
Glenoid Inclination: Choosing the Transverse Axis Is Critical—A 3D Automated versus Manually Measured Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Cohort
2.2. Data Acquisition
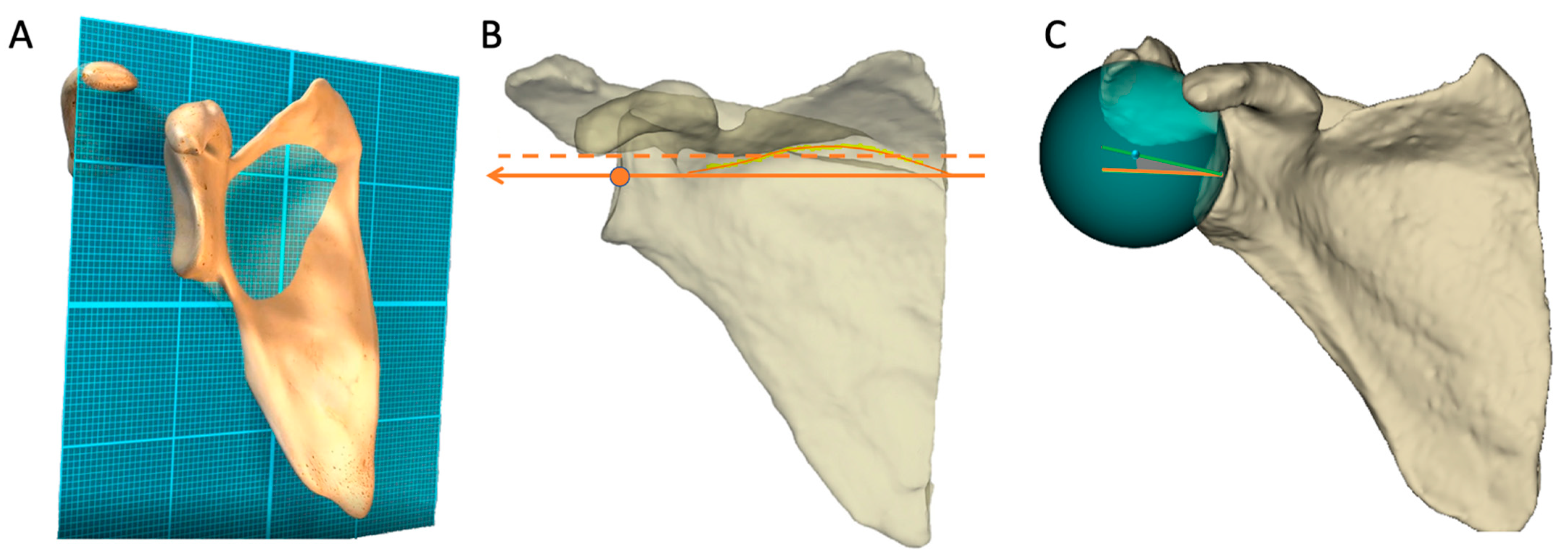
2.3. Method Glenoid Inclination Measure
- The scapula frontal plane.
- The transverse axis.
- The glenoid mediolateral axis.
