
Autologous Fat Plus Platelet-Rich Plasma versus Autologous Fat Alone on Sulcus Vocalis

 ,
,
Abstract
:1. Introduction
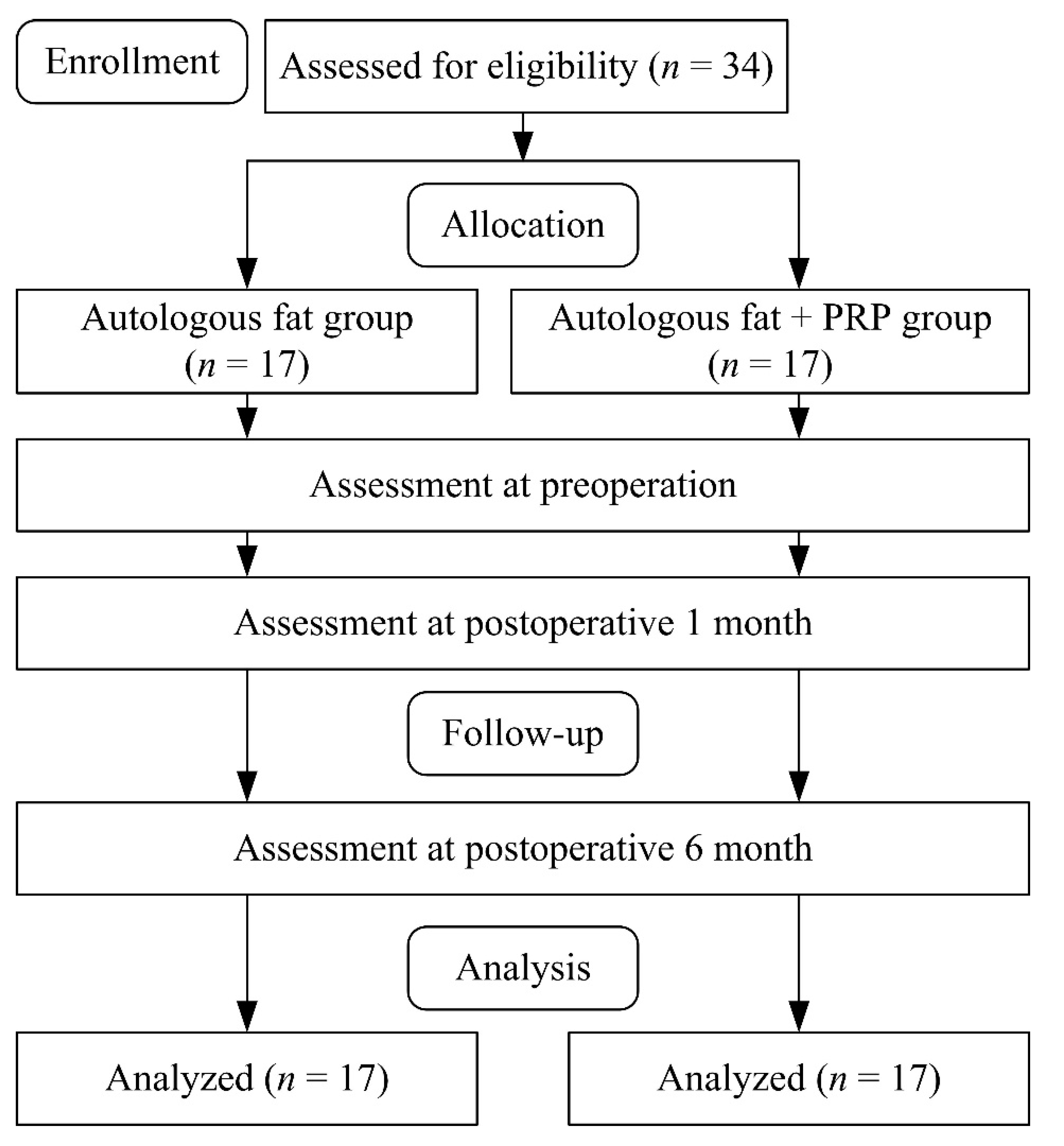
2. Materials and Methods
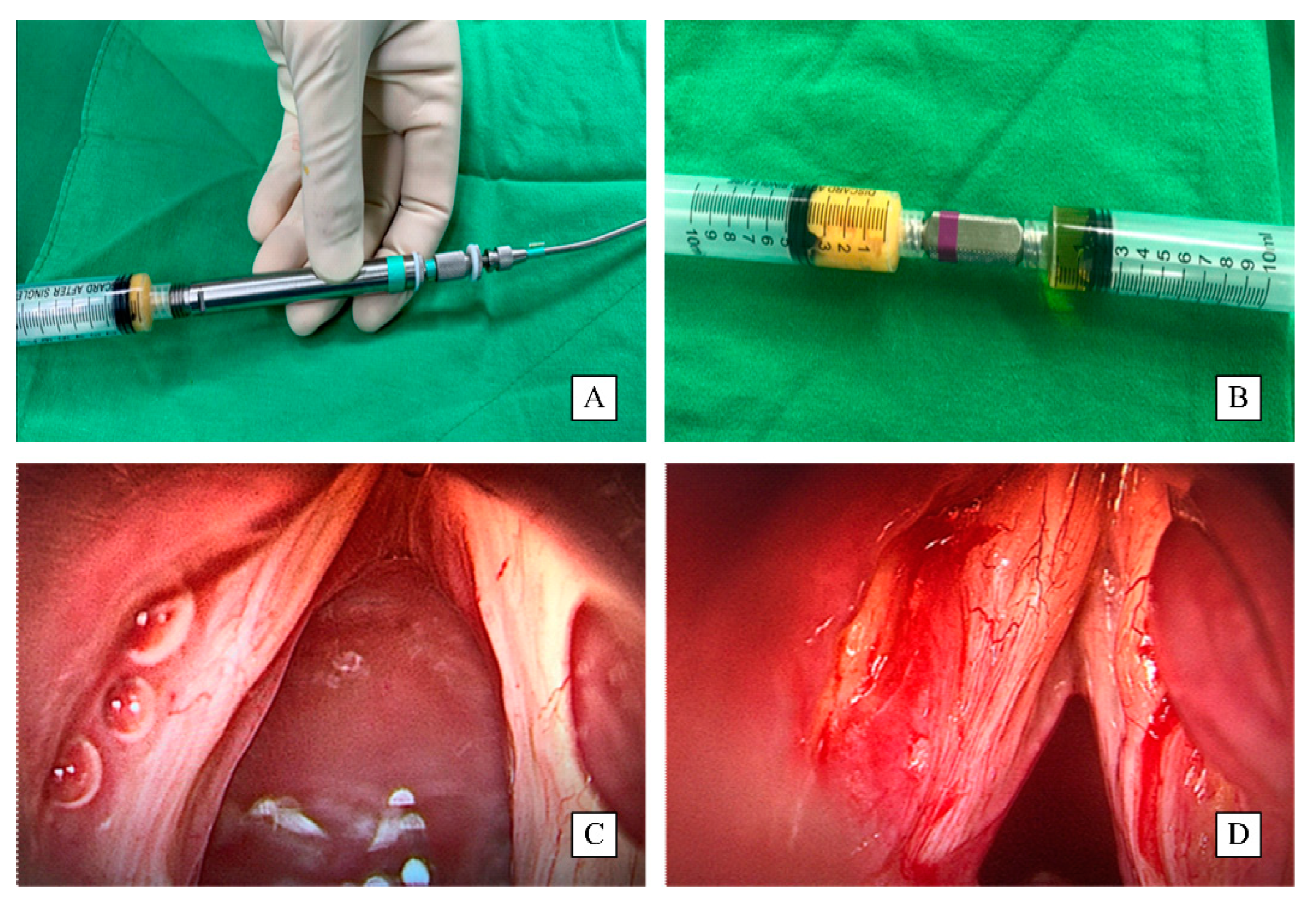
2.1. Procedure
2.2. Assessments
2.2.1. Videostroboscopic Examination
2.2.2. Acoustic Analysis
2.2.3. Grade, Roughness, Breathiness, Asthenia, and Strain Scale (GRBAS)
2.2.4. Voice Handicap Index
2.3. Statistical Analysis
3. Results
3.1. Outcomes of Fat Alone Group versus Fat Plus PRP Group
3.2. Acoustic Characteristic of Fat-Only Group versus Fat Plus PRP Group by Gender
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ford, C.N.; Inagi, K.; Khidr, A.; Bless, D.M.; Gilchrist, K.W. Sulcus vocalis: A rational analytical approach to diagnosis and management. Ann. Otol. Rhinol. Laryngol. 1996, 105, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Miaśkiewicz, B.; Szkiełkowska, A.; Gos, E.; Panasiewicz, A.; Włodarczyk, E.; Skarżyński, P.H. Pathological sulcus vocalis: Treatment approaches and voice outcomes in 36 patients. Eur. Arch. Otorhinolaryngol. 2018, 275, 2763–2771. [Google Scholar] [CrossRef] [PubMed]
- Lindestad, P.A.; Hertegard, S. Spindle-shaped glottal insufficiency with and without sulcus vo-calis: A retrospective study. Ann. Otol. Rhinol. Laryngol. 1994, 103, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Giovanni, A.; Chanteret, C.; Lagier, A. Sulcus vocalis: A review. Eur. Arch. Otorhinolaryngol. 2007, 264, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Watson, G.J.; Jones, P.H. Videographic documentation of an open cyst converting into a sulcus vocalis. J. Voice 2011, 25, e221–e222. [Google Scholar] [CrossRef] [PubMed]
- Van den Broek, E.; Heijnen, B.J.; Hendriksma, M.; Langeveld, A.; van Benthem, P.; Sjögren, E.V. Bilateral trial vocal fold injection with hyaluronic acid in patients with vocal fold atrophy with or without sulcus. Eur. Arch. Otorhinolaryngol. 2019, 276, 1413–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lisi, C.; Hawkshaw, M.J.; Sataloff, R.T. Viscosity of materials for laryngeal injection: A review of current knowledge and clinical implications. J. Voice 2013, 27, 119–123. [Google Scholar] [CrossRef]
- Shindo, M.L.; Zaretsky, L.S.; Rice, D.H. Autologous fat injection for unilateral vocal fold paraly-sis. Ann. Otol. Rhinol. Laryngol. 1996, 105, 602–606. [Google Scholar] [CrossRef]
