2. Materials and Methods
2.1. Trial Design and Allocation Ratio
The 2010 consort statement for reporting pilot or feasibility studies was followed when appropriate [
9]. This study is a randomised matched-pair design pilot study. Patients undergoing EMLP were invited to participate in this study. At the time of surgery, the patient was randomised to undergo an anterior pedicled flap on the right or the left side. The contralateral side was not covered with a pedicled flap or mucosal graft. As such, the allocation ratio for this trial was 1:1 as each individual patient was their own control.
2.2. Participant Eligibility
This study was approved by Southern Adelaide Clinical Human Research Ethics Committee (SAC HREC 293.17). Informed consent was obtained from all subjects involved in the study. Inclusion criteria were any patients undergoing an EMLP. Exclusion criteria included any patient who would be unable to follow up post-operatively for routine post-operative reviews.
2.3. Setting of Participant Recruitment
Patients were recruited from a rhinology clinic at a tertiary care teaching hospital as well as from Flinders Private Hospital rhinology clinic, both of which are located in Adelaide, Australia. Patients who met the study eligibility criteria were identified as potential candidates for the study. Informed consent was obtained from patients wishing to participate in the trial.
2.4. Randomisation and Intervention
Computer-generated randomisation was determined pre-operatively to determine the side that would have a flap and the other side would not have a flap. Sealed envelopes designating which side the anteriorly-based flap should be used were prepared at the commencement of the trial. On the day of surgery, the sealed envelope would be given to the operating surgeon to open. The flap side was recorded in the patient’s data collection sheet as well as their operative report.
