
Eryptosis in Patients with Chronic Kidney Disease: A Possible Relationship with Oxidative Stress and Inflammatory Markers
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Enrollment and Blood Collection
2.2. Eryptosis Evaluation
2.3. Oxidative Stress Detection
2.3.1. Myeloperoxidase (MPO) Enzyme-Linked Immunosorbent Assay (ELISA) Detection
2.3.2. Copper/Zinc Superoxide Dismutase (Cu/ZnSOD) ELISA Detection
2.4. Inflammation Evaluation: IL-6 Detection
2.5. Statistical Analysis
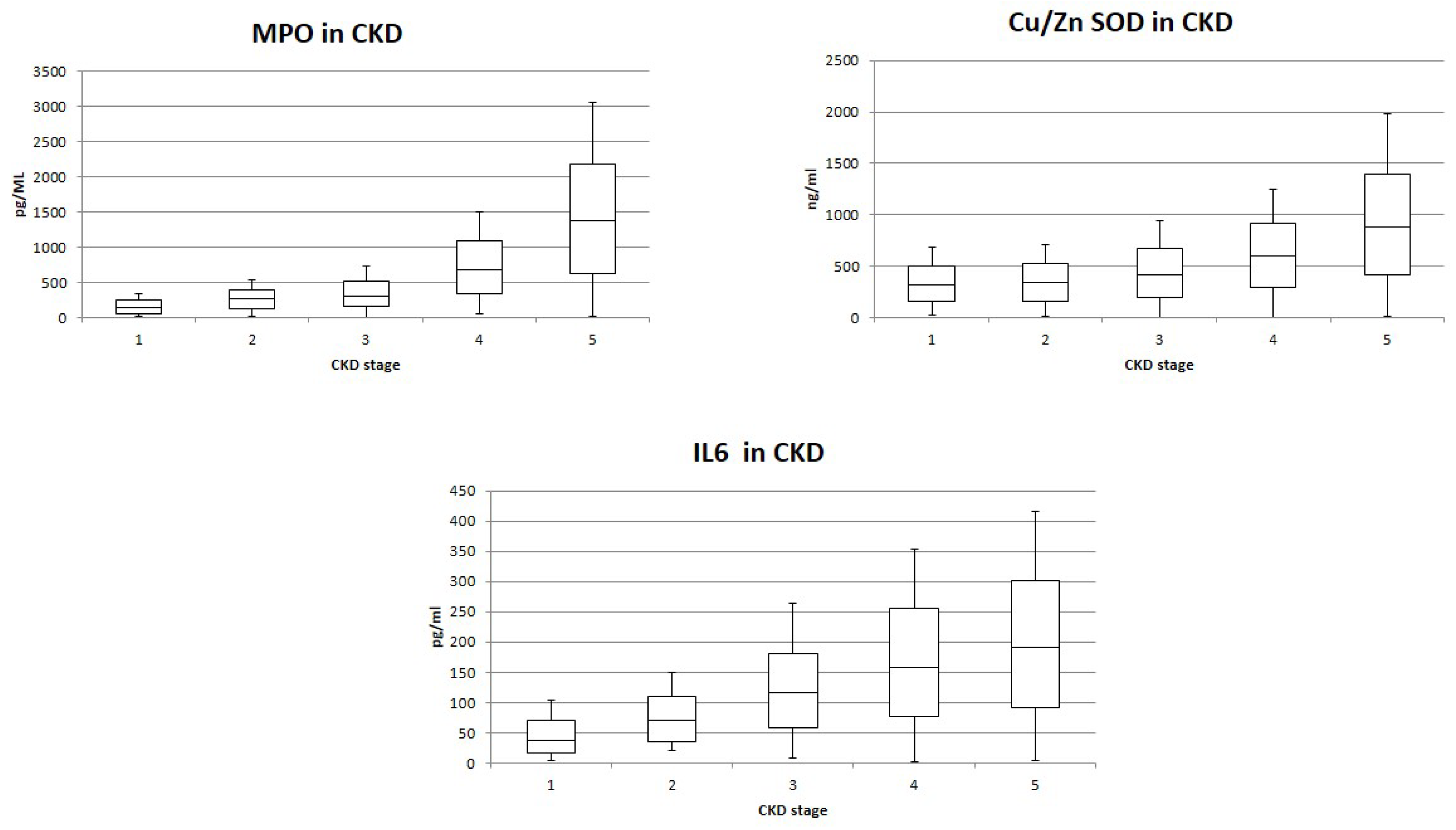
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Lang, F.; Quadri, S.M. Mechanisms and significance of eryptosis, the suicidal death of erythrocytes. Blood Purif. 2012, 33, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Lang, F.; Huber, S.M.; Szabo, I.; Gulbins, E. Plasma membrane ion channels in suicidal cell death. Arch. Biochem. Biophysl. 2007, 462, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Föller, M.; Lang, F. Ion Transport in Eryptosis, the Suicidal Death ofErythrocytes. Front. Cell Dev. Biol. 2020, 8, 597. [Google Scholar] [CrossRef]
- Lang, F.; Lang, E.; Fller, M. Physiology and pathophysiology of eryptosis. Trans. Med. Hemotherapy 2012, 39, 308–314. [Google Scholar] [CrossRef]
- Bonomini, M.; Sirolli, V.; Reale, M.; Arduini, A. Involvement of phosphatidylserine exposure in the recognition and phagocytosis of uremic erythrocytes. Am. J. Kid. Dis. 2001, 37, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Bonan, N.B.; Steiner, T.M.; Kuntsevich, V.; Virzì, G.M.; Azevedo, M.; Nakao, L.S.; Barreto, F.C.; Ronco, C.; Thijssen, A.; Kotanko, P.; et al. Uremic toxicity-induced eryptosis and monocyte modulation: The erythrophagocytosis as a novel pathway to renal anemia. Blood Purif. 2016, 41, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Bonomini, M.; Sirolli, V.; Settefrati, N.; Dottori, S.; Di Liberato, L.; Arduini, A. Increased erythrocyte phosphatidylserine exposure in chronic renal failure. J. Am. Soc. Nephrol. 1999, 10, 1982–1990. [Google Scholar] [CrossRef]
- Ahmed, M.S.; Abed, M.; Voelkl, J.; Lang, F. Triggering of suicidal erythrocyte death by uremic toxin indoxyl sulphate. BMC Nephrol. 2013, 14, 244. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.S.; Langer, H.; Abed, M.; Voelkl, J.; Lang, F. The uremic toxin acrolein promotes suicidal erythrocyte death. Kidney Blood Press. Res. 2013, 37, 158–167. [Google Scholar] [CrossRef]
- Gao, C.; Ji, S.; Dong, W.; Qi, Y.; Song, W.; Cui, D.; Shi, J. Indolic uremic solutes enhance procoagulant activity of red blood cells through phosphatidylserine exposure and microparticle release. Toxins 2015, 7, 4390–4403. [Google Scholar] [CrossRef]
