
Erythema Migrans-like COVID Vaccine Arm: A Literature Review

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
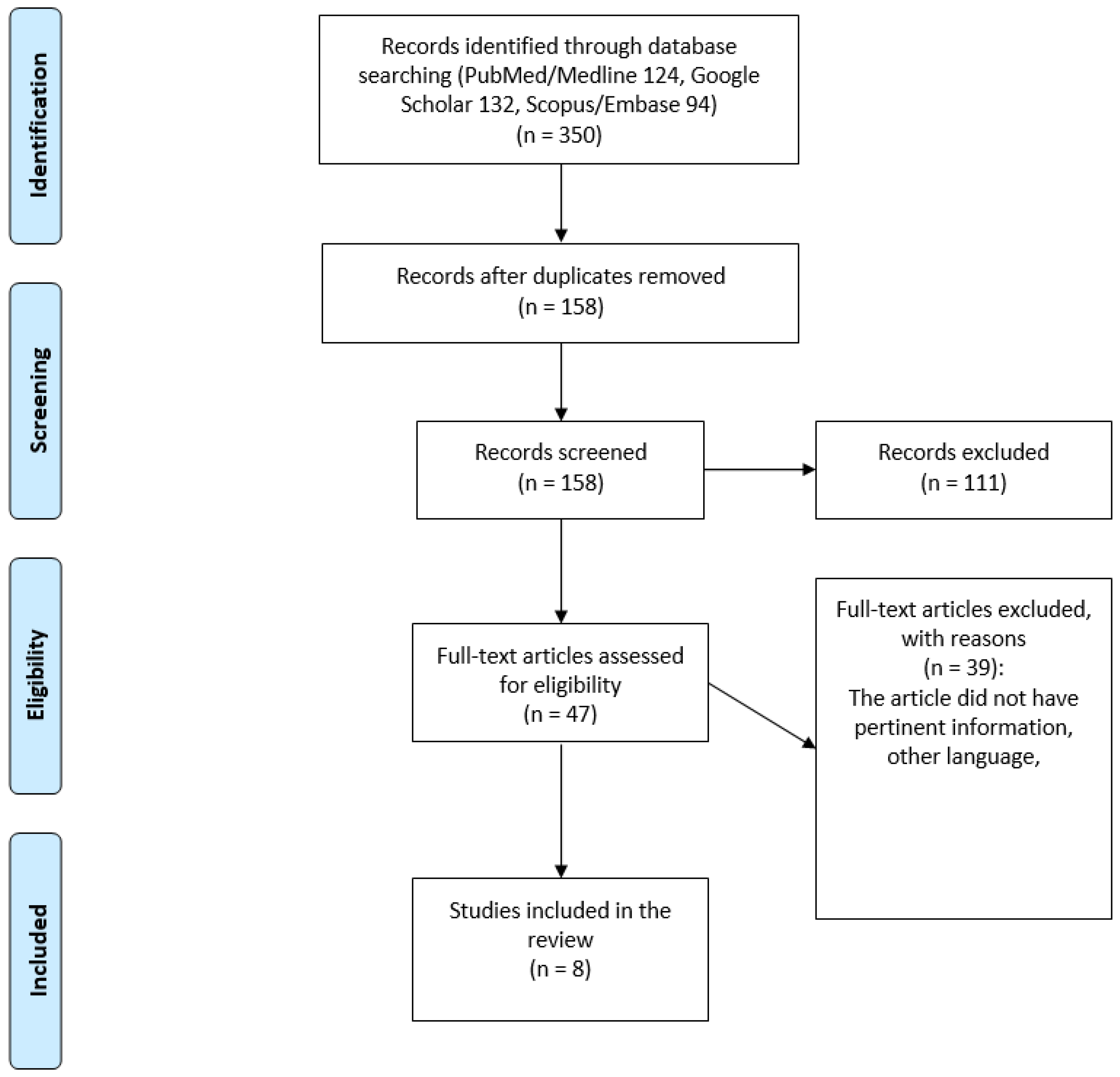
2. Materials and Methods
3. Results
4. Discussion
4.1. Cutaneous Reactions after COVID-19 Vaccination
4.2. Differential Diagnosis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. COVID Data Tracker. Available online: http://covid.cdc.gov/covid-data-tracker/#global-counts-rates (accessed on 12 February 2021).
