
The Impact of a CMV Infection on the Expression of Selected Immunological Parameters in Liver Tissue in Children with Biliary Atresia
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
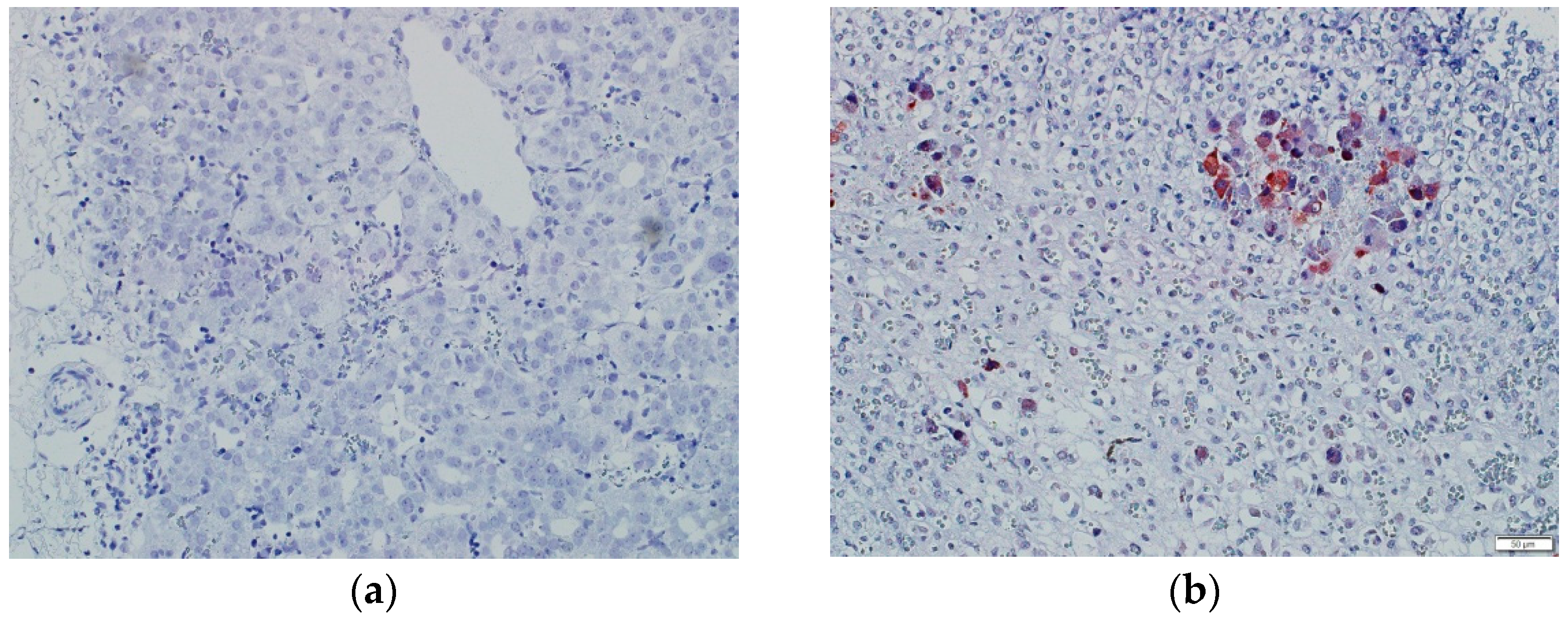
2.2. Determination of EBV and CMV Infection Status
2.3. In Situ Hybridization Technique
2.4. Immunohistochemistry
2.5. Morphometric Analyses
2.6. Statistical Analyses
2.7. Ethics
3. Results
3.1. Patients’ Characteristics
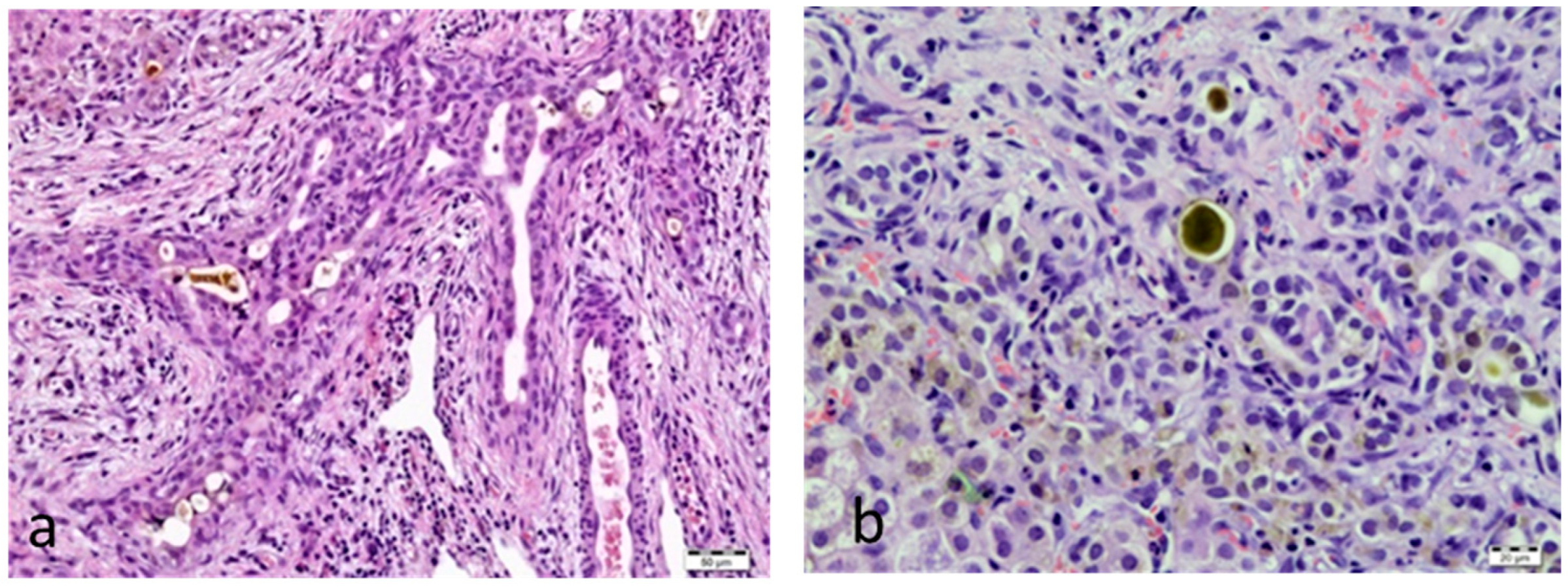
3.2. Histopathology
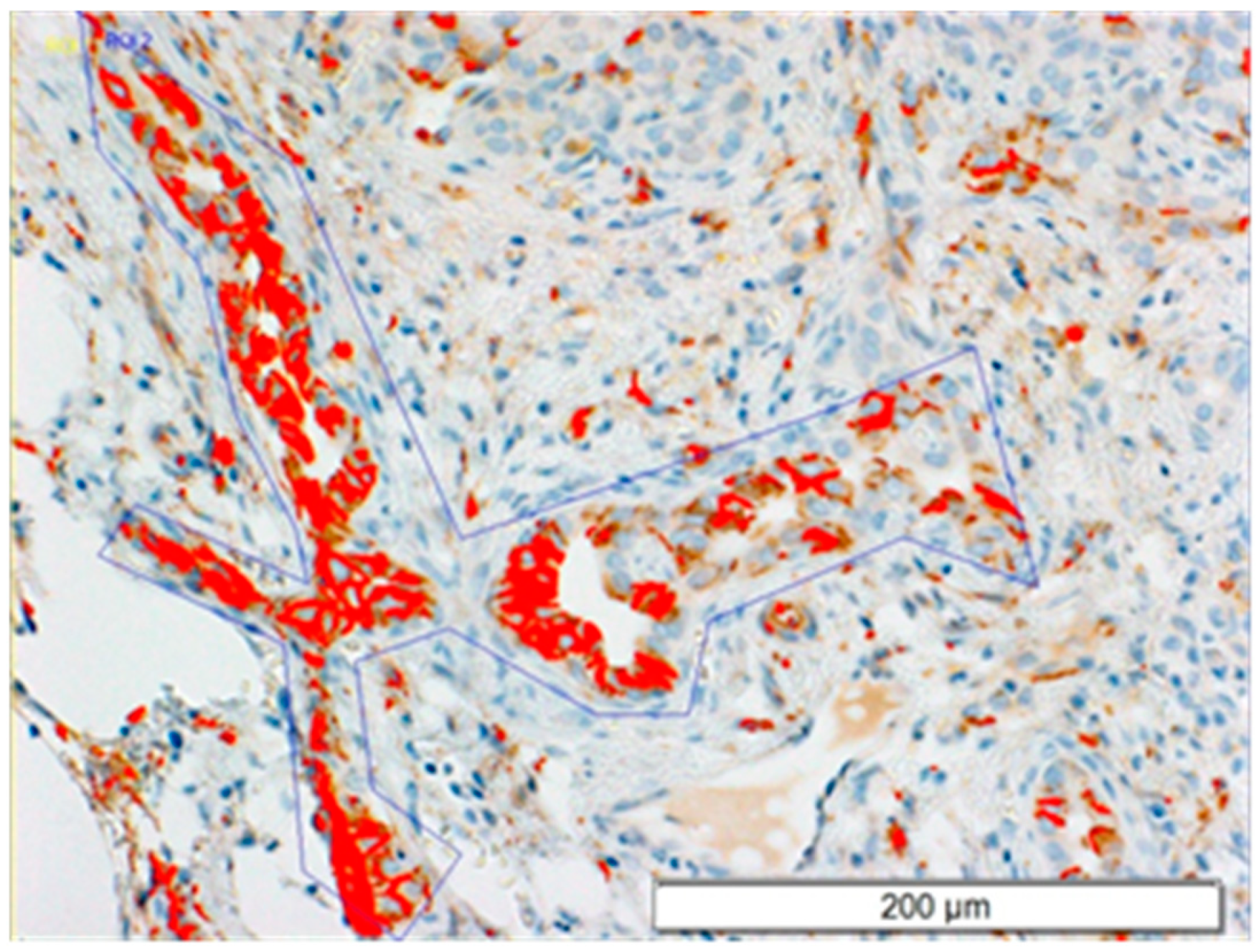
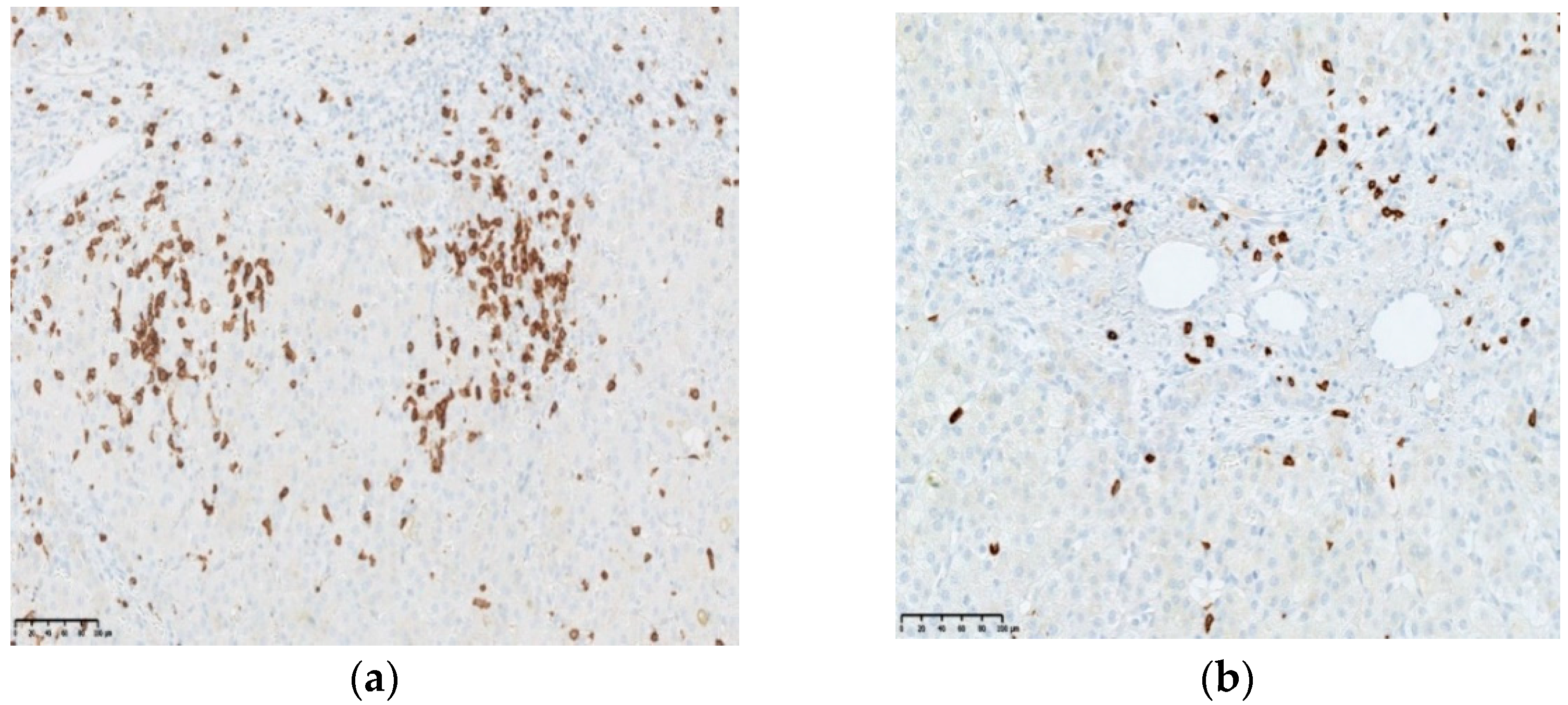
3.3. CD8 Expression
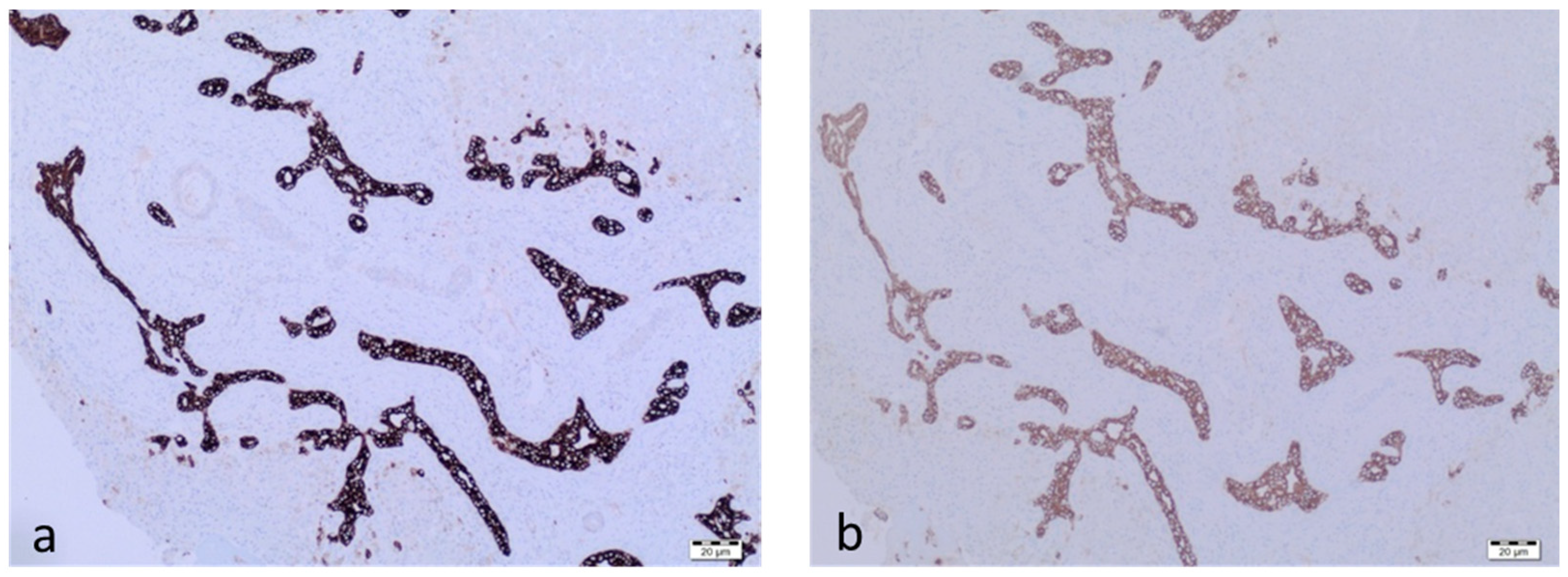
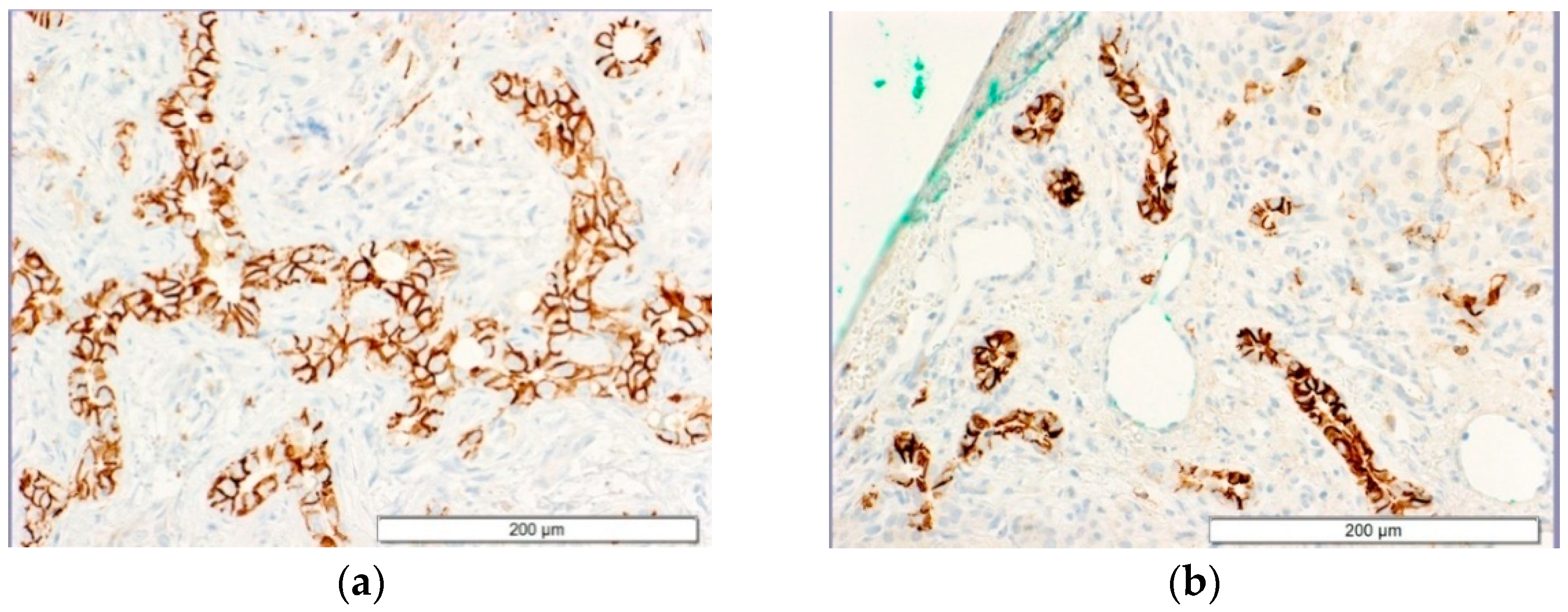
3.4. CD56 Expression
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Verkade, H.J.; Bezerra, J.A.; Davenport, M.; Schreiber, R.A.; Mieli-Vergani, G.; Hulscher, J.B.; Sokol, R.J.; Kelly, D.A.; Ure, B.; Whitington, P.F.; et al. Biliary atresia and other cholestatic childhood diseases: Advances and future challenges. J. Hepatol. 2016, 65, 631–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlmutter, D.H.; Shepherd, R.W. Extrahepatic biliary atesia: A disease or a phenotype? Hepatology 2002, 35, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Petersen, C.; Davenport, M. Aetiology of biliary atresia: What is actually