

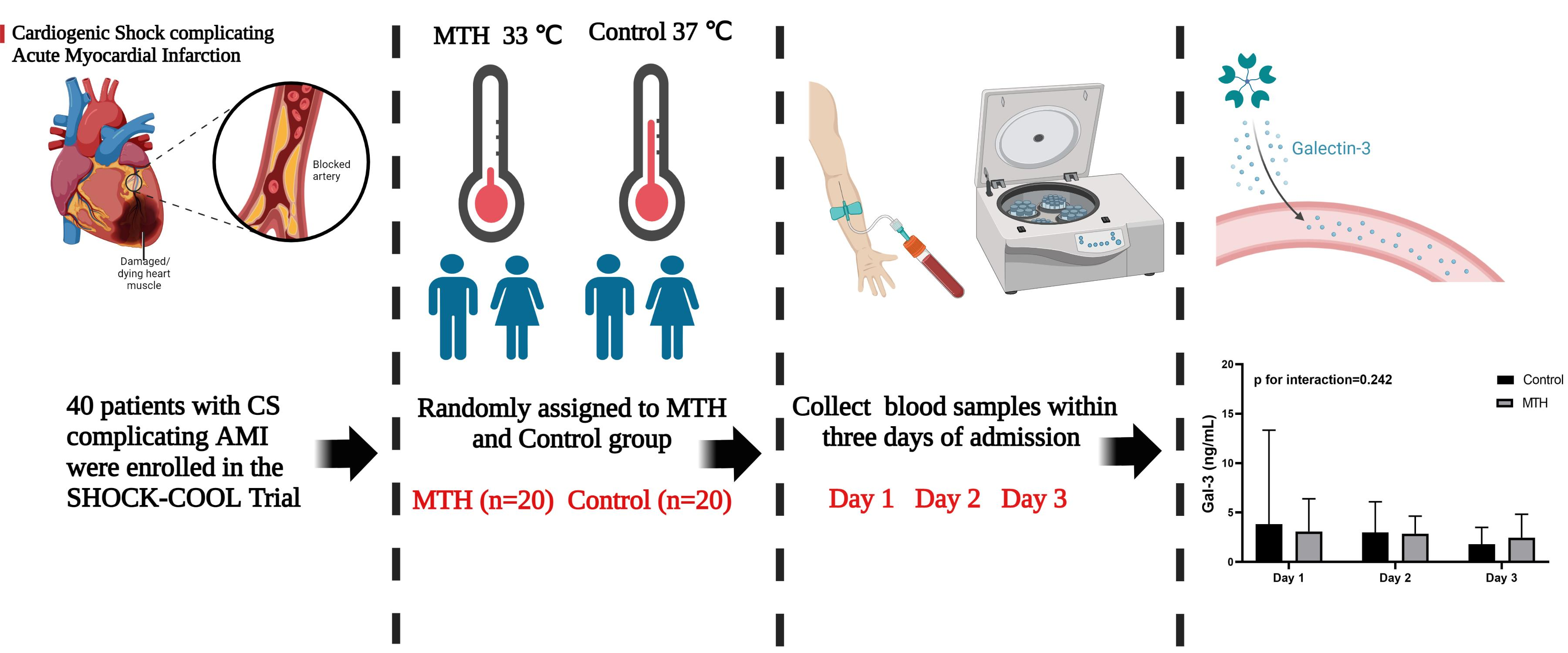
Circulating Galectin-3 in Patients with Cardiogenic Shock Complicating Acute Myocardial Infarction Treated with Mild Hypothermia: A Biomarker Sub-Study of the SHOCK-COOL Trial
 , , and
, , and
Abstract
:
1. Introduction
2. Methods
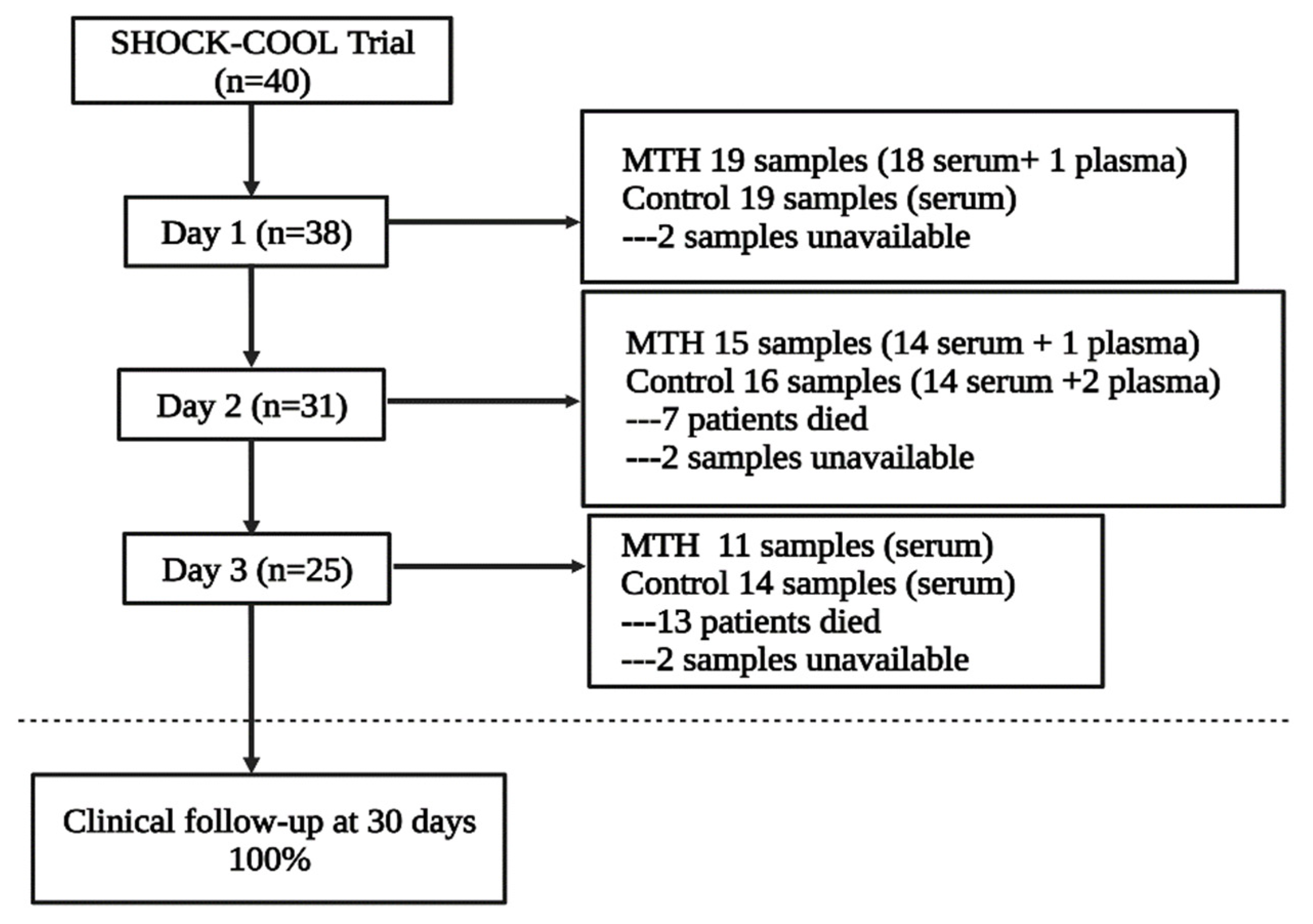
2.1. Patients and Study Design
2.2. Laboratory Measurements
2.3. Statistical Analysis
3. Results
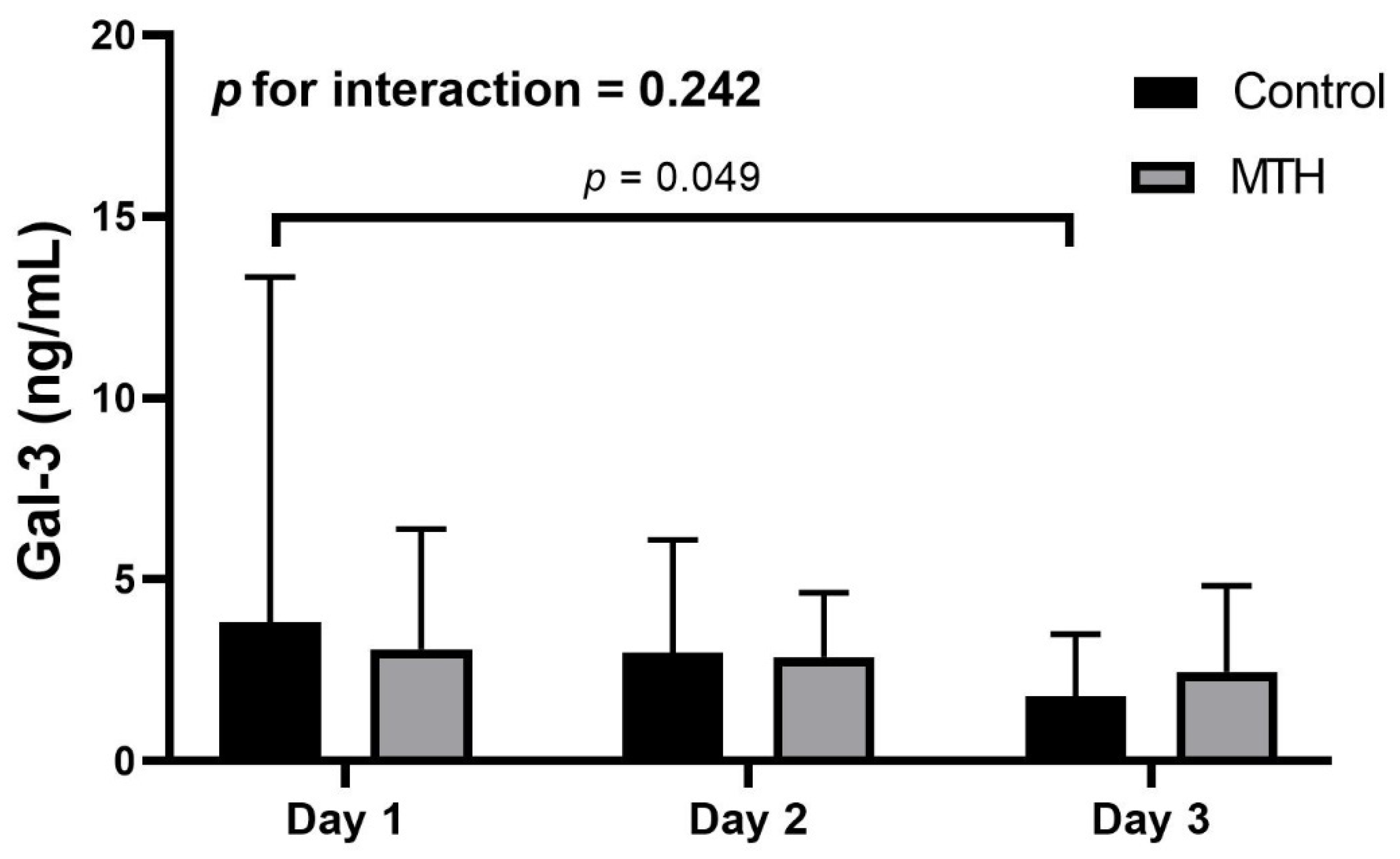
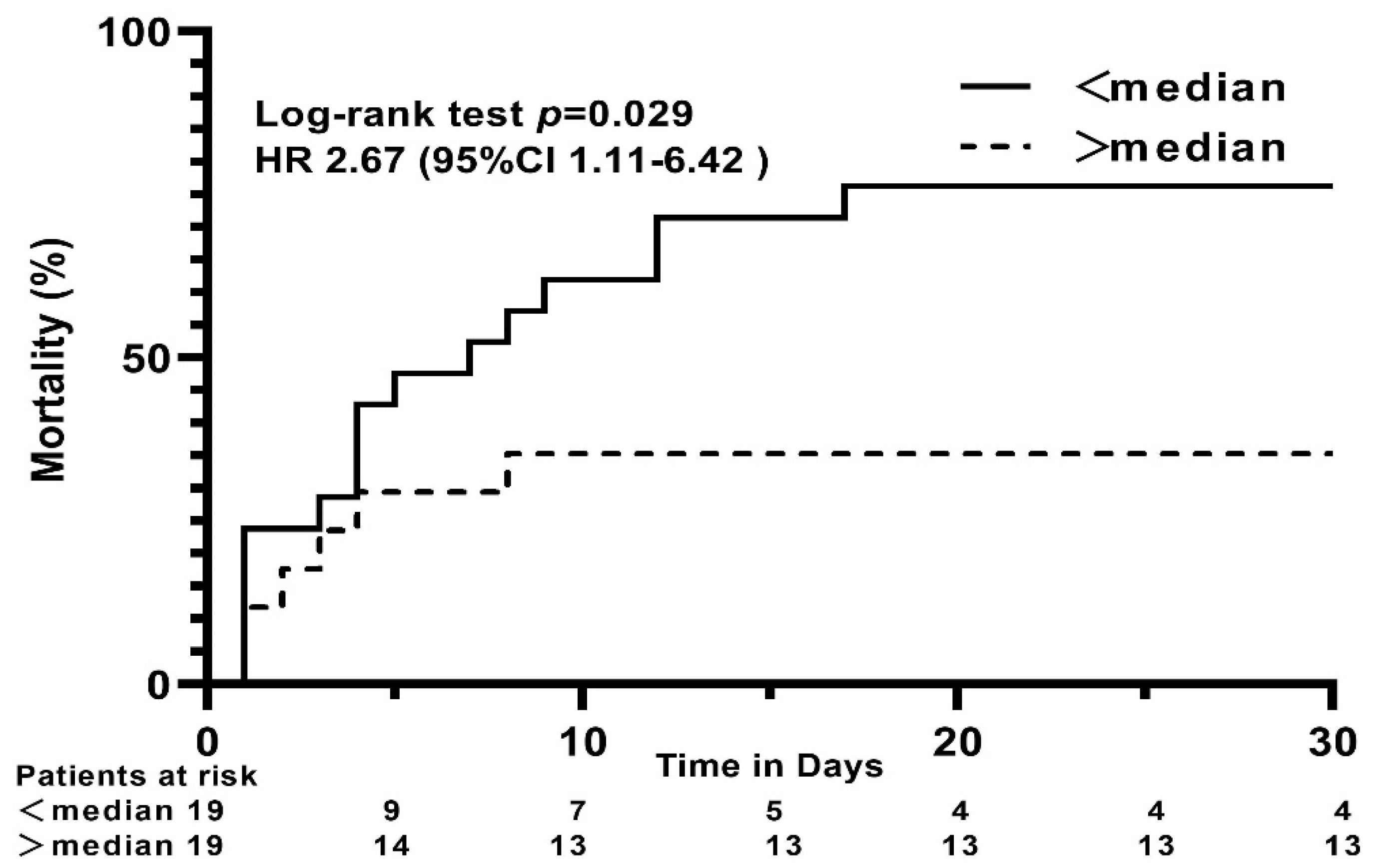
Gal-3 Levels in MTH and Control Groups
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thiele, H.; Ohman, E.M.; Waha-Thiele, S.; de Zeymer, U.; Desch, S. Management of cardiogenic shock complicating myocardial infarction: An update 2019. Eur. Heart J. 2019, 40, 2671–2683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, A.H.; Puri, R.; Kalra, A. Management of cardiogenic shock complicating acute myocardial infarction: A review. Clin. Cardiol. 2019, 42, 484–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapur, N.K.; Thayer, K.L.; Zweck, E. Cardiogenic Shock in the Setting of Acute Myocardial Infarction. Methodist Debakey Cardiovasc. J. 2020, 16, 16–21. [Google Scholar] [CrossRef]
- Kolte, D.; Khera, S.; Aronow, W.S.; Mujib, M.; Palaniswamy, C.; Sule, S.; Jain, D.; Gotsis, W.; Ahmed, A.; Frishman, W.H.; et al. Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States. J. Am. Heart Assoc. 2014, 3, e000590. [Google Scholar] [CrossRef] [Green Version]
- Barcan, A.; Suciu, Z.; Rapolti, E. Monitoring Acute Myocardial Infarction Complicated with Cardiogenic Shock—From the Emergency Room to Coronary Care Units. J. Cardiovasc. Emergencies 2017, 3, 61–71. [Google Scholar] [CrossRef] [Green Version]
