
Underweight Is Associated with a Higher Risk of Acute Pancreatitis in Type 2 Diabetes: A Nationwide Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Subjects
2.2. Definitions of Acute Pancreatitis and Chronic Diseases
2.3. Assessment of Obesity and Glycemic Status
2.4. Lifestyle Behaviors and Economic Status
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
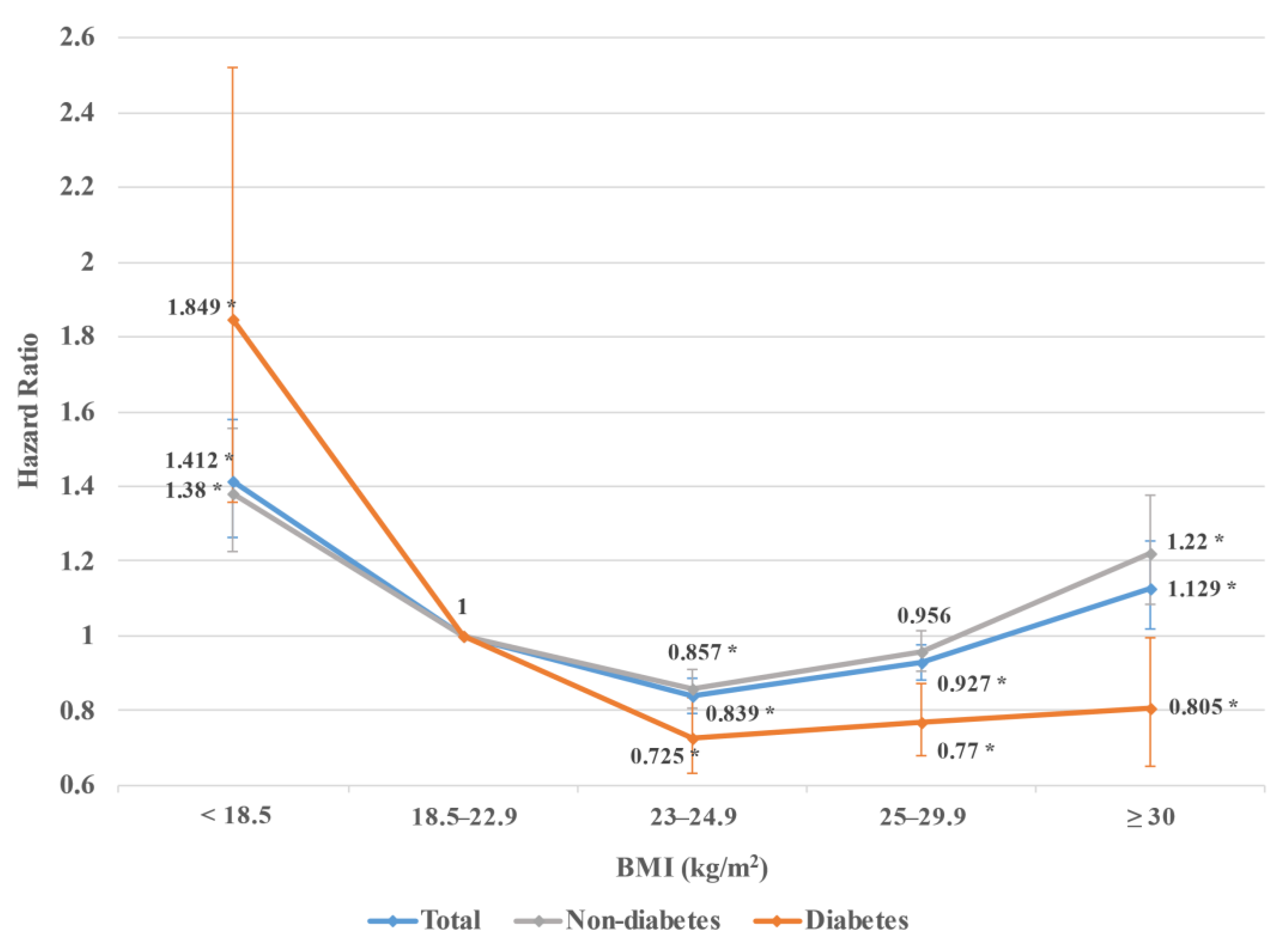
3.2. Risk of Acute Pancreatitis for Each BMI Group Depending on the Presence or Absence of Type 2 Diabetes
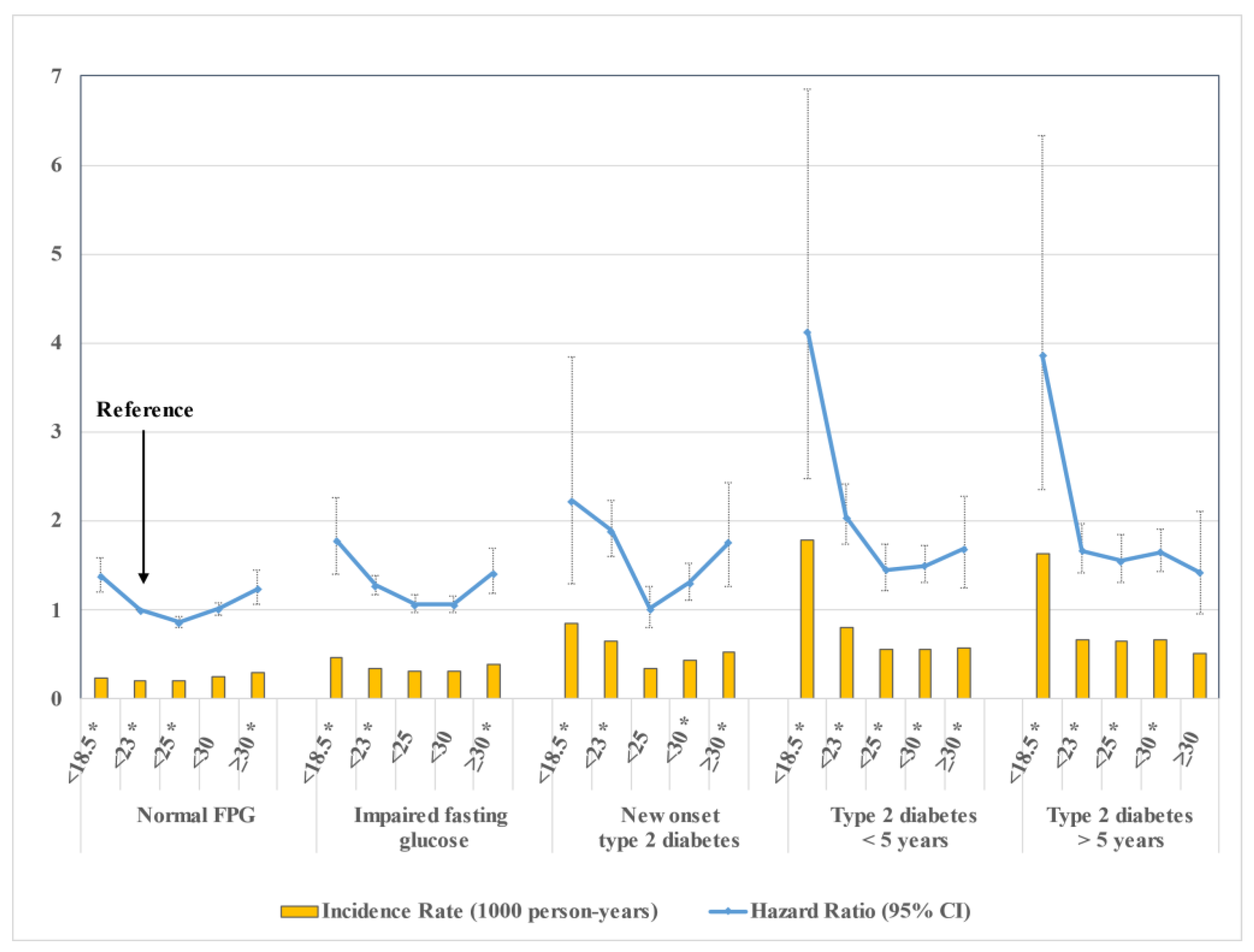
3.3. Risk of Acute Pancreatitis According to Glycemic Status and BMI Category
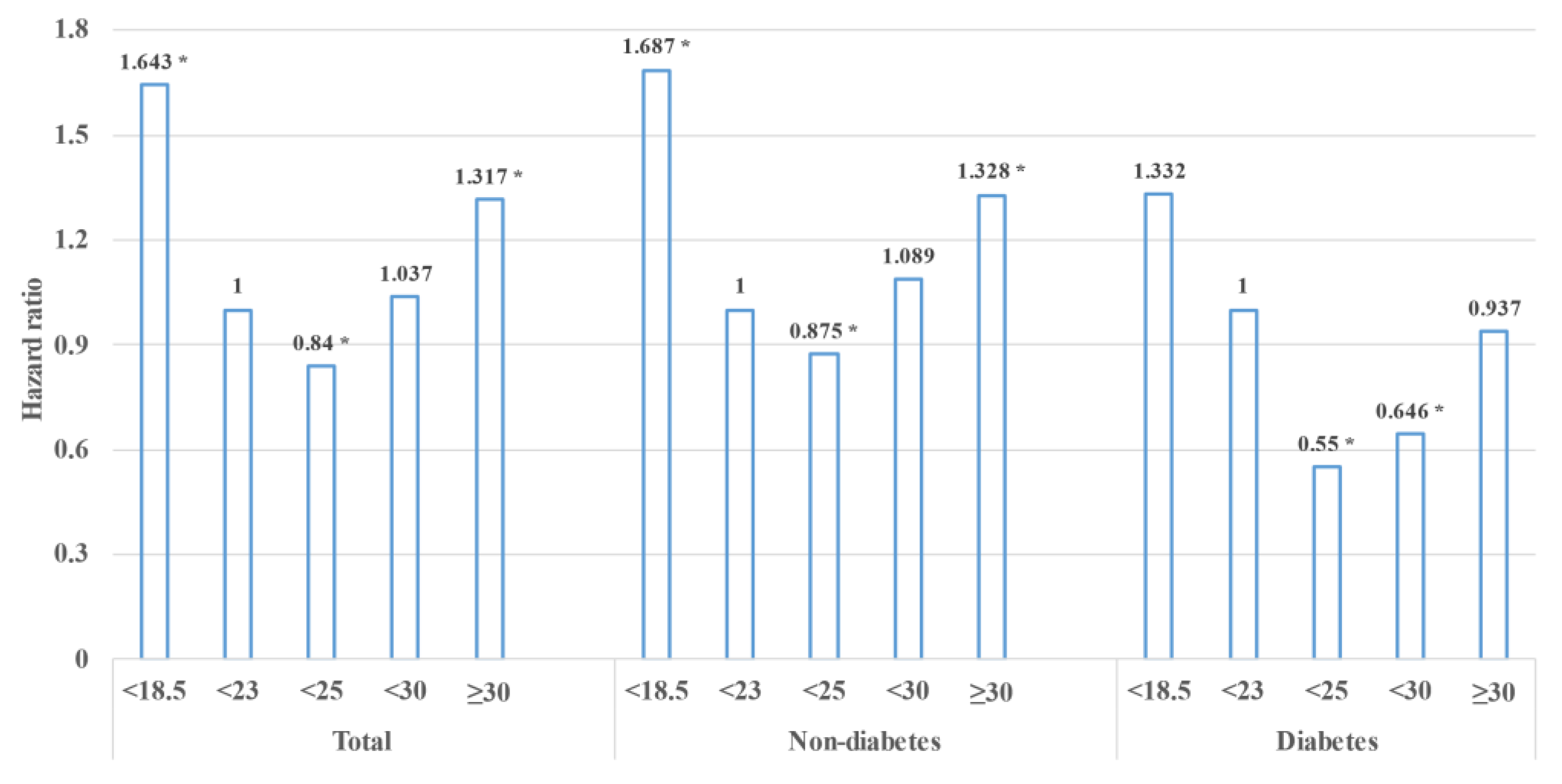
3.4. Subgroup Analysis with Constant BMI
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mederos, M.A.; Reber, H.A.; Girgis, M.D. Acute Pancreatitis: A Review. JAMA 2021, 325, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Xiao, A.Y.; Tan, M.L.Y.; Wu, L.M.; Asrani, V.M.; Windsor, J.A.; Yadav, D.; Petrov, M.S. Global incidence and mortality of pancreatic diseases: A systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol. Hepatol. 2016, 1, 45–55. [Google Scholar] [CrossRef]
- Roberts, S.E.; Morrison-Rees, S.; John, A.; Williams, J.G.; Brown, T.H.; Samuel, D.G. The incidence and aetiology of acute pancreatitis across Europe. Pancreatology 2017, 17, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Kingsnorth, A.; O’Reilly, D. Acute pancreatitis. BMJ 2006, 332, 1072–1076. [Google Scholar] [CrossRef]
- Aune, D.; Vatten, L.J. Diabetes mellitus and the risk of gallbladder disease: A systematic review and meta-analysis of prospective studies. J. Diabetes Complicat. 2016, 30, 368–373. [Google Scholar] [CrossRef]