known? Orphanet. J. Rare Dis. 2013, 8, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarr, P.I.; Haas, J.E.; Christie, D.L. Biliary atresia, cytomegalovirus, and age at referral. Pediatrics 1996, 97, 828–831. [Google Scholar] [CrossRef] [PubMed]
- Fischler, B.; Ehrnst, A.; Forsgren, M.; Örvell, C.; Nemeth, A. The viral association of neonatl cholestasis in Sweden: A possible link between cytomegalovirus infection and extrhepatic biliary atresia. J. Pediatr. Gastroenterol. Nutr. 1998, 27, 57–64. [Google Scholar] [CrossRef]
- Xu, Y.; Yu, J.; Zhang, R.; Yin, Y.; Ye, J.; Tan, L.; Xia, H. The prenatal infection of cytomegalowirus is an important etiology for biliary atresia in China. Clin. Pediatr. 2012, 51, 109–113. [Google Scholar] [CrossRef]
- Brindley, S.M.; Lanham, A.M.; Karrer, F.M.; Tucker, R.M.; Fontenot, A.P.; Mack, C.L. Cytomegalovirusspecific T-cell reactivity in biliary atresia at the time of diagnosis is associated with deficits in regulatory T cells. Hepatology 2012, 55, 1130–1138. [Google Scholar] [CrossRef] [Green Version]
- Zani, A.; Quaglia, A.; Hadzić, N.; Zuckerman, M.; Davenport, M. Cytomegalovirus-associated biliary atresia: Anaetiological and prognostic subgroup. J. Pediatr. Surg. 2015, 50, 1739–1745. [Google Scholar] [CrossRef]