- Fernandez-Nieto, D.; Hammerle, J.; Fernandez-Escribano, M.; Moreno-Del Real, C.M.; Garcia-Abellas, P.; Carretero-Barrio, I.; Solano-Solares, E.; de-la-Hoz-Caballer, B.; Jimenez-Cauhe, J.; Ortega-Quijano, D.; et al. Skin manifestations of the BNT162b2 mRNA COVID-19 vaccine in healthcare workers. ‘COVID-arm’: A clinical and histological characterization. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e425–e427. [Google Scholar] [CrossRef] [PubMed]
- Gregoriou, S.; Kleidona, I.A.; Tsimpidakis, A.; Nicolaidou, E.; Stratigos, A.; Rigopoulos, D. ‘COVID vaccine arm’ may present after both mRNA vaccines vaccination. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e867–e868. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, K.G.; Freeman, E.E.; Saff, R.R. Delayed large local reactions to mRNA-1273 vaccine against SARS-CoV-2. N. Engl. J. Med. 2021, 384, 1273–1277. [Google Scholar] [CrossRef] [PubMed]
- Cdc.gov. Reactions and Adverse Events of the Pfizer-BioNTech COVID-19 Vaccine j CDC. 2021. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/pfizer/reactogenicity.html (accessed on 4 February 2021).
- Banerji, A.; Wickner, P.G.; Saff, R.; Stone, C.A., Jr.; Robinson, L.B.; Long, A.A.; Wolfson, A.R.; Williams, P.; Khan, D.A.; Phillips, E.; et al. mRNA vaccines to prevent COVID-19 disease and reported allergic reactions: Current evidence and suggested approach. J. Allergy Clin. Immunol. Pract. 2020, 9, 1423–1437. [Google Scholar] [CrossRef]
- Wei, N.; Fishman, M.; Wattenberg, D.; Gordon, M.; Lebwohl, M. “COVID arm”: A reaction to the Moderna vaccine. JAAD Case Rep. 2021, 10, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Saifuddin, A.; Koesnoe, S.; Kurniati, N.; Sirait, S.; Arisanty, R.; Yunihastuti, E. COVID Arm After Moderna Booster in Healthcare Worker: A Case Report. Acta Med. Indones. 2021, 53, 326–330. [Google Scholar] [PubMed]
- Johnston, M.S.; Galan, A.; Watsky, K.L.; Little, A.J. Delayed Localized Hypersensitivity Reactions to the Moderna COVID-19 Vaccine: A Case Series. JAMA Dermatol. 2021, 157, 716–720. [Google Scholar] [CrossRef]
- Barriere, J.; Bondouy, M. COVID arm and PET/FDG imaging. Bull. Cancer 2021, 108, 668–669. [Google Scholar] [CrossRef]
- Zengarini, C.; Artanidi, C.; Preci, C.; Gaspari, V. Erythema migrans-like rash after Moderna vaccine: An uncommon type of “COVID arm”. Dermatol. Ther. 2021, 34, e15063. [Google Scholar] [CrossRef]
- Kempf, W.; Kettelhack, N.; Kind, F.; Courvoisier, S.; Galambos, J.; Pfaltz, K. ‘COVID arm’—Histological features of a delayed-type hypersensitivity reaction to Moderna mRNA-1273 SARS-CoV2 vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e730–e732. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, A.L.; Austin, A.H.; Welsh, K.M. COVID Arm: Delayed Hypersensitivity Reactions to SARS-CoV-2 Vaccines Misdiagnosed as Cellulitis. J. Prim. Care Community Health 2021, 12, 21501327211024431. [Google Scholar] [CrossRef]
- Mauriello, P.M.; Barde, S.H.; Georgitis, J.W.; Reisman, R.E. Natural history of large local reactions from stinging insects. J. Allergy Clin. Immunol. 1984, 74 (Pt 1), 494–498. [Google Scholar] [CrossRef]
- Allergic Reactions. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/allergic-reaction.html (accessed on 26 August 2021).
