
Management of Out-of-Hospital Cardiac Arrest during COVID-19: A Tale of Two Cities
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Sources
2.3. Data Elements and Definitions
2.4. Statistical Analysis
3. Results
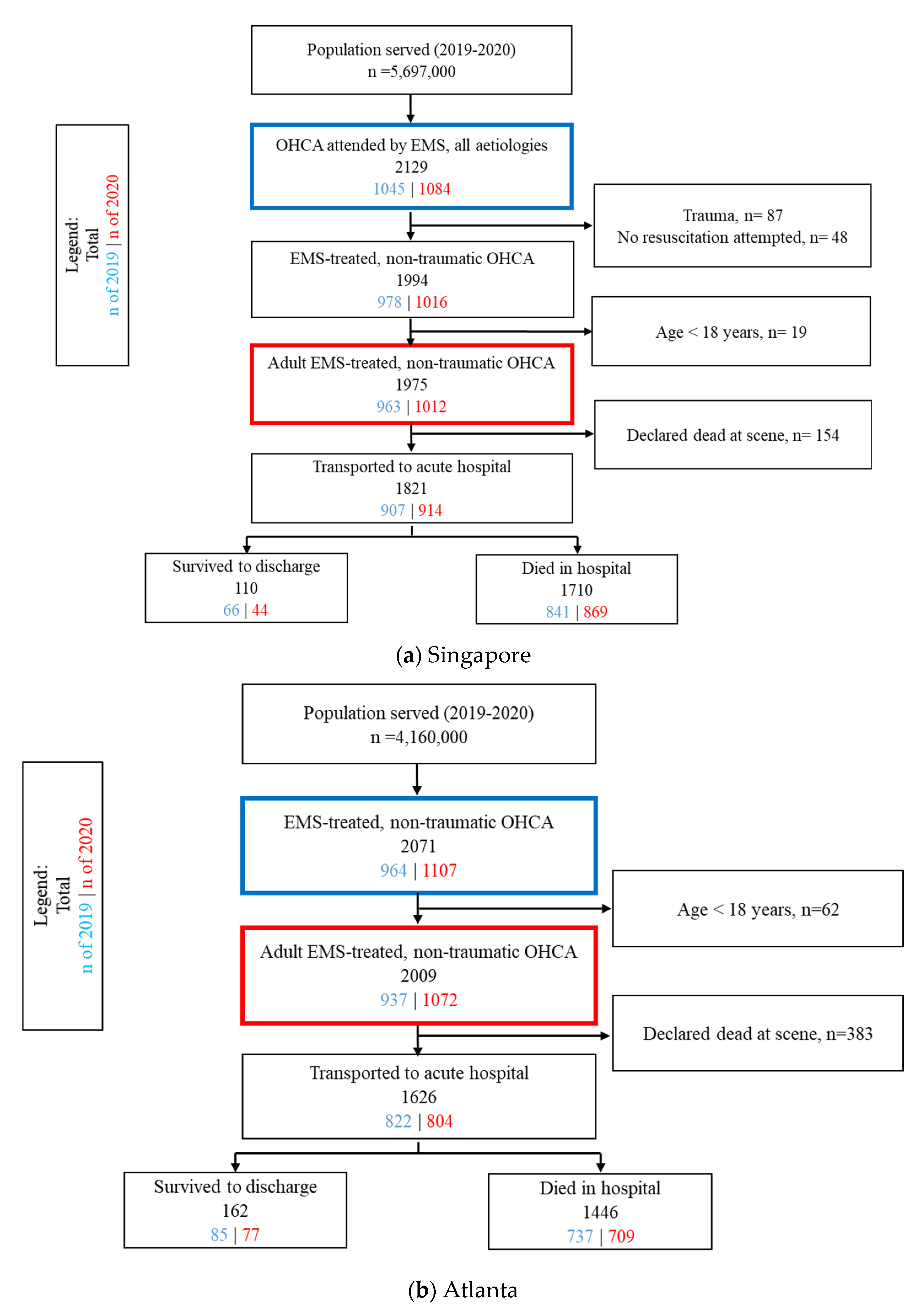
3.1. Overall Characteristics
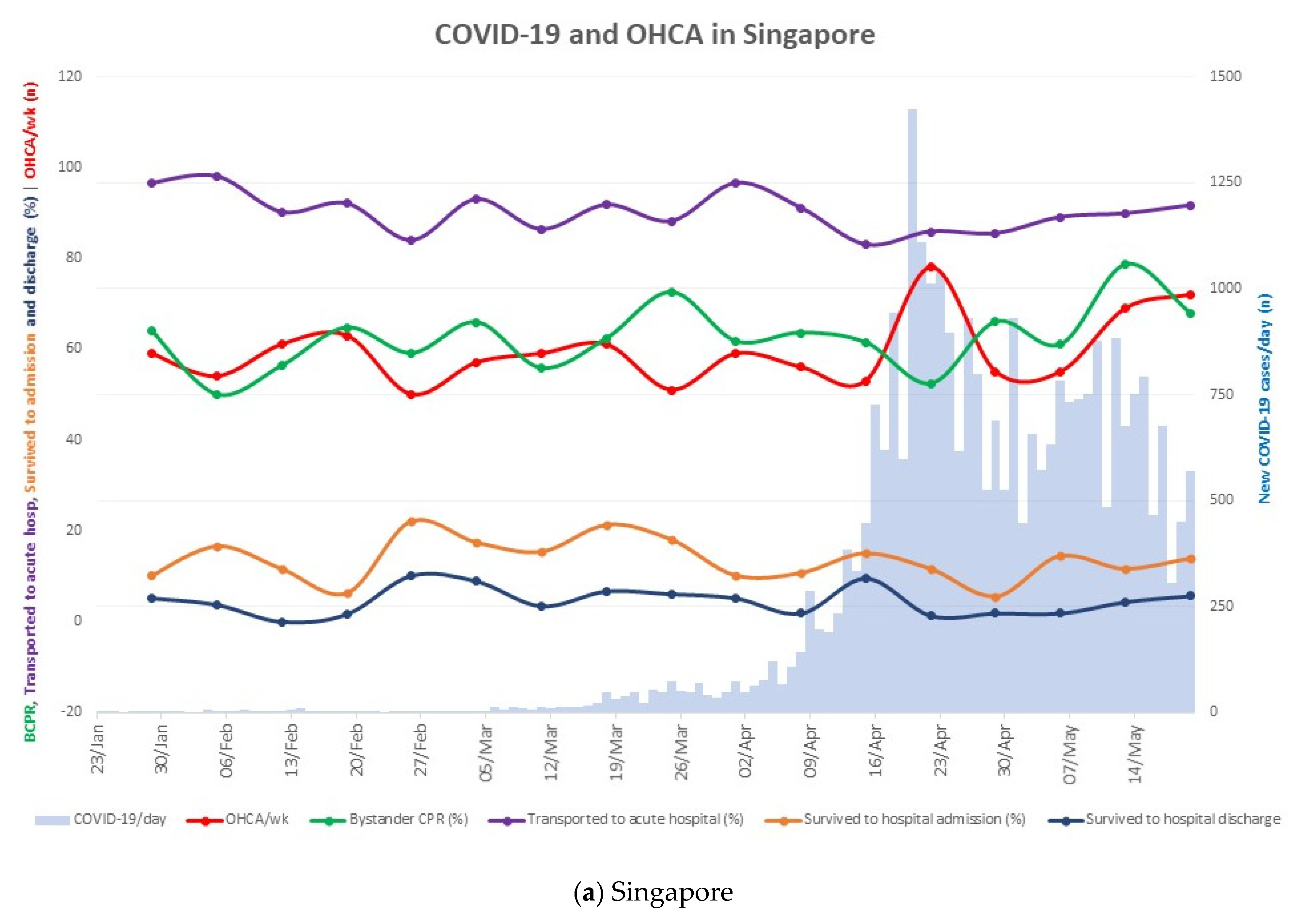
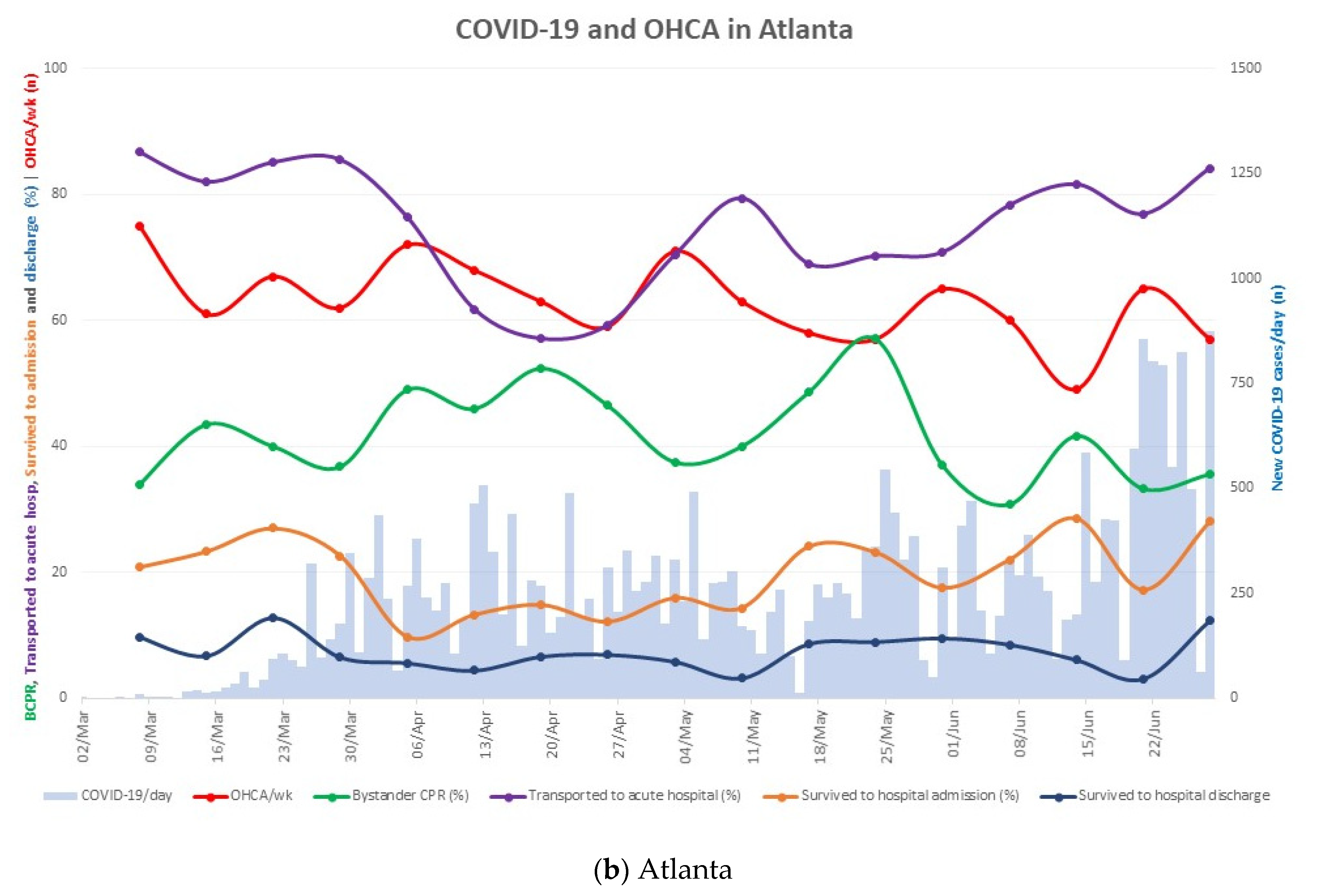
3.2. Changes in OHCA Epidemiology against the Backdrop of the COVID-19 Pandemic
3.3. Descriptive Comparison between Pandemic and Pre-Pandemic Periods in Singapore and Atlanta
3.4. Comparison between Pandemic and Pre-Pandemic Periods in Singapore and Atlanta by Logistic Regression
3.5. Comparison of the Impact of COVID-19 Pandemic between Singapore and Atlanta
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teoh, S.E.; Masuda, Y.; Tan, D.J.H.; Liu, N.; Morrison, L.J.; Ong, M.E.H.; Blewer, A.L.; Ho, A.F.W. Impact of the COVID-19 pandemic on the epidemiology of out-of-hospital cardiac arrest: A systematic review and meta-analysis. Ann. Intensive Care 2021, 11, 169. [Google Scholar] [CrossRef] [PubMed]