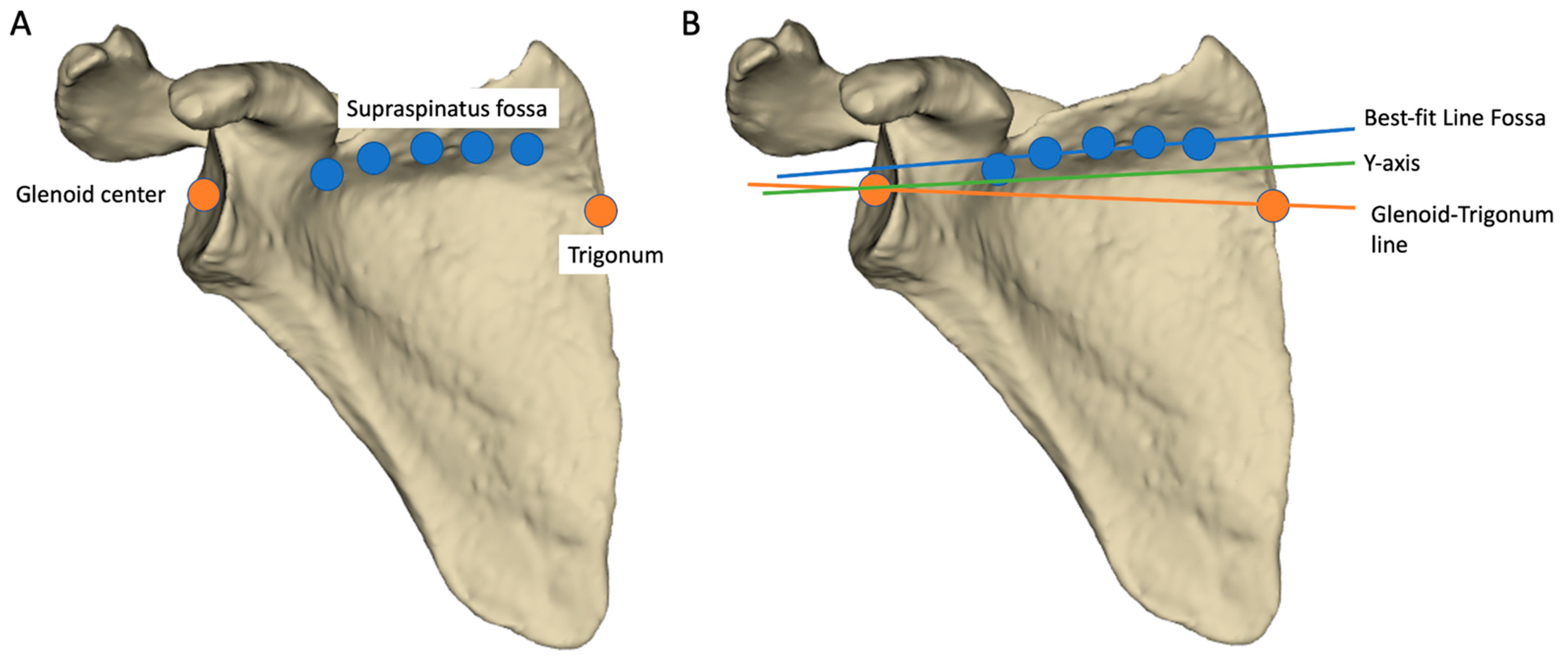
2.4. Input Data Definitions
- The trigonum: point at the intersection of the scapular spine and the medial border of the scapula.
- The glenoid center: a point determined by the center of the segment between the upper and lower apex of the glenoid.
- Five points were picked regularly along the bottom of the supraspinatus fossa and used to define the best-fit line fossa, as described by Terrier et al. [5].