- Özgürsoy, S.K.; Tunçkaşık, F.; Tunçkaşık, M.E.; Akıncıoğlu, E.; Doğan, H.; Beriat, G.K. Histo-pathologic evaluation of hyaluronic acid and plasma-rich platelet injection into rabbit vocal cords: An experimental study. Turk. Arch. Otorhinolaryngol. 2018, 56, 30–35. [Google Scholar] [CrossRef]
- Sakalys, D.; Rokicki, J.P.; Januzis, G.; Kubilius, R. Plasma rich in growth factors injection effec-tiveness for myofascial pain treatment in masticatory muscles. Randomised controlled trial. J. Oral Rehabil. 2020, 47, 796–801. [Google Scholar] [CrossRef]
- Chang, W.D.; Chen, S.H.; Tsai, M.H.; Tsou, Y.A. Autologous fat injection laryngoplasty for unilateral vocal fold paralysis. J. Clin. Med. 2021, 10, 5034. [Google Scholar] [CrossRef] [PubMed]
- Stavrakas, M.; Karkos, P.D.; Markou, K.; Grigoriadis, N. Platelet-rich plasma in otolaryngology. J. Laryngol. Otol. 2016, 130, 1098–1102. [Google Scholar] [CrossRef] [PubMed]
- Poburka, B.J.; Patel, R.R.; Bless, D.M. Voice-vibratory assessment with laryngeal imaging (VALI) form: Reliability of rating stroboscopy and high-speed videoendoscopy. J. Voice 2017, 31, 513.e1–513.e14. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.R.; Awan, S.N.; Barkmeier-Kraemer, J.; Courey, M.; Deliyski, D.; Eadie, T.; Paul, D.; Švec, J.G.; Hillman, R. Recommended protocols for instrumental assessment of voice: American speech-language-hearing association expert panel to develop a protocol for instrumental assessment of vocal function. Am. J. Speech Lang. Pathol. 2018, 27, 887–905. [Google Scholar] [CrossRef]
- Franca, M.C. Acoustic comparison of vowel sounds among adult females. J. Voice 2012, 26, 671. [Google Scholar] [CrossRef] [PubMed]
- Akil, F.; Yollu, U.; Ozturk, O.; Yener, M. Differences of the voice parameters between the population of different hearing tresholds: Findings by using the multi-dimensional voice program. Clin. Exp. Otorhinolaryngol. 2017, 10, 278–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, Y.S.; Chang, J.W.; Yang, S.M.; Wu, H.W.; Cho, M.H.; Kim, C.H. Persistent dysphonia after laryngomicrosurgery for benign vocal fold disease. Clin. Exp. Otorhinolaryngol. 2013, 6, 166–170. [Google Scholar] [CrossRef]
- Lam, P.K.; Chan, K.M.; Ho, W.K.; Kwong, E.; Yiu, E.M.; Wei, W.I. Cross-cultural adaptation and validation of the Chinese Voice Handicap Index-10. Laryngoscope 2006, 116, 1192–1198. [Google Scholar] [CrossRef]
- Behlau, M.; Madazio, G.; Moreti, F.; Oliveira, G.; dos Santos, L.d.M.A.; Paulinelli, B.R.; Couto Junior Ede, B. Efficiency and cutoff values of self-assessment instruments on the impact of a voice problem. J. Voice 2016, 30, e9–e506. [Google Scholar] [CrossRef]