- Fang, L.; Moore, X.-L.; Dart, A.M.; Wang, L.-M. Systemic inflammatory response following acute myocardial infarction. J. Geriatr. Cardiol. 2015, 12, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Fuernau, G.; Beck, J.; Desch, S.; Eitel, I.; Jung, C.; Erbs, S.; Mangner, N.; Lurz, P.; Fengler, K.; Jobs, A.; et al. Mild Hypothermia in Cardiogenic Shock Complicating Myocardial Infarction. Circulation 2019, 139, 448–457. [Google Scholar] [CrossRef]
- Shi, J.; Dai, W.; Kloner, R.A. Therapeutic Hypothermia Reduces the Inflammatory Response Following Ischemia/Reperfusion Injury in Rat Hearts. Hypothermia Temp. Manag. 2017, 7, 162–170. [Google Scholar] [CrossRef]
- Diestel, A.; Roessler, J.; Berger, F.; Schmitt, K.R.L. Hypothermia downregulates inflammation but enhances IL-6 secretion by stimulated endothelial cells. Cryobiology 2008, 57, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Shao, Z.-H.; Chang, W.-T.; Chan, K.C.; Wojcik, K.R.; Hsu, C.-W.; Li, C.-Q.; Li, J.; Anderson, T.; Qin, Y.; Becker, L.B.; et al. Hypothermia-induced cardioprotection using extended ischemia and early reperfusion cooling. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, H1995–H2003. [Google Scholar] [CrossRef]
- van der Pals, J.; Götberg, M.I.; Götberg, M.; Hultén, L.M.; Magnusson, M.; Jern, S.; Erlinge, D. Hypothermia in cardiogenic shock reduces systemic t-PA release. J. Thromb. Thrombolysis 2011, 32, 72–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibarrola, J.; Matilla, L.; Martínez-Martínez, E.; Gueret, A.; Fernández-Celis, A.; Henry, J.-P.; Nicol, L.; Jaisser, F.; Mulder, P.; Ouvrard-Pascaud, A.; et al. Myocardial Injury After Ischemia/Reperfusion Is Attenuated By Pharmacological Galectin-3 Inhibition. Sci. Rep. 2019, 9, 9607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, R.Y.; Hill, P.N.; Hsu, D.K.; Liu, F.T. Role of the carboxyl-terminal lectin domain in self-association of galectin-3. Biochemistry 1998, 37, 4086–4092. [Google Scholar] [CrossRef] [PubMed]
- Al-Salam, S.; Hashmi, S. Myocardial Ischemia Reperfusion Injury: Apoptotic, Inflammatory and Oxidative Stress Role of Galectin-3. Cell Physiol. Biochem. 2018, 50, 1123–1139. [Google Scholar] [CrossRef]