- Girman, C.J.; Kou, T.D.; Cai, B.; Alexander, C.M.; O’Neill, E.A.; Williams-Herman, D.E.; Katz, L. Patients with type 2 diabetes mellitus have higher risk for acute pancreatitis compared with those without diabetes. Diabetes Obes. Metab. 2010, 12, 766–771. [Google Scholar] [CrossRef]
- Urushihara, H.; Taketsuna, M.; Liu, Y.; Oda, E.; Nakamura, M.; Nishiuma, S.; Maeda, R. Increased risk of acute pancreatitis in patients with type 2 diabetes: An observational study using a Japanese hospital database. PLoS ONE 2012, 7, e53224. [Google Scholar]
- Shen, H.N.; Chang, Y.-H.; Chen, H.-F.; Lu, C.-L.; Li, C.-Y. Increased risk of severe acute pancreatitis in patients with diabetes. Diabet Med. 2012, 29, 1419–1424. [Google Scholar] [CrossRef]
- Hong, S.; Qiwen, B.; Ying, J.; Wei, A.; Chaoyang, T. Body mass index and the risk and prognosis of acute pancreatitis: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2011, 23, 1136–1143. [Google Scholar] [CrossRef]
- Hansen, S.E.J.; Madsen, C.M.; Varbo, A.; Nordestgaard, B.G. Body Mass Index, Triglycerides, and Risk of Acute Pancreatitis: A Population-Based Study of 118 000 Individuals. J. Clin. Endocrinol. Metab. 2020, 105, 163–174. [Google Scholar] [CrossRef]
- Coleman, N.J.; Miernik, J.; Philipson, L.; Fogelfeld, L. Lean versus obese diabetes mellitus patients in the United States minority population. J. Diabetes Complicat. 2014, 28, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.S.; Yi, S.W.; Park, J.W.; Lee, S.; Jeong, S.-H.; Yi, J.