- Gambichler, T.; Boms, S.; Susok, L.; Dickel, H.; Finis, C.; Abu Rached, N.; Barras, M.; Stücker, M.; Kasakovski, D. Cutaneous findings following COVID-19 vaccination: Review of world literature and own experience. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 172–180. [Google Scholar] [CrossRef]
- Sun, Q.; Fathy, R.; McMahon, D.E.; Freeman, E.E. COVID-19 Vaccines and the Skin: The Landscape of Cutaneous Vaccine Reactions Worldwide. Dermatol. Clin. 2021, 39, 653–673. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2020, 384, 403–416. [Google Scholar] [CrossRef]
- Bennardo, L.; Nisticò, S.P.; Dastoli, S.; Provenzano, E.; Napolitano, M.; Silvestri, M.; Passante, M.; Patruno, C. Erythema Multiforme and COVID-19: What Do We Know? Medicina 2021, 57, 828. [Google Scholar] [CrossRef]
- Dastoli, S.; Bennardo, L.; Patruno, C.; Nisticò, S.P. Are erythema multiforme and urticaria related to a better outcome of COVID-19? Dermatol. Ther. 2020, 33, e13681. [Google Scholar] [CrossRef] [PubMed]
- Mazzitelli, M.; Dastoli, S.; Mignogna, C.; Bennardo, L.; Lio, E.; Pelle, M.C.; Trecarichi, E.M.; Pereira, B.I.; Nisticò, S.P.; Torti, C. Histopathology and immunophenotyping of late onset cutaneous manifestations of COVID-19 in elderly patients: Three case reports. World J. Clin Cases 2021, 9, 5744–5751. [Google Scholar] [CrossRef] [PubMed]
- Khalid, M.; Lipka, O.; Becker, C. Moderna COVID-19 vaccine induced skin rash. Vis. J. Emerg. Med. 2021, 25, 101108. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, M.; Henry, D.; Finon, A.; Binois, R.; Esteve, E. Persistent maculopapular rash after the first dose of Pfizer-BioNTech COVID-19 vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 423–425. [Google Scholar] [CrossRef] [PubMed]
- Soyfer, V.; Gutfeld, O.; Shamai, S.; Schlocker, A.; Merimsky, O. COVID-19 vaccine-induced radiation recall phenomenon. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 957–961. [Google Scholar] [CrossRef]
- Munavalli, G.G.; Guthridge, R.; Knutsen-Larson, S. COVID-19/SARS-CoV-2 virus spike protein-related delayed inflammatory reaction to hyaluronic acid dermal fillers: A challenging clinical conundrum in diagnosis and treatment. Arch. Dermatol. Res. 2022, 314, 1–15. [Google Scholar] [CrossRef]
- Lopatynsky-Reyes, E.Z.; Acosta-Lazo, H.; Ulloa-Gutierrez, R.; Ávila-Aguero, M.L.; Chacon-Cruz, E. BCG Scar Local Skin Inflammation as a Novel Reaction Following mRNA COVID-19 Vaccines in Two International Healthcare Workers. Cureus 2021, 13, e14453. [Google Scholar] [CrossRef] [PubMed]
- Clinical Trial Data Moderna COVID-19 Vaccine (EUA). Available online: https://www.modernatx.com/covid19vaccine-eua/providers/clinical-trial-data (accessed on 4 February 2021).
- McMahon, D.E.; Amerson, E.; Rosenbach, M.; Lipoff, J.B.; Moustafa, D.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W.; Thiers, B.H.; et al. Cutaneous reactions reported after Moderna and Pfizer COVID-19 vaccination: A registry-based study of 414 cases. J. Am. Acad. Dermatol. 2021, 85, 46–55. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- De Montjove, L.; Marot, L.; Baeck, M. Eosinophilic cellulitis after BNT162b2 mRNA Covid-19 vaccine. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e26–e28. [Google Scholar]
- Yu, A.M.; Ito, S.; Leibson, T.; Lavi, S.; Fu, L.W.; Weinstein, M.; Skotnicki, S.M. Pediatric Wells syndrome (eosinophilic cellulitis) after vaccination: A case report and review of the literature. Pediatr. Dermatol. 2018, 35, e262–e264. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Local Reactions, Systemic Reactions, Adverse Events, and Serious Adverse Events: Moderna COVID-19 Vaccine. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/moderna/reactogenicity.html (accessed on 12 February 2021).