- Li, D.; Zheng, X.; Zhang, Y.; Li, X.; Chen, X.; Yin, Y.; Hu, J.; Li, J.; Guo, M.; Wang, X. What Should Be Responsible for Eryptosis in Chronic Kidney Disease? Kidney Blood Press. Res. 2022, 47, 375–390. [Google Scholar] [CrossRef] [PubMed]
- Gok, M.G.; Paydas, S.; Boral, B.; Onan, E.; Kaya, B. Evaluation of eryptosis inpatients with chronic kidney disease. Int. Urol. Nephrol. 2022, 54, 2919–2928. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Virzì, G.M.; Milan Manani, S.; Clementi, A.; Castegnaro, S.; Brocca, A.; Riello, C.; de Cal, M.; Giuliani, A.; Battaglia, G.G.; Crepaldi, C.; et al. Eryptosis Is Altered in Peritoneal Dialysis Patients. Blood Purif. 2019, 48, 351–357. [Google Scholar] [CrossRef]
- Benabe, J.E.; Echegoyen, L.A.; Pastrana, B.; Martinez-Maldonado, M. Mechanism of inhibition of glycolysis by vanadate. J. Biol. Chem. 1987, 262, 9555–9560. [Google Scholar] [CrossRef]
- Virzì, G.M.; Mattiotti, M.; Clementi, A.; Milan Manani, S.; Battaglia, G.G.; Ronco, C.; Zanella, M. In Vitro Induction of Eryptosis by Uremic Toxins and Inflammation Mediators in Healthy Red Blood Cells. J. Clin. Med. 2022, 11, 5329. [Google Scholar] [CrossRef]
- Terawaki, H.; Yoshimura, K.; Hasegawa, T.; Matsuyama, Y.; Negawa, T.; Yamada, K.; Matsushima, M.; Nakayama, M.; Hosoya, T.; Era, S. Oxidative stress is enhanced in correlation with renal dysfunction: Examination with the redox state of albumin. Kidney Int. 2004, 66, 1988–1993. [Google Scholar] [CrossRef] [Green Version]
- Locatelli, F.; Canaud, B.; Eckardt, K.U.; Stenvinkel, P.; Wanner, C.; Zoccali, C. Oxidative stress in end-stage renal disease: An emerging threat to patient outcome. Nephrol. Dial. Transpl. 2003, 18, 1272–1280. [Google Scholar] [CrossRef] [Green Version]
- Vodosek, H.; Bevc, S.; Ekart, R.; Hojs, R. Oxidative stress markers in chronic kidney disease with emphasis on diabetic nephropathy. Antioxidants 2020, 9, 925. [Google Scholar] [CrossRef]
- Calderón-Salinas, J.V.; Muñoz-Reyes, E.G.; Guerrero-Romero, J.F.; Rodríguez-Morán, M.; Bracho-Riquelme, R.L.; Carrera-Gracia, M.A.; Quintanar-Escorza, M.A. Eryptosis and oxidative damage in type 2 diabetic mellitus patients with chronic kidney disease. Mol. Cell Biochem. 2011, 357, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Mekki, K.; Taleb, W.; Bouzidi, N.; Kaddous, A.; Bouchenak, M. Effect of hemodialysis and peritoneal dialysis on redox status in chronic renal failure patients: A comparative study. Lipids Health Dis. 2010, 9, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tozoni, S.S.; Dias, G.F.; Bohnen, G.; Grobe, N.; Pecoits-Filho, R.; Kotanko, P.; Moreno-Amaral, A.N. Uremia and Hypoxia Independently Induce Eryptosis and Erythrocyte Redox Imbalance. Cell Physiol. Biochem. 2019, 53, 794–804. [Google Scholar] [PubMed]
