
Gastrointestinal and Liver Complications in Patients with Diabetes Mellitus—A Review of the Literature

Abstract
:1. Introduction
2. Diabetic Autonomic Neuropathy of the Gastrointestinal Tract
2.1. Gastroesophageal Reflux Disease (GERD)
2.2. Diabetic Gastroparesis
2.3. Diabetic Enteropathy
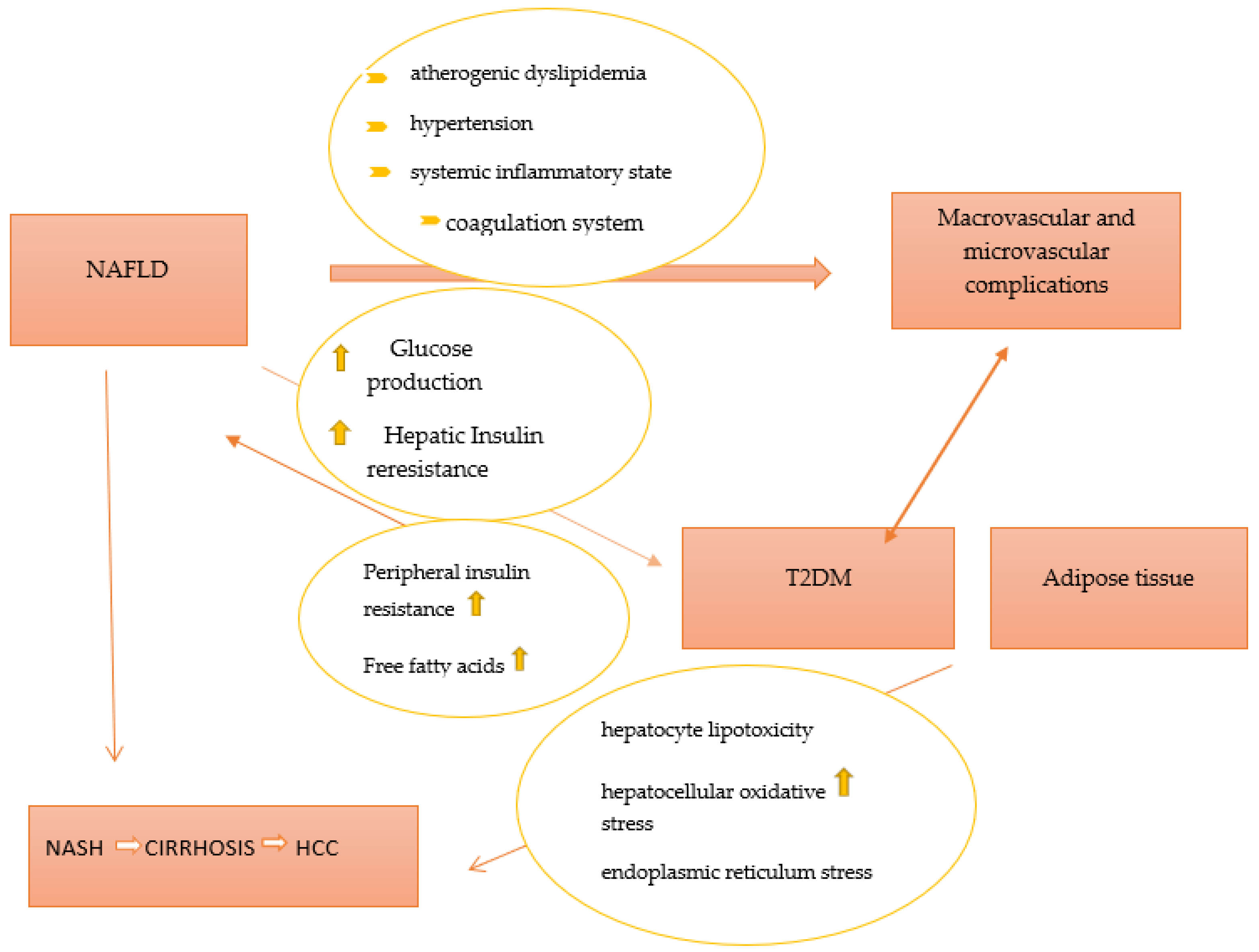
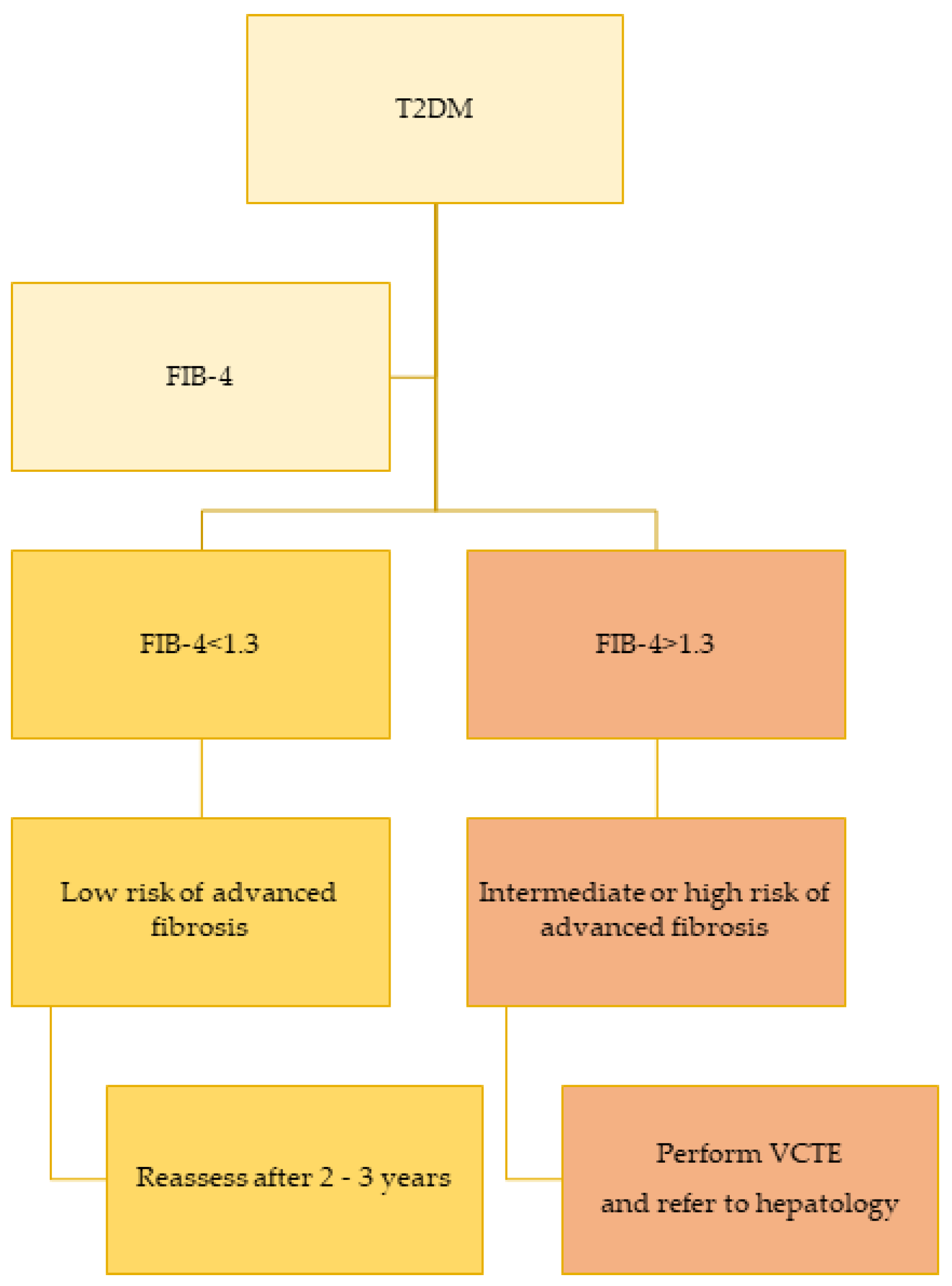
3. Non-Alcoholic Fatty Liver Disease and Diabetes
4. Association between Diabetes and Other GI Diseases
4.1. Diabetes and Gallbladder Stones
4.2. Diabetes and Helicobacter pylori Infection
4.3. Diabetes and Colorectal Cancer
4.4. Diabetes and Hemochromatosis
4.5. Diabetes and Celiac Disease
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, Regional and Country-Level Diabetes Prevalence Estimates for 2021 and Projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Bytzer, P.; Talley, N.J.; Leemon, M.; Young, L.J.; Jones, M.P.; Horowitz, M. Prevalence of Gastrointestinal Symptoms Associated with Diabetes Mellitus: A Population-Based Survey of 15,000 Adults. Arch. Intern. Med. 2001, 161, 1989–1996. [Google Scholar] [CrossRef]
- Koch, K.L.; Calles-Escandón, J. Diabetic Gastroparesis. Gastroenterol. Clin. N. Am. 2015, 44, 39–57. [Google Scholar] [CrossRef]
- Horowitz, M.; O’Donovan, D.; Jones, K.L.; Feinle, C.; Rayner, C.K.; Samsom, M. Gastric Emptying in Diabetes: Clinical Significance and Treatment. Diabet. Med. 2002, 19, 177–194. [Google Scholar] [CrossRef]
- Intagliata, N.; Koch, K.L. Gastroparesis in Type 2 Diabetes Mellitus: Prevalence, Etiology, Diagnosis, and Treatment. Curr. Gastroenterol. Rep. 2007, 9, 270–279. [Google Scholar] [CrossRef]