- Masuda, Y.; Teoh, S.E.; Yeo, J.W.; Tan, D.J.H.; Jimian, D.L.; Lim, S.L.; Ong, M.E.H.; Blewer, A.L.; Ho, A.F.W. Variation in community and ambulance care processes for out-of-hospital cardiac arrest during the COVID-19 pandemic: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 800. [Google Scholar] [CrossRef] [PubMed]
- Baldi, E.; Sech, G.M.; Mare, C.; Canevari, F.; Brancaglione, A.; Primi, R.; Klersy, C.; Palo, A.; Contri, E.; Ronchi, V.; et al. Out-of-Hospital Cardiac Arrest during the Covid-19 Outbreak in Italy. N. Engl. J. Med. 2020, 383, 496–498. [Google Scholar] [CrossRef]
- Lai, P.H.; Lancet, E.A.; Weiden, M.D.; Webber, M.P.; Zeig-Owens, R.; Hall, C.B.; Prezant, D.J. Characteristics Associated with Out-of-Hospital Cardiac Arrests and Resuscitations During the Novel Coronavirus Disease 2019 Pandemic in New York City. JAMA Cardiol. 2020, 5, 1154–1163. [Google Scholar] [CrossRef] [PubMed]
- Marijon, E.; Karam, N.; Jost, D.; Perrot, D.; Frattini, B.; Derkenne, C.; Sharifzadehgan, A.; Waldmann, V.; Beganton, F.; Narayanan, K.; et al. Out-of-hospital cardiac arrest during the COVID-19 pandemic in Paris, France: A population-based, observational study. Lancet Public Health 2020, 5, e437–e443. [Google Scholar] [CrossRef]