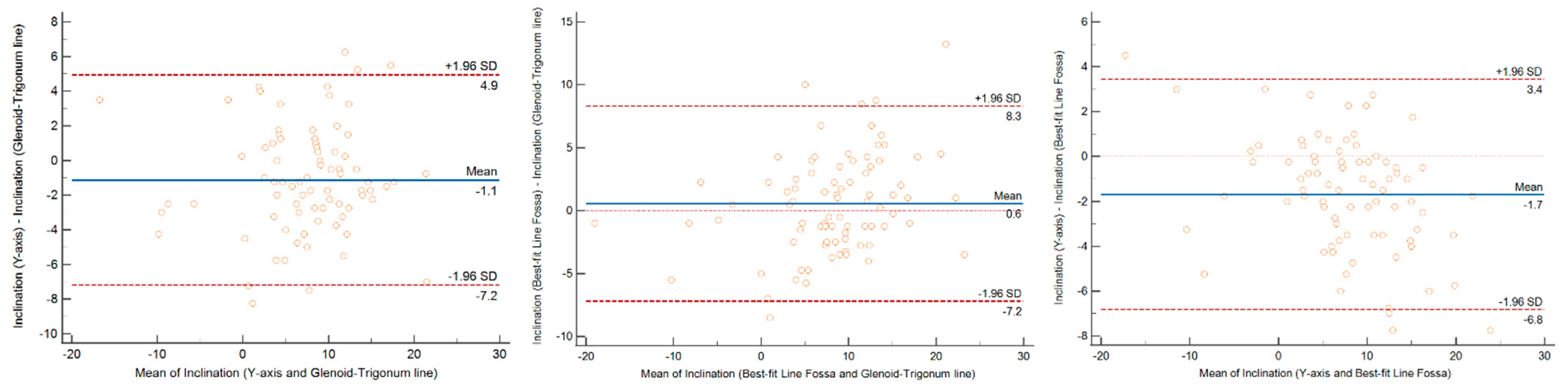
2.5. Statistical Analysis
- We calculated the linear correlation coefficient between the two samples.
- Then, if significant (r > 0.7), we interpreted a Bland and Altman graph and see if the chosen predefined thresholds were met: maximum mean arithmetic bias at 3° and/or 95% confidence interval at 5° [21].
- If the value was below the established thresholds (mean or confidence interval), the method was declared as concordant and we did not calculate the Lin’s concordance coefficient in that case.
- If the value was over the established thresholds, to interpret the source of the mismatch, the Lin’s concordance coefficient was calculated, making it possible to assess whether it was a lack of precision (LoP, %) or a lack of accuracy (LoA, %). The sum of both LoP and LoA was 100%.
3. Results
3.1. Glenoid Inclination Values and ICC
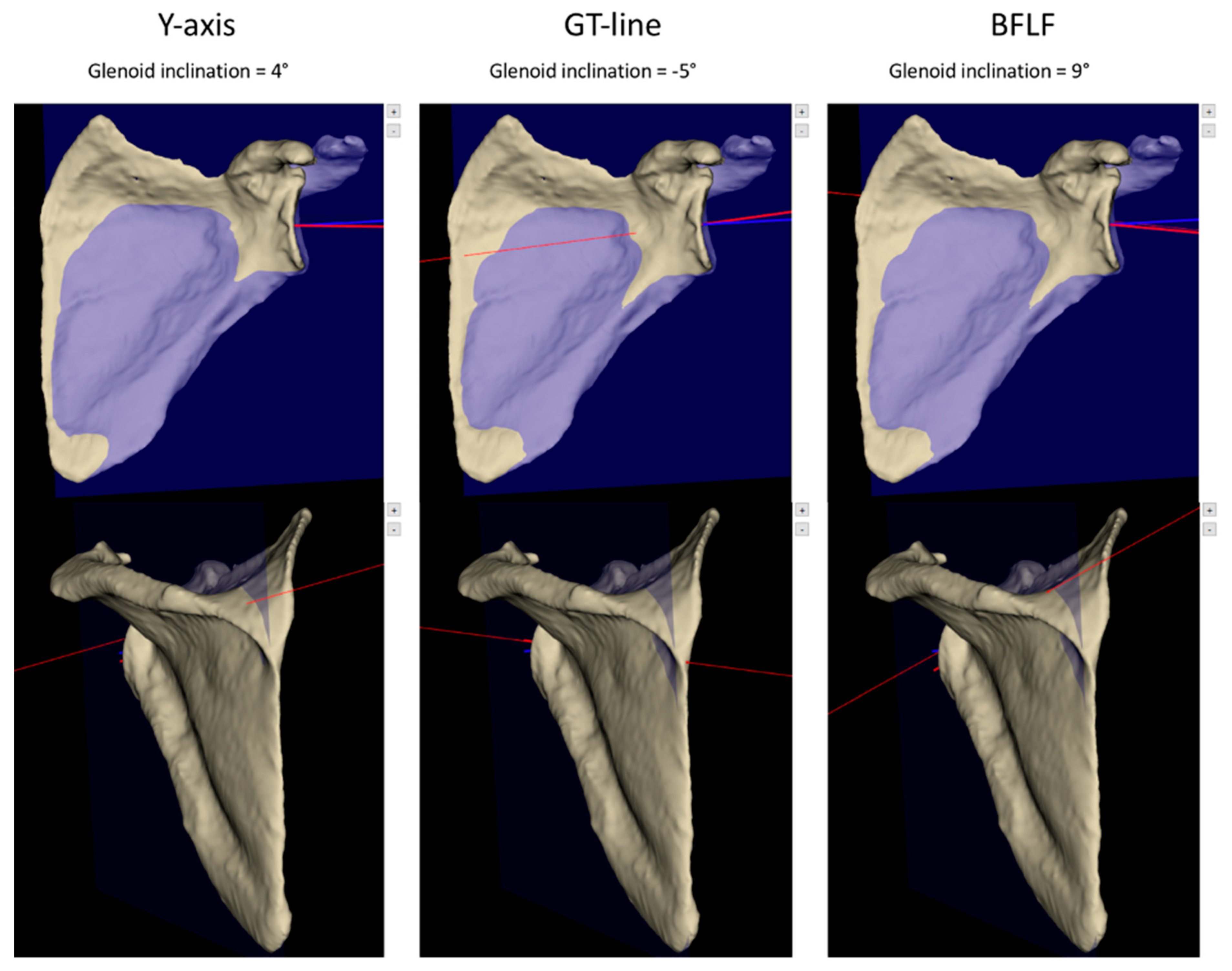
3.2. Identification of the Differences between the Inclination Measurement Methods
4. Discussion
4.1. Inclination Variability
4.2. Factors Influencing the Transverse Axis
4.3. Strengths and Limits
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Basmajian, J.V.; Bazant, F.J. Factors Preventing Downward Dislocation of the Adducted Shoulder Joint. An Electromyographic and Morphological Study. J. Bone Jt. Surg. Am. 1959, 41-A, 1182–1186. [Google Scholar] [CrossRef]
- Bokor, D.J.; O’Sullivan, M.D.; Hazan, G.J. Variability of Measurement of Glenoid Version on Computed Tomography Scan. J. Shoulder Elb. Surg. 1999, 8, 595–598. [Google Scholar] [CrossRef]
- Kwon, Y.W.; Powell, K.A.; Yum, J.K.; Brems, J.J.; Iannotti, J.P. Use of Three-Dimensional Computed Tomography for the Analysis of the Glenoid Anatomy. J. Shoulder Elb. Surg. 2005, 14, 85–90. [Google Scholar] [CrossRef]