- Williamson, R.M.; Price, J.F.; Glancy, S.; Perry, E.; Nee, L.D.; Hayes, P.C.; Frier, B.M.; Van Look, L.A.F.; Johnston, G.I.; Reynolds, R.M.; et al. Prevalence of and Risk Factors for Hepatic Steatosis and Nonalcoholic Fatty Liver Disease in People with Type 2 Diabetes: The Edinburgh Type 2 Diabetes Study. Diabetes Care 2011, 34, 1139–1144. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee 4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45, S46–S59. [Google Scholar] [CrossRef]
- Rayner, C.K.; Samsom, M.; Jones, K.L.; Horowitz, M. Relationships of Upper Gastrointestinal Motor and Sensory Function with Glycemic Control. Diabetes Care 2001, 24, 371–381. [Google Scholar] [CrossRef]
- Kuźnik, E.; Dudkowiak, R.; Adamiec, R.; Poniewierka, E. Diabetic Autonomic Neuropathy of the Gastrointestinal Tract. Prz. Gastroenterol. 2020, 15, 89–93. [Google Scholar] [CrossRef]
- Young, C.F.; Moussa, M.; Shubrook, J.H. Diabetic Gastroparesis: A Review. Diabetes Spectr. 2020, 33, 290–297. [Google Scholar] [CrossRef]
- Parkman, H.P.; Hasler, W.L.; Fisher, R.S.; American Gastroenterological Association. American Gastroenterological Association Technical Review on the Diagnosis and Treatment of Gastroparesis. Gastroenterology 2004, 127, 1592–1622. [Google Scholar] [CrossRef]
- Maleki, D.; Locke, G.R.; Camilleri, M.; Zinsmeister, A.R.; Yawn, B.P.; Leibson, C.; Melton, L.J. Gastrointestinal Tract Symptoms among Persons with Diabetes Mellitus in the Community. Arch. Intern. Med. 2000, 160, 2808–2816. [Google Scholar] [CrossRef]