- Salvagno, G.L.; Pavan, C. Prognostic biomarkers in acute coronary syndrome. Ann. Transl. Med. 2016, 4, 258. [Google Scholar] [CrossRef] [Green Version]
- Dong, R.; Zhang, M.; Hu, Q.; Zheng, S.; Soh, A.; Zheng, Y.; Yuan, H. Galectin-3 as a novel biomarker for disease diagnosis and a target for therapy (Review). Int. J. Mol. Med. 2018, 41, 599–614. [Google Scholar] [CrossRef] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.J.R.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll Cardiol. 2017, 70, 776–803. [Google Scholar] [CrossRef]
- Park, S.-Y.; Freedman, N.D.; Haiman, C.A.; Le Marchand, L.; Wilkens, L.R.; Setiawan, V.W. Association of Coffee Consumption With Total and Cause-Specific Mortality Among Nonwhite Populations. Ann. Intern. Med. 2017, 167, 228–235. [Google Scholar] [CrossRef]
- Arrich, J. Clinical application of mild therapeutic hypothermia after cardiac arrest. Crit Care Med. 2007, 35, 1041–1047. [Google Scholar] [CrossRef]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef]
- Li, M.; Yuan, Y.; Guo, K.; Lao, Y.; Huang, X.; Feng, L. Value of Galectin-3 in Acute Myocardial Infarction. Am. J. Cardiovasc. Drugs 2020, 20, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Boer, R.A.; de van Veldhuisen, D.J.; Gansevoort, R.T.; Muller Kobold, A.C.; van Gilst, W.H.; Hillege, H.L.; Bakker, S.J.L.; van der Harst, P. The fibrosis marker galectin-3 and outcome in the general population. J. Intern. Med. 2012, 272, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Lok, D.J.; Lok, S.I.; Bruggink-André de la Porte Pieta, W.; Badings, E.; Lipsic, E.; van Wijngaarden, J.; Boer, R.A.; de van Veldhuisen, D.J.; van der Meer, P. Galectin-3 is an independent marker for ventricular remodeling and mortality in patients with chronic heart failure. Clin. Res. Cardiol. 2013, 102, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Agnello, L.; Bivona, G.; Lo Sasso, B.; Scazzone, C.; Bazan, V.; Bellia, C.; Ciaccio, M. Galectin-3 in acute coronary syndrome. Clin. Biochem. 2017, 50, 797–803. [Google Scholar] [CrossRef]
