
Cardiac Biomarkers and Risk Scores in Relation with History of Atherosclerotic Cardiovascular Disease in Patients Admitted with COVID-19: The Experience of an Eastern European Center
 , ,
, ,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population and Setting
2.3. Variables and Data Collection
2.4. Statistical Methods
3. Results
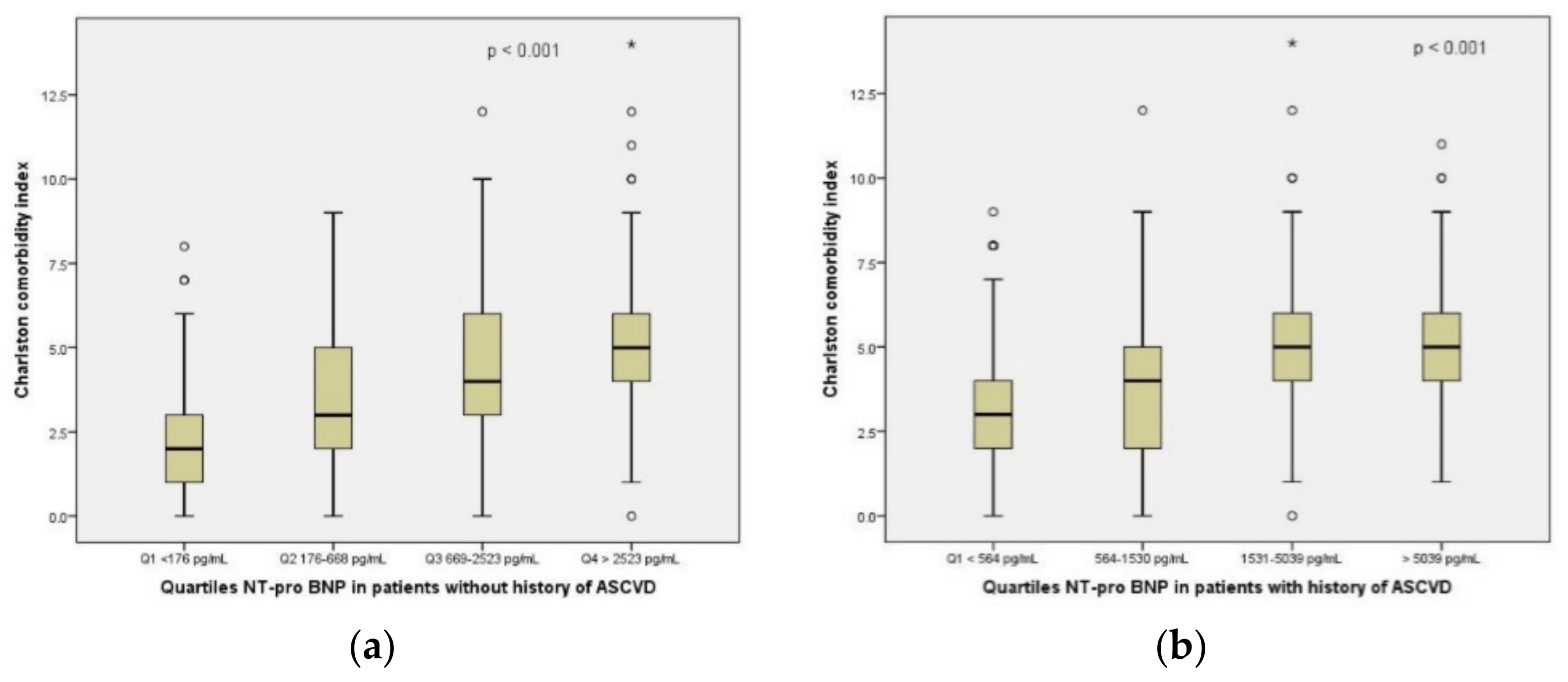
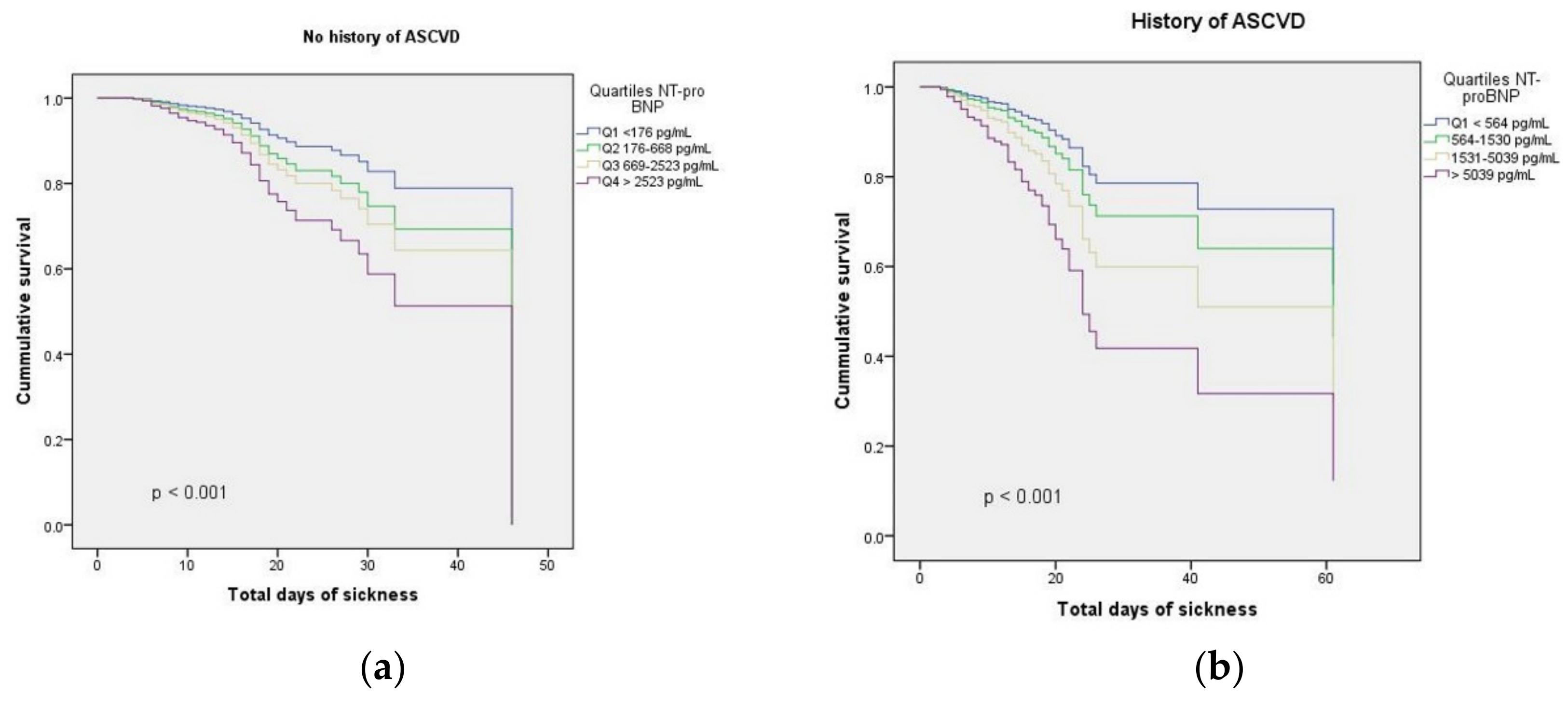
3.1. NT-proBNP and Risk Scores in Relation with the Outcomes
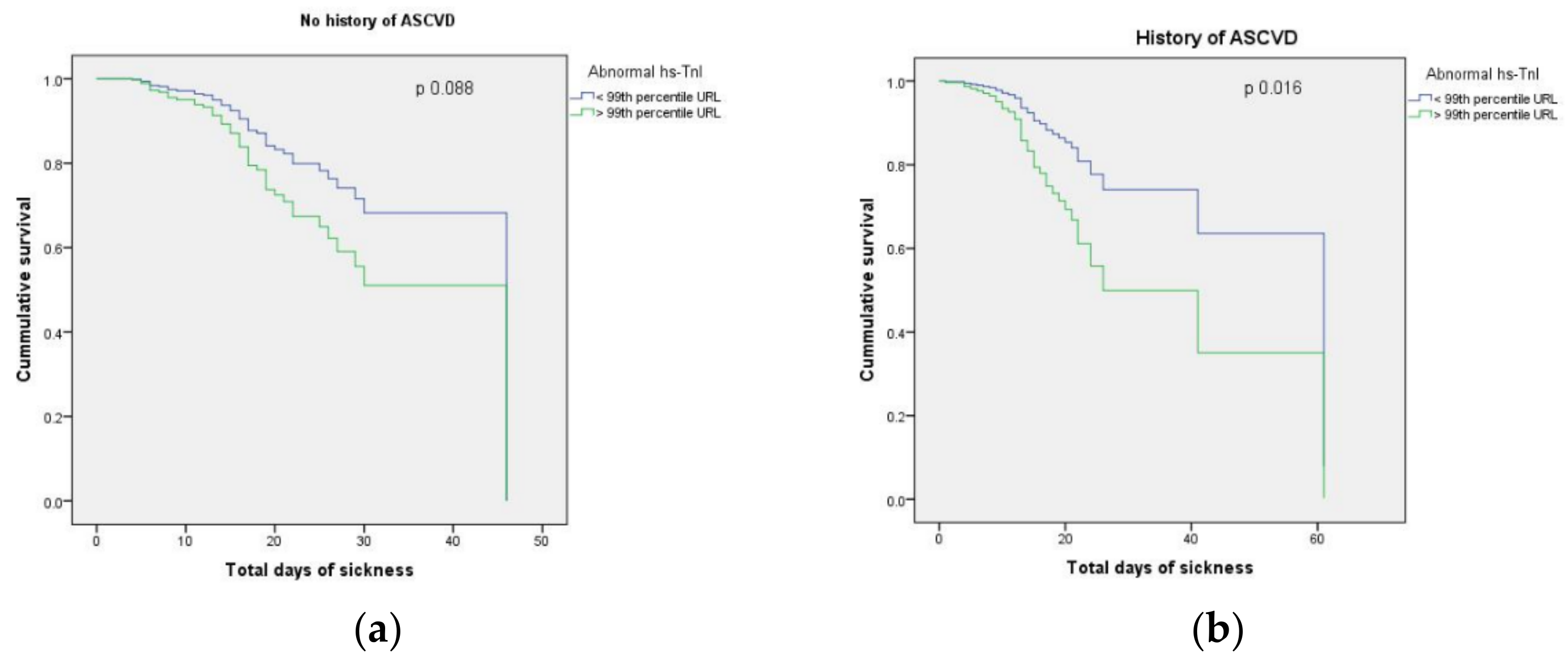
3.2. hs-TnI and Risk Scores in Relation with the Outcomes
3.3. Predictive Capacity of Biomarkers in Relation with the Main Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, X.; Pan, X.; Li, Y.; An, N.; Xing, Y.; Yang, F.; Tian, L.; Sun, J.; Gao, Y.; Shang, H.; et al. Cardiac injury associated with severe disease or ICU admission and death in hospitalized patients with COVID-19: A meta-analysis and systematic review. Crit. Care 2020, 24, 468. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Qin, M.; Cai, Y.; Liu, T.; Shen, B.; Yang, F.; Cao, S.; Liu, X.; Xiang, Y.; Zhao, Q.; et al. Characteristics and clinical significance of myocardial injury in patients with severe coronavirus disease 2019. Eur. Heart J. 2020, 41, 2070–2079. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Rasool, S.T.; Ahmed, S.I. Role of Cardiac Biomarkers in COVID-19: What Recent Investigations Tell Us? Curr. Probl. Cardiol. 2021, 46, 100842. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, A.; Sotgia, S.; Carru, C.; Mangoni, A.A. B-Type Natriuretic Peptide Concentrations, COVID-19 Severity, and Mortality: A Systematic Review and Meta-Analysis with Meta-Regression. Front. Cardiovasc. Med. 2021, 8, 690790. [Google Scholar] [CrossRef]
- Soumya, R.S.; Govindan Unni, T.; Raghu, K.G. Impact of COVID-19 on the Cardiovascular System: A Review of Available Reports. Cardiovasc. Drugs Ther. 2021, 35, 411–425. [Google Scholar] [CrossRef]