- Rosen, C.A.; Lee, A.S.; Osborne, J.; Zullo, T.; Murry, T. Development and validation of the voice handicap index-10. Laryngoscope 2004, 114, 1549–1556. [Google Scholar] [CrossRef]
- Tafiadis, D.; Helidoni, M.E.; Chronopoulos, S.K.; Kosma, E.I.; Alexandropoulou, A.; Velegrakis, S.; Konitsiotis, S.; Ziavra, N. ROC analysis cut-off points of hellenic voice handicap index for neurogenic voice disorders patients: An exploratory study. J. Voice, 2020; in press. [Google Scholar] [CrossRef] [PubMed]
- Tafiadis, D.; Helidoni, M.E.; Chronopoulos, S.K.; Kosma, E.I.; Ziavra, N.; Velegrakis, G.A. Cross-cultural adaptation and validation of the Greek voice handicap index-10 (GVHI-10) with additional receiver operating characteristic analysis. J. Voice 2020, 34, 304.e1–304.e8. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.Y.; Kim, J.; Choi, S.H.; Kim, K.M.; Kim, Y.H.; Kim, H.S.; Choi, H.S. Sulcus configura-tions of vocal folds during phonation. Acta Otolaryngol. 2009, 129, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Soni, R.S.; Dailey, S.H. Sulcus Vocalis. Otolaryngol. Clin. N. Am. 2019, 52, 735–743. [Google Scholar] [CrossRef]
- Woo, P. 4K video-laryngoscopy and video—Stroboscopy: Preliminary findings. Ann. Otol. Rhinol. Laryngol. 2016, 125, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Woo, P.; Murry, T. Short-term voice improvement after repeated office-based platelet-rich plasma PRP injection in patients with vocal fold scar, sulcus, and atrophy. J. Voice 2021. Available online: https://doi.org/10.1016/j.jvoice.2021.02.022 (accessed on 18 March 2021). [CrossRef]
- Hansen, J.K.; Thibeault, S.L. Current understanding and review of the literature: Vocal fold scarring. J. Voice 2006, 20, 110–120. [Google Scholar] [CrossRef]
- Mallur, P.S.; Gartner-Schmidt, J.; Rosen, C.A. Voice outcomes following the gray minithyrotomy. Ann. Otol. Rhinol. Laryngol. 2012, 121, 490–496. [Google Scholar] [CrossRef]
- Sataloff, R.T.; Spiegel, J.R.; Hawkshaw, M.; Rosen, D.C.; Heuer, R.J. Autologous fat implanta-tion for vocal fold scar: A preliminary report. J. Voice 1997, 11, 238–246. [Google Scholar] [CrossRef]
- Pontes, P.; Behlau, M. Treatment of sulcus vocalis: Auditory perceptual and acoustical analysis of the slicing mucosa surgical technique. J. Voice 1993, 7, 365–376. [Google Scholar] [CrossRef]
- Courey, M.S. Injection laryngoplasty. Otolaryngol. Clin. N. Am. 2004, 37, 121–138. [Google Scholar] [CrossRef] [PubMed]