- Maurer, A.; Fucentese, S.F.; Pfirrmann, C.W.A.; Wirth, S.H.; Djahangiri, A.; Jost, B.; Gerber, C. Assessment of Glenoid Inclination on Routine Clinical Radiographs and Computed Tomography Examinations of the Shoulder. J. Shoulder Elb. Surg. 2012, 21, 1096–1103. [Google Scholar] [CrossRef] [Green Version]
- Terrier, A.; Ston, J.; Larrea, X.; Farron, A. Measurements of Three-Dimensional Glenoid Erosion When Planning the Prosthetic Replacement of Osteoarthritic Shoulders. Bone Jt. J. 2014, 96-B, 513–518. [Google Scholar] [CrossRef] [Green Version]
- Boileau, P.; Cheval, D.; Gauci, M.-O.; Holzer, N.; Chaoui, J.; Walch, G. Automated Three-Dimensional Measurement of Glenoid Version and Inclination in Arthritic Shoulders. J. Bone Jt. Surg. Am. 2018, 100, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.R.; Bodendorfer, B.M.; Laucis, N.C.; Wang, D.X.; Dean, D.M.; Rabe, J.L.; Soliman, S.B.; Klochko, C.L.; Argintar, E.H.; Lutton, D.M.; et al. Significant Variability Exists in Preoperative Planning Software Measures of Glenoid Morphology for Shoulder Arthroplasty. Semin. Arthroplast. JSES 2021, 32, 82–92. [Google Scholar] [CrossRef]
- Beeler, S.; Hasler, A.; Götschi, T.; Meyer, D.C.; Gerber, C. Critical Shoulder Angle: Acromial Coverage Is More Relevant than Glenoid Inclination. J. Orthop. Res. 2019, 37, 205–210. [Google Scholar] [CrossRef] [Green Version]
- Boileau, P.; Gauci, M.-O.; Wagner, E.R.; Clowez, G.; Chaoui, J.; Chelli, M.; Walch, G. The Reverse Shoulder Arthroplasty Angle: A New Measurement of Glenoid Inclination for Reverse Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2019, 28, 1281–1290. [Google Scholar] [CrossRef] [Green Version]
- Gauci, M.O.; Boileau, P.; Baba, M.; Chaoui, J.; Walch, G. Patient-Specific Glenoid Guides Provide Accuracy and Reproducibility in Total Shoulder Arthroplasty. Bone Jt. J. 2016, 98-B, 1080–1085. [Google Scholar] [CrossRef]
