
Survivorship of Reverse Shoulder Arthroplasty According to Indication, Age and Gender

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Demographics
- -
- 0 to 2 years: 354 shoulders;
- -
- 2 to 5 years: 348 shoulders;
- -
- 5 to 10 years: 661 shoulders;
- -
- 10 to 15 years: 225 shoulders;
- -
- 15+ years: 23 shoulders.
2.3. Surgical Technique
2.4. Statistical Analysis
3. Results
3.1. Postoperative Complications
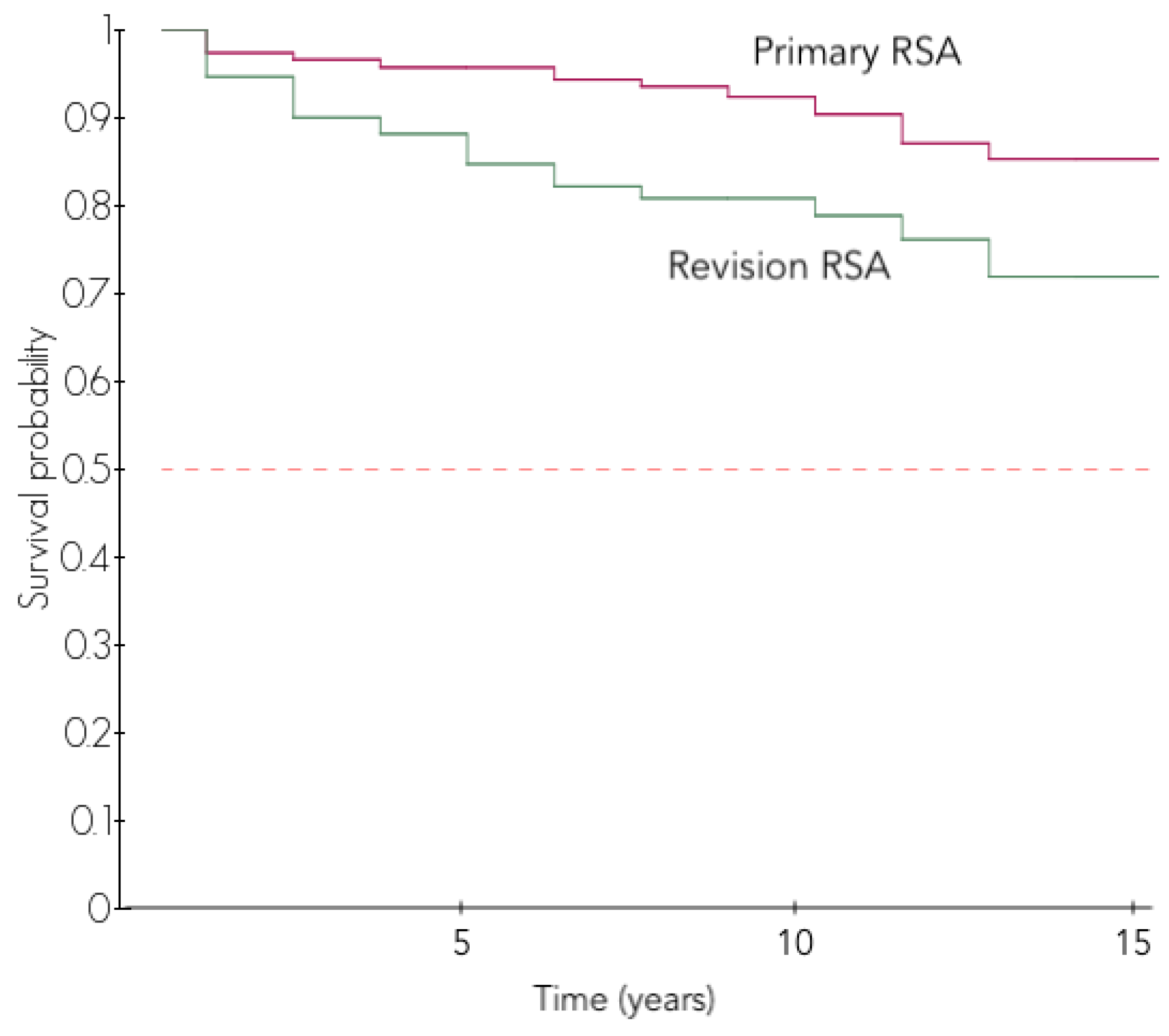
3.2. Survival Analysis
3.3. Predictive Factors for Survival without Revision Surgery
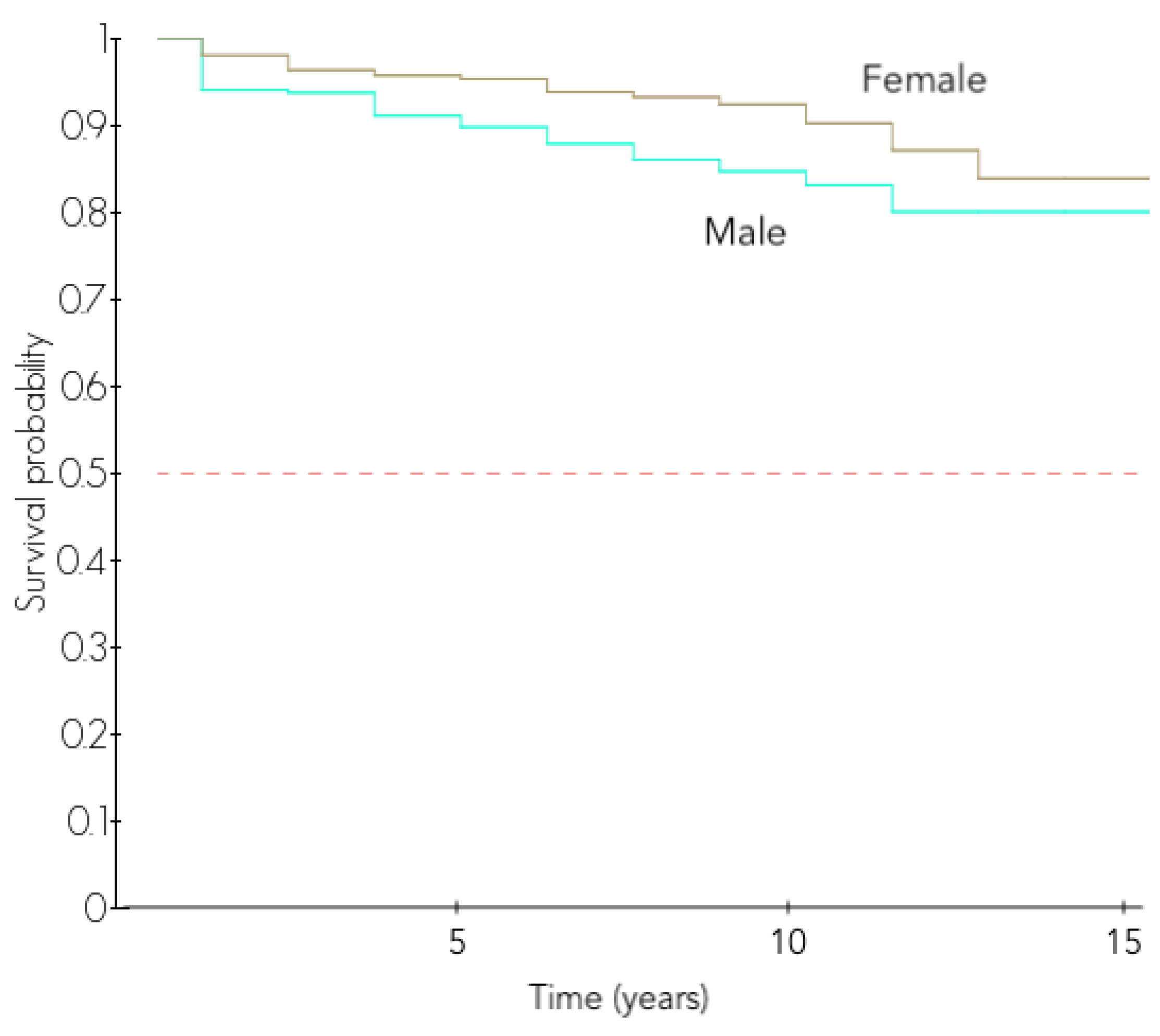
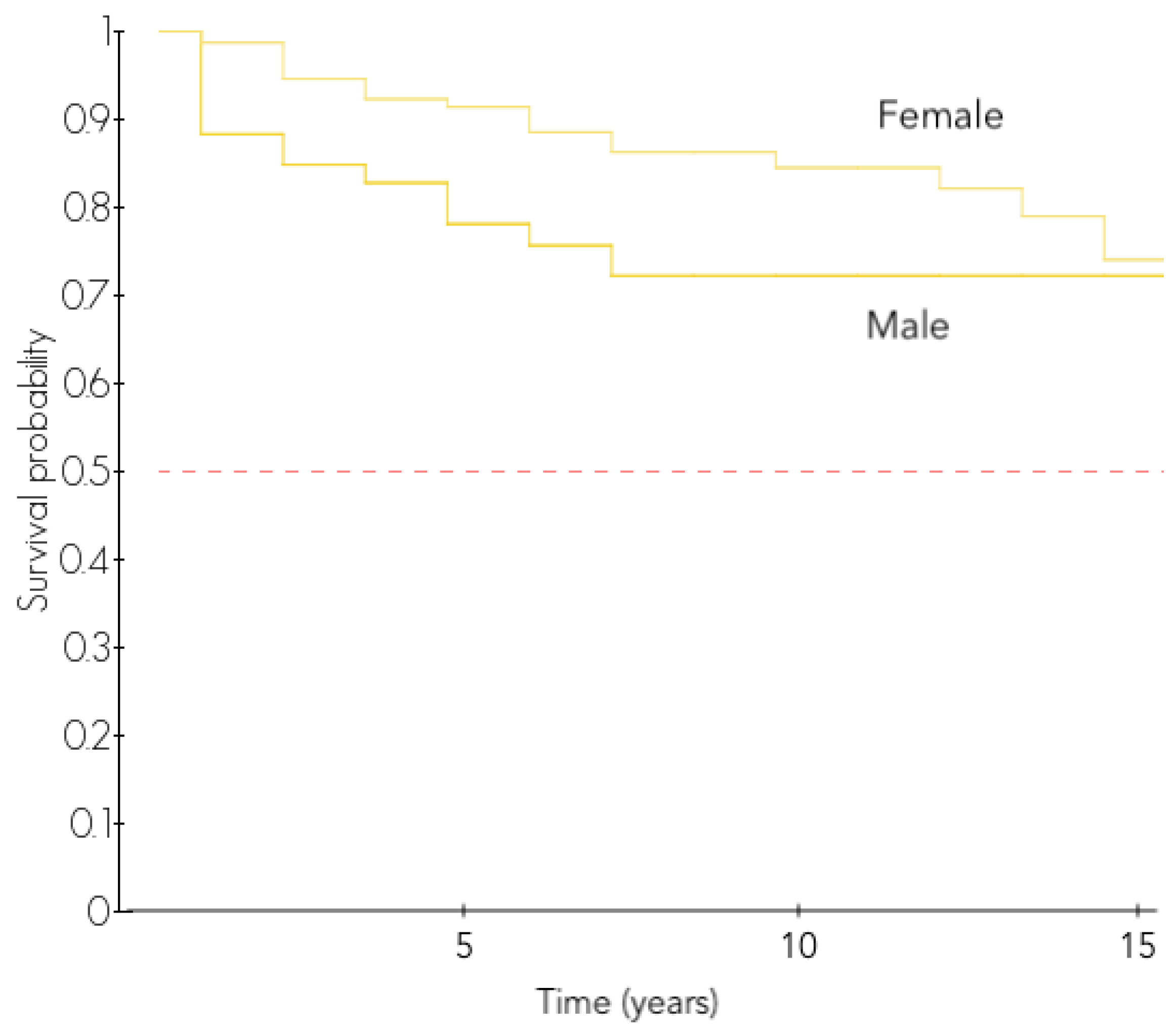
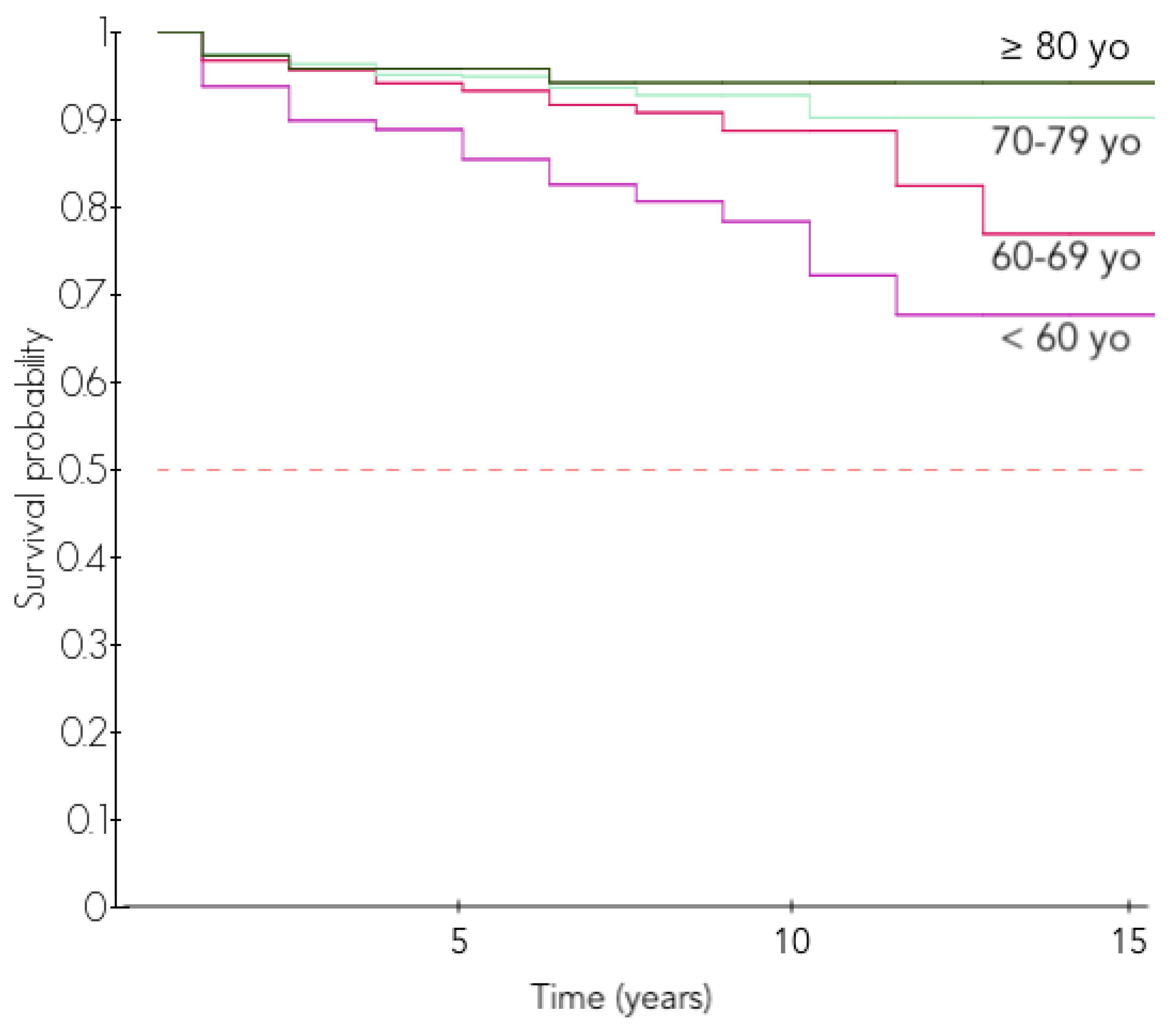
3.3.1. Influence of Gender and Age
3.3.2. Influence of Diagnosis
4. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | N = | Indication | FU (y) | Complication (%) | 5-Year Survival | 10-Year Survival |
|---|---|---|---|---|---|---|
| Bacle [13] | 87 | MCT, CTA, Revision, Post-trauma, POA | 12.5 | 29% | - | 93% |
| Beck [42] | 29 | CTA, FS, Revision | 8.5 | 14% | - | 93% |
| Cuff [30] | 76 | MCT, CTA | 5.1 | - | 94% | - |
| Ek [14] | 46 | MCT, CTA < 65 years | 7.8 | 38% | 98% | 88% |
| Favard [15] | 489 | MCT, CTA, POA | 4.5 | 18% | - | 89% |
| Guery [16] | 60 | MCT, CTA, Revision, Post-trauma, RA | 5.8 | 15% | - | 91% |
| Gallinet [17] | 422 | Acute fracture | 2.3 | 13% | - | 91% |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grammont, P.; Trouilloud, P.; Laffay, J.; Deries, X. Etude et réalisation d’une nouvelle prothèse d’épaule. Rhumatologie 1987, 11, 407–418. [Google Scholar]
- Boileau, P.; Watkinson, D.J.; Hatzidakis, A.M.; Balg, F. Grammont reverse prosthesis: Design, rationale, and biomechanics. J. Shoulder Elb. Surg. 2005, 14, S147–S161. [Google Scholar] [CrossRef] [PubMed]
- Sirveaux, F.; Favard, L.; Oudet, D.; Huquet, D.; Walch, G.; Mole, D. Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff RESULTS OF A MULTICENTRE STUDY OF 80 SHOULDERS. J. Bone Jt. Surg. Br. Vol. 2004, 86, 388–395. [Google Scholar] [CrossRef]