- Tamura, E.; Fukuda, H.; Tabata, Y. Intracordal injection technique: Materials and injection site. Tokai. J. Exp. Clin. Med. 2008, 33, 119–123. [Google Scholar] [PubMed]
- Lasso, J.M.; Poletti, D.; Scola, B.; Gómez-Vilda, P.; García-Martín, A.I.; Fernández-Santos, M.E. Injection laryngoplasty using autologous fat enriched with adipose-derived regenerative stem cells: A safe therapeutic option for the functional reconstruction of the glottal gap after unilateral vocal fold paralysis. Stem Cells Int. 2018, 2018, 8917913. [Google Scholar] [CrossRef] [Green Version]
- Butterwick, K.J.; Nootheti, P.K.; Hsu, J.W.; Goldman, M.P. Autologous fat transfer: An in-depth look at varying concepts and techniques. Facial Plast. Surg. Clin. N. Am. 2007, 15, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Kruschewsky, L.d.S.; de Mello-Filho, F.V.; dos Santos, A.C.; Rosen, C.A. Autologous fat graft absorption in unilateral paralyzed canine vocal folds. Laryngoscope 2007, 117, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Tamura, E.; Tabata, Y.; Yamada, C.; Okada, S.; Iida, M. Autologous fat augmentation of the vocal fold with basic fibroblast growth factor: Computed tomographic assessment of fat tissue survival after augmentation. Acta. Otolaryngol. 2015, 135, 1163–1167. [Google Scholar] [CrossRef] [PubMed]
- Knop, E.; Paula, L.E.; Fuller, R. Platelet-rich plasma for osteoarthritis treatment. Rev. Bras. Reumatol. Engl. Ed. 2016, 56, 152–164. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Gou, L.; Zhang, P.; Li, H.; Qiu, S. Platelet-rich plasma and regenerative dentistry. Aust. Dent. J. 2020, 65, 131–142. [Google Scholar] [CrossRef]
- Peng, G.L. Platelet-rich plasma for skin rejuvenation: Facts, fiction, and pearls for practice. Facial Plast. Surg. Clin. N. Am. 2019, 27, 405–411. [Google Scholar] [CrossRef]
- Elghblawi, E. Platelet-rich plasma, the ultimate secret for youthful skin elixir and hair growth triggering. J. Cosmet. Dermatol. 2018, 17, 423–430. [Google Scholar] [CrossRef]
- Filardo, G.; Di Matteo, B.; Kon, E.; Merli, G.; Marcacci, M. Platelet-rich plasma in tendon-related disorders: Results and indications. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1984–1999. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Fernández-de-Retana, S.; Alkhraisat, M.H. Platelet rich plasma in oral and maxillofacial surgery from the perspective of composition. Platelets 2021, 32, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Tandulwadkar, S.R.; Naralkar, M.V.; Surana, A.D.; Selvakarthick, M.; Kharat, A.H. Autologous intrauterine platelet-rich plasma instillation for suboptimal endometrium in frozen embryo transfer cycles: A Pilot Study. J. Hum. Reprod. Sci. 2017, 10, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Houdek, M.T.; Wyles, C.C.; Stalboerger, P.G.; Terzic, A.; Behfar, A.; Moran, S.L. Collagen and fractionated platelet-rich plasma scaffold for dermal regeneration. Plast. Reconstr. Surg. 2016, 137, 1498–1506. [Google Scholar] [CrossRef] [PubMed]
- Cobden, S.B.; Oztürk, K.; Duman, S.; Esen, H.; Aktan, T.M.; Avunduk, M.C.; Elsurer, C. Treatment of acute vocal fold injury with platelet-rich plasma. J. Voice 2016, 30, 731–735. [Google Scholar] [CrossRef] [PubMed]
- Seria, E.; Galea, G.; Borg, J.; Schembri, K.; Grech, G.; Tagliaferro, S.S.; Felice, A. Novel leukocyte-depleted platelet-rich plasma-based skin equivalent as an in vitro model of chronic wounds: A preliminary study. BMC Mol. Cell Biol. 2021, 22, 28. [Google Scholar] [CrossRef] [PubMed]
- Smith, O.J.; Jell, G.; Mosahebi, A. The use of fat grafting and platelet-rich plasma for wound healing: A review of the current evidence. Int. Wound J. 2019, 16, 275–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, S.; Yi, C.; Pu, L.L.Q. An overview of principles and new techniques for facial fat grafting. Clin. Plast Surg. 2020, 47, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.; Qiu, L.; Su, Y.; Zheng, H.; Yi, C. Platelet-rich plasma and platelet-rich fibrin enhance the outcomes of fat grafting: A comparative study. Plast. Reconstr. Surg. 2019, 143, 1201–1212. [Google Scholar] [CrossRef] [PubMed]
- Zamani, M.; Yaghoubi, Y.; Movassaghpour, A.; Shakouri, K.; Mehdizadeh, A.; Pishgahi, A.; Yousefi, M. Novel therapeutic approaches in utilizing platelet lysate in regenerative medicine: Are we ready for clinical use? J. Cell Physiol. 2019, 234, 17172–17186. [Google Scholar] [CrossRef]
- Lei, X.; Liu, H.; Pang, M.; Zheng, Z.; Tan, X.; Cheng, B. Effects of platelet-rich plasma on fat and nanofat survival: An experimental study on mice. Aesthet. Plast. Surg. 2019, 43, 1085–1094. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Gan, D.; Wang, G.; Ru, Y.; Huang, C.; Lin, J.; Zhang, L.; Meng, Z.; Zhu, S. Associations of platelet indices with body fat mass and fat distribution. Obesity 2018, 26, 1637–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, O.J.; Leigh, R.; Kanapathy, M.; Macneal, P.; Jell, G.; Hachach-Haram, N.; Mann, H.; Mosahebi, A. Fat grafting and platelet-rich plasma for the treatment of diabetic foot ulcers: A feasibility-randomised controlled trial. Int. Wound J. 2020, 17, 1578–1594. [Google Scholar] [CrossRef]