2.5. Surgical Technique
The surgical technique has previously been described [
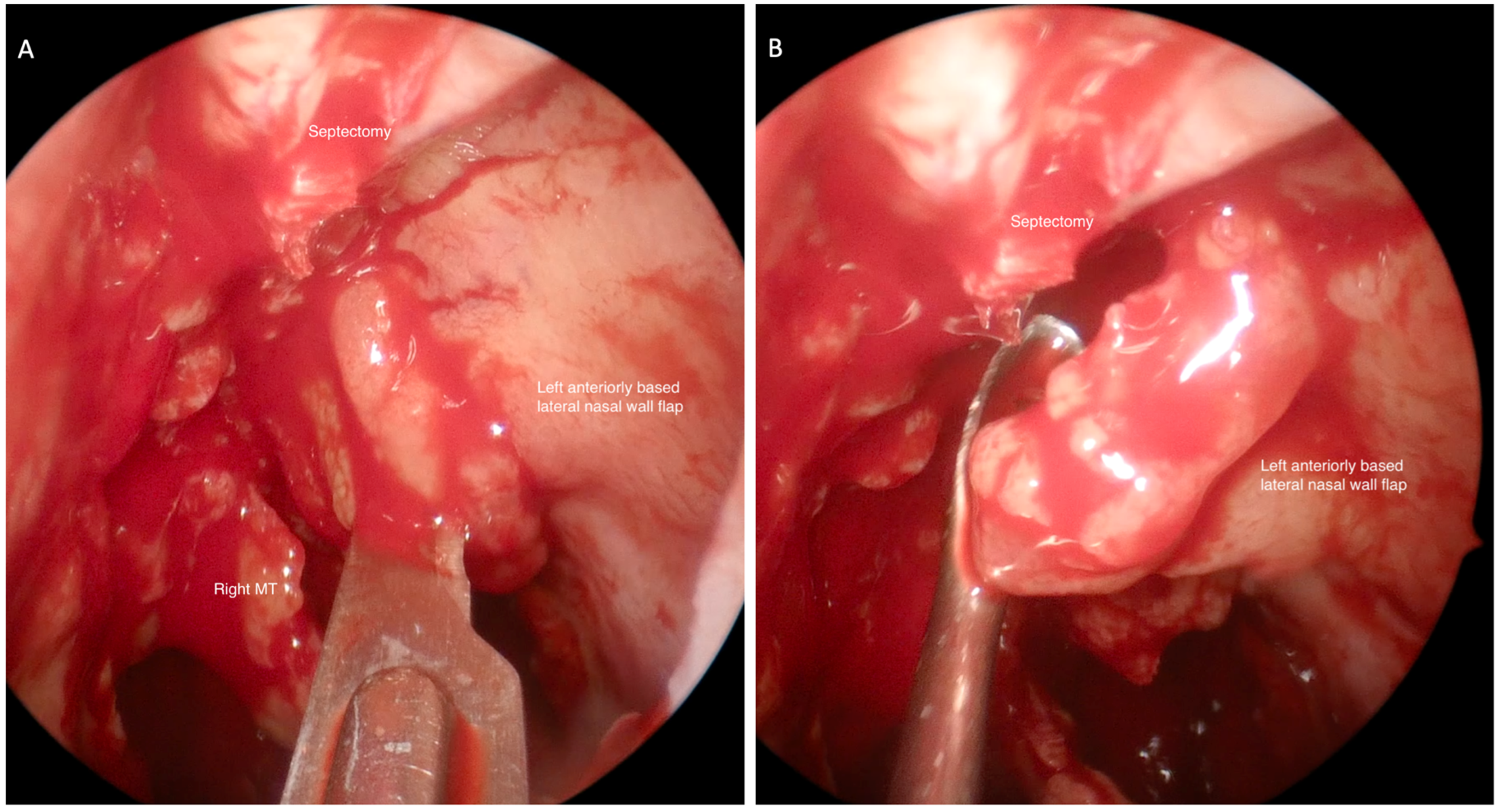
5]. After the superior septectomy is performed, a nasal flap is raised from the lateral nasal wall (
Figure 1). Once this has been raised, the nasal flap is displaced on the ipsilateral side superiorly and anteriorly toward the nasal vestibule so as to avoid injury while drilling the frontal sinus floor (
Figure 2). At the completion of the operation, the nasal flap is replaced to cover the exposed bone laterally.
2.6. Study Outcomes
Prior to surgery, baseline sinonasal outcomes were recorded, including the Sinonasal Outcome test-22 (SNOT22) [
10] and The University of Pennsylvania Smell Identification Test™ [UPSIT] [
11].
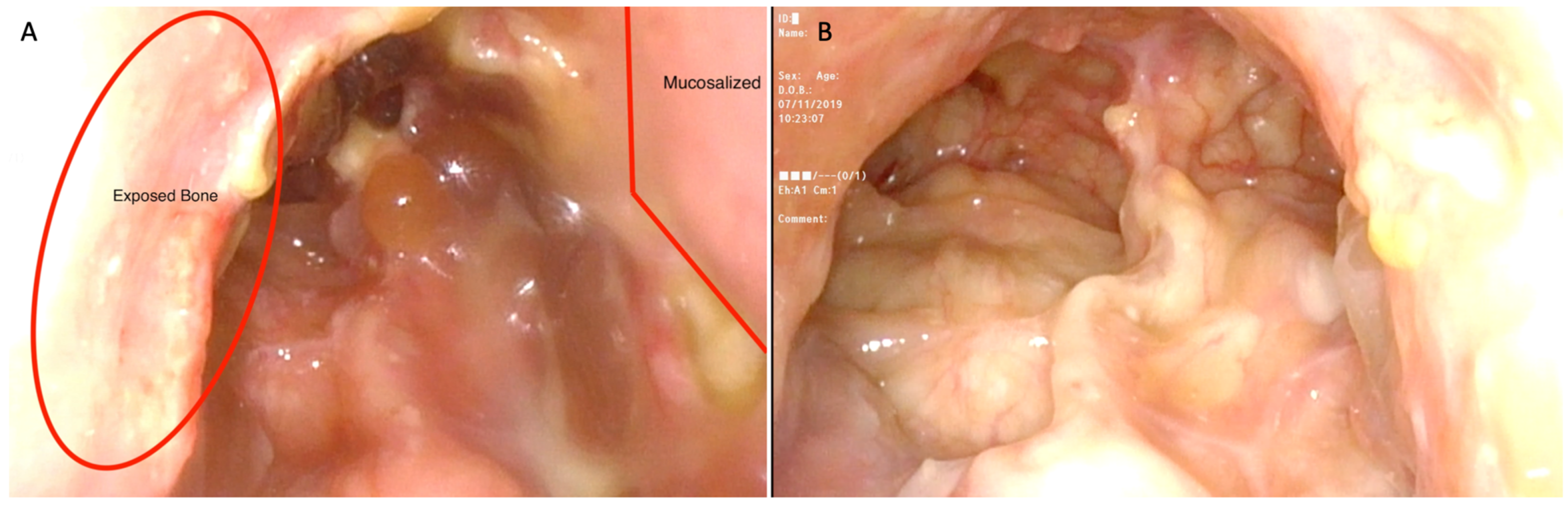
Patients were followed post-operatively every two weeks (standard clinic protocol) until adequate healing had occurred. At each post-operative appointment, the clinician endoscopically examined the patient after sufficient debridement, and recorded the endoscopic exam for subsequent analysis. Debridement was performed by the rhinology fellow or senior consultant. Based on the endoscopic examination, it was determined whether remnant bony exposure was visible in the frontal sinus neo-ostium or whether healing had occurred. Healing was defined as mucosalisation and absence of exposed bone. Differences between each side of the frontal sinus neo-ostium were recorded.