- Bechtold, D.A.; Ganapathy, P.K.; Aleem, A.W.; Chamberlain, A.M.; Keener, J.D. The Relationship between Glenoid Inclination and Instability following Primary Reverse Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2020, 30, e370–e377. [Google Scholar] [CrossRef] [PubMed]
- Tashjian, R.Z.; Martin, B.I.; Ricketts, C.A.; Henninger, H.B.; Granger, E.K.; Chalmers, P.N. Superior Baseplate Inclination Is Associated with Instability after Reverse Total Shoulder Arthroplasty. Clin. Orthop. Relat. Res. 2018, 476, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.; Martin, J.R.; Campbell, D.H.; Fernandes, R.R.; Amini, M.H. Inferior Tilt of the Glenoid Leads to Medialization and Increases Impingement on the Scapular Neck in Reverse Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2021, 30, 1273–1281. [Google Scholar] [CrossRef]
- Knighton, T.W.; Chalmers, P.N.; Sulkar, H.J.; Aliaj, K.; Tashjian, R.Z.; Henninger, H.B. Reverse Total Shoulder Glenoid Component Inclination Affects Glenohumeral Kinetics During Abduction: A Cadaveric Study. J. Shoulder Elb. Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Walch, G.; Badet, R.; Boulahia, A.; Khoury, A. Morphologic Study of the Glenoid in Primary Glenohumeral Osteoarthritis. J. Arthroplast. 1999, 14, 756–760. [Google Scholar] [CrossRef]
- Bercik, M.J.; Kruse, K.; Yalizis, M.; Gauci, M.-O.; Chaoui, J.; Walch, G. A Modification to the Walch Classification of the Glenoid in Primary Glenohumeral Osteoarthritis Using Three-Dimensional Imaging. J. Shoulder Elb. Surg. 2016, 25, 1601–1606. [Google Scholar] [CrossRef]
- Favard, L.; Lautmann, S.; Sirveaux, F.; Oudet, D.; Kerjean, Y.; Huguet, D. Hemiarthroplasty versus Reverse Arthroplasty in the Treatment of Osteoarthritis with Massive Rotator Cuff Tear. In 2000 Shoulder Prostheses. Two to Ten Years Follow-Up; Walch, G., Boileau, P., Mole, D., Eds.; 2001; pp. 261–268. Available online: https://www.researchgate.net/publication/288193095_2000_Shoulder_Prosthesis_Two_to_Ten_Year_Follow-up (accessed on 17 July 2022).