-J.; Han, K.J. Body mass index and the risk of acute pancreatitis by etiology: A prospective analysis of Korean National Screening Cohort. J. Gastroenterol. Hepatol. 2019, 34, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.W.; Cho, B.; Guallar, E. Korean National Health Insurance Database. JAMA Intern. Med. 2016, 176, 138. [Google Scholar] [CrossRef]
- Floyd, A.; Pedersen, L.; Nielsen, G.L.; Thorladcius-Ussing, O.; Sorensen, H.T. Secular trends in incidence and 30-day case fatality of acute pancreatitis in North Jutland County, Denmark: A register-based study from 1981–2000. Scand. J. Gastroenterol. 2002, 37, 1461–1465. [Google Scholar] [CrossRef]
- Razavi, D.; Ljung, R.; Lu, Y.; Andrén-Sandberg, A.; Lindblad, M. Reliability of acute pancreatitis diagnosis coding in a National Patient Register: A validation study in Sweden. Pancreatology 2011, 11, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F.; Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and its Treatment; Health Communications Australia: Melbourne, Australia, 2000. [Google Scholar]
- Kim, E.S.; Jeong, J.S.; Han, K.; Kim, M.K.; Lee, S.-H.; Park, Y.-M.; Baek, K.H.; Moon, S.D.; Han, J.-H.; Song, K.-H.; et al. Impact of weight changes on the incidence of diabetes mellitus: A Korean nationwide cohort study. Sci. Rep. 2018, 8, 3735. [Google Scholar] [CrossRef] [PubMed]
- Lindkvist, B.; Appelros, S.; Manjer, J.; Berglund, G.; Borgstrom, A. A prospective cohort study of smoking in acute pancreatitis. Pancreatology 2008, 8, 63–70. [Google Scholar] [CrossRef]