- Task Force for the Management of COVID-19 of the European Society of Cardiology. European Society of Cardiology guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: Part 1-epidemiology, pathophysiology, and diagnosis. Eur. Heart J. 2022, 43, 1033–1058. [Google Scholar] [CrossRef]
- Okor, I.; Bob-Manuel, T.; Price, J.; Sleem, A.; Amoran, O.; Kelly, J.; Ekerete, M.F.; Bamgbose, M.O.; Bolaji, O.A.; Krim, S.R. COVID-19 Myocarditis: An Emerging Clinical Conundrum. Curr. Probl. Cardiol. 2022, 47, 101268. [Google Scholar] [CrossRef]
- Bansal, M. Cardiovascular disease and COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 247–250. [Google Scholar] [CrossRef]
- De Michieli, L.; Jaffe, A.S.; Sandoval, Y. Use and Prognostic Implications of Cardiac Troponin in COVID-19. Cardiol. Clin. 2022, 40, 287–300. [Google Scholar] [CrossRef]
- Calvo-Fernández, A.; Izquierdo, A.; Subirana, I.; Farré, N.; Vila, J.; Durán, X.; García-Guimaraes, M.; Valdivielso, S.; Cabero, P.; Soler, C.; et al. Markers of myocardial injury in the prediction of short-term COVID-19 prognosis. Rev. Esp. Cardiol. 2021, 74, 576–583. [Google Scholar] [CrossRef]
- Stefanini, G.G.; Chiarito, M.; Ferrante, G.; Cannata, F.; Azzolini, E.; Viggiani, G.; De Marco, A.; Briani, M.; Bocciolone, M.; Bragato, R.; et al. Humanitas COVID-19 Task Force. Early detection of elevated cardiac biomarkers to optimise risk stratification in patients with COVID-19. Heart 2020, 106, 1512–1518. [Google Scholar] [CrossRef] [PubMed]
- Chehrazi, M.; Yavarpour, H.; Jalali, F.; Saravi, M.; Jafaripour, I.; Hedayati, M.T.; Amin, K.; Pourkia, R.; Abroutan, S.; Javanian, M.; et al. Optimal cut points of N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) in patients with COVID-19. Egypt. Heart J. 2022, 74, 16. [Google Scholar] [CrossRef] [PubMed]
- Inciardi, R.M.; Adamo, M.; Lupi, L.; Cani, D.S.; Di Pasquale, M.; Tomasoni, D.; Italia, L.; Zaccone, G.; Tedino, C.; Fabbricatore, D.; et al. Characteristics and outcomes of patients hospitalized for COVID-19 and cardiac disease in Northern Italy. Eur. Heart J. 2020, 41, 1821–1829. [Google Scholar] [CrossRef] [PubMed]