- Ball, J.; Nehme, Z.; Bernard, S.; Stub, D.; Stephenson, M.; Smith, K. Collateral damage: Hidden impact of the COVID-19 pandemic on the out-of-hospital cardiac arrest system-of-care. Resuscitation 2020, 156, 157–163. [Google Scholar] [CrossRef]
- Lim, S.L.; Shahidah, N.; Saffari, S.E.; Ng, Q.X.; Ho, A.F.W.; Leong, B.S.; Arulanandam, S.; Siddiqui, F.J.; Ong, M.E.H. Impact of COVID-19 on Out-of-Hospital Cardiac Arrest in Singapore. Int. J. Environ. Res. Public Health 2021, 18, 3646. [Google Scholar] [CrossRef] [PubMed]
- Elmer, J.; Okubo, M.; Guyette, F.X.; Martin-Gill, C. Indirect effects of COVID-19 on OHCA in a low prevalence region. Resuscitation 2020, 156, 282–283. [Google Scholar] [CrossRef] [PubMed]
- Sayre, M.R.; Barnard, L.M.; Counts, C.R.; Drucker, C.J.; Kudenchuk, P.J.; Rea, T.D.; Eisenberg, M.S. Prevalence of COVID-19 in Out-of-Hospital Cardiac Arrest. Circulation 2020, 142, 507–509. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Singapore. COVID-19 Situation Report. Available online: https://www.moh.gov.sg/docs/librariesprovider5/local-situation-report/situation-report---31-may-2020.pdf (accessed on 13 September 2020).
- COVID-19 Daily Status Report. 2020. Available online: https://dph.georgia.gov/covid-19-daily-status-report (accessed on 31 July 2021).
