
Clinical and Radiological Outcomes after Total Shoulder Arthroplasty Using Custom-Made Glenoid Components: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
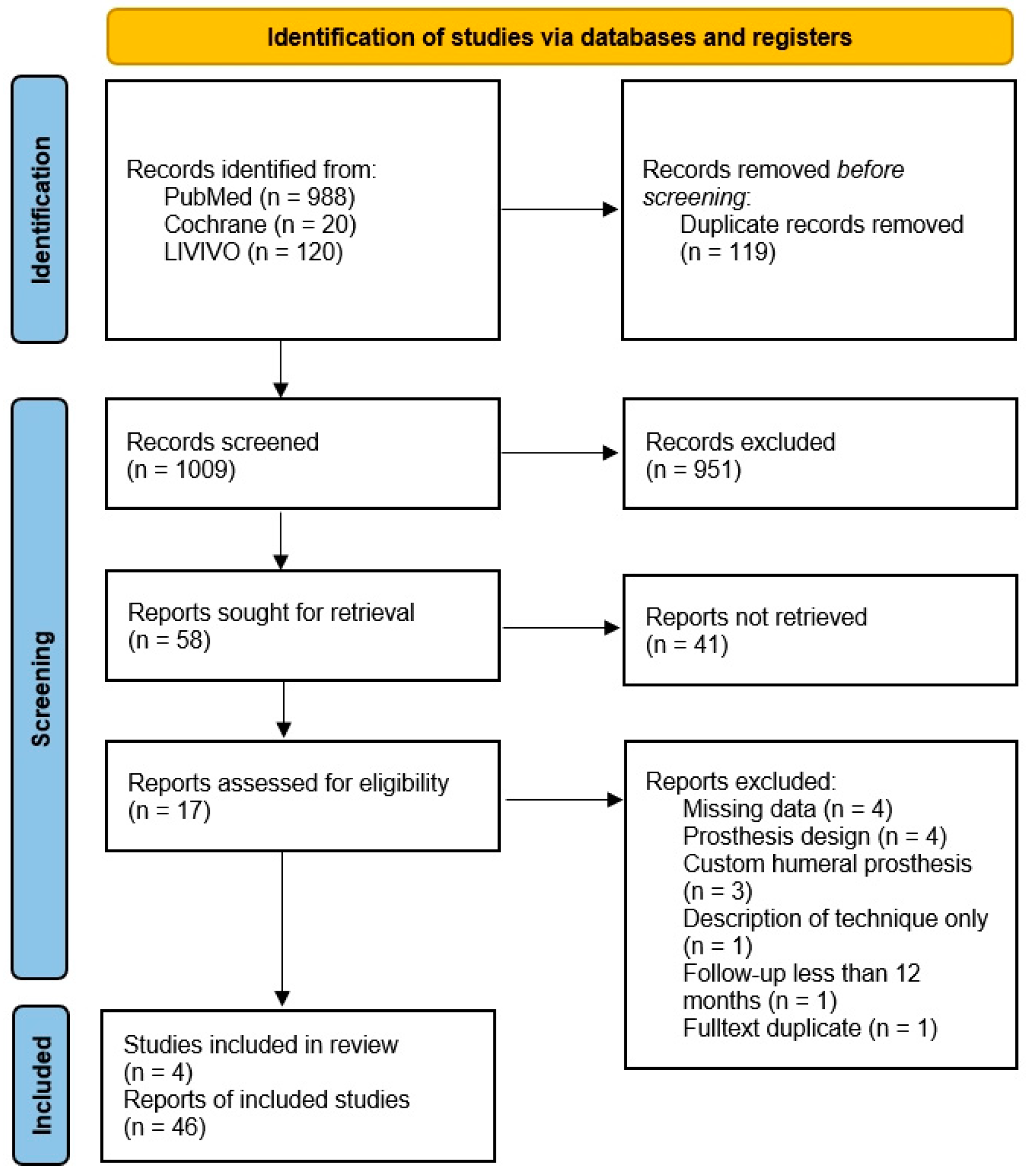
2.1. Searching Procedure and Eligibility Criteria
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
3.1. Studies in Detail
3.2. Weighted Means Calculation

{kind=link}
| Bodendorfer et al. [20] | Ortmaier et al. [17] | Porcellini et al. [19] | Rangarajan et al. [18] | |
|---|---|---|---|---|
| CMS b (0–100) | ||||
| preOP | - | 10.9 ± 4.2 | 15 | 24.6 ± 10.2 |
| postop | - | 51.7 ± 9.9 | 24.8 | 60.4 ± 14.5 |
| ASES c (0–100) | ||||
| preOP | 33 | - | 15.3 | 32 ± 18.2 |
| postop | 80 | - | 45.8 | 79 ± 15.6 |
| VAS d (0–10) | ||||
| preOP | 7 | - | 8 | 6.2 ± 2.9 |
| postop | 0 | - | 2.3 | 0.7 ± 1.3 |
| Anteversion (deg) | ||||
| preOP | 95 | 28 ± 10.3 | 41.7 | 53 ± 27 |
| postop | 150 | 132 ± 27 | 62 | 124 ± 23 |
| Abduction (deg) | ||||
| preOP | - | 19 ± 7.4 | 35.8 | 42 ± 17 |
| postOP | - | 121 ± 31.4 | 55 | 77 ± 15 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, J.A.; Sperling, J.W.; Cofield, R.H. Revision surgery following total shoulder arthroplasty: Analysis of 2588 shoulders over three decades (1976 to 2008). J. Bone Jt. Surg.—Ser. B 2011, 93 B, 1513–1517. [Google Scholar] [CrossRef]
- Barco, R.; Savvidou, O.D.; Sperling, J.W.; Sanchez-Sotelo, J.; Cofield, R.H. Complications in reverse shoulder arthroplasty. EFORT Open Rev. 2016, 1, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Cofield, R.H. Bone grafting for glenoid bone deficiencies in shoulder arthritis: A review. J. Shoulder Elb. Surg. 2007, 16, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Debeer, P.; Berghs, B.; Pouliart, N.; Van den Bogaert, G.; Verhaegen, F.; Nijs, S. Treatment of severe glenoid deficiencies in reverse shoulder arthroplasty: The Glenius Glenoid Reconstruction System experience. J. Shoulder Elb. Surg. 2019, 28, 1601–1608. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Thussbas, C.; Koch, M.; Seebauer, L. Management of glenoid bone defects with reverse shoulder arthroplasty—Surgical technique and clinical outcomes. J. Shoulder Elb. Surg. 2018, 27, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Strauss, E.J.; Roche, C.; Flurin, P.H.; Wright, T.; Zuckerman, J.D. The glenoid in shoulder arthroplasty. J. Shoulder Elb. Surg. 2009, 18, 819–833. [Google Scholar] [CrossRef]
- Kocsis, G.; Thyagarajan, D.S.; Fairbairn, K.J.; Wallace, W.A. A new classification of glenoid bone loss to help plan the implantation of a glenoid component before revision arthroplasty of the shoulder. Bone Joint J. 2016, 98-B, 374–380. [Google Scholar] [CrossRef]
- Seidl, A.J.; Williams, G.R.; Boileau, P. Challenges in Reverse Shoulder Arthroplasty: Addressing Glenoid Bone Loss. Orthopedics 2016, 39, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Salhi, A.; Burdin, V.; Boutillon, A.; Brochard, S.; Mutsvangwa, T.; Borotikar, B. Statistical Shape Modeling Approach to Predict Missing Scapular Bone. Ann. Biomed. Eng. 2020, 48, 367–379. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Prospective Register Of Systematic Reviews. Available online: http://www.crd.york.ac.uk/prospero (accessed on 1 March 2022).
- Kohl, C.; McIntosh, E.J.; Unger, S.; Haddaway, N.R.; Kecke, S.; Schiemann, J.; Wilhelm, R. Online tools supporting the conduct and reporting of systematic reviews and systematic maps: A case study on CADIMA and review of existing tools. Environ. Evid. 2018, 7, 8. [Google Scholar] [CrossRef] [Green Version]
- CADIMA. Quedlinburg, Germany: Julius Kühn-Institut; 2017. Available online: https://www.cadima.info/index.php (accessed on 1 March 2022).
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H.; Goddard, O.; et al. Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence. Available online: http://www.cebm.net/index.aspx?o=5653 (accessed on 1 July 2022).