- Bivona, G.; Bellia, C.; Lo Sasso, B.; Agnello, L.; Scazzone, C.; Novo, G.; Ciaccio, M. Short-term Changes in Gal 3 Circulating Levels After Acute Myocardial Infarction. Arch. Med. Res. 2016, 47, 521–525. [Google Scholar] [CrossRef]
- Polderman, K.H. Application of therapeutic hypothermia in the intensive care unit. Opportunities and pitfalls of a promising treatment modality--Part 2: Practical aspects and side effects. Intensive Care Med. 2004, 30, 757–769. [Google Scholar] [CrossRef]
- Nishimura, Y.; Naito, Y.; Nishioka, T.; Okamura, Y. The effects of cardiac cooling under surface-induced hypothermia on the cardiac function in the in situ heart. Interact. Cardiovasc. Thorac. Surg. 2005, 4, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Hamamoto, H.; Sakamoto, H.; Leshnower, B.G.; Parish, L.M.; Kanemoto, S.; Hinmon, R.; Plappert, T.; Miyamoto, S.; St John-Sutton, M.G.; Gorman, J.H.; et al. Very mild hypothermia during ischemia and reperfusion improves postinfarction ventricular remodeling. Ann. Thorac. Surg. 2009, 87, 172–177. [Google Scholar] [CrossRef] [Green Version]
- Stegman, B.M.; Newby, L.K.; Hochman, J.S.; Ohman, E.M. Post-myocardial infarction cardiogenic shock is a systemic illness in need of systemic treatment: Is therapeutic hypothermia one possibility? J. Am. Coll Cardiol. 2012, 59, 644–647. [Google Scholar] [CrossRef] [Green Version]
- Mohammad, M.A.; Noc, M.; Lang, I.; Holzer, M.; Clemmensen, P.; Jensen, U.; Metzler, B.; Erlinge, D. Proteomics in Hypothermia as Adjunctive Therapy in Patients with ST-Segment Elevation Myocardial Infarction: A CHILL-MI Substudy. Hypothermia Temp. Manag. 2017, 7, 152–161. [Google Scholar] [CrossRef]