- Lim, S.L.; Smith, K.; Dyson, K.; Chan, S.P.; Earnest, A.; Nair, R.; Bernard, S.; Leong, B.S.; Arulanandam, S.; Ng, Y.Y.; et al. Incidence and Outcomes of Out-of-Hospital Cardiac Arrest in Singapore and Victoria: A Collaborative Study. J. Am. Heart Assoc. 2020, 9, e015981. [Google Scholar] [CrossRef] [PubMed]
- Blewer, A.L.; Ho, A.F.W.; Shahidah, N.; White, A.E.; Pek, P.P.; Ng, Y.Y.; Mao, D.R.; Tiah, L.; Chia, M.Y.; Leong, B.S.; et al. Impact of bystander-focused public health interventions on cardiopulmonary resuscitation and survival: A cohort study. Lancet Public Health 2020, 5, e428–e436. [Google Scholar] [CrossRef]
- Singapore Civil Defence Force. Fire, Emergency Medical Services and Enforcement Statistics 2019. Available online: https://www.scdf.gov.sg/docs/default-source/scdf-library/amb-fire-inspection-statistics/scdf-annual-statistics-2019.pdf (accessed on 31 July 2021).
- Ministry of Health Singapore. Confirmed Imported Case of Novel Coronavirus Infection in Singapore; Multi-Ministry Taskforce Ramps Up Precautionary Measures. Available online: https://www.moh.gov.sg/news-highlights/details/confirmed-imported-case-of-novel-coronavirus-infection-in-singapore-multi-ministry-taskforce-ramps-up-precautionary-measures (accessed on 31 July 2021).