- Favard, L.; Lautmann, S.; Sirveaux, F.; Oudet, D.; Kerjean, Y.; Huguet, D. Hemiarthroplasty versus reverse arthroplasty in the treatment of osteoarthritis with massive rotator cuff tear. In 2000 Shoulder Prostheses. Two to Ten Years Follow-Up; Walch, G., Boileau, P., Molé, D., Eds.; Sauramps Medical: Saintines, France, 2001; pp. 261–268. [Google Scholar]
- Boileau, P.; Watkinson, D.; Hatzidakis, A.M.; Hovorka, I. Neer Award 2005: The Grammont reverse shoulder prosthesis: Results in cuff tear arthritis, fracture sequelae, and revision arthroplasty. J. Shoulder Elb. Surg. 2006, 15, 527–540. [Google Scholar] [CrossRef]
- Wall, B. Reverse Total Shoulder Arthroplasty: A Review of Results According to Etiology. J. Bone Jt. Surg. 2007, 89, 1476. [Google Scholar] [CrossRef]
- Matsen, F.A.; Boileau, P.; Walch, G.; Gerber, C.; Bicknell, R.T. The reverse total shoulder arthroplasty. J. Bone Jt. Surg. Am. 2007, 89, 660–667. [Google Scholar] [CrossRef]
- Lehtimäki, K.; Rasmussen, J.V.; Mokka, J.; Salomonsson, B.; Hole, R.; Jensen, S.L.; Äärimaa, V. Risk and risk factors for revision after primary reverse shoulder arthroplasty for cuff tear arthropathy and osteoarthritis: A Nordic Arthroplasty Register Association study. J. Shoulder Elb. Surg. 2018, 27, 1596–1601. [Google Scholar] [CrossRef]
- Porcellini, G.; Combi, A.; Merolla, G.; Bordini, B.; Stea, S.; Zanoli, G.; Paladini, P. The experience of the RIPO, a shoulder prosthesis registry with 6-year follow-up. Musculoskelet. Surg. 2017, 11, 5291. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, J.V.; Olsen, B.S. The Danish Shoulder Arthroplasty Registry. Obere. Extrem. 2019, 14, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Moeini, S.; Rasmussen, J.V.; Salomonsson, B.; Domeij-Arverud, E.; Fenstad, A.M.; Hole, R.; Jensen, S.L.; Brorson, S. Reverse shoulder arthroplasty has a higher risk of revision due to infection than anatomical shoulder arthroplasty: 17 730 primary shoulder arthroplasties from the nordic arthroplasty register association. Bone Jt. J. 2019, 101-B, 702–707. [Google Scholar] [CrossRef]
- NJR Editorial Board National Joint Registry for England, Wales, Northern Ireland and the Isle of Man—14th Annual Report 2017.pdf 2017. Available online: https://www.hqip.org.uk/wp-content/uploads/pelerous_media_manager/public/253/NJR/NJR%2014th%20Annual%20Report%202017.pdf (accessed on 11 June 2017).