- Sudnitsyna, J.; Skverchinskaya, E.; Dobrylko, I.; Nikitina, E.; Gambaryan, S.; Mindukshev, I. Microvesicle Formation Induced by Oxidative Stress in Human Erythrocytes. Antioxidants 2020, 9, 929. [Google Scholar] [CrossRef] [PubMed]
- Tbahriti, H.F.; Meknassi, D.; Moussaoui, R.; Messaoudi, A.; Zemour, L.; Kaddous, A.; Bouchenak, M.; Mekki, K. Inflammatory status in chronic renal failure: The role of homocysteinemia and pro-inflammatory cytokines. World J. Nephrol. 2013, 2, 31–37. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Male/Female | 14 M/11 F |
|---|---|
| Age, years | 57 ± 17 |
| Diabetic nephropathy | 7/25 |
| Hypertension | 8/25 |
| Nephroangiosclerosis | 3/25 |
| Polycystic kidney disease | 2/25 |
| Other causes | 3/25 |
| Unknown causes | 2/25 |
| Chronic Kidney Disease Stages | eGFR, mL/min/1.73 m2 | Hb, g/dL | Hct, % | Fe, µg/dL | Ferritin, ng/mL |
|---|---|---|---|---|---|
| G1 | 95 ± 5 | 12.2 ± 0.9 | 37.8± 0.8 | 75 ± 7 | 152 ± 10 |
| G2 | 74 ±8 | 11.7 ± 1.4 | 37.2 ± 1.0 | 71 ± 8 | 133 ± 12 |
| G3 | 50 ± 6 | 11.4 ± 1.5 | 35.6 ± 1.3 | 64 ± 12 | 119 ± 15 |
| G4 | 24 ± 4 | 11.1 ± 1.4 | 35.1 ± 1.1 | 40 ± 7 | 122 ± 12 |
| G5 | 13 ± 2 | 10.4 ± 1.8 | 33.8 ± 2.0 | 34 ± 6 | 116 ± 17 |
| Correlation Values | |
|---|---|
| Eryptosis/eGFR | −0.76 |
| Eryptosis/Hb | −0.49 |
| Eryptosis/Hct | −0.64 |
| Eryptosis/Fe | −0.75 |
| Eryptosis/ferritin | −0.45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clementi, A.; Virzì, G.M.; Milan Manani, S.; Battaglia, G.G.; Ronco, C.; Zanella, M. Eryptosis in Patients with Chronic Kidney Disease: A Possible Relationship with Oxidative Stress and Inflammatory Markers. J. Clin. Med. 2022, 11, 7167. https://doi.org/10.3390/jcm11237167
Clementi A, Virzì GM, Milan Manani S, Battaglia GG, Ronco C, Zanella M. Eryptosis in Patients with Chronic Kidney Disease: A Possible Relationship with Oxidative Stress and Inflammatory Markers. Journal of Clinical Medicine. 2022; 11(23):7167. https://doi.org/10.3390/jcm11237167
Chicago/Turabian StyleClementi, Anna, Grazia Maria Virzì, Sabrina Milan Manani, Giovanni Giorgio Battaglia, Claudio Ronco, and Monica Zanella. 2022. "Eryptosis in Patients with Chronic Kidney Disease: A Possible Relationship with Oxidative Stress and Inflammatory Markers" Journal of Clinical Medicine 11, no. 23: 7167. https://doi.org/10.3390/jcm11237167