- Moineau, G.; Levigne, C.; Boileau, P.; Young, A.; Walch, G. Three-Dimensional Measurement Method of Arthritic Glenoid Cavity Morphology: Feasibility and Reproducibility. Orthop. Traumatol. Surg. Res. 2012, 98, S139–S145. [Google Scholar] [CrossRef] [Green Version]
- Walch, G.; Vezeridis, P.S.; Boileau, P.; Deransart, P.; Chaoui, J. Three-Dimensional Planning and Use of Patient-Specific Guides Improve Glenoid Component Position: An In Vitro Study. J. Shoulder Elb. Surg. 2015, 24, 302–309. [Google Scholar] [CrossRef]
- Gauci, M.-O.; Deransart, P.; Chaoui, J.; Urvoy, M.; Athwal, G.S.; Sanchez-Sotelo, J.; Boileau, P.; Walch, G. Three-Dimensional Geometry of the Normal Shoulder: A Software Analysis. J. Shoulder Elb. Surg. 2020, 29, e468–e477. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Amini, M.H.; Ricchetti, E.T.; Iannotti, J.P. Three-Dimensional Templating and Use of Standard Instrumentation in Primary Anatomic Total Shoulder Arthroplasty. JBJS Essent Surg. Tech. 2017, 7, e28. [Google Scholar] [CrossRef] [PubMed]
- Iannotti, J.P.; Walker, K.; Rodriguez, E.; Patterson, T.E.; Jun, B.-J.; Ricchetti, E.T. Accuracy of 3-Dimensional Planning, Implant Templating, and Patient-Specific Instrumentation in Anatomic Total Shoulder Arthroplasty. J. Bone Jt. Surg. Am. 2019, 101, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Mallon, W.J.; Brown, H.R.; Vogler, J.B.; Martinez, S. Radiographic and Geometric Anatomy of the Scapula. Clin. Orthop. Relat. Res. 1992, 277, 142–154. [Google Scholar] [CrossRef]
- Habermeyer, P.; Magosch, P.; Luz, V.; Lichtenberg, S. Three-Dimensional Glenoid Deformity in Patients with Osteoarthritis: A Radiographic Analysis. J. Bone Jt. Surg. Am. 2006, 88, 1301–1307. [Google Scholar] [CrossRef]
- Chalmers, P.N.; Suter, T.; Jacxsens, M.; Zhang, Y.; Zhang, C.; Tashjian, R.Z.; Henninger, H.B. Influence of Radiographic Viewing Perspective on Glenoid Inclination Measurement. J. Shoulder Elb. Arthroplast. 2019, 3, 2471549218824986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalmers, P.N.; Salazar, D.; Chamberlain, A.; Keener, J.D. Radiographic Characterization of the B2 Glenoid: The Effect of Computed Tomographic Axis Orientation. J. Shoulder Elb. Surg. 2016, 26, 258–264. [Google Scholar] [CrossRef]
- Denard, P.J.; Provencher, M.T.; Lädermann, A.; Romeo, A.A.; Parsons, B.O.; Dines, J.S. Version and Inclination Obtained with 3-Dimensional Planning in Total Shoulder Arthroplasty: Do Different Programs Produce the Same Results? JSES Open Access 2018, 2, 200–204. [Google Scholar] [CrossRef] [Green Version]
- Mahendraraj, K.A.; Shields, M.V.; Grubhofer, F.; Golenbock, S.W.; Jawa, A. Reassessing Glenoid Inclination in Reverse Total Shoulder Arthroplasty with Glenosphere Lateralization. Bone Jt. J. 2021, 103-B, 360–365. [Google Scholar] [CrossRef]
- Ho, J.C.; Sabesan, V.J.; Iannotti, J.P. Glenoid Component Retroversion Is Associated with Osteolysis. J. Bone Jt. Surg. Am. 2013, 95, e82. [Google Scholar] [CrossRef]