- Rauschenfels, S.; Krassmann, M.; Al-Masri, A.N.; Verhagen, W.; Leonhardt, J.; Kuebler, J.F.; Petersen, C. Incidence of hepatotropic viruses in biliary atresia. Eur. J. Pediatr. 2009, 168, 469–476. [Google Scholar] [CrossRef]
- Bezerra, J.A.; Wells, R.G.; Mack, C.L.; Karpen, S.J.; Hoofnagle, J.H.; Doo, E.; Sokol, R.J. Biliary atresia: Clinical and research challenges for the twenty-first century. Hepatology 2018, 68, 1163–1173. [Google Scholar] [CrossRef]
- Mack, C.L.; Tucker, R.M.; Lu, B.R.; Sokol, R.J.; Fontenot, A.P.; Ueno, Y.; Gill, R.G. Cellular and humoral autoimmunity directed at bile duct epithelia in murine biliary atresia. Hepatology 2006, 44, 1231–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sokol, R.J.; Mack, C. Etiopathogenesis of biliary atresia. Semin. Liver Dis. 2001, 21, 517–524. [Google Scholar] [CrossRef]
- Guo, C.; Zhu, J.; Pu, C.L.; Deng, Y.H.; Zhang, M.M. Combinatory effects of hepatic CD8+ and NK lymphocytes in bile duct injury from biliary atresia. Pediatr. Res. 2012, 71, 638–644. [Google Scholar] [CrossRef] [Green Version]
- Mack, C.L.; Falta, M.T.; Sullivan, A.K.; Karrer, F.; Sokol, R.J.; Freed, B.M.; Fontenot, A.P. Oligoclonal Expansions of CD4+ and CD8+ T-Cells in the Target Organ of Patients With Biliary Atresia. Gastroenterology 2007, 133, 