- Bacle, G.; Nové-Josserand, L.; Garaud, P.; Walch, G. Long-Term Outcomes of Reverse Total Shoulder Arthroplasty: A Follow-up of a Previous Study. J. Bone Jt. Surg. Am. 2017, 99, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Ek, E.T.H.; Neukom, L.; Catanzaro, S.; Gerber, C. Reverse total shoulder arthroplasty for massive irreparable rotator cuff tears in patients younger than 65 years old: Results after five to fifteen years. J. Shoulder Elb. Surg. 2013, 22, 1199–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favard, L.; Levigne, C.; Nerot, C.; Gerber, C.; De Wilde, L.; Mole, D. Reverse Prostheses in Arthropathies With Cuff Tear: Are Survivorship and Function Maintained Over Time? Clin. Orthop. Relat. Res. 2011, 469, 2469–2475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guery, J.; Favard, L.; Sirveaux, F.; Oudet, D.; Mole, D.; Walch, G. Reverse total shoulder arthroplasty. Survivorship analysis of eighty replacements followed for five to ten years. J. Bone Jt. Surg. Am. 2006, 88, 1742–1747. [Google Scholar] [CrossRef]
- Gallinet, D.; Cazeneuve, J.-F.; Boyer, E.; Menu, G.; Obert, L.; Ohl, X.; Bonnevialle, N.; Valenti, P.; Boileau, P. Reverse shoulder arthroplasty for recent proximal humerus fractures: Outcomes in 422 cases. Orthop. Traumatol. Surg. Res. 2019, 19, S1877056819301835. [Google Scholar] [CrossRef]
- Cuff, D.; Clark, R.; Pupello, D.; Frankle, M. Reverse shoulder arthroplasty for the treatment of rotator cuff deficiency: A concise follow-up, at a minimum of five years, of a previous report. J. Bone Jt. Surg. Am. 2012, 94, 1996–2000. [Google Scholar] [CrossRef]
- Davidson, M.D.; Tomkins, A.; Rainbird, D.S.; Morris, R. Australian orthopaedic association national joint replacement registry. Med. J. Aust. 2004, 180, S31–S34. [Google Scholar]
- Zumstein, M.A.; Pinedo, M.; Old, J.; Boileau, P. Problems, complications, reoperations, and revisions in reverse total shoulder arthroplasty: A systematic review. J. Shoulder Elb. Surg. 2011, 20, 146–157. [Google Scholar] [CrossRef]