{kind=link}
{kind=link}
| Author | Study Type | Number of Patients | Type of Vaccine |
|---|---|---|---|
| Wei et al. [8] | Case series | 4 | Moderna mRNA-1273 |
| Anshari et al. [9] | Case report | 1 | Moderna mRNA-1273 |
| Zengarini et al. [12] | Case report | 1 | Moderna mRNA-1273 |
| Kempf et al. [13] | Case series | 3 | Moderna mRNA-1273 |
| Barriere et al. [11] | Case report | 1 | Cominarty (Pfizer/BioNTech) |
| Gregoriou et al. [4] | Case series | 4 | Moderna mRNA-1273 and Cominarty (Pfizer/BioNTech) |
| Blumenthal et al. [5] | Case series | 12 | Moderna mRNA-1273 |
| Lindgren et al. [14] | Case series | 3 | Moderna mRNA-1273 and Cominarty (Pfizer/BioNTech) |
| Study and Patient’s Number | Age | Gender | Medical History or Allergies | Type of Vaccine | Days after Vaccination | Localized Symptoms | Rash Diameter | Systemic Symptoms | Skin Biopsy | Therapy | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Wei et al. [1] | 74 | Female | No | Moderna mRNA-1273 | 8 days after first dose | Pruritus, erythematous plaque, mild scaling | 15 cm | No | No | Topical clobetasol proprionate 0.05% cream and oral cetirizine 10 mg | Partial resolution after 1 week |
| Wei et al. [2] | 62 | Female | No | Moderna mRNA-1273 | 8 days after first dose | Pruritus, erythematous plaque, edema, warmth | Not reported | No | No | Mometasone furoate 0.01% ointment, diphenhydramine hydrochloride 1% cream, oral loratadine 10 mg | |
| Wei et al. [3] | 54 | Female | No | Moderna mRNA-1273 | 7 days after first dose | Erythematous rash | Not reported | No | No | No | Resolving spontaneously in 4 days |
| Wei et al. [4] | 72 | Female | Psoriasis, atrial fibrillation, hypercholesterolemia, hypothyroidism | Moderna mRNA-1273 | 10 days after first dose | Pruritus, Erythematous plaque, warmth | 14 cm | No | No | No | Resolving spontaneously in 2 days |
| Anshari et al. [1] | 56 | Female | Breast cancer, atopic history with eczema and allergic rhinitis, thalassemia trait | Moderna mRNA-1273 | 3 days after second dose | Swell, redness, warm, pain | Not reported | No | Focal spongiosis and vacuolar alteration in the epidermidis. Inflammatory infiltrate perivascular in the dermis with lymphocytes and some histocytes and neutrophils. | Surface cooling and compression | Resolution after 5 days |
| Zengarini et al. [1] | 63 | Female | No | Moderna mRNA-1273 | 5 days after first dose | Flat and targetoid erythema with bull’s eye aspect | Not reported | No | No | Surface cooling and compression | Resolution after 2 days |
| Kempf et al. [1] | 84 | Male | Melanoma, non-melanoma skin cancer | Moderna mRNA-1273 | 7 days after first dose | Erythema | Not reported | No | Focal spongiosis and exocytosis of a few lymphocytes in the epidermidis. Inflammatory infiltrate perivascular in the dermis with lymphocytes and some eosinophilic granulocytes and neutrophils. | ||
| Kempf et al. [2] | 86 | Female | Non-melanoma skin cancer | Moderna mRNA-1273 | 7 days after first dose | Erythema | Not reported | No | Focal spongiosis and exocytosis of a few lymphocytes in the epidermidis. Inflammatory infiltrate perivascular in the dermis with lymphocytes and some eosinophilic granulocytes and neutrophils. | ||
| Kempf et al. [3] | 81 | Female | Non-melanoma skin cancer, eczema of hand | Moderna mRNA-1273 | 7 days after first dose | Erythema | Not reported | No | Focal spongiosis and exocytosis of a few lymphocytes in the epidermidis. Inflammatory infiltrate perivascular in the dermis with lymphocytes and some eosinophilic granulocytes and neutrophils. | ||
| Barriere et al. [1] | 76 | Female | Ovarian Neoplasia | Comirnaty Pfizer-Biontech | 5 days after the second dose | Inflammatory edema, pain | Not reported | No | No | ||
| Gregoriou et al. [1] | 733 | Female | No | Moderna mRNA-1273 | 9 days after first dose | Erythematous papules with red plaque, scaling, pruritus | 7 cm | No | No | Topical methylprednisolone-aceponate 0.1% cream and desloratadine | Resolution after 4 days |
| Gregoriou et al. [2] | 74 | Female | Chronic obstructive pulmonary disease (COPD), pulmonary hypertension | Cominarty (Pfizer/BioNTech) | 8 days after second dose | Erythematous plaque | Not reported | No | No | Topical methylprednisolone-aceponate 0.1% cream | Resolution after 3 days |