- Szarpak, L.; Mierzejewska, M.; Jurek, J.; Kochanowska, A.; Gasecka, A.; Truszewski, Z.; Pruc, M.; Blek, N.; Rafique, Z.; Filipiak, K.J.; et al. Effect of Coronary Artery Disease on COVID-19-Prognosis and Risk Assessment: A Systematic Review and Meta-Analysis. Biology 2022, 11, 221. [Google Scholar] [CrossRef]
- Wei, J.F.; Huang, F.Y.; Xiong, T.Y.; Wei, J.F.; Huang, F.Y.; Xiong, T.Y.; Liu, Q.; Chen, H.; Wang, H.; Huang, H.; et al. Acute myocardial injury is common in patients with COVID-19 and impairs their prognosis. Heart 2020, 106, 1154–1159. [Google Scholar] [CrossRef]
- Klok, F.A.; Mos, I.C.; Huisman, M.V. Brain-type natriuretic peptide levels in the prediction of adverse outcome in patients with pulmonary embolism. Am. J. Respir. Crit. Care Med. 2008, 178, 425–430. [Google Scholar] [CrossRef]
- Nowak, A.; Breidthardt, T.; Christ-Crain, M.; Bingisser, R.; Meune, C.; Tanglay, Y.; Heinisch, C.; Reiter, M.; Drexler, B.; Arenja, N.; et al. Direct comparison of three natriuretic peptides for prediction of short- and long-term mortality in patients with community-acquired pneumonia. Chest 2012, 141, 974–982. [Google Scholar] [CrossRef]
- Varol, Y.; Hakoglu, B.; Kadri Cirak, A.; Polat, G.; Komurcuoglu, B.; Akkol, B.; Atasoy, C.; Bayramic, E.; Balci, G.; Ataman, S.; et al. The impact of Charlson comorbidity index on mortality from SARS-CoV-2 virus infection and A novel COVID-19 mortality index: CoLACD. Int. J. Clin. Pract. 2021, 75, e13858. [Google Scholar] [CrossRef]
- Baker, K.F.; Hanrath, A.T.; van der Loeff, I.S.; Kay, L.J.; Back, J.; Duncan, C.J. National Early Warning Score 2 (NEWS2) to identify inpatient COVID-19 deterioration: A retrospective analysis. Clin. Med. 2021, 21, 84–89. [Google Scholar] [CrossRef]
- Faxon, D.P.; Creager, M.A.; Smith, S.C., Jr.; Pasternak, R.C.; Olin, J.W.; Bettmann, M.A.; Criqui, M.H.; Milani, R.V.; Loscalzo, J.; Kaufman, J.A.; et al. Atherosclerotic Vascular Disease Conference: Executive summary: Atherosclerotic Vascular Disease Conference proceeding for healthcare professionals from a special writing group of the American Heart Association. Circulation 2004, 109, 2595–2604. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 25 May 2022).