- Gregory, T.M.; Boukebous, B.; Gregory, J.; Pierrart, J.; Masemjean, E. Short, Medium and Long Term Complications After Total Anatomical Shoulder Arthroplasty. Open Orthop. J. 2017, 11, 1133–1141. [Google Scholar] [CrossRef]
- Bohsali, K.I.; Bois, A.J.; Wirth, M.A. Complications of Shoulder Arthroplasty. J. Bone Jt. Surg. 2017, 99, 256–269. [Google Scholar] [CrossRef]
- Ascione, F.; Domos, P.; Guarrella, V.; Chelli, M.; Boileau, P.; Walch, G. Long-term humeral complications after Grammont-style reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2018, 27, 1065–1071. [Google Scholar] [CrossRef] [PubMed]
- Groh, G.I.; Groh, G.M. Complications rates, reoperation rates, and the learning curve in reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2014, 23, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, B.M.; Chalmers, P.N.; Gupta, A.K.; Romeo, A.A.; Nicholson, G.P. Complication rates comparing primary with revision reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2014, 23, 1647–1654. [Google Scholar] [CrossRef] [PubMed]
- Greiner, S.; Uschok, S.; Herrmann, S.; Gwinner, C.; Perka, C.; Scheibel, M. The metaphyseal bone defect predicts outcome in reverse shoulder arthroplasty for proximal humerus fracture sequelae. Arch. Orthop. Trauma Surg. 2014, 134, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Raiss, P.; Edwards, T.B.; da Silva, M.R.; Bruckner, T.; Loew, M.; Walch, G. Reverse shoulder arthroplasty for the treatment of nonunions of the surgical neck of the proximal part of the humerus (type-3 fracture sequelae). J. Bone Jt. Surg. Am. 2014, 96, 2070–2076. [Google Scholar] [CrossRef] [Green Version]
- Teunis, T.; Nota, S.P.F.T.; Hornicek, F.J.; Schwab, J.H.; Lozano-Calderón, S.A. Outcome After Reconstruction of the Proximal Humerus for Tumor Resection: A Systematic Review. Clin. Orthop. Relat. Res. 2014, 472, 2245–2253. [Google Scholar] [CrossRef] [Green Version]
- Grey, B.; Rodseth, R.N.; Roche, S.J. Humeral Stem Loosening Following Reverse Shoulder Arthroplasty: A Systematic Review and Meta-Analysis. JBJS Rev. 2018, 1, 129. [Google Scholar] [CrossRef]