| Gregoriou et al. [3] | 51 | Female | No | Moderna mRNA-1273 | 9 days after first dose | Erythematous plaque | Not reported | No | No | Topical methylprednisolone-aceponate 0.1% cream | Resolution after 3 days |
| Gregoriou et al. [4] | 53 | Female | No | Moderna mRNA-1273 | 11 days after first dose | Erythematous plaque | 8 cm | No | No | Topical mometasone furoate 0.1% cream | Resolution after 5 days |
| Blumenthal et al. [1] | 37 | Female | No | Moderna mRNA-1273 | 8 days after first dose | Annular papules, pruritus | 9 cm | No | No | No | |
| Blumenthal et al. [2] | 61 | Female | Contrast allergy | Moderna mRNA-1273 | 8 days after first dose | Edematous plaque, pruritus, warmth | 10 cm | No | No | Topical clobetasol propionate 0.05% cream | |
| Blumenthal et al. [3] | 45 | Female | Rhinits, penicillin allergy | Moderna mRNA-1273 | 8 days after first dose | Edematous plaque, pruritus, pain | 14 cm | Fatigue, headache, myalgias, chills | No | Topical hydrocortisone 1% cream, diphenhydramine 25 mg | |
| Blumenthal et al. [4] | 31 | Female | Urticaria, rhinits | Moderna mRNA-1273 | 8 days after first dose | Erythematous plaque, pruritus | 5 cm | Lymphadenopathy | No | Topical triamcinolone 0.1% cream, diclofenac 1% topical gel, cetirizine 10 mg | |
| Blumenthal et al. [5] | 40 | Female | No | Moderna mRNA-1273 | 4 days after first dose | Erythematous plaque, pruritus, pain | 13 cm | Papules on the palm and fingers. Headache, fatigue, fever | No | No | |
| Blumenthal et al. [6] | 43 | Male | No | Moderna mRNA-1273 | 9 days after first dose | Erythematous plaque, pruritus, pain, warmth | 12.5 cm | Urticarial plaques on the elbows | No | Diphenhydramine 25 mg, famotidine 20 mg | |
| Blumenthal et al. [7] | 38 | Female | Wasp allergy | Moderna mRNA-1273 | 9 days after first dose | Erythematous plaque, pain | 7 cm | No | No | Loratadine 10 mg | |
| Blumenthal et al. [8] | 49 | Female | Idiopathic urticaria | Moderna mRNA-1273 | 8 days after first dose | Indurated plaque, pruritus, pain, burning, warmth | 4 cm | No | No | No | |
| Blumenthal et al. [9] | 41 | Female | No | Moderna mRNA-1273 | 10 days after first dose | Indurated plaque, pruritus, warmth | 7.5 cm | Fatigue | No | No | |
| Blumenthal et al. [10] | 47 | Male | Almond allergy, rhinits | Moderna mRNA-1273 | 11 days after first dose | Erythematous plaque, pain | 7 cm | Fatigue, myalgias | No | No | |
| Blumenthal et al. [11] | 52 | Female | Angioedema, | Moderna mRNA-1273 | 8 days after first dose | Erythematous plaque, swelling, pain | 19.5 cm | Tachycardia, hypertension | No | No | |
| Blumenthal et al. [12] | 46 | Female | Penicillin allergy | Moderna mRNA-1273 | 9 days after first dose | Erythematous plaque, pruritus | 7 cm | Headache | No | No | |
| Lindgren et al. [1] | 60 | Female | No | Moderna mRNA-1273 | 6 days after first dose | Erythematous papules with pruritus, swollen, pain | Not reported | No | No | Topical clobetasol 0.05% cream | Resolution after 1 day |
| Lindgren et al. [2] | 44 | Female | No | Cominarty (Pfizer/BioNTech) | 7 days after first dose | Erythema, pain, pruritus, sweeling | Not reported | Fever, chills, headache, myalgias | No | Topical triamcinolone 0.1% cream | Resolution after 2 days |
| Lindgren et al. [3] | 33 | Female | No | Moderna mRNA-1273 | 7 days after first dose | Erythema, pain, pruritus, swelling | Not reported | No | No | Topical hydrocortisone 1% cream | Resolution after 4 days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fasano, G.; Bennardo, L.; Ruffolo, S.; Passante, M.; Ambrosio, A.G.; Napolitano, M.; Provenzano, E.; Nisticò, S.P.; Patruno, C. Erythema Migrans-like COVID Vaccine Arm: A Literature Review. J. Clin. Med. 2022, 11, 797. https://doi.org/10.3390/jcm11030797
Fasano G, Bennardo L, Ruffolo S, Passante M, Ambrosio AG, Napolitano M, Provenzano E, Nisticò SP, Patruno C. Erythema Migrans-like COVID Vaccine Arm: A Literature Review. Journal of Clinical Medicine. 2022; 11(3):797. https://doi.org/10.3390/jcm11030797
Chicago/Turabian StyleFasano, Gaia, Luigi Bennardo, Silvana Ruffolo, Maria Passante, Azzurra Gaia Ambrosio, Maddalena Napolitano, Eugenio Provenzano, Steven Paul Nisticò, and Cataldo Patruno. 2022. "Erythema Migrans-like COVID Vaccine Arm: A Literature Review" Journal of Clinical Medicine 11, no. 3: 797. https://doi.org/10.3390/jcm11030797