- Blomgren, K.B.; Sundström, A.; Steineck, G.; Wiholm, B.E. Obesity and treatment of diabetes with glyburide may both be risk factors for acute pancreatitis. Diabetes Care 2002, 25, 298–302. [Google Scholar] [CrossRef]
- Noel, R.A.; Braun, D.K.; Patterson, R.E.; Bloomgren, G.L. Increased risk of acute pancreatitis and biliary disease observed in patients with type 2 diabetes: A retrospective cohort study. Diabetes Care 2009, 32, 834–838. [Google Scholar] [CrossRef]
- Zhang, Y.; Guo, Y.; Shen, X.; Zhao, F.; Yan, S. Lower body mass index is not of more benefit for diabetic complications. J. Diabetes Investig. 2019, 10, 1307–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohan, V.; Vijayaprabha, R.; Rema, M.; Premalatha, G.; Poongothai, S.; Deepa, R.; Bhatia, E.; Mackay, I.; Zimmet, P. Clinical profile of lean NIDDM in South India. Diabetes Res. Clin. Pract. 1997, 38, 101–108. [Google Scholar] [CrossRef]
- Preiss, D.; Tikkanen, M.J.; Welsh, P.; Ford, I.; Lovato, L.C.; Elam, M.B.; LaRosa, J.C.; DeMicco, D.A.; Colhoun, H.M.; Goldenberg, I.; et al. Lipid-modifying therapies and risk of pancreatitis: A meta-analysis. JAMA 2012, 308, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Norat, T.; Vatten, L.J. Body mass index, abdominal fatness and the risk of gallbladder disease. Eur. J. Epidemiol. 2015, 30, 1009–1019. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients without Diabetes and with a BMI < 18.5 | Patients without Diabetes and with a BMI ≥ 18.5 | Patients with Diabetes and with a BMI < 18.5 | Patients with Diabetes and with a BMI ≥ 18.5 | Absolute Standardized Difference (Max) | |
|---|---|---|---|---|---|