- Cuff, D.; Levy, J.C.; Gutiérrez, S.; Frankle, M.A. Torsional stability of modular and non-modular reverse shoulder humeral components in a proximal humeral bone loss model. J. Shoulder Elb. Surg. 2011, 20, 646–651. [Google Scholar] [CrossRef]
- Collin, P.; Hervé, A.; Walch, G.; Boileau, P.; Muniandy, M.; Chelli, M. Mid-term results of reverse shoulder arthroplasty for glenohumeral osteoarthritis with posterior glenoid deficiency and humeral subluxation. J. Shoulder Elb. Surg. 2019, 10, 32. [Google Scholar] [CrossRef]
- Wright, M.A.; Keener, J.D.; Chamberlain, A.M. Comparison of Clinical Outcomes After Anatomic Total Shoulder Arthroplasty and Reverse Shoulder Arthroplasty in Patients 70 Years and Older With Glenohumeral Osteoarthritis and an Intact Rotator Cuff. J. Am. Acad. Orthop. Surg. 2019, 1, 166. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Wanderman, N.R.; Assenmacher, A.T.; Sperling, J.W.; Cofield, R.H.; Sánchez-Sotelo, J. Anatomic total shoulder arthroplasty with posterior capsular plication versus reverse shoulder arthroplasty in patients with biconcave glenoids: A matched cohort study. J. Orthop. Surg. 2018, 26, 230949901876857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlow, J.D.; Yuan, B.J.; Schleck, C.D.; Harmsen, W.S.; Cofield, R.H.; Sperling, J.W. Shoulder arthroplasty for rheumatoid arthritis: 303 consecutive cases with minimum 5-year follow-up. J. Shoulder Elb. Surg. 2014, 23, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Collins, D.N.; Harryman, D.T.; Wirth, M.A. Shoulder arthroplasty for the treatment of inflammatory arthritis. J. Bone Jt. Surg. Am. 2004, 86, 2489–2496. [Google Scholar] [CrossRef]
- Lévigne, C.; Franchesci, J. Rheumatoid shoulder. Radiographic forms and results of shoulder arthroplasty. About 50 cases. In Shoulder Arthroplasty; Springer: Berlin/Heidelberg, Germany, 1999; pp. 221–230. [Google Scholar]
- Leathers, M.P.; Ialenti, M.N.; Feeley, B.T.; Zhang, A.L.; Ma, C.B. Do younger patients have better results after reverse total shoulder arthroplasty? J. Shoulder Elb. Surg. 2018, 11, 14. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.J.; Wright, T.W.; Farmer, K.W.; Struk, A.M.; Vasilopoulos, T.; King, J.J. Outcomes of Primary Reverse Total Shoulder Arthroplasty in Patients Younger Than 65 Years Old. J. Hand Surg. 2019, 44, 104–111. [Google Scholar] [CrossRef]