- Hara, A.; Niwa, M.; Noguchi, K.; Kanayama, T.; Niwa, A.; Matsuo, M.; Hatano, Y.; Tomita, H. Galectin-3 as a Next-Generation Biomarker for Detecting Early Stage of Various Diseases. Biomolecules 2020, 10, 389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satoh, K.; Niwa, M.; Goda, W.; Binh, N.H.; Nakashima, M.; Takamatsu, M.; Hara, A. Galectin-3 expression in delayed neuronal death of hippocampal CA1 following transient forebrain ischemia, and its inhibition by hypothermia. Brain Res. 2011, 1382, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.Q.; Ochieng, J. Rapid release of intracellular galectin-3 from breast carcinoma cells by fetuin. Cancer Res. 2001, 61, 1869–1873. [Google Scholar] [PubMed]
- Hildebrand, F.; van Griensven, M.; Giannoudis, P.; Luerig, A.; Harwood, P.; Harms, O.; Fehr, M.; Krettek, C.; Pape, H.-C. Effects of hypothermia and re-warming on the inflammatory response in a murine multiple hit model of trauma. Cytokine 2005, 31, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Bisschops, L.L.A.; van der Hoeven Johannes, G.; Mollnes, T.E.; Hoedemaekers, C.W.E. Seventy-two hours of mild hypothermia after cardiac arrest is associated with a lowered inflammatory response during rewarming in a prospective observational study. Crit Care 2014, 18, 546. [Google Scholar] [CrossRef] [PubMed]
- Bisschops, L.L.A.; Hoedemaekers, C.W.E.; Mollnes, T.E.; van der Hoeven Johannes, G. Rewarming after hypothermia after cardiac arrest shifts the inflammatory balance. Crit Care Med. 2012, 40, 1136–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yalta, K.; Yilmaz, M.B.; Yalta, T.; Palabiyik, O.; Taylan, G.; Zorkun, C. Late Versus Early Myocardial Remodeling After Acute Myocardial Infarction: A Comparative Review on Mechanistic Insights and Clinical Implications. J. Cardiovasc. Pharm. 2020, 25, 15–26. [Google Scholar] [CrossRef]