- O’Connell, B.; Wragg, N.M.; Wilson, S.L. The use of PRP injections in the management of knee osteoarthritis. Cell Tissue Res. 2019, 376, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, Y.; Saita, Y.; Takaku, T.; Yokomizo, T.; Nishio, H.; Ikeda, H.; Takazawa, Y.; Nagao, M.; Kaneko, K.; Komatsu, N. Platelet-rich plasma (PRP) accelerates murine patellar tendon healing through enhancement of angiogenesis and collagen synthesis. J. Exp. Orthop. 2020, 7, 49. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Zhai, Z.; Lu, H.; Jin, X.; Yang, X.; Qi, Z. Platelet-rich fibrin improves fat graft survival possibly by promoting angiogenesis and adipogenesis, inhibiting apoptosis, and regulat-ing collagen production. Aesthet. Surg. J. 2020, 40, 530–545. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Park, E.S.; Kim, T.H. Rejuvenation using platelet-rich plasma and lipofilling for vaginal atrophy and lichen sclerosus. J. Menopausal Med. 2017, 23, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Guler, S.; Akcali, O.; Sen, B.; Micili, S.C.; Sanli, N.K.; Cankaya, D. Effect of platelet-rich plasma, fat pad and dural matrix in preventing epidural fibrosis. Acta. Ortop. Bras. 2020, 28, 31–35. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Autologous Fat Injection Group (n = 17) | Autologous Fat plus PRP Group (n = 17) | p Value | |
|---|---|---|---|
| Age (years) | 57.21 ± 10.68 | 60.12 ± 9.89 | 0.41 |
| Weight (kg) | 75.67 ± 15.78 | 76.33 ± 18.21 | 0.91 |
| Height (cm) | 171.34 ± 10.56 | 169.78 ± 11.84 | 0.68 |
| Sex (no., %) | |||
| Male | 7 (41.17%) | 8 (47.06%) | 0.11 |
| Female | 10 (58.82%) | 9 (52.95%) | |
| Side, (no., %) | |||
| Left | 4 (23.53%) | 3 (17.65%) | 0.81 |
| Right | 2 (11.76%) | 2 (11.76%) | |
| Bilateral | 11 (64.71%) | 12 (70.59%) |
| Autologous Fat Injection Group (n = 17) | Autologous Fat plus PRP Group (n = 17) | |||||
|---|---|---|---|---|---|---|
| Preoperative | Postoperative (1 Month) | Postoperative (6 Months) | Preoperative | Postoperative (1 Month) | Postoperative (6 Months) | |
| VHI-10 | 26.92 ± 7.76 c | 21.88 ± 7.36 a | 16.69 ± 5.35 b | 28.13 ± 10.81 c | 17.12 ± 6.41 a,d | 12.47 ± 5.21 b |
| GRBAS | ||||||
| G | 2.54 ± 0.52 c | 1.41 ± 0.63 a | 0.78 ± 0.63 b | 2.01 ± 0.79 c | 1.11 ± 0.59 a | 0.69 ± 0.42 b |
| R | 2.16 ± 0.76 c | 1.32 ± 0.43 a | 0.67 ± 0.43 b | 1.76 ± 0.83 c | 0.83 ± 0.21 a | 0.63 ± 0.22 b |