- Charlson, M.E.; Pompei, P.; Ales, K.L.; Mackenzie, R.C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chron. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef] [PubMed]
- Muneer, M.; Akbar, I. Acute Metabolic Emergencies in Diabetes: DKA, HHS and EDKA. In Diabetes: From Research to Clinical Practice; Advances in Experimental Medicine andBiology; Islam, M.S., Ed.; Springer Nature: Cham, Switzerland, 2020; Volume 1307, pp. 85–114. [Google Scholar] [CrossRef]
- Crouch, R.; Charters, A.; Dawood, M.; Bennett, P. (Eds.) Endocrine and metabolic emergencies. In Oxford Handbook of Emergency Nursing, 2nd ed.; Oxford University Press: Oxford, UK, 2016; Available online: https://oxfordmedicine.com/view/10.1093/med/9780199688869.001.0001/med-9780199688869-chapter-16 (accessed on 2 May 2022).
- Royal College of Physicians. National Early Warning Score (NEWS) 2. RCP. 2017. Available online: https://www.rcplondon.ac.uk/projects/outputs/national-early-warning-score-news-2 (accessed on 14 October 2020).
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef] [PubMed]
- Caro-Codón, J.; Rey, J.R.; Buño, A.; Iniesta, A.M.; Rosillo, S.O.; Castrejon-Castrejon, S.; Rodriguez-Sotelo, L.; Martinez, L.A.; Marco, I.; Merino, C.; et al. Characterization of NT-proBNP in a large cohort of COVID-19 patients. Eur. J. Heart Fail. 2021, 23, 456–464. [Google Scholar] [CrossRef]
- Sheth, A.; Modi, M.; Dawson, D.; Dominic, P. Prognostic value of cardiac biomarkers in COVID-19 infection. Sci. Rep. 2021, 11, 4930. [Google Scholar] [CrossRef]
- Kaufmann, C.C.; Ahmed, A.; Burger, A.L.; Muthspiel, M.; Jäger, B.; Wojta, J.; Huber, K. Biomarkers Associated with Cardiovascular Disease in COVID-19. Cells 2022, 11, 922. [Google Scholar] [CrossRef]
- De Giorgi, A.; Fabbian, F.; Greco, S.; Di Simone, E.; De Giorgio, R.; Passaro, A.; Zuliani, G.; Manfredini, R. Prediction of in-hospital mortality of patients with SARS-CoV-2 infection by comorbidity indexes: An Italian internal medicine single center study. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 10258–10266. [Google Scholar]
- Zuin, M.; Rigatelli, G.; Bilato, C.; Zanon, F.; Zuliani, G.; Roncon, L. Pre-existing atrial fibrillation is associated with increased mortality in COVID-19 Patients. J. Interv. Card. Electrophysiol. 2021, 62, 231–238. [Google Scholar] [CrossRef]
- Zuin, M.; Rigatelli, G.; Zuliani, G.; Rigatelli, A.; Mazza, A.; Roncon, L. Arterial hypertension and risk of death in patients with COVID-19 infection: Systematic review and meta-analysis. J. Infect. 2020, 81, e84–e86. [Google Scholar] [CrossRef]
- De Michieli, L.; Babuin, L.; Vigolo, S.; Berti De Marinis, G.; Lunardon, A.; Favretto, F.; Lobo, R.; Sandoval, Y.; Bryant, S.C.; Donato, D.; et al. Using high sensitivity cardiac troponin values in patients with SARS-CoV-2 infection (COVID-19): The Padova experience. Clin. Biochem. 2021, 90, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Omland, T.; Prebensen, C.; Røysland, R.; Søvik, S.; Sørensen, V.; Røsjø, H.; Svensson, M.; Berdal, J.E.; Myhre, P.L. Established Cardiovascular Biomarkers Provide Limited Prognostic Information in Unselected Patients Hospitalized with COVID-19. Circulation 2020, 142, 1878–1880. [Google Scholar] [CrossRef] [PubMed]
- Perrone, M.A.; Zaninotto, M.; Masotti, S.; Musetti, V.; Padoan, A.; Prontera, C.; Plebani, M.; Passino, C.; Romeo, F.; Bernardini, S.; et al. The combined measurement of high-sensitivity cardiac troponins and natriuretic peptides: A useful tool for clinicians? J. Cardiovasc. Med. 2020, 21, 953–963. [Google Scholar] [CrossRef] [PubMed]