| (n = 140,516) | (n = 3,430,160) | (n = 4846) | (n = 336,974) | ||
| Age, years | 39.81 ± 16.29 | 46.45 ± 13.65 | 59.7 ± 15.74 | 57.26 ± 12.01 | 1.242 |
| Male sex | 45,163 (32.14) | 1,878,366 (54.76) | 2877 (59.37) | 20,6840 (61.38) | 0.613 |
| BMI, kg/m2 | 17.57 ± 0.79 | 23.82 ± 3.29 | 17.43 ± 0.93 | 25.14 ± 3.2 | 3.272 |
| Waist circumference, cm | 66 ± 5.69 | 80.28 ± 9.1 | 70.27 ± 6.43 | 85.71 ± 8.77 | 2.666 |
| Blood pressure, mmHg | |||||
| Systolic | 113.33 ± 13.83 | 122.15 ± 14.76 | 123.08 ± 17.71 | 129.28 ± 15.82 | 1.073 |
| Diastolic | 71.12 ± 9.23 | 76.25 ± 9.99 | 75.67 ± 10.84 | 79.17 ± 10.24 | 0.826 |
| Alcohol | 0.257 | ||||
| Nondrinker | 79,717 (56.73) | 1,747,393 (50.94) | 3022 (62.36) | 191,982 (56.97) | |
| Mild | 54,833 (39.02) | 1,413,461 (41.21) | 1408 (29.05) | 111,272 (33.02) | |
| Heavy | 5966 (4.25) | 269,306 (7.85) | 416 (8.58) | 33,720 (10.01) | |
| Smoking | 0.372 | ||||
| Nonsmoker | 99,667 (70.93) | 2,043,383 (59.57) | 2577 (53.18) | 187,838 (55.74) | |
| Former | 9438 (6.72) | 488,384 (14.24) | 567 (11.7) | 62010 (18.4) | |
| Current | 31,411 (22.35) | 898,393 (26.19) | 1702 (35.12) | 87,126 (25.86) | |
| Glucose, mg/dL | 88.55 ± 10.71 | 92.73 ± 11.52 | 156.57 ± 68.39 | 146.51 ± 49.38 | 1.622 |
| * Triglyceride, mg/dL | 73.89 (73.71–74.07) | 111.45 (111.38–111.51) | 102.47 (100.84–104.13) | 150.31 (150.01–150.61) | 0.989 |
| Total cholesterol, mg/dL | 177.69 ± 35.41 | 195.78 ± 40.99 | 184.91 ± 47.85 | 197.77 ± 47.76 | 0.478 |
| HDL cholesterol, mg/dL | 64.31 ± 37 | 56.5 ± 32.51 | 60.01 ± 35.34 | 52.67 ± 32.94 | 0.332 |
| LDL cholesterol, mg/dL | 118.62 ± 381.44 | 122.13 ± 213.86 | 105.53 ± 151.43 | 113.18 ± 99.48 | 0.090 |