- Chelli, M. Reverse shoulder arthroplasty in patients aged 65 years or younger: A systematic review of the literature. JSES Open Access 2019, 6, 119. [Google Scholar] [CrossRef]
- Fevang, B.-T.S.; Lie, S.A.; Havelin, L.I.; Skredderstuen, A.; Furnes, O. Risk factors for revision after shoulder arthroplasty: 1825 shoulder arthroplasties from the Norwegian Arthroplasty Register. Acta Orthop. 2009, 80, 83–91. [Google Scholar] [CrossRef]
- Singh, J.A.; Sperling, J.W.; Schleck, C.; Harmsen, W.S.; Cofield, R.H. Periprosthetic infections after total shoulder arthroplasty: A 33-year perspective. J. Shoulder Elb. Surg. 2012, 21, 1534–1541. [Google Scholar] [CrossRef] [Green Version]
- Beck, S.; Patsalis, T.; Busch, A.; Dittrich, F.; Dudda, M.; Jäger, M.; Wegner, A. Long-Term Results of the Reverse Total Evolutive Shoulder System (TESS). Arch. Orthop. Trauma Surg. 2019, 139, 1039–1044. [Google Scholar] [CrossRef]




| Diagnosis | Frequency |
|---|---|
| Cuff Tear Arthropathy (Hamada IV and V) | 497 (30.9%) |
| Revision of a Failed Arthroplasty, including: | 239 (14.8%) |
| Revision of Hemi-Arthroplasty | 138 (8.5%) |
| Revision of Anatomic Shoulder Arrthroplasty | 85 (5.2%) |
| Revision of Reverse Shoulder Arrthroplasty | 16 (1%) |
| Massive Cuff Tear (Hamada I, II, and III) | 188 (11.7%) |
| Proximal Humerus Fracture Sequelae | 185 (11.5%) |
| Failed Cuff Repair | 153 (9.5%) |
| Primary Osteoarthritis | 142 (8.9%) |
| Acute Proximal Humerus Fracture | 84 (5.2%) |
| Rheumatoid Arthritis | 53 (3.3%) |
| Malignant Tumor | 25 (1.6%) |
| Instability Arthropathy | 22 (1.4%) |
| Other (septic arthritis, osteonecrosis) | 24 (1.5%) |
| Complication | Frequency | Mean Delay (mo.) | Surgical Treatment |
|---|---|---|---|
| Infection | 61 (3.8%) | 26.3 (±28.4) (0.6–112) | Washout (21) Explantation (12) Two-stage exchange (10) One-stage exchange (8) Washout + Mobile implant change (4) Glenoid component revision (2) Revision to HA (1) |
| Instability | 45 (2.8%) | 19.2 (±32.7) (0–139) | Open reduction + Mobile implant change (17) Closed reduction (16) Open reduction without implant change (5) Humeral component revision (2) Glenoid component revision (2) One-stage RSA exchange (2) Revision to HA (1) |