Post-operative reviews continued at two-week intervals until mucosalisation had occurred on both sides of the frontal neo-ostium. Once mucosalisation had occurred bilaterally, post-operative SNOT-22 and smell identification tests were performed. The results of these tests were compared to pre-operative scores collected on the day of their surgery.
2.7. Sample Size
This was a randomised control pilot trial to determine the effect size on time required to achieve post-operative healing and mucosalisation in the presence vs. the absence of a nasal mucosal flap. As this was a pilot trial, no sample size was calculated. The trial was concluded after 12 patients.
2.8. Statistical Analysis
Time to healing data were not normally distributed (Shapiro–Wilk); therefore, non-parametric tests were used (Related-samples Wilcoxon signed-rank test).
3. Results
3.1. Study Participants
Twelve participants were recruited for this study, five female and seven male (
Table 1). The median age was 54.8, and age ranged from 23–72 years of age. All patients had undergone previous endoscopic sinus surgery. In 10 cases, the underlying indication for surgery were patients with chronic rhinosinusitis (CRS), defined as refractory sinonasal symptoms for greater than 8–12 weeks with endoscopic or radiologic evidence of sinonasal polyposis or inflammation [
12,
13]. In addition, one patient had an expansile frontal sinus mucocele that had failed primary surgical management, and one patient with primary ciliary dyskinesia had multiple previous sinonasal surgeries.
3.2. Recruitment
The first participant was recruited in September 2018, with the last patient recruited in February 2020. The randomisation allocation was six patients with right-sided flaps and six patients with left-sided flaps.
3.3. Result Outcomes
The median healing time to mucosalisation of exposed bone was not statistically different between the non-flap side vs. flap side (4.0, range 2.0–6.0 vs. 4.0, range 2.0–6.0) (
p > 0.05;
Table 1).
Eleven of the twelve patients completed both the pre-operative and post-operative SNOT-22 questionnaire. One patient did not complete the pre-operative SNOT-22 questionnaire. The average pre-operative SNOT-22 score was 50.4 (range 18–81). The post-operative SNOT-22 score was recorded when healing of the frontal neo-ostium had completed. The average post-operative SNOT22 score was 23.9 (range 2–72). Overall, there was a decrease in SNOT-22 scores for our patient population on average by −24.4 points (range −75 to +9, p > 0.5). Three patients reported a similar or slight increase in sinonasal symptoms post-operatively.
Smell testing was completed pre-operatively and again post-operatively when the neostium achieved healing on both sides; 8 out of the 12 patients completed both pre-operative and post-operative smell tests. Four patients failed to answer the pre-operative smell test as instructed or declined to complete the post-operative smell test. The average pre-operative UPSIT score was 18.7 (range 8–30). The average post-operative UPSIT score was 28.1 (range 17–30). Overall, an increase in post-operative UPSIT score was observed, with an average increase of 6.6 points (range −13 to +27, p > 0.5). Two patients had a decreased post-operative UPSIT score.
Post-hoc chart review demonstrated that patients were followed for an average of 17.8 weeks after surgery (range 6–37 weeks). Of the 12 patients who underwent EMLP, 3 had stenosis develop within 6 months of surgery and required revision EMLP. In all three cases, stenosis was demonstrated bilaterally. There was no difference appreciated between the flap or non-flap side. No other significant complications were recorded in the remainder of our patient population.