| Hypertension | 12,522 (8.91) | 842,226 (24.55) | 2004 (41.35) | 201,813 (59.89) | 1.272 |
| Dyslipidemia | 6880 (4.9) | 565,078 (16.47) | 1012 (20.88) | 139,486 (41.39) | 0.960 |
| Insulin administration | 0 (0) | 0 (0) | 290 (5.98) | 12,687 (3.76) | 0.354 |
| Chronic kidney disease | 7459 (5.31) | 21,9381 (6.4) | 665 (13.72) | 42,446 (12.6) | 0.290 |
| Chronic pancreatitis | 213 (0.15) | 3460 (0.1) | 46 (0.95) | 874 (0.26) | 0.136 |
| Regular physical activity | 13,099 (9.32) | 61,3862 (17.9) | 730 (15.06) | 73,666 (21.86) | 0.351 |
| Low income | 31,586 (22.48) | 661,006 (19.27) | 1118 (23.07) | 69,326 (20.57) | 0.093 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.H.; Han, K.-D.; Cho, I.R.; Lee, I.S.; Ryu, J.K.; Kim, Y.-T.; Chung, K.H.; Lee, S.H. Underweight Is Associated with a Higher Risk of Acute Pancreatitis in Type 2 Diabetes: A Nationwide Cohort Study. J. Clin. Med. 2022, 11, 5641. https://doi.org/10.3390/jcm11195641
Choi YH, Han K-D, Cho IR, Lee IS, Ryu JK, Kim Y-T, Chung KH, Lee SH. Underweight Is Associated with a Higher Risk of Acute Pancreatitis in Type 2 Diabetes: A Nationwide Cohort Study. Journal of Clinical Medicine. 2022; 11(19):5641. https://doi.org/10.3390/jcm11195641
Chicago/Turabian StyleChoi, Young Hoon, Kyung-Do Han, In Rae Cho, In Seok Lee, Ji Kon Ryu, Yong-Tae Kim, Kwang Hyun Chung, and Sang Hyub Lee. 2022. "Underweight Is Associated with a Higher Risk of Acute Pancreatitis in Type 2 Diabetes: A Nationwide Cohort Study" Journal of Clinical Medicine 11, no. 19: 5641. https://doi.org/10.3390/jcm11195641