- Young, A.A.; Walch, G.; Pape, G.; Gohlke, F.; Favard, L. Secondary Rotator Cuff Dysfunction Following Total Shoulder Arthroplasty for Primary Glenohumeral Osteoarthritis: Results of a Multicenter Study with More than Five Years of Follow-Up. J. Bone Jt. Surg. Am. 2012, 94, 685–693. [Google Scholar] [CrossRef]
- Erickson, B.J.; Chalmers, P.N.; Denard, P.; Lederman, E.; Horneff, G.; Werner, B.C.; Provencher, M.T.; Romeo, A.A. Does Commercially Available Shoulder Arthroplasty Preoperative Planning Software Agree with Surgeon Measurements of Version, Inclination, and Subluxation? J. Shoulder Elb. Surg. 2020, 30, 413–420. [Google Scholar] [CrossRef] [PubMed]
- De Wilde, L.F.; Verstraeten, T.; Speeckaert, W.; Karelse, A. Reliability of the Glenoid Plane. J. Shoulder Elb. Surg. 2010, 19, 414–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Parys, M.; Alkiar, O.; Naidoo, N.; Van Tongel, A.; De Wilde, L. 3D Evaluation of the Scapular Morphology in Primary Glenohumeral Arthritis, Rotator Cuff Arthropathy and Asymptomatic Shoulders. J. Shoulder Elb. Surg. 2020, 30, 1803–1810. [Google Scholar] [CrossRef] [PubMed]
- Cabarcas, B.C.; Cvetanovich, G.L.; Espinoza-Orias, A.A.; Inoue, N.; Gowd, A.K.; Bernardoni, E.; Verma, N.N. Novel 3-Dimensionally Printed Patient-Specific Guide Improves Accuracy Compared with Standard Total Shoulder Arthroplasty Guide: A Cadaveric Study. JSES Open Access 2019, 3, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Ricchetti, E.T.; Hendel, M.D.; Collins, D.N.; Iannotti, J.P. Is Premorbid Glenoid Anatomy Altered in Patients with Glenohumeral Osteoarthritis? Clin. Orthop. Relat. Res. 2013, 471, 2932–2939. [Google Scholar] [CrossRef] [Green Version]
- Casier, S.J.; Van den Broecke, R.; Van Houcke, J.; Audenaert, E.; De Wilde, L.F.; Van Tongel, A. Morphologic Variations of the Scapula in 3-Dimensions: A Statistical Shape Model Approach. J. Shoulder Elb. Surg. 2018, 27, 2224–2231. [Google Scholar] [CrossRef]
- Walker, K.E.; Simcock, X.C.; Jun, B.J.; Iannotti, J.P.; Ricchetti, E.T. Progression of Glenoid Morphology in Glenohumeral Osteoarthritis. J. Bone Jt. Surg. Am. 2018, 100, 49–56. [Google Scholar] [CrossRef]
- Plessers, K.; Verhaegen, F.; Dijck, C.V.; Wirix-Speetjens, R.; Debeer, P.; Jonkers, I.; Sloten, J.V. Automated Quantification of Glenoid Bone Defects Using 3-Dimensional Measurements. J. Shoulder Elb. Surg. 2020, 29, 1050–1058. [Google Scholar] [CrossRef]
- Shukla, D.R.; McLaughlin, R.J.; Lee, J.; Nguyen, N.T.V.; Sanchez-Sotelo, J. Automated Three-Dimensional Measurements of Version, Inclination, and Subluxation. Shoulder Elb. 2019, 12, 31–37. [Google Scholar] [CrossRef]
- Jacquot, A.; Gauci, M.-O.; Urvoy, M.; de Casson, F.B.; Berhouet, J.; Letissier, H. Anatomical Plane and Transverse Axis of the Scapula: Reliability of Manual Positioning of the Anatomical Landmarks. Shoulder Elb. 2021, 14, 17585732211001756. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years) | 61 ± 17 |