278–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shivakumar, P.; Sabla, G.; Mohanty, S.; McNeal, M.; Ward, R.; Stringer, K.; Caldwell, C.; Chougnet, C.; Bezerra, J.A. Effector role of neonatal hepatic CD8+ lymphocytes in epithelial injury and autoimmunity in experimental biliary atresia. Gastroenterology 2007, 133, 268–277. [Google Scholar] [CrossRef] [Green Version]
- Miethke, A.G.; Saxena, V.; Shivakumar, P.; Sabla, G.E.; Simmons, J.; Chougnet, C.A. Post-natal paucity of regulatory T cells and control of NK cell activation in experimental biliary atresia. J. Hepatol. 2010, 52, 718–726. [Google Scholar] [CrossRef] [Green Version]
- Davenport, M.; Gonde, C.; Redkar, R.; Koukoulis, G.; Tredger, M.; Mieli-Vergani, G.; Portmann, B.; Howard, E.R. Immunohistochemistry of the liver and biliary tree in extrahepatic biliary atresia. J. Pediatr. Surg. 2001, 36, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Shivakumar, P.; Sabla, G.E.; Whitington, P.; Chougnet, C.A.; Bezerra, J.A. Neonatal NK cells target the mouse duct epithelium via Nkg2d and drive tissue-specific injury in experimental biliary atresia. J. Clin. Investig. 2009, 119, 2281–2290. [Google Scholar] [CrossRef] [Green Version]
- Vivier, E.; Tomasello, E.; Baratin, M.; Walzer, T.; Ugolini, S. Functions of natural killer cells. Nat. Immunol. 