- Mueller, C.; Giannitsis, E.; Jaffe, A.S.; Huber, K.; Mair, J.; Cullen, L.; Hammarsten, O.; Mills, N.L.; Möckel, M.; Krychtiuk, K.; et al. Cardiovascular biomarkers in patients with COVID-19. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 310–319. [Google Scholar] [CrossRef]
- Bojkova, D.; Wagner, J.U.; Shumliakivska, M.; Aslan, G.S.; Saleem, U.; Hansen, A.; Luxán, G.; Günther, S.; Pham, M.D.; Krishnan, J.; et al. SARS-CoV-2 infects and induces cytotoxic effects in human cardiomyocytes. Cardiovasc. Res. 2020, 116, 2207–2215. [Google Scholar] [CrossRef]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential effects of coronaviruses on the cardiovascular system: A review. JAMA Cardiol. 2020, 5, 831–840. [Google Scholar] [CrossRef]
- Mirò, Ò.; Sabaté, M.; Jiménez, S.; Mebazaa, A.; Martínez-Nadal, G.; Piñera, P.; Burillo-Putze, G.; Martín, A.; Martín-Sánchez, F.J.; Jacob, J.; et al. A Case-Control, Multicentre Study of Consecutive Patients with COVID-19 and Acute (Myo)Pericarditis: Incidence, Risk Factors, Clinical Characteristics and Outcomes. Emerg. Med. J. 2022, 39, 402–410. [Google Scholar] [CrossRef]
- Srinivasan, A.; Wong, F.; Couch, L.S.; Wang, B.X. Cardiac Complications of COVID-19 in Low-Risk Patients. Viruses 2022, 14, 1322. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Fauvel, C.; Weizman, O.; Trimaille, A.; Mika, D.; Pommier, T.; Pace, N.; Douair, A.; Barbin, E.; Fraix, A.; Bouchot, O.; et al. Pulmonary embolism in COVID-19 patients: A French multicentre cohort study. Eur. Heart J. 2020, 41, 3058–3068. [Google Scholar] [CrossRef]
- Naruse, H.; Ishii, J.; Takahashi, H.; Kitagawa, F.; Sakaguchi, E.; Nishimura, H.; Kawai, H.; Muramatsu, T.; Harada, M.; Yamada, A.; et al. Combined assessment of D-dimer with the get with the guidelines—Heart failure risk score and N-terminal pro-B-type natriuretic peptide in patients with acute decompensated heart failure with preserved and reduced ejection fraction. J. Clin. Med. 2021, 10, 3564. [Google Scholar] [CrossRef] [PubMed]
- Zwaenepoel, B.; Dhont, S.; Hoste, E.; Gevaert, S.; Schaubroeck, H. The Prognostic Value of Cardiac Biomarkers and Echocardiography in Critical COVID-19. Front. Cardiovasc. Med. 2021, 8, 752237. [Google Scholar] [CrossRef] [PubMed]
- Shanbhag, V.; Arjun, N.R.; Chaudhuri, S.; Pandey, A.K. Utility of Age-adjusted Charlson Comorbidity Index as a Predictor of Need for Invasive Mechanical Ventilation, Length of Hospital Stay, and Survival in COVID-19 Patients. Indian J. Crit. Care Med. 2021, 25, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Lampert, J.; Miller, M.; Halperin, J.L.; Oates, C.; Giustino, G.; Nelson, K.; Feinman, J.; Kocovic, N.; Pulaski, M.; Musikantow, D.; et al. Prognostic Value of Electrocardiographic QRS Diminution in Patients Hospitalized with COVID-19 or Influenza. Am. J. Cardiol. 2021, 159, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Mountantonakis, S.E.; Saleh, M.; Fishbein, J.; Gandomi, A.; Lesser, M.; Chelico, J.; Gabriels, J.; Qiu, M.; Epstein, L.M.; Northwell COVID-19 Research Consortium. Atrial fibrillation is an independent predictor for in-hospital mortality in patients admitted with SARS-CoV-2 infection. Heart Rhythm 2021, 18, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Wong, J.; Henry, B.M. Hypertension and its severity or mortality in Coronavirus Disease 2019 (COVID-19): A pooled analysis. Pol. Arch. Intern. Med. 2020, 130, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Rey, J.R.; Caro-Codón, J.; Rosillo, S.O.; Iniesta, Á.M.; Castrejón-Castrejón, S.; Marco-Clement, I.; Martín-Polo, L.; Merino-Argos, C.; Rodríguez-Sotelo, L.; García-Veas, J.M.; et al. Heart failure in COVID-19 patients: Prevalence, incidence and prognostic implications. Eur. J. Heart Fail. 2020, 22, 2205–2215. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Wen, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe COVID-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Lopinavir-ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef]
- WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients with COVID-19: A Meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar]
- WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group. Association Between Administration of IL-6 Antagonists and Mortality Among Patients Hospitalized for COVID-19: A Meta-analysis. JAMA 2021, 326, 499–518. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total Patients (N = 1066) | Patients without ASCVD (N = 705) | Patients with ASCVD (N = 361) | ||||
|---|---|---|---|---|---|---|---|
| Survivors (N = 409) | ICU/Death (N = 296) | p-Value | Survivors (N = 195) | ICU/Death (N = 166) | p-Value | ||
| Age (years) * | 70 (60–78) | 65 (53–73) | 70 (62–79) | <0.001 | 72 (65–80) | 76 (68–82) | 0.020 |
| Viral strain, N (%) # | <0.001 | <0.001 | |||||
| Alpha | 509 (47.7) | 272 (66.5) | 83 (28.0) | 99 (50.8) | 55 (33.1) | ||
| Beta | 120 (11.3) | 39 (9.5) | 39 (13.2) | 21 (10.8) | 21 (12.7) | ||
| Delta | 349 (32.7) | 69 (16.9) | 166 (56.1) | 34 (17.4) | 80 (48.2) | ||
| Omicron | 88 (8.3) | 29 (7.1) | 8 (2.7) | 41 (21.0) | 10 (6.0) | ||
| Male gender, N (%) # | 542 (51.3) | 202 (49.4) | 159 (53.7) | 0.285 | 93 (47.7) | 89 (53.6) | 0.291 |
| Urban residence, N (%) # | 576 (54.0) | 197 (48.2) | 182 (61.5) | 0.001 | 102 (52.3) | 95 (57.2) | 0.396 |
| Smoking, N (%) # | 187 (17.5) | 74 (18.1) | 39 (13.2) | 0.096 | 46 (23.6) | 28 (16.9) | 0.119 |
| BMI ≥25 kg/m2, N (%) # | 550 (51.6) | 186 (45.5) | 172 (58.1) | 0.001 | 94 (48.2) | 98 (59.0) | 0.045 |
| History HF, N (%) # | 0.301 | <0.001 | |||||
| No HF | 708 (66.4) | 307 (75.1) | 232 (78.4) | 72 (36.9) | 97 (58.4) | ||
| HFpEF | 172 (16.2) | 51 (12.5) | 26 (8.8) | 66 (33.8) | 29 (17.5) | ||
| HFrEF | 186 (17.4) | 51 (12.5) | 38 (12.8) | 57 (29.2) | 40 (24.1) | ||
| History CKD, N (%) # | 244 (22.9) | 49 (12.0) | 80 (27.0) | <0.001 | 46 (23.6) | 69 (41.6) | <0.001 |
| History DM, N (%) # | 320 (30.0) | 127 (31.1) | 85 (28.7) | 0.560 | 54 (27.7) | 54 (32.5) | 0.357 |
| CCI score * | 4 (2–5) | 3 (1–4) | 3 (2–5) | 0.001 | 5 (3–6) | 5 (4–6) | 0.771 |
| NEWS2 score * | 6 (4–8) | 5 (3–7) | 7 (5–9) | <0.001 | 5 (3–7) | 6 (4–9) | <0.001 |
| CoLACD score * | 4 (3–4) | 3 (2–4) | 4 (3–4) | <0.001 | 4 (3–5) | 4 (3–5) | 0.514 |
| SaO2 < 90%, N (%) # | 356 (33.4) | 64 (15.7) | 172 (58.3) | <0.001 | 31 (16.0) | 89 (53.6) | <0.001 |
| SBP (mmHg) * | 131 (120–150) | 130 (120–145) | 130 (114–150) | 0.999 | 136 (120–154) | 133 (117–148) | 0.062 |
| HR (bpm) * | 85 (75–100) | 83 (75–95) | 90 (80–100) | <0.001 | 83 (75–95) | 88 (76–100) | <0.046 |
| GOT (U/L) * | 39 (25–65) | 33 (22–53) | 51 (32–93) | <0.001 | 30 (22–48) | 45 (30–75) | <0.001 |
| Creatinine (mg/dl) * | 0.9 (0.8–1.2) | 0.8 (0.7–1.1) | 1.0 (0.8–1.3) | <0.001 | 0.9 (0.8–1.2) | 1.1 (0.8–1.6) | <0.001 |
| Hemoglobin (g/dl) * | 13 (11.3–14.2) | 13.1 (11.4–14.2) | 13.2 (11.4–14.4) | 0.353 | 12.7 (10.9–13.8) | 12.9 (11.7–14.1) | 0.253 |
| WBC (×1000/microL) * | 8 (5.7–11.2) | 6.9 (5.0–9.6) | 8.8 (6.3–12.9) | <0.001 | 7.9 (5.7–10.2) | 9.9 (7.0–13.8) | <0.001 |
| CRP (mg/dL) * | 6.5 (2.1–15) | 4.4 (1.3–10.2) | 12.1 (5.9–21.3) | <0.001 | 3.3 (1.1–7.9) | 10.7 (4.2–19.1) | <0.001 |
| NT-pro BNP (pg/mL) * | 923 (250–3432) | 499 (128–1560) | 1172 (309–3344) | <0.001 | 1243 (377–3837) | 2078 (775–7877) | 0.003 |
| hs-TnI (ng/L) * | 9.5 (1.9–38.9) | 5.9 (1.6–20.6) | 15.9 (2.8–61.5) | 0.001 | 9.0 (2.3–26.9) | 23.1 (5.4–83.8) | 0.003 |
| D-dimer (mcg/mL) * | 1.4 (0.7–3.4) | 1.2 (0.6–2.7) | 1.8 (0.9–4.5) | <0.001 | 1.2 (0.6–3.3) | 1.6 (0.8–5.0) | 0.037 |