- Constant, C.R.; Murley, A.H. A Clinical Method of Functional Assessment of the Shoulder. Clin. Orthop. Relat. Res. 1987, 214, 160–164. [Google Scholar] [CrossRef]
- Richards, R.R.; An, K.N.; Bigliani, L.U.; Friedman, R.J.; Gartsman, G.M.; Gristina, A.G.; Iannotti, J.P.; Mow, V.C.; Sidles, J.A.; Zuckerman, J.D. A standardized method for the assessment of shoulder function. J. Shoulder Elb. Surg. 1994, 3, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Ortmaier, R.; Wierer, G.; Gruber, M.S. Functional and Radiological Outcomes after Treatment with Custom-Made Glenoid Components in Revision Reverse Shoulder Arthroplasty. J. Clin. Med. 2022, 11, 551. [Google Scholar] [CrossRef] [PubMed]
- Rangarajan, R.; Blout, C.K.; Patel, V.V.; Bastian, S.A.; Lee, B.K.; Itamura, J.M. Early results of reverse total shoulder arthroplasty using a patient-matched glenoid implant for severe glenoid bone deficiency. J. Shoulder Elb. Surg. 2020, 29, S139–S148. [Google Scholar] [CrossRef]
- Porcellini, G.; Micheloni, G.M.; Tarallo, L.; Paladini, P.; Merolla, G.; Catani, F. Custom-made reverse shoulder arthroplasty for severe glenoid bone loss: Review of the literature and our preliminary results. J. Orthop. Traumatol. 2021, 22, 2. [Google Scholar] [CrossRef]
- Bodendorfer, B.M.; Loughran, G.J.; Looney, A.M.; Velott, A.T.; Stein, J.A.; Lutton, D.M.; Wiesel, B.B.; Murthi, A.M. Short-term outcomes of reverse shoulder arthroplasty using a custom baseplate for severe glenoid deficiency. J. Shoulder Elb. Surg. 2021, 30, 1060–1067. [Google Scholar] [CrossRef]
- Antuna, S.A.; Sperling, J.W.; Cofield, R.H.; Rowland, C.M. Glenoid revision surgery after total shoulder arthroplasty. J. Shoulder Elb. Surg. 2001, 10, 217–224. [Google Scholar] [CrossRef]
- Page, R.S.; Haines, J.F.; Trail, I. Impaction Bone Grafting of the Glenoid in Revision Shoulder Arthroplasty: Classification, Technical Description and Early Results. Shoulder Elb. 2009, 1, 81–88. [Google Scholar] [CrossRef]
- Rockwood, C.A.J.; Matsen, F.A.I. The Shoulder; Elsevier Health Sciences: Amsterdam, The Netherlands, 2009; ISBN 9780323698368. [Google Scholar]
- Bercik, M.J.; Kruse, K.; Yalizis, M.; Gauci, M.O.; Chaoui, J.; Walch, G. A modification to the Walch classification of the glenoid in primary glenohumeral osteoarthritis using three-dimensional imaging. J. Shoulder Elb. Surg. 2016, 25, 1601–1606. [Google Scholar] [CrossRef]
- Sirveaux, F.; Favard, L.; Oudet, D.; Huquet, D.; Walch, G.; Mole, D. Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff. J. Bone Joint Surg. Br. 2004, 86-B, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Huskisson, E.C. Measurement of pain. J. Rheumatol. 1982, 9, 768–769. [Google Scholar] [CrossRef] [PubMed]
- Simovitch, R.; Flurin, P.-H.; Wright, T.; Zuckerman, J.D.; Roche, C.P. Quantifying success after total shoulder arthroplasty: The substantial clinical benefit. J. Shoulder Elb. Surg. 2018, 27, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Simovitch, R.; Flurin, P.-H.; Wright, T.; Zuckerman, J.D.; Roche, C.P. Quantifying success after total shoulder arthroplasty: The minimal clinically important difference. J. Shoulder Elb. Surg. 2018, 27, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Tashjian, R.Z.; Shin, J.; Broschinsky, K.; Yeh, C.-C.; Martin, B.; Chalmers, P.N.; Greis, P.E.; Burks, R.T.; Zhang, Y. Minimal clinically important differences in the American Shoulder and Elbow Surgeons, Simple Shoulder Test, and visual analog scale pain scores after arthroscopic rotator cuff repair. J. Shoulder Elb. Surg. 2020, 29, 1406–1411. [Google Scholar] [CrossRef] [PubMed]