2008, 9, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Rogler, L.E.; Teperman, L.; Morgan, G.; Rogler, C.E. Identification of hepatocytic and bile ductular cell lineages and candidate stem cells in bipolar ductular reactions in cirrhotic human liver. Hepatology 2007, 45, 716–724. [Google Scholar] [CrossRef]
- Torbenson, M.; Wang, J.; Abraham, S.; Maitra, A.; Boitnott, J. Bile ducts and ductules are positive for CD56 (N-CAM) in most cases of extrahepatic biliary atresia. Am. J. Surg. Pathol. 2003, 27, 1454–1457. [Google Scholar] [CrossRef] [PubMed]
- Sira, M.M.; El-Guindi, M.A.; Saber, M.A.; Ehsan, N.A.; Rizk, M.S. Differential hepatic expression of CD56 can discriminate biliary atresia from other neonatal cholestatic disorders. Eur. J. Gastroenterol. Hepatol. 2012, 24, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.Z.; Yu, J.K.; Peng, J.; Wang, F.H.; Liu, H.Y.; Lui, V.C.; Nicholls, J.M.; Tam, P.K.; Lamb, J.R.; Chen, Y.; et al. Role of CD56-expressing immature biliary epithelial cells in biliary atresia. World J. Gastroenterol. 2016, 22, 2545–2557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cielecka-Kuszyk, J.; Janowska, M.; Markiewicz, M.; Czubkowski, P.; Ostoja-Chyżyńska, A.; Bierła, J.; Cukrowska, B.; Pawłowska, J. The Usefulness of Immunohistochemical Staining of Bile Tracts in Biliary Atresia. Clin. Exp. Hepatol. 2021, 7, 41–46. [Google Scholar] [CrossRef]