| LDH (U/L) * | 284 (210–448) | 247 (196–342) | 458 (288–674) | <0.001 | 246 (202–335) | 390 (218–569) | <0.001 |
| Presepsin (pg/mL) * | 363 (196–701) | 280 (158–531) | 604 (309–588) | <0.001 | 296 (179–464) | 570 (370–1391) | <0.001 |
| Abnormal ECG, N (%) # ST/T changes Dysrhythmias | 74 (6.9) 493 (46.2) | 19 (4.6) 163 (39.9) | 24 (8.1) 138 (46.6) | 0.013 | 15 (7.7) 109 (55.9) | 16 (9.6) 83 (50.0) | 0.510 |
| Abnormal chest CT, N (%) # | 746 (70.0) | 251 (61.4) | 249 (84.1) | <0.001 | 115 (59.0) | 131 (78.9) | <0.001 |
| Variable | Total Patients (N = 1066) | Patients without ASCVD (N = 705) | Patients with ASCVD (N = 361) | ||||
|---|---|---|---|---|---|---|---|
| Survivors (N = 409) | ICU/Death (N = 296) | p-Value | Survivors (N = 195) | ICU/Death (N = 166) | p-Value | ||
| Main diagnosis, N (%) # | |||||||
| New onset AF | 15 (1.4) | 6 (1.5) | 4 (1.4) | 0.583 | 2 (1.0) | 3 (1.8) | 0.425 |
| Another CV emergency | 343 (32.2) | 88 (21.5) | 54 (18.2) | 0.297 | 108 (55.4) | 93 (56.0) | 0.916 |
| HT emergency | 572 (53.7) | 223 (54.5) | 166 (56.1) | 0.702 | 109 (55.9) | 74 (44.6) | 0.035 |
| Metabolic emergency | 161 (15.1) | 55 (13.4) | 46 (15.5) | 0.447 | 34 (17.4) | 26 (15.7) | 0.673 |
| Liver cirrhosis/LF | 38 (3.6) | 15 (3.7) | 13 (4.4) | 0.383 | 5 (2.6) | 5 (3.0) | 0.522 |
| Acute pancreatitis | 18 (1.7) | 12 (2.9) | 3 (1.0) | 0.112 | 1 (0.5) | 2 (1.2) | 0.596 |
| COPD/acute asthma | 62 (5.8) | 19 (4.6) | 13 (4.4) | 0.513 | 16 (8.2) | 14 (8.4) | 0.543 |
| Other infection | 73 (6.8) | 33 (8.1) | 18 (6.1) | 0.377 | 13 (6.7) | 9 (5.4) | 0.665 |
| Complications, N (%) # | 869 (82.3) | 298 (73.8) | 283 (95.6) | <0.001 | 130 (67.7) | 158 (95.8) | <0.001 |
| MACEs, N (%) # | 73 (6.8) | 3 (0.7) | 39 (13.2) | <0.001 | 6 (3.1) | 25 (15.1) | <0.001 |
| H-F oxygen (NC), N (%) # | 468 (43.9) | 183 (44.7) | 114 (38.5) | 0.057 | 83 (42.6) | 88 (53.0) | 0.030 |
| CPAP or noninvasive positive pressure, N (%) # | 150 (14.1) | 12 (2.9) | 104 (35.1) | <0.001 | 6 (3.1) | 28 (16.9) | <0.001 |
| MV, N (%) | 439 (41.2) | 74 (18.1) | 215 (72.6) | <0.001 | 34 (17.4) | 116 (69.9) | <0.001 |
| Anticoagulation, N (%) # | <0.001 | 0.037 | |||||
| Prophylactic dose | 432 (40.5) | 188 (46.9) | 119 (40.2) | 57 (29.2) | 68 (41.0) | ||
| Therapeutic dose | 505 (47.4) | 142 (34.7) | 155 (52.4) | 119 (61.0) | 89 (53.6) | ||
| Treatment, N (%) # | |||||||
| Corticotherapy | 604 (56.7) | 206 (88.4) | 217 (98.2) | <0.001 | 76 (68.5) | 105 (92.9) | <0.001 |
| Antivirals | 143 (13.4) | 75 (18.3) | 42 (14.2) | 0.087 | 14 (4.9) | 12 (7.2) | 0.253 |
| Immunomodulators | 126 (12.9) | 37 (9.0) | 35 (11.8) | 0.257 | 19 (14.1) | 35 (25.4) | 0.023 |
| Hospitalization (days) * | 12 (4–16) | 14 (11–17) | 4 (2–10) | <0.001 | 15 (12–18) | 5 (2–11) | <0.001 |
| Patients without ASCVD | Patients with ASCVD | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |||||
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| NT-pro BNP * | 1.70 (1.22–2.38) | 0.002 | 1.66 (1.10–2.53) | 0.016 | 2.37 (1.56–3.59) | <0.001 | 2.63 (1.65–4.18) | <0.001 |
| Strain (Delta) | 2.51 (0.90–6.95) | 0.078 | 7.45 (0.90–61.48) | 0.062 | 2.32 (1.08–4.99) | 0.031 | 4.82 (1.06–22.01) | 0.042 |
| HT emergency | 1.22 (0.78–1.90) | 0.099 | 1.07 (0.59–1.97) | 0.182 | 1.87 (1.09–3.20) | 0.024 | 2.08 (1.03–4.21) | 0.042 |
| CCI score | 1.17 (1.07–1.29) | 0.001 | 1.07 (0.91–1.26) | 0.397 | 1.10 (0.99–1.22) | 0.081 | 1.13 (0.96–1.33) | 0.134 |
| NEWS2 score > 5 | 1.68 (1.07–2.64) | 0.023 | 0.69 (0.35–1.34) | 0.268 | 1.16 (0.72–1.88) | 0.053 | 1.55 (0.79–3.03) | 0.205 |
| CoLACD score | 1.14 (0.97–1.34) | 0.098 | 1.12 (0.90–1.40) | 0.214 | 1.11 (0.87–1.41) | 0.094 | 1.13 (0.85–1.51) | 0.384 |