- Suthahar, N.; Meijers, W.C.; Silljé, H.H.W.; Ho, J.E.; Liu, F.-T.; de Boer, R.A. Galectin-3 Activation and Inhibition in Heart Failure and Cardiovascular Disease: An Update. Theranostics 2018, 8, 593–609. [Google Scholar] [CrossRef]
- González, G.E.; Cassaglia, P.; Noli Truant, S.; Fernández, M.M.; Wilensky, L.; Volberg, V.; Malchiodi, E.L.; Morales, C.; Gelpi, R.J. Galectin-3 is essential for early wound healing and ventricular remodeling after myocardial infarction in mice. Int. J. Cardiol. 2014, 176, 1423–1425. [Google Scholar] [CrossRef]
- Hashmi, S.; Al-Salam, S. Galectin-3 is expressed in the myocardium very early post-myocardial infarction. Cardiovasc. Pathol. 2015, 24, 213–223. [Google Scholar] [CrossRef]
- Matarrese, P.; Tinari, N.; Semeraro, M.L.; Natoli, C.; Iacobelli, S.; Malorni, W. Galectin-3 overexpression protects from cell damage and death by influencing mitochondrial homeostasis. FEBS Lett. 2000, 473, 311–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuernau, G.; Poenisch, C.; Eitel, I.; Waha, S.; de Desch, S.; Schuler, G.; Adams, V.; Werdan, K.; Zeymer, U.; Thiele, H. Growth-differentiation factor 15 and osteoprotegerin in acute myocardial infarction complicated by cardiogenic shock: A biomarker substudy of the IABP-SHOCK II-trial. Eur. J. Heart Fail. 2014, 16, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Fuernau, G.; Traeder, F.; Lele, S.S.; Rajapurkar, M.M.; Mukhopadhyay, B.; Waha, S.; de Desch, S.; Eitel, I.; Schuler, G.; Adams, V.; et al. Catalytic iron in acute myocardial infarction complicated by cardiogenic shock—A biomarker substudy of the IABP-SHOCK II-trial. Int. J. Cardiol. 2017, 227, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Pöss, J.; Fuernau, G.; Denks, D.; Desch, S.; Eitel, I.; Waha, S.; de Link, A.; Schuler, G.; Adams, V.; Böhm, M.; et al. Angiopoietin-2 in acute myocardial infarction complicated by cardiogenic shock--a biomarker substudy of the IABP-SHOCK II-Trial. Eur. J. Heart Fail. 2015, 17, 1152–1160. [Google Scholar] [CrossRef] [Green Version]