| Glenoid loosening | 25 (1.6%) | 45.5 (±52.3) (0.4–154) | Revision to HA (9) Glenoid component revision (7) One-stage RSA exchange (5) Explantation (1) |
| Humeral loosening | 23 (1.4%) | 62.8 (±55.1) (9–180) | Humeral component revision (9) One-stage RSA exchange (5) |
| Humeral fracture | 23 (1.4%) | 49.5 (±38.1) (0.1–121) | Open reduction and internal fixation (11) Humeral component revision (3) |
| Nerve injury | 22 (1.4%) | - | - |
| Scapular spine fracture | 11 (0.7%) | 47.4 (±66.4) (1–167) | Open reduction and internal fixation (2) |
| Acromial fracture | 6 (0.4%) | 2.1 (±1.3) (1–4) | - |
| Severe stiffness | 4 (0.3%) | - | Arthroscopic arthrolysis (3) Humeral component revision (1) |
| Primary RSA n = 1282 | Revision RSA for Failed Arthroplasty n = 329 | p-Value for the Difference between Primary and Revision RSA | |
|---|---|---|---|
| Reoperation-free survival (%) | |||
| 5-year | 97.3 (96–98) | 93.2 (89–96) | 0.002 * |
| 10-year | 95.3 (93–97) | 89.9 (84–94) | |
| 15-year | 94.1 (91–96) | 89.9 (84–94) | |
| Revision-free survival (%) | |||
| 5-year | 95.8 (94–97) | 84.3 (78–89) | <0.001 * |
| 10-year | 91.0 (88–93) | 80.4 (74–86) | |
| 15-year | 85.3 (79–90) | 71.5 (58–81) | |
| N = | Complication Rate (%) | Reoperation Rate (%) | Revision Rate (%) | 5-Year Revision-Free Survival | 10-Year Revision Free Survival | |
|---|---|---|---|---|---|---|
| Gender | ||||||
| Male | 402 | 23.1 | 6.7 | 10.4 | 90.3 | 83.2 |
| Female | 1207 | 14.2 | 3.0 | 5.6 | 95.4 | 91.5 |
| p-Value | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | |
| Age at RSA | ||||||
| <60 years | 118 | 34.7 | 8.5 | 19.5 | 86.7 | 75.7 |
| 60–69 years | 327 | 20.5 | 3.7 | 9.5 | 93.3 | 88.8 |
| 70–79 years | 830 | 14.5 | 3.9 | 5.4 | 95.0 | 91.3 |
| ≥80 years | 331 | 11.5 | 3.0 | 3.3 | 95.9 | 94.3 |
| p-Value | <0.001 * | 0.068 | <0.001 * | <0.001 * | <0.001 * | |
| Revision Rate (%) | <60 Years (n = 118) | 60–69 Years (n = 327) | 70–79 Years (n = 830) | ≥80 Years (n = 331) | p-Value According to Age |
|---|---|---|---|---|---|