| SaO2 > 90% | 0.22 (0.14–0.33) | <0.001 | 0.42 (0.22–0.79) | 0.007 | 0.31 (0.20–0.49) | <0.001 | 0.55 (0.27–1.10) | 0.090 |
| hs-CRP | 1.05 (1.03–1.06) | <0.001 | 1.01 (0.97–1.04) | 0.678 | 1.04 (1.03–1.06) | <0.001 | 1.04 (1.01–1.07) | 0.009 |
| BMI < 25 kg/m2 | 0.57 (0.38–0.85) | 0.006 | 0.82 (0.45–1.47) | 0.497 | 0.46 (0.29–0.75) | 0.002 | 0.50 (0.26–0.96) | 0.037 |
| CKD | 0.40 (0.26–0.62) | <0.001 | 0.69 (0.36–1.34) | 0.278 | 0.51 (0.32–0.80) | 0.003 | 1.62 (0.79–3.35) | 0.192 |
| Anticoagulation ** | 0.56 (0.27–1.18) | 0.017 | 0.63 (0.40–1.00) | 0.052 | 0.44 (0.11–1.82) | 0.098 | 0.79 (0.45–1.37) | 0.401 |
| Age >65 years | 0.42 (0.26–0.67) | <0.001 | 0.62 (0.32–1.19) | 0.150 | 0.87 (0.51–1.50) | 0.086 | 1.29 (0.60–2.80) | 0.519 |
| Patients without ASCVD | Patients with ASCVD | |||||||
| Univariate | Multivariate | Univariate | Multivariate | |||||
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| hs-TnI * | 1.26 (0.95–1.68) | 0.092 | 1.09 (0.84–1.43) | 0.522 | 1.31 (1.03–1.65) | 0.025 | 1.51 (1.13–2.03) | 0.006 |
| HT emergency | 1.22 (0.78–1.90) | 0.099 | 0.98 (0.47–2.03) | 0.947 | 1.87 (1.09–3.20) | 0.024 | 2.94 (1.19–7.28) | 0.020 |
| Strain (Delta) | 2.51 (0.90–6.95) | 0.078 | 2.63 (0.55–12.56) | 0.226 | 2.32 (1.08–4.99) | 0.031 | 1.17 (0.26–5.25) | 0.835 |
| CCI score | 1.17 (1.07–1.29) | 0.001 | 1.21 (0.99–1.49) | 0.064 | 1.10 (0.99–1.22) | 0.081 | 1.20 (0.99–1.46) | 0.069 |
| NEWS2 score > 5 | 1.68 (1.07–2.64) | 0.023 | 0.52 (0.21–1.34) | 0.176 | 1.16 (0.72–1.88) | 0.053 | 1.69 (0.75–3.82) | 0.210 |
| CoLACD score | 1.14 (0.97–1.34) | 0.098 | 1.17 (0.90–1.52) | 0.236 | 1.11 (0.87–1.41) | 0.094 | 1.07 (0.76–1.51) | 0.686 |
| SaO2 > 90% | 0.22 (0.14–0.33) | <0.001 | 0.44 (0.21–0.92) | 0.030 | 0.31 (0.20–0.49) | <0.001 | 0.22 (0.09–0.57) | 0.002 |
| hs-CRP | 1.05 (1.03–1.06) | <0.001 | 1.05 (1.01–1.08) | 0.015 | 1.04 (1.03–1.06) | <0.001 | 1.07 (1.03–1.11) | <0.001 |
| BMI < 30 kg/m2 | 0.57 (0.38–0.85) | 0.006 | 1.21 (0.59–2.51) | 0.600 | 0.46 (0.29–0.75) | 0.002 | 0.93 (0.37–2.34) | 0.880 |
| CKD | 0.40 (0.26–0.62) | <0.001 | 0.68 (0.33–1.41) | 0.299 | 0.51 (0.32–0.80) | 0.003 | 1.67 (0.73–3.84) | 0.228 |
| Anticoagulation ** | 0.56 (0.27–1.18) | 0.017 | 0.51 (0.29–0.90) | 0.020 | 0.44 (0.11–1.82) | 0.098 | 0.54 (0.28–1.06) | 0.072 |
| Age < 65 years | 0.42 (0.26–0.67) | <0.001 | 0.71 (0.33–1.54) | 0.380 | 0.87 (0.51–1.50) | 0.086 | 0.69 (0.26–1.83) | 0.454 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lionte, C.; Sorodoc, V.; Haliga, R.E.; Bologa, C.; Ceasovschih, A.; Sirbu, O.; Gorciac, V.; Chelariu, A.-C.; Stoica, A.; Tocila, R.E.; et al. Cardiac Biomarkers and Risk Scores in Relation with History of Atherosclerotic Cardiovascular Disease in Patients Admitted with COVID-19: The Experience of an Eastern European Center. J. Clin. Med. 2022, 11, 5671. https://doi.org/10.3390/jcm11195671
Lionte C, Sorodoc V, Haliga RE, Bologa C, Ceasovschih A, Sirbu O, Gorciac V, Chelariu A-C, Stoica A, Tocila RE, et al. Cardiac Biomarkers and Risk Scores in Relation with History of Atherosclerotic Cardiovascular Disease in Patients Admitted with COVID-19: The Experience of an Eastern European Center. Journal of Clinical Medicine. 2022; 11(19):5671. https://doi.org/10.3390/jcm11195671
Chicago/Turabian StyleLionte, Catalina, Victorita Sorodoc, Raluca Ecaterina Haliga, Cristina Bologa, Alexandr Ceasovschih, Oana Sirbu, Victoria Gorciac, Andrei-Costin Chelariu, Alexandra Stoica, Roxana Elena Tocila, and et al. 2022. "Cardiac Biomarkers and Risk Scores in Relation with History of Atherosclerotic Cardiovascular Disease in Patients Admitted with COVID-19: The Experience of an Eastern European Center" Journal of Clinical Medicine 11, no. 19: 5671. https://doi.org/10.3390/jcm11195671