- Cheng, W.; Fuernau, G.; Desch, S.; Freund, A.; Feistritzer, H.-J.; Pöss, J.; Buettner, P.; Thiele, H. Circulating Monocyte Chemoattractant Protein-1 in Patients with Cardiogenic Shock Complicating Acute Myocardial Infarction Treated with Mild Hypothermia: A Biomarker Substudy of SHOCK-COOL Trial. JCDD 2022, 9, 280. [Google Scholar] [CrossRef]
- Chen, C.; Duckworth, C.A.; Fu, B.; Pritchard, D.M.; Rhodes, J.M.; Yu, L.-G. Circulating galectins -2, -4 and -8 in cancer patients make important contributions to the increased circulation of several cytokines and chemokines that promote angiogenesis and metastasis. Br. J. Cancer 2014, 110, 741–752. [Google Scholar] [CrossRef] [Green Version]
- Meijers, W.C.; van der Velde, A.; de Rogier Boer, R.A. The ARCHITECT galectin-3 assay: Comparison with other automated and manual assays for the measurement of circulating galectin-3 levels in heart failure. Expert Rev. Mol. Diagn. 2014, 14, 257–266. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day 1 | Day 2 | Day 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| MTH (n = 19) | Control (n = 19) | p-Value | MTH (n = 14) | Control (n = 16) | p-Value | MTH (n = 11) | Control (n = 14) | p-Value | |
| Age, years (IQR) | 76 (71–80) | 75 (70–81) | 0.79 | 76 (68.5–78.5) | 75.5 (70.8–82) | 0.67 | 75 (61–77) | 73.5 (65–81.5) | 0.68 |
| Female, n (%) | 8 (42.1) | 5 (26.3) | 0.5 | 4 (28.6) | 5 (31.3) | >0.99 | 5 (45.5) | 5 (35.7) | 0.7 |
| Active smoker, n (%) | 4 (21) | 4 (21) | >0.99 | 4 (28.6) | 3 (18.8) | 0.67 | 2 (18.2) | 4 (28.6) | 0.66 |
| Diabetes mellitus, n (%) | 7 (36.8) | 4 (21) | 0.48 | 4 (28.6) | 3 (18.8) | 0.67 | 4 (36.4) | 4 (28.6) | >0.99 |
| CK (U/L) (IQR) | 6.4 (3–21.9) | 19.7 (7.4–39) | 0.1 | 4.8 (1.8–15) | 19.1 (9.8–35.3) | 0.022 | 3.8 (2.8–9.2) | 15 (4.7–29) | 0.067 |