- Ministry of Health Singapore. Risk Assessment Raised to DORSCON Orange. Available online: https://www.moh.gov.sg/news-highlights/details/risk-assessment-raised-to-dorscon-orange (accessed on 31 July 2021).
- Ministry of Health Singapore. End of Circuit Breaker, Phased Approach to Resuming Activities Safely 2020. Available online: https://www.moh.gov.sg/news-highlights/details/end-of-circuit-breaker-phased-approach-to-resuming-activities-safely (accessed on 31 July 2021).
- United States Census Bureau. QuickFacts. Available online: https://www.census.gov/quickfacts (accessed on 31 July 2021).
- Georgia Deaprtment of Public Health. Gov. Kemp, Officials Confirm Two Cases of COVID-19 in Georgia. Available online: https://dph.georgia.gov/press-releases/2020-03-02/gov-kemp-officials-confirm-two-cases-covid-19-georgia (accessed on 31 July 2021).
- Georgia Department of Public Health. State of Georgia, Department of Public Health, Administrative Order for Public Health Control Measures. Available online: https://dph.georgia.gov/state-georgia-department-public-health-administrative-order-public-health-control-measure (accessed on 31 July 2021).
- Department of Statistics Singapore. Population Trends 2019. Available online: https://tablebuilder.singstat.gov.sg/table/TS/M810001#! (accessed on 31 July 2021).
- Georgia Department of Public Health. Georgia OEMS COVID-19 Guidance. Available online: https://dph.georgia.gov/EMS/oems-covid-19 (accessed on 31 July 2021).
- Centers for Disease Control and Prevention. Interim Recommendations for Emergency Medical Services (EMS) Systems and 911 Public Safety Answering Points/Emergency Communication Centers (PSAP/ECCs) in the United States during the Coronavirus Disease (COVID-19) Pandemic. Available online: https://stacks.cdc.gov/view/cdc/90581 (accessed on 31 July 2021).
- Ong, M.E.; Shin, S.D.; Tanaka, H.; Ma, M.H.; Khruekarnchana, P.; Hisamuddin, N.; Atilla, R.; Middleton, P.; Kajino, K.; Leong, B.S.; et al. Pan-Asian Resuscitation Outcomes Study (PAROS): Rationale, methodology, and implementation. Acad. Emerg. Med. 2011, 18, 890–897. [Google Scholar] [CrossRef]
- McNally, B.; Stokes, A.; Crouch, A.; Kellermann, A.L. CARES: Cardiac Arrest Registry to Enhance Survival. Ann. Emerg. Med. 2009, 54, 674–683.e2. [Google Scholar] [CrossRef]
- McNally, B.; Robb, R.; Mehta, M.; Vellano, K.; Valderrama, A.L.; Yoon, P.W.; Sasson, C.; Crouch, A.; Perez, A.B.; Merritt, R.; et al. Out-of-hospital cardiac arrest surveillance—Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005--December 31, 2010. MMWR Surveill. Summ. 2011, 60, 1–19. [Google Scholar]
- Perkins, G.D.; Jacobs, I.G.; Nadkarni, V.M.; Berg, R.A.; Bhanji, F.; Biarent, D.; Bossaert, L.L.; Brett, S.J.; Chamberlain, D.; de Caen, A.R.; et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update of the Utstein Resuscitation Registry Templates for Out-of-Hospital Cardiac Arrest: A statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Circulation 2015, 132, 1286–1300. [Google Scholar]
- Goh, E.S.; Liang, B.; Fook-Chong, S.; Shahidah, N.; Soon, S.S.; Yap, S.; Leong, B.; Gan, H.N.; Foo, D.; Tham, L.P.; et al. Effect of location of out-of-hospital cardiac arrest on survival outcomes. Ann. Acad. Med. Singap. 2013, 42, 437–444. [Google Scholar]
- Han, M.X.; Yeo, A.; Ong, M.E.H.; Smith, K.; Lim, Y.L.; Lin, N.H.; Tan, B.; Arulanandam, S.; Ho, A.F.W.; Ng, Q.X. Cardiac Arrest Occurring in High-Rise Buildings: A Scoping Review. J. Clin. Med. 2021, 10, 4684. [Google Scholar] [CrossRef]