| B | 1.78 ± 0.85 | 1.55 ± 0.67 | 0.75 ± 0.98 | 1.65 ± 1.01 | 0.79 ± 0.68 a | 0.80 ± 0.52 |
| A | 1.38 ± 0.97 | 1.28 ± 0.87 | 0.66 ± 1.32 | 1.29 ± 1.10 | 1.13 ± 0.83 | 0.98 ± 0.82 |
| S | 1.15 ± 0.74 | 1.14 ± 0.83 | 1.10 ± 0.92 | 1.47 ± 0.94 | 1.09 ± 0.89 | 1.01 ± 0.61 |
| Total | 7.52 ± 2.61 c | 5.68 ± 2.45 a | 3.38 ± 1.98 b | 6.86 ± 3.79 c | 4.45 ± 2.53 a | 3.11 ± 1.01 b |
| Stroboscopy examination | ||||||
| Anterior–posterior | 2.29 ± 0.38 | 1.08 ± 0.45 a | 2.02 ± 1.98 | 2.32 ± 0.42 c | 0.98 ± 0.55 a | 1.03 ± 0.47 d |
| Left–right | 2.49 ± 0.45 | 1.06 ± 0.34 a | 1.98 ± 1.87 | 2.44 ± 0.52 c | 1.02 ± 0.45 a | 1.12 ± 0.32 d |
| Group | Time | Group × Time | |||||||
|---|---|---|---|---|---|---|---|---|---|
| F | p | η2 | F | p | η2 | F | p | η2 | |
| MPT | 0.77 | 0.39 | 0.04 | 17.21 | 0.02 * | 0.69 | 0.65 | 0.53 | 0.08 |
| High frequency (Hz) | 0.05 | 0.90 | 0.04 | 2.86 | 0.09 | 0.27 | 0.18 | 0.83 | 0.02 |
| Low frequency (Hz) | 0.03 | 0.81 | 0.01 | 3.23 | 0.07 | 0.30 | 1.29 | 0.31 | 0.14 |
| NHR | 10.72 | 0.01 * | 0.40 | 9.65 | 0.01 * | 0.56 | 0.39 | 0.68 | 0.05 |
| VTI | 0.05 | 0.81 | 0.02 | 4.01 | 0.04 * | 0.34 | 0.69 | 0.51 | 0.08 |
| SPI | 0.06 | 0.78 | 0.01 | 2.87 | 0.08 | 0.26 | 0.11 | 0.90 | 0.01 |
| Jitter (%) | 0.81 | 0.37 | 0.04 | 59.85 | 0.01 * | 0.87 | 7.97 | 0.01 * | 0.51 |
| Shimmer (%) | 2.72 | 0.11 | 0.14 | 58.12 | 0.01 * | 0.78 | 8.05 | 0.01 * | 0.49 |
| Autologous Fat Injection Group (n = 17) | Autologous Fat plus PRP Group (n = 17) | |||||
|---|---|---|---|---|---|---|
| Preoperative | Postoperative (1 Month) | Postoperative (6 Months) | Preoperative | Postoperative (1 Month) | Postoperative (6 Months) | |
| MPT | 6.79 ± 2.21 | 8.32 ± 2.14 a | 8.89 ± 6.98 | 7.12 ± 2.24 c | 8.65 ± 2.02 a | 10.76 ± 3.56 b |
| High frequency (Hz) | 236.74 ± 78.32 | 247.64 ± 81.11 | 235.73 ± 77.47 | 240.12 ± 66.89 | 249.32 ± 92.33 | 233.43 ± 78.56 |
| Low frequency (Hz) | 150.21 ± 55.63 | 143.13 ± 63.84 | 138.26 ± 65.35 | 141.36 ± 69.83 | 139.98 ± 80.47 | 140.77 ± 76.88 |
| NHR | 0.35 ± 0.32 | 0.29 ± 0.17 | 0.20 ± 0.06 b | 0.25 ± 0.21 c | 0.14 ± 0.16 a,d | 0.04 ± 0.01 b,d |
| VTI | 0.12 ± 0.11 | 0.07 ± 0.08 | 0.08 ± 0.12 | 0.09 ± 0.18 | 0.07 ± 0.13 | 0.08 ± 0.11 |
| SPI | 24.33 ± 13.34 | 23.65 ± 12.20 | 22.66 ± 13.09 | 23.67 ± 12.59 | 22.45 ± 13.63 | 21.98 ± 12.56 |
| Jitter (%) | 5.82 ± 1.98 c | 5.51 ± 2.01 | 4.05 ± 1.10 b | 6.77 ± 1.66 c | 4.34 ± 1.38 a,d | 3.02 ± 1.61 b,d |
| Shimmer (%) | 12.72 ± 3.12 c | 12.45 ± 3.32 | 10.21 ± 2.67 b | 13.86 ± 2.97 c | 10.01 ± 3.22 a,d | 7.18 ± 2.35 b,d |
