---|
| systematic review [3] | Evaluated presentations, post-infection change in the manifestation, diagnosis, and management of flare-ups | 9 patients with psoriasis and COVID-19 | 5 cases of flare-ups due to hydroxychloroquine or systemic corticosteroids therapy for COVID-19 3 cases of exacerbation of psoriasis (2 resulted from the discontinuation of treatments 1 case due to COVID-19) |
| Case report [4] | New onset of pustular psoriasis (PP) | A case of a 62-year-old woman with family history of psoriasis | New PP 2 weeks after resolution of symptoms of SARS-CoV-2 infection |
| Case report [5] | New onset of pustular psoriasis (PP) | Patient with personal history of psoriasis | Administration of hydroxychloroquine before the flare |
| Case report [6] | New onset of generalized PP (GPP) | 60-year-old male patient with personal history of psoriasis | New GPP 26 days after the onset of initial COVID-19 symptoms |
| Case report [7] | New onset of pustular psoriasis (PP) | 62-year-old patient with a history of Acrodermatitis of Hallopeau | New PP after SARS-CoV-2 infection |
| Type of Study [Reference] | Outcomes | Number of Patients | Results |
|---|---|---|---|
| Reviews, meta-analysis [11,12] | The role of angiotensin converting enzyme in the link between psoriasis and risk of the COVID-19 | NA | Psoriasic patients may be at an higher risk of worsening cardiovascular events in case of COVID-19 infection |
| Epidemiological analysis [13] | Genome-wide association study transdisease meta-analysis between COVID-19 susceptibility and two skin diseases (psoriasis and atopic dermatitis). | 435,019 patients | Having an inflammatory skin disease decreased the risk of requiring mechanical ventilation |
| Reviews, meta-analysis, National Psoriasis Foundation guidelines [14,15,16,17,18,19,20,21] | Prognostic factors of COVID-19 outcome in psoriatic patients | NA | Severity of COVID-19 is primarily driven by smoking status, sex (male), older age, and underlying comorbidities; Age, male sex, and pre-existing comorbidities are crucial drivers for poor COVID-19 outcome in patients with psoriasis |
| Type of Study [Reference] | Outcomes | Number of Patients | Results |
|---|---|---|---|
| Cohort study [40] | COVID-19 infection, hospitalization, and mortality rates in psoriatic patients on biologic treatment | 1830 patients | COVID-19 infection, hospitalization, and mortality rates were not increased in psoriatic patients on biologic treatment compared to the general population. COVID-19 incidence rate IR: 9.7 (95% CI 3.9–20.1) vs. 11.5 (95% CI 11.4–11.7) per 10,000 person-months; Hospitalization IR: 6.5 (95% CI 2.0–15.6) vs. 9.6 (95% CI 9.4–9.7) per 10,000 person-months COVID-19-related death IR: 0 (95% CI 0–10.4) vs. 1.16 (95% CI 1.10–1.21) per 10,000 person-months |
| Global registry-based study [37] | 374 clinician-reported patients | The risk of COVID-19-related hospitalization is lower in patients treated with biologic drugs than in those treated with nonbiologic systemic therapies | |
| Multicenter study [41] | 1322 patients with psoriasis | Not statistically significant difference in COVID-19-related hospitalization between psoriatic patients using biologics (n = 9) and those not using biologics (n = 14) | |
| TNF alpha inhibitors | |||
| Population-based cohort study [42] | Risk of COVID-19 infection, COVID-19-associated hospitalization, and mortality among patients with psoriasis treated by TNF alpha inhibitors compared with psoriatic patients receiving other systemic agents. | Psoriatic patients treated with: TNF alpha inhibitors (n = 1943) methotrexate (n = 1929) ustekinumab (n = 348) acitretin (n = 1892) | The risk of COVID-19 infection was comparable among subjects treated with TNF alpha inhibitors vs. methotrexate, ustekinumab and acitretin; Exposure to TNF alpha inhibitors reduced the risk of COVID-19-associated hospitalization compared with methotrexate and ustekinumab, but not with acitretin No significant difference in COVID-19-associated mortality was observed among the treatment groups |
| IL17A/IL17R inhibitors | |||
| Clinical trial [43] | Safety and efficacy of ixekizumab treatment for psoriatic patients with COVID-19 | recruiting | No evidence that IL-17 inhibitors increase the risk of SARS-CoV-2 infection or result in more severe COVID-19 |
| Case report [44] | Psoriatic patient infected during ixekizumab induction phase | Recovered from a completely asymptomatic SARS-CoV-2 infection after 1 month without specific treatment | |
| 136-week real-life study [45] | Safety of secukinumab treatment for psoriatic patients with COVID-19 | 151 patients with moderate to severe plaque psoriasis | 119 out of 151 patients continued treatment with secukinumab during the pandemic and none developed confirmed SARS-CoV-2 infection |
| Case series [46] | 2 psoriatic patients infected with SARS-CoV-2 under long-term secukinumab | Recovered from the infection between the two scheduled doses of secukinumab | |
| Case report [47] | Elderly psoriatic patient with hypertension | Recovered from mild COVID-19 during treatment with secukinumab with a favorable outcome | |
| IL-23 inhibitors | |||
| Multicentric study [48] | Safety of IL-23 inhibitors treatment for psoriatic patients with COVID-19 | 57 patients with moderate to severe plaque psoriasis monitored during the first 4 months of the pandemic. | In this study, only one patient (1.8%) experienced upper respiratory tract infection; three patients (5.3%) had contact with SARS-CoV-2- infected subjects, and none among them developed SARS-CoV-2 disease |