- Edelson, D.P.; Sasson, C.; Chan, P.S.; Atkins, D.L.; Aziz, K.; Becker, L.B.; Berg, R.A.; Bradley, S.M.; Brooks, S.C.; Cheng, A.; et al. Interim Guidance for Basic and Advanced Life Support in Adults, Children, and Neonates With Suspected or Confirmed COVID-19: From the Emergency Cardiovascular Care Committee and Get With The Guidelines-Resuscitation Adult and Pediatric Task Forces of the American Heart Association. Circulation 2020, 141, e933–e943. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Singapore | Atlanta | |
|---|---|---|
| Geography | ||
| Land size | 728.3 km2 | 7587.6 km2 8 counties (Cobb, Clayton, DeKalb, Douglas, Fulton, Gwinnett, Newton and Rockdale) |
| Population (2019 estimates) [18,21] | 5,704,000 | 4,160,864 |
| Population density | 7832 persons per km2 | 548 persons per km2 |
| EMS systems | ||
| Number of agencies | One national EMS agency, the Singapore Civil Defense Force Fire-based system activated by a centralised 995 dispatch system | 13 EMS agencies serving these 8 counties A combination of fire-based, hospital-based, third party and volunteer systems A centralised 911 PSAP/ECC connects the call to the agency serving the area |
| Response to OHCA | Community first responders activated by mobile applications Multi-tier response to OHCA commenced April 2019
Transport to the nearest restructured hospital Protocols for withholding and terminating resuscitation, with the latter commencing in January 2019 | EMS providers are EMT-I, EMT-A and paramedics Multi-tier response to OHCA
Encouraged to resuscitate in place and transport once ROSC obtained unless witnessed arrest, traumatic arrest, refractory VF or public setting. OHCA patients are transported to appropriately resourced Emergency Cardiac Centres (designated by Levels ie Levels I, II and III). |
| Training/Skills | EMT-B equivalents need to undergo 5 weeks of training. They are BLS-certified and able to carry out defibrillation. EMT-I equivalents require 15 months of training, and are able to administer IV and IO drugs, as well as insert laryngeal mask airway. | EMT-I/A undergo 20 weeks; 303 contact hours of training. They are BLS-certified and able to use an AED, insert supraglottic airway, IV/IO and administer fluids and dextrose. Paramedics undergo 16 months; minimum 1084 contact hours of training and are able to provide ALS level of care including manual defibrillation, intubation, IV/IO and administer ALS medication including epinephrine/amiodarone and atropine. |
| COVID-19 Epidemiology * | ||
| Incidence | 29,320 cumulative new cases Incidence rate of 514 per 100,000 population [10] | 29,005 cumulative new cases Incidence rate of 697 per 100,000 population [11] |
| Mortality | 22 deaths Case-fatality rate of 0.08% | 1034 deaths Case-fatality rate of 3.6% |
| Response to COVID-19 | ||
| Public | Disease Outbreak Response System Condition (DORSCON) raised to Orange on 7 February 2020 Additional public health measures and travel advisories imposed on 6 March in response to increasing community transmissions Partial national lockdown from 3 April to 2 June 2020
Mandatory mask wearing imposed on all >2 years of age from 14 April 2020, which is still in place | Public health state of emergency declared in Georgia on 14 March 2020 (last beyond study period)