| Autologous Fat Injection Male (n = 7) | Autologous Fat plus PRP Group Male (n = 8) | |||||
|---|---|---|---|---|---|---|
| Preoperative | Postoperative (1 Month) | Postoperative (6 Months) | Preoperative | Postoperative (1 Month) | Postoperative (6 Months) | |
| High frequency (Hz) | 160.57 ± 44.84 | 169.29 ± 47.74 | 170.71 ± 46.14 | 188.88 ± 37.28 | 169.63 ± 45.21 | 168.75 ± 48.83 |
| Low frequency (Hz) | 115.43 ± 21.90 | 108.43 ± 44.58 | 95.01 ± 32.02 | 93.13 ± 19.07 | 87.25 ± 15.04 | 90.02 ± 14.78 |
| NHR | 0.50 ± 0.39 | 0.35 ± 0.19 | 0.22 ± 0.07 | 0.26 ± 0.17 | 0.09 ± 0.04 a | 0.03 ± 0.02 b |
| Jitter (%) | 6.57 ± 1.51 | 6.29 ± 1.80 | 4.57 ± 1.13 | 7.13 ± 1.83 | 4.38 ± 1.30 a | 3.34 ± 2.24 |
| Shimmer (%) | 13.02 ± 2.94 | 12.64 ± 2.21 | 10.20 ± 2.52 | 15.13 ± 2.10 | 11.70 ± 2.21 | 8.16 ± 2.12 |
| Autologous Fat Injection Female (n = 10) | Autologous Fat plus PRP Group Female (n = 9) | |||||
|---|---|---|---|---|---|---|
| Preoperative | Postoperative (1 Month) | Postoperative (6 Months) | Preoperative | Postoperative (1 Month) | Postoperative (6 Months) | |
| High frequency (Hz) | 289.70 ± 42.91 | 301.61 ± 48.75 | 281.12 ± 60.20 | 286.56 ± 50.43 | 319.11 ± 60.62 | 291.02 ± 48.25 |
| Low frequency (Hz) | 174.50 ± 59.87 | 168.20 ± 64.41 | 169.51 ± 66.75 | 184.33 ± 69.53 | 186.04 ± 87.60 | 185.89 ± 81.83 |
| NHR | 0.25 ± 0.21 | 0.24 ± 0.16 | 0.19 ± 0.07 | 0.25 ± 0.25 | 0.20 ± 0.21 | 0.04 ± 0.02 b |
| Jitter (%) | 5.30 ± 2.06 | 5.04 ± 2.05 | 3.72 ± 0.95 | 6.44 ± 1.59 | 4.26 ± 1.51 | 2.76 ± 0.98 b |
| Shimmer (%) | 12.52 ± 3.50 | 12.30 ± 4.04 | 10.21 ± 3.01 | 12.78 ± 3.19 | 8.56 ± 3.40 a | 6.33 ± 2.24 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsou, Y.-A.; Tien, V.H.-C.; Chen, S.-H.; Shih, L.-C.; Lin, T.-C.; Chiu, C.-J.; Chang, W.-D. Autologous Fat Plus Platelet-Rich Plasma versus Autologous Fat Alone on Sulcus Vocalis. J. Clin. Med. 2022, 11, 725. https://doi.org/10.3390/jcm11030725
Tsou Y-A, Tien VH-C, Chen S-H, Shih L-C, Lin T-C, Chiu C-J, Chang W-D. Autologous Fat Plus Platelet-Rich Plasma versus Autologous Fat Alone on Sulcus Vocalis. Journal of Clinical Medicine. 2022; 11(3):725. https://doi.org/10.3390/jcm11030725
Chicago/Turabian StyleTsou, Yung-An, Vincent Hui-Chi Tien, Sheng-Hwa Chen, Liang-Chun Shih, Tzu-Chieh Lin, Chien-Jen Chiu, and Wen-Dien Chang. 2022. "Autologous Fat Plus Platelet-Rich Plasma versus Autologous Fat Alone on Sulcus Vocalis" Journal of Clinical Medicine 11, no. 3: 725. https://doi.org/10.3390/jcm11030725