4. Discussion
Restenosis of the frontal sinus neo-ostium is the most common aetiology for surgical failure in patients undergoing EMLP [
14]. While other studies have illustrated that the use of nasal mucosal flaps and free mucosal grafts improved surgical outcomes, our pilot trial did not demonstrate a significant difference in healing time post-operatively between patients with a mucosal flap and those without [
1,
5,
15]. It is conceivable that the follow-up of these patients at two-week intervals was too far apart to detect differences in healing time, and therefore, differences may not have been captured in our study design.
The focus of this study was on the peri-operative healing time after EMLP. Post-hoc chart review, however, demonstrated that three patients had stenosis develop within 6 months of surgery and required revision EMLP. This rate of stenosis is similar to previously published rates of stenosis requiring revision surgery [
16]. However, long-term data was not available for the majority of our patient population due to clinic closure and logistical issues encountered in 2020 from the COVID pandemic. Future studies may be able to re-capture this patient population to obtain adequate longer-term data.
This study examined post-operative outcomes in patients with EMLP, where the patient is their own control. This is an important difference from previous study designs, as an alternative theory that could be deduced from this trial is that the post-operative healing time benefited from having at least one flap on a single side. This would be clinically significant and informative to the surgeon as these flaps can sometimes be damaged during surgery or injured while drilling the frontal and nasal bone. As such, if this occurred during a case, it is postulated that having one side with a mucosal flap can still help improve post-operative healing and possibly reduce the risk of stenosis. Further studies with longer-term follow-up would be needed to test this hypothesis, however.
A two-week interval between post-operative assessments was used as this is the interval typically used in the peri-operative period to review patients undergoing EMLP at this centre. For the purpose of this study, we wanted to maintain routine post-operative clinical visits for patients in this pilot study. However, to further evaluate the peri-operative differences in healing post-EMLP, it would be worthwhile for future studies to use a shorter time interval.
Further evaluation in the peri-operative period in this population would be beneficial. Wormald et al. have previously demonstrated the long-term outcomes of patients undergoing EMLP and that frontal nasal ostium has been observed to stabilise 12 months post-surgery [
17]. In addition, previous studies have histologically demonstrated that neo-osteogenesis is found in animal models 6 months post-surgery [
6]. However, to date, no study has followed the immediate peri-operative differences in healing in patients undergoing EMLP with versus without mucosal flaps. Understanding the normal peri-operative time toward healing can better guide clinical decisions as to the frequency and length of follow-up needed in the immediate post-operative period. Previous reports have shown that in the post-operative period, after sinus surgery, nasal debridement is associated with improved ostium patency and a lower rate of intranasal scarring [
18]. As such, one hypothesis that could be deduced is that earlier mucosalisation of exposed bone may lead to less crusting, less need for debridement in the peri-operative period and possibly improved rates of longer-term patency.
Several further limitations to this study have been identified. Surgeons were not blinded post-operatively as to the sidedness of the nasal flap. This introduces the possibility of confirmation bias; we recommend in the next randomised trial that reviewers be blinded to the side of the flap. Furthermore, patients were followed for a short duration post-surgery, limiting the evaluation of the long-term benefits of utilising a mucosal flap. Future studies should formally follow patients for longer follow-up periods to delineate the long-term outcomes of single-sided nasal flaps. A larger sample size is required to adequately power any future RCT. The data from this pilot study was utilised in an a priori power calculation for planning a prospective study. The study would require a sample size of 24 (power 0.80 at α = 0.05) to provide a 1-week improvement in healing. This would require a larger volume of patients meeting the criteria to undergo EMLP. As such, it may be worthwhile for future RCTs to consider a multi-centre trial in order to achieve the necessary patient participation to adequately power a future RCT within a reasonable time period. Finally, there are several factors that may impact post-operative healing (diabetes, smoking, etc.); these factors were not controlled for or standardly recorded as part of our data collection. Future studies should aim to better account for these potential confounding variables.
There is evidence that would suggest that the use of nasal flaps during EMLP can help to prevent surgical failure and restenosis. Our study demonstrated that mucosalisation was achieved in all patients within 6 weeks regardless of whether a flap was placed within the neo-ostium. This leaves the possibility that a single-sided mucosal flap may have provided at least some benefit in post-operative healing for both sides of the neo-ostium. Similar to previous studies, the majority of our patients had improved SNOT-22 scores and that the use of nasal flaps overall did not interfere with post-operative smell outcomes [
5]. Further studies are needed to elucidate the peri-operative healing in patients post-EMLP.


 ,
, 


{kind=link}
{kind=link}