- Ayyanar, P.; Mahalik, S.K.; Haldar, S.; Purkait, S.; Patra, S.; Mitra, S. Expression of CD56 is Not Limited to Biliary Atresia and Correlates with the Degree of Fibrosis in Pediatric Cholestatic Diseases. Fetal Pediatr. Pathol. 2022, 41, 87–97. [Google Scholar] [CrossRef]
- Van Wessel, D.B.; Boere, T.; Hulzebos, C.V.; de Kleine, R.H.; Verkade, H.J.; Hulscher, J.B. Preterm Infants With Biliary Atresia: A Nationwide Cohort Analysis From The Netherlands. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 370–374. [Google Scholar] [CrossRef]
- Yang, C.; Xing, H.; Tan, B.; Zhang, M. Immune Characteristics in Biliary Atresia Based on Immune Genes and Immune Cell Infiltration. Front. Pediatr. 2022, 10, 902571. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hbd (Weeks) | Age of HPE (Weeks) * | Total Bilirubin (mg/dL) | Direct Bilirubin (mg/dL) | ALT (U/L) | AST (U/L) | GGTP (U/L) | INR | |
|---|---|---|---|---|---|---|---|---|
| Q1 | 36 | 8.1 | 6.44 | 5.8 | 82 | 134 | 302 | 1.03 |
| median | 39 | 11.0 | 8.74 | 7.22 | 128 | 177 | 457 | 1.07 |
| Q3 | 39.5 | 13.9 | 10.39 | 9.11 | 175 | 248.5 | 784 | 1.1 |
| Patient | Sex | Hbd (Weeks) | Age of HPE (Weeks) * | Total Bilirubin (mg/dL) | Direct Bilirubin (mg/dL) | ALT (U/L) | AST (U/L) | GGTP (U/L) | INR | Age of LTx (Weeks) * | Time between LTx and HPE (Weeks) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group I | 1 | M | 40 | 12 | 6.31 | 7.01 | 88 | 143 | 820 | 1 | 29 | 17 |