| BMI, kg/m2 (IQR) | 27.5 (23.6–33) | 27.8 (26–31) | 0.85 | 26.9 (23.5–30.6) | 27.8 (25–30.7) | 0.53 | 29.4 (23–36.7) | 28.4 (25.7–31) | 0.85 |
| White blood cell, 109/L (IQR) | 16.5 (13–19) | 13 (9.6–17.7) | 0.12 | 15.9 (13.2–18.2) | 14.1 (10.5–17.8) | 0.3 | 16.8 (15.2–19.3) | 13.1 (8.5–17.5) | 0.1 |
| Creatinine, µmol/L (IQR) | 131 (78–217) | 158 (99–250) | 0.26 | 123.5 (69–171) | 147 (95–223) | 0.22 | 119 (67–162) | 146.5 (91.5–227) | 0.32 |
| CRP (IQR) | 21.4 (3.1–72) | 12.4 (7–64.9) | 0.72 | 5.5 (2.5–78.6) | 14.3 (7.2–64.3) | 0.48 | 12 (2.4–86.1) | 14.3 (7.6–63.1) | >0.99 |
| Maximum CK-MB, U/L(IQR) | 2.6 (1.4–6.2) | 3.5 (1.9–8.8) | 0.49 | 2.3 (1.3–8.5) | 2.6 (1.8–9) | 0.71 | 2.7 (5.51–1.41) | 2.64 (1.6–6.6) | 0.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, W.; Fuernau, G.; Desch, S.; Freund, A.; Feistritzer, H.-J.; Pöss, J.; Besler, C.; Lurz, P.; Büttner, P.; Thiele, H. Circulating Galectin-3 in Patients with Cardiogenic Shock Complicating Acute Myocardial Infarction Treated with Mild Hypothermia: A Biomarker Sub-Study of the SHOCK-COOL Trial. J. Clin. Med. 2022, 11, 7168. https://doi.org/10.3390/jcm11237168
Cheng W, Fuernau G, Desch S, Freund A, Feistritzer H-J, Pöss J, Besler C, Lurz P, Büttner P, Thiele H. Circulating Galectin-3 in Patients with Cardiogenic Shock Complicating Acute Myocardial Infarction Treated with Mild Hypothermia: A Biomarker Sub-Study of the SHOCK-COOL Trial. Journal of Clinical Medicine. 2022; 11(23):7168. https://doi.org/10.3390/jcm11237168
Chicago/Turabian StyleCheng, Wenke, Georg Fuernau, Steffen Desch, Anne Freund, Hans-Josef Feistritzer, Janine Pöss, Christian Besler, Philipp Lurz, Petra Büttner, and Holger Thiele. 2022. "Circulating Galectin-3 in Patients with Cardiogenic Shock Complicating Acute Myocardial Infarction Treated with Mild Hypothermia: A Biomarker Sub-Study of the SHOCK-COOL Trial" Journal of Clinical Medicine 11, no. 23: 7168. https://doi.org/10.3390/jcm11237168