- Chammaa, R.; Uri, O.; Lambert, S. Primary shoulder arthroplasty using a custom-made hip-inspired implant for the treatment of advanced glenohumeral arthritis in the presence of severe glenoid bone loss. J. Shoulder Elb. Surg. 2017, 26, 101–107. [Google Scholar] [CrossRef]
- Ortmaier, R.; Resch, H.; Matis, N.; Blocher, M.; Auffarth, A.; Mayer, M.; Hitzl, W.; Tauber, M. Reverse shoulder arthroplasty in revision of failed shoulder arthroplasty—Outcome and follow-up. Int. Orthop. 2013, 37, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Ravi, V.; Murphy, R.J.; Moverley, R.; Derias, M.; Phadnis, J. Outcome and complications following revision shoulder arthroplasty. A systematic review and meta-analysis. Bone Jt. Open 2021, 2, 618–630. [Google Scholar] [CrossRef]
- Iannotti, J.P.; Frangiamore, S.J. Fate of large structural allograft for treatment of severe uncontained glenoid bone deficiency. J. Shoulder Elbow Surg. 2012, 21, 765–771. [Google Scholar] [CrossRef]
- Scalise, J.J.; Iannotti, J.P. Bone grafting severe glenoid defects in revision shoulder arthroplasty. Clin. Orthop. Relat. Res. 2008, 466, 139–145. [Google Scholar] [CrossRef]
- Hsu, J.E.; Ricchetti, E.T.; Huffman, G.R.; Iannotti, J.P.; Glaser, D.L. Addressing glenoid bone deficiency and asymmetric posterior erosion in shoulder arthroplasty. J. Shoulder Elbow Surg. 2013, 22, 1298–1308. [Google Scholar] [CrossRef] [PubMed]

| Author | Year | Shoulders | Primary/ Revision | Follow-Up (m) | Age (y) | Sex (m/f) |
|---|---|---|---|---|---|---|
| Bodendorfer et al. [20] | 2020 | 12 | 7/5 | 30.9 (24–52) | 68.0 (57–78) | 7/5 |
| Ortmaier et al. [17] | 2022 | 10 | 0/10 | 23.1 (16–30) | 76.6 (65–83) | 0/10 |
| Porcellini et al. [19] | 2021 | 6 | 2/4 | 31.7 (25–38) | 64.0 (48–74) | 3/3 |
| Rangarajan et al. [18] | 2020 | 18 | 8/10 | 18.2 (12–27) | 66.6 (50–80) | 11/7 |
| Summary | 46 | 17/29 | 24.3 (12–52) | 68.8 (48–83) | 21/25 |
| preOP | postOP | |
|---|---|---|
| CMS (n = 34) b | 18.9 (5–45) | 51.6 (12–85) |
| ASES (n = 40) c | 26.6 (3.3–66.7) | 66.4 (25–100) |
| VAS (n = 40) d | 6.1 (1–10) | 0.7 (0–5) |
| Active Anteversion (n = 46) | 57 (0–123) | 124.4 (90–170) |
| Active Abduction (n = 34) | 34.2 (0–70) | 86.1 (45–170) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gruber, M.S.; Schwarz, T.; Lindorfer, M.; Rittenschober, F.; Bischofreiter, M.; Hochreiter, J.; Ortmaier, R. Clinical and Radiological Outcomes after Total Shoulder Arthroplasty Using Custom-Made Glenoid Components: A Systematic Review. J. Clin. Med. 2022, 11, 7268. https://doi.org/10.3390/jcm11247268
Gruber MS, Schwarz T, Lindorfer M, Rittenschober F, Bischofreiter M, Hochreiter J, Ortmaier R. Clinical and Radiological Outcomes after Total Shoulder Arthroplasty Using Custom-Made Glenoid Components: A Systematic Review. Journal of Clinical Medicine. 2022; 11(24):7268. https://doi.org/10.3390/jcm11247268
Chicago/Turabian StyleGruber, Michael Stephan, Tamara Schwarz, Marlene Lindorfer, Felix Rittenschober, Martin Bischofreiter, Josef Hochreiter, and Reinhold Ortmaier. 2022. "Clinical and Radiological Outcomes after Total Shoulder Arthroplasty Using Custom-Made Glenoid Components: A Systematic Review" Journal of Clinical Medicine 11, no. 24: 7268. https://doi.org/10.3390/jcm11247268