Closure of public elementary, secondary and post-secondary schools in Georgia from 18 to 31 March 2020. This was subsequently extended through the end of 2019–2020 school year. Additional measures: isolation, quarantine and shelter regulations, increased social distancing measures Gradual re-starting of the economy from 24 April 2021 |
| EMS | Non-emergent, COVID-19 suspect cases were managed by a separate dedicated fleet of ambulances managed by a separate call center (operated by centralised “993” dispatch system) Single-tier response to OHCA from 7 February 2020 onwards, where fast response bikes and fire appliances stopped being deployed All ambulance personnel operate in full PPE for every emergency case attended All ambulance personnel to don PPE prior | Modified caller queries about SARS-CoV-2 infection
Universal source control measures
Universal use of PPE in areas with moderate to substantial community transmission, optional in areas with low community transmission [22] Encourage physical distancing
Guidance on management of those with suspected or confirmed COVID-19, including PPE, aerosol-generating procedures, advanced life support, transport to a healthcare facility and cleaning of vehicle following transport [23] |
| Singapore N = 1975 | Atlanta N = 2009 | p-Value *** | |
|---|---|---|---|
| Demographics | |||
| Age in years, median [Q1, Q3] | 72.0 [61.0, 83.0] | 66.0 [54.0, 76.0] | <0.001 |
| Male gender, n (%) | 1266 (64.1%) | 1130 (56.2%) | <0.001 |
| Event information, n (%) | |||
| Arrest location | <0.001 | ||
| 1532 (77.6%) | 1412 (70.3%) | |
| 183 (9.3%) | 369 (18.4%) | |
| 260 (13.2%) | 228 (11.3%) | |
| Presumed cardiac aetiology | 1781 (90.2%) | 1742 (86.7%) | <0.001 |
| Initial shockable rhythm | 316 (16.0%) | 333 (16.6%) | 0.654 |
| Witnessed arrest | |||
| 919 (46.5%) | 966 (48.1%) | |
| 858 (43.4%) | 758 (37.7%) | <0.001 |
| 198 (10.0%) | 285 (14.2%) | |
| Pre-hospital resuscitation, n(%) | |||
| Bystander CPR | 1049 (65.0%) | 574 (41.4%) | <0.001 |
| Bystander AED application | 66 (28.6%) | 20 (10.1%) | <0.001 |
| Pre-hospital defibrillation | 462 (23.4%) | 535 (26.6%) | 0.020 |
| EMS response times in min, median [Q1, Q3) * | |||
| EMS response time | 8.28 [6.76, 10.2] | 9.00 [6.43, 12.0] | <0.001 |
| Total response time | 12.0 [10.0, 14.5] | 11.0 [8.38, 14.2) | <0.001 |
| 2.07 [1.53, 2.78] | 0.633 [0.133, 1.39] | <0.001 |
| 6.07 [4.70, 7.92] | 7.74 [5.12, 10.4] | <0.001 |
| 3.35 [2.07, 4.87] | 1.45 [0.917, 2.66] | <0.001 |
| Time at scene | 23.9 [20.5, 27.5] | 21.8 [16.0, 29.0] | 0.939 |
| Patient outcomes, n (%) ** | |||
| Transported | 1821 (92.2%) | 1626 (80.9%) | <0.001 |
| Survived to hospital admission | 308 (15.6%) | 425 (21.3%) | <0.001 |
| Survived to hospital discharge | 110 (5.6%) | 162 (8.1%) | 0.002 |
| Discharged with good neurological outcome | 93 (4.7%) | 114 (5.7%) | 0.174 |
| Singapore | Atlanta | |||
|---|---|---|---|---|
| Pandemic N = 1012 | Pre-Pandemic N = 963 | Pandemic N = 1072 | Pre-Pandemic N = 937 | |
| Demographics | ||||
| Age in years, median [Q1, Q3] | 73.0 [61.0, 84.0] | 72.0 [60.0, 83.0] | 66.0 [54.0, 76.0] | 66.0 [54.0, 77.0] |
| Male gender, n (%) | 654 (64.6%) | 612 (63.6%) | 581 (54.2%) | 549 (58.6%) |
| Event information, n (%) | ||||
| Arrest location | ||||
| 808 (79.8%) | 724 (75.2%) | 792 (73.9%) | 620 (66.2%) |
| 99 (9.8%) | 84 (8.7%) | 190 (17.7%) | 179 (19.1%) |
| 105 (10.4%) | 155 (16.1%) | 90 (8.4%) | 138 (14.7%) |
| Presumed cardiac aetiology | 928 (91.7%) | 853 (88.6%) | 913 (85.2%) | 829 (88.5%) |