| All RSA (n = 1611) | |||||
| Women (n = 1207) | 14.3 | 9.0 | 4.5 | 2.9 | <0.001 * |
| Men (n = 404) | 26.5 | 10.4 | 8.5 | 3.5 | <0.001 * |
| p-Value (according to gender) | 0.096 | 0.701 | 0.034 * | 0.817 | |
| Revision RSA (n = 238) | |||||
| Women (n = 168) | 20.0 | 19.6 | 5.5 | 17.4 | 0.078 |
| Men (n = 70) | 36.4 | 18.2 | 18.2 | 0 | 0.261 |
| p-Value (according to gender) | 0.314 | 1 | 0.087 | 1 | |
| Complication Rate (%) | Reoperation Rate (%) | Revision Rate (%) | 5-Year Revision-Free Survival | 10-Year Revision Free Survival | |
|---|---|---|---|---|---|
| Revision RSA | 32.6 | 8.0 | 16.0 | 84.8 | 80.9 |
| Revision of HA | 32.8 | 7.3 | 13.9 | 86.8 | 83.2 |
| Revision of ATSA | 25 | 8.3 | 11.9 | 87.8 | 83.3 |
| Revision of RSA | 66.7 | 11.1 | 55.6 | 50.0 | 50.0 |
| CTA (Hamada IV and V) | 12.3 | 2.8 | 5.0 | 95.7 | 91.9 |
| MCT (Hamada I, II, and III) | 17.6 | 5.9 | 3.7 | 96.4 | 95.3 |
| Fracture Sequelae | 20.0 | 3.8 | 10.8 | 92.9 | 83.9 |
| Failed Cuff Repair | 11.8 | 3.9 | 3.3 | 96.1 | 96.1 |
| Primary Osteoarthritis | 8.5 | 0.7 | 3.5 | 97.5 | 90.3 |
| Acute Fracture | 6.0 | 1.2 | 2.4 | 98.7 | 88.9 |
| Rheumatoid Arthritis | 9.4 | 0.0 | 1.9 | 97.6 | 97.6 |
| Tumor | 56 | 12.0 | 20.0 | 86.2 | 59.1 |
| Instability Arthropathy | 4.5 | 4.5 | 0.0 | 100.0 | 100.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chelli, M.; Boileau, P.; Domos, P.; Clavert, P.; Berhouet, J.; Collin, P.; Walch, G.; Favard, L. Survivorship of Reverse Shoulder Arthroplasty According to Indication, Age and Gender. J. Clin. Med. 2022, 11, 2677. https://doi.org/10.3390/jcm11102677
Chelli M, Boileau P, Domos P, Clavert P, Berhouet J, Collin P, Walch G, Favard L. Survivorship of Reverse Shoulder Arthroplasty According to Indication, Age and Gender. Journal of Clinical Medicine. 2022; 11(10):2677. https://doi.org/10.3390/jcm11102677
Chicago/Turabian StyleChelli, Mikaël, Pascal Boileau, Peter Domos, Philippe Clavert, Julien Berhouet, Philippe Collin, Gilles Walch, and Luc Favard. 2022. "Survivorship of Reverse Shoulder Arthroplasty According to Indication, Age and Gender" Journal of Clinical Medicine 11, no. 10: 2677. https://doi.org/10.3390/jcm11102677