| 2 | M | 40 | 13 | 8.34 | 7.47 | 128 | 202 | 1616 | 1.05 | |||
| 3 | M | 40 | 10 | 9.37 | 7.92 | 225 | 358 | 314 | 1.08 | 38 | 28 | |
| 4 | M | 27 | 15 | 11.66 | 10.24 | 271 | 439 | 450 | 1.28 | 28 | 13 | |
| Group II | 5 | F | 38 | 12 | 9.46 | 8.27 | 176 | 228 | 1652 | 1.08 | 43 | 29 |
| 6 | F | 39 | 11 | 5.91 | 5.24 | 104 | 177 | 358 | 1.07 | 41 | 30 | |
| 7 | F | 26 | 11 | 10.5 | 9.3 | 544 | 685 | 204 | 1.15 | 166 | 155 | |
| 8 | F | 24 | 15 | 14.44 | 12.62 | 271 | 326 | 754 | 1.07 | dq |
| Patient | CMV | |||
|---|---|---|---|---|
| IgM (AU/mL) | IgG (AU/mL) | PCR | ||
| Group I | 1 | 0.57 | 59.7 | (+) |
| 2 | 7.5 | 41.5 | (+) | |
| 3 | 0.79 | 715.2 | (+) | |
| 4 | 8.9 | 1181 | (+) | |
| Group II | 5 | 0.23 | 3.0 | (−) |
| 6 | 0.13 | 1.5 | (−) | |
| 7 | 0.15 | 0.53 | (−) | |
| 8 | 0.25 | 0.4 | (−) | |
| The Surface of Slides (µm2) | The Surface of Portal Areas (µm2) | The Number of CD8+ Cells Per µm2 of Portal Areas | The Surface of Bile Ducts in Portal Areas (µm2) | The Number of CD8+ Cells Per µm2 of Bile Ducts | |
|---|---|---|---|---|---|
| Group I | 17.67 ± 7.86 | 0.62 ± 0.35 | 206.92 ± 82.01 * p = 0.0019 | 2870.55 ± 3279.32 | 0.73 ± 1.23 # p = 0.0019 |