| Case report [49] | 32-year-old woman under Guselkumab | Full recovery from COVID-19, remained asymptomatic | |
| Case report [50] | 40-year-old under Guselkumab | Full recovery from COVID-19 with development of mild symptoms | |
| Case report [51] | 45-year-old man under Risankizumab | Full recovery from COVID-19, remained asymptomatic | |
| Cyclosporine | |||
| Observational cohort study [52] | Safety of cyclosporine treatment for psoriatic patients with COVID-19 | 114 adult patients with psoriasis under cyclosporine | Neither COVID-related deaths nor hospitalizations for COVID-19-related interstitial pneumonia have been reported Two psoriatic patients reported mild respiratory symptoms, with no need for hospital admission: a preventive suspension of CsA was adopted at the onset of symptoms until their complete remission |
| Methotrexate | |||
| Case–control study [53] | Safety of MTX treatment for psoriatic patients with COVID-19 | 3151 patients with psoriasis tested positive for COVID-19 | Increased hospitalization risk inde-pendently associated with MTX |
| Observational cohort study [54] | 104 psoriasic patients under MTX | No significant difference in COVID-19 severity between the 13 COVID-19 patients treated with methotrexate (10–22.5 mg/week) and psoriasis patients not receiving any systemic treatment | |
| Retrospective cohort analysis [55] | 65 psoriatic patients under MTX | No significant association of methotrexate use with SARS-CoV-2 infection rates, percentage of COVID-19-positive patients who required hospitalization, need for ventilator use, or mortality | |
| Apremilast | |||
| Retrospective analysis [56] | Safety of Apremilst treatment for psoriatic patients with COVID-19 | 402 psoriatic patients under apremilast | No documented cases of COVID-19 |
| Case report [57] | 45-year-old man with erythrodermic psoriasis | Affected by SARS-CoV-2 pneumonia. He continued Apremilast and recovered after six days of therapy with lopinavir/ritonavir 400/100 mg twice daily and intravenous ceftriaxone 2 g/day | |
| Type of Study [Reference] | Outcomes | Number of Patients | Results |
|---|---|---|---|
| Case series [80] | Aggravation of psoriasis following COVID-19 immunization | 14 episodes | Exacerbation of psoriasis occurred in all patients shortly after vaccination with no difference in timing (mean, 10.36 days +/− 7.71) or severity between the vaccinations employed (50% mRNA technology vaccines and 50% adenovirus vaccine) 9 cases treated with systemic drugs or phototherapy 5 patients received topical therapy |
| Case series [83] | 11 occurrences of psoriasis aggravation | 2 cases of switch in biological agents 54.5% of psoriasis flares associated with the COVID-19 vaccination occurred in individuals receiving biologic therapy; topical calcipotriol/betamethasone and/or phototherapy added to therapy; | |
| Survey [84] | Safety of SARS-CoV-2 vaccinations in patients with psoriasis under biologic therapy | 50 psoriatic patients under biologic treatment (24 under anti-TNF therapy, 14 under anti-IL17, 7 under anti-IL12-23 and 5 under anti-IL23) received 2 doses of SARS-CoV-2 vaccination | 1 episode of aggravation of psoriasis under infliximab biosimilar, following vaccination |
| Case series [85] | Safety of SARS-CoV-2 vaccinations in patients with psoriasis undergoing topical treatment | 2 psoriatic patients receiving CoronaVac, China and Pfizer/Biontech, Germany respectively | one month after the second dosage of CoronaVac, China and two weeks after first dosage of Pfizer/Biontech, Germany, onset of extensive plaque expansion topically treated |
| Case report [86] | 72-year-old man previously treated with topicals | Beginning of generalized pustular psoriasis four days after receiving the first dose of the inactivated SARS-CoV-2 vaccine (CoronaVac, China) | |
| Case report [87] | New-onset of psoriasis following COVID-19 immunization | 79-year-old female | New-onset of guttate psoriasis 10 days after the first dosage and flared up following the second dose of BNT162b2 mRNA vaccination. Recovered after calcipotriol/betamethasone ointment and UVB phototherapy |
| Case report [88] | Safety of SARS-CoV-2 vaccinations in patients with psoriasis treated with Deucravacitinib | Psoriatic patient in full remission | Aggravation of plaque psoriasis five days after receiving the second dose of BNT162b2 mRNA SARS-CoV-2 vaccination, |
| Observational cohort study [89] | Safety of SARS-CoV-2 vaccinations in patients with psoriatic arthritis PsA | 131 patients with PsA | PASI value remained constant in the majority of cases following immunization |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campanati, A.; Diotallevi, F.; Martina, E.; Radi, G.; Offidani, A. Treatment of Moderate to Severe Psoriasis during the COVID-19 Pandemic: Lessons Learned and Opportunities. J. Clin. Med. 2022, 11, 2422. https://doi.org/10.3390/jcm11092422
Campanati A, Diotallevi F, Martina E, Radi G, Offidani A. Treatment of Moderate to Severe Psoriasis during the COVID-19 Pandemic: Lessons Learned and Opportunities. Journal of Clinical Medicine. 2022; 11(9):2422. https://doi.org/10.3390/jcm11092422
Chicago/Turabian StyleCampanati, Anna, Federico Diotallevi, Emanuela Martina, Giulia Radi, and Annamaria Offidani. 2022. "Treatment of Moderate to Severe Psoriasis during the COVID-19 Pandemic: Lessons Learned and Opportunities" Journal of Clinical Medicine 11, no. 9: 2422. https://doi.org/10.3390/jcm11092422