| Men/Women | 26/56 |
| Diagnosis | |
| Normal shoulder | 26 |
| PGHOA | |
| Type A | 11 |
| Type B | 18 |
| Type C | 1 |
| Type D | 1 |
| Massive Rotator Cuff Tear (E0) | 5 |
| Cuff Tear Arthropathy | |
| Type E1 | 5 |
| Type E2 | 2 |
| Type E3 | 4 |
| Post traumatic arthritis | 4 |
| Rhumatoid arthritis | 2 |
| Post-instability | 2 |
| Avascular osteonecrosis | 1 |
| Total | 82 |
| Input Data Name | Definition | Acquisition Method |
|---|---|---|
| Transverse axis | ||
| Y-axis [20] | Best-fit line to all points at the intersection of the scapular spine and the scapular body | Fully Automated |
| Glenoid-Trigonum line [3] | Line through the glenoid center and the trigonum | Need a manual picking |
| Best Line Fossa [5] | Best-fit line to five regular landmarks positioned at the bottom of the supraspinatus fossa | Need a manual picking |
| Transverse Axis | |||
|---|---|---|---|
| Y-Axis | Glenoid-Trigonum Line | Best-Fit Line Fossa | |
| Mean (°) | 6.8 | 8.0 | 8.5 |
| Minimum (°) | −15.0 | −18.5 | −19.5 |
| Maximum (°) | 21.0 | 25.0 | 27.8 |
| Standard Deviation (°) | 6.8 | 6.6 | 7.8 |
| ICC | 95%CI | |
|---|---|---|
| Y-axis (Blueprint software automatic measure) | 1.00 | 1.00; 1.00 |
| Glenoid-Trigonum line | 0.87 | 0.78; 0.92 |
| Best fit line fossa | 0.96 | 0.94; 0.97 |
| Variable Referential | Compared Methods | Linear Coefficient of Correlation | Concordance | |||||
|---|---|---|---|---|---|---|---|---|
| Pearson (r) | Bland & Altman | Lin | ||||||
| r | 95%CI | Mean Biase (°) | 95%CI (°) | CCC | LoP | LoA | ||
| Transverse axis | ||||||||
| Y-axis vs. Glenoid-Trigonum line | 0.89 | (0.84; 0.93) | −1.1 | (−7.2; 4.9) | 0.88 | 88% | 12% | |
| Best-fit Line Fossa vs. Glenoid-Trigonum line | 0.86 | (0.80; 0.91) | 0.6 | (−7.1; 8.3) | 0.85 | 89% | 11% | |
| Y-axis vs. Best-fit Line Fossa | 0.95 | (0.92; 0.97) | −1.7 | (−6.8; 3.4) | 0.91 | 61% | 39% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gauci, M.-O.; Jacquot, A.; Boux de Casson, F.; Deransart, P.; Letissier, H.; Berhouet, J. Glenoid Inclination: Choosing the Transverse Axis Is Critical—A 3D Automated versus Manually Measured Study. J. Clin. Med. 2022, 11, 6050. https://doi.org/10.3390/jcm11206050
Gauci M-O, Jacquot A, Boux de Casson F, Deransart P, Letissier H, Berhouet J. Glenoid Inclination: Choosing the Transverse Axis Is Critical—A 3D Automated versus Manually Measured Study. Journal of Clinical Medicine. 2022; 11(20):6050. https://doi.org/10.3390/jcm11206050
Chicago/Turabian StyleGauci, Marc-Olivier, Adrien Jacquot, François Boux de Casson, Pierric Deransart, Hoël Letissier, and Julien Berhouet. 2022. "Glenoid Inclination: Choosing the Transverse Axis Is Critical—A 3D Automated versus Manually Measured Study" Journal of Clinical Medicine 11, no. 20: 6050. https://doi.org/10.3390/jcm11206050