| Group II | 17.99 ± 5.06 | 0.41 ± 0.28 | 82.00 ± 38.98 | 2089.63 ± 1973.30 | 0.37 ± 0.62 |
| Group I (n =4) (%) | Group II (n =4) (%) | p-Value |
|---|---|---|
| 2.92 ± 1.43 | 1.43 ± 0.28 | 0.00003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janowska, M.; Bierła, J.B.; Kaleta, M.; Wierzbicka-Rucińska, A.; Czubkowski, P.; Kanarek, E.; Cukrowska, B.; Pawłowska, J.; Cielecka-Kuszyk, J. The Impact of a CMV Infection on the Expression of Selected Immunological Parameters in Liver Tissue in Children with Biliary Atresia. J. Clin. Med. 2022, 11, 7269. https://doi.org/10.3390/jcm11247269
Janowska M, Bierła JB, Kaleta M, Wierzbicka-Rucińska A, Czubkowski P, Kanarek E, Cukrowska B, Pawłowska J, Cielecka-Kuszyk J. The Impact of a CMV Infection on the Expression of Selected Immunological Parameters in Liver Tissue in Children with Biliary Atresia. Journal of Clinical Medicine. 2022; 11(24):7269. https://doi.org/10.3390/jcm11247269
Chicago/Turabian StyleJanowska, Maria, Joanna B. Bierła, Magdalena Kaleta, Aldona Wierzbicka-Rucińska, Piotr Czubkowski, Ewelina Kanarek, Bożena Cukrowska, Joanna Pawłowska, and Joanna Cielecka-Kuszyk. 2022. "The Impact of a CMV Infection on the Expression of Selected Immunological Parameters in Liver Tissue in Children with Biliary Atresia" Journal of Clinical Medicine 11, no. 24: 7269. https://doi.org/10.3390/jcm11247269