| Initial shockable rhythm | 158 (15.6%) | 158 (16.4%) | 163 (15.2%) | 170 (18.1%) |
| Witnessed arrest | ||||
| 394 (38.9%) | 525 (54.5%) | 529 (49.3%) | 437 (46.6%) |
| 510 (50.4%) | 348 (36.1%) | 392 (36.6%) | 366 (39.1%) |
| 108 (10.7%) | 90 (9.4%) | 151 (14.1%) | 134 (14.3%) |
| Pre-hospital resuscitation, n (%) | ||||
| Bystander CPR | 511 (62.5%) | 538 (67.7%) | 309 (41.7%) | 265 (41.1%) |
| Bystander AED application | 19 (21.3%) | 47 (33.1%) | 7 (9.21%) | 13 (10.6%) |
| Pre-hospital defibrillation | 227 (22.4%) | 235 (24.4%) | 275 (25.7%) | 260 (27.7%) |
| EMS response times in min, median [Q1, Q3] * | ||||
| EMS response times | 8.6 [6.9, 10.5] | 8.0 [6.5, 9.8] | 9.4 [6.6, 12.3] | 9.0 [6.3, 11.9] |
| Total response time | 12.8 [10.8, 15.1] | 11.3 [9.34, 13.4] | 11.4 [8.8, 14.9] | 10.9 [8.0, 13.8] |
| 2.0 [1.5, 2.8] | 2.1 [1.6, 2.8] | 0.6 [0.1, 1.1] | 0.7 [0.1, 1.6] |
| 6.3 [4.9, 8.2] | 5.9 [4.5, 7.6] | 8.0 [5.3, 10.9] | 7.1 [5.0, 10.0] |
| 3.9 [2.7, 5.5] | 2.8 [1.6, 4.0] | 1.6 [1.0, 3.0] | 1.3 [0.8, 2.2] |
| Time at scene | 24.8 [21.3, 28.5] | 22.8 [19.6, 26.4] | 23.0 [17.5, 31.0] | 20.3 [15.2, 27.3] |
| Patient outcomes, n (%) ** | ||||
| Transported | 914 (90.3%) | 907 (94.2%) | 804 (75.0%) | 822 (87.7%) |
| Survived to hospital admission | 136 (13.5%) | 172 (17.9%) | 204 (19.4%) | 221 (23.6%) |
| Survived to hospital discharge | 44 (4.4%) | 66 (6.9%) | 77 (7.3%) | 85 (9.1%) |
| Discharged with good neurological outcome | 36 (3.6%) | 57 (5.9%) | 54 (5.1%) | 60 (6.4%) |
| Variable | Event vs. Reference Level | Pandemic vs. Pre-Pandemic | ||||
|---|---|---|---|---|---|---|
| Singapore | Atlanta | Singapore vs. Atlanta * | ||||
| Adjusted OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | p Value | ||
| OHCA characteristics 1 | ||||||
| Location type | Home vs. Non-home | 2.05 (1.50, 2.80) | <0.001 | 2.03 (1.47, 2.81) | <0.001 | NS |
| Witnessed arrest | Yes vs. No | 1.96 (1.59, 2.40) | <0.001 | 0.96 (0.77, 1.19) | 0.683 | <0.001 |
| Bystander CPR | Yes vs. No | 0.81 (0.66, 0.99) | 0.049 | 1.07 (0.86, 1.34) | 0.536 | 0.042 |
| Clinical Outcomes 2 | ||||||
| Transport to acute hospital | Yes vs. No | 0.59 (0.41,0.85) | 0.005 | 0.36 (0.26,0.50) | <0.001 | 0.096 |
| Survived to admission | Yes vs. No | 0.74 (0.54, 1.00) | 0.053 | 0.83 (0.63, 1.01) | 0.186 | NS |
| Survived to discharge | Yes vs. No | 0.72 (0.43, 1.20) | 0.208 | 1.10 (0.71, 1.71) | 0.660 | NS |
| Discharged with good neurological outcome | Yes vs. No | 0.64 (0.37, 1.13) | 0.127 | 1.02 (0.61, 1.69) | 0.948 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.L.; Kumar, L.; Saffari, S.E.; Shahidah, N.; Al-Araji, R.; Ng, Q.X.; Ho, A.F.W.; Arulanandam, S.; Leong, B.S.-H.; Liu, N.; et al. Management of Out-of-Hospital Cardiac Arrest during COVID-19: A Tale of Two Cities. J. Clin. Med. 2022, 11, 5177. https://doi.org/10.3390/jcm11175177
Lim SL, Kumar L, Saffari SE, Shahidah N, Al-Araji R, Ng QX, Ho AFW, Arulanandam S, Leong BS-H, Liu N, et al. Management of Out-of-Hospital Cardiac Arrest during COVID-19: A Tale of Two Cities. Journal of Clinical Medicine. 2022; 11(17):5177. https://doi.org/10.3390/jcm11175177
Chicago/Turabian StyleLim, Shir Lynn, Lekshmi Kumar, Seyed Ehsan Saffari, Nur Shahidah, Rabab Al-Araji, Qin Xiang Ng, Andrew Fu Wah Ho, Shalini Arulanandam, Benjamin Sieu-Hon Leong, Nan Liu, and et al. 2022. "Management of Out-of-Hospital Cardiac Arrest during COVID-19: A Tale of Two Cities" Journal of Clinical Medicine 11, no. 17: 5177. https://doi.org/10.3390/jcm11175177