- Bharucha, A.E.; Camilleri, M.; Forstrom, L.A.; Zinsmeister, A.R. Relationship between Clinical Features and Gastric Emptying Disturbances in Diabetes Mellitus. Clin. Endocrinol. 2009, 70, 415–420. [Google Scholar] [CrossRef]
- Gill, R.C.; Murphy, P.D.; Hooper, H.R.; Bowes, K.L.; Kingma, Y.J. Effect of the Menstrual Cycle on Gastric Emptying. Digestion 1987, 36, 168–174. [Google Scholar] [CrossRef]
- Datz, F.L.; Christian, P.E.; Moore, J. Gender-Related Differences in Gastric Emptying. J. Nucl. Med. 1987, 28, 1204–1207. [Google Scholar]
- Soykan, I.; Sivri, B.; Sarosiek, I.; Kiernan, B.; McCallum, R.W. Demography, Clinical Characteristics, Psychological and Abuse Profiles, Treatment, and Long-Term Follow-up of Patients with Gastroparesis. Dig. Dis. Sci. 1998, 43, 2398–2404. [Google Scholar] [CrossRef]
- Parkman, H.P.; Yates, K.; Hasler, W.L.; Nguyen, L.; Pasricha, P.J.; Snape, W.J.; Farrugia, G.; Koch, K.L.; Calles, J.; Abell, T.L.; et al. Similarities and Differences between Diabetic and Idiopathic Gastroparesis. Clin. Gastroenterol. Hepatol. 2011, 9, 1056–1064, quiz e133-134. [Google Scholar] [CrossRef]
- Fritz, T.; Hünseler, C.; Broekaert, I. Assessment of Whole Gut Motility in Adolescents Using the Wireless Motility Capsule Test. Eur. J. Pediatr. 2022, 181, 1197–1204. [Google Scholar] [CrossRef]
- Bonfrate, L.; Grattagliano, I.; Palasciano, G.; Portincasa, P. Dynamic Carbon 13 Breath Tests for the Study of Liver Function and Gastric Emptying. Gastroenterol. Rep. 2015, 3, 12–21. [Google Scholar] [CrossRef]
- Koch, K.L. Chapter 15—Electrogastrography for Suspected Gastroparesis. In Gastroparesis; McCallum, R.W., Parkman, H.P., Eds.; Academic Press: Cambridge, MA, USA, 2021; pp. 189–205. ISBN 978-0-12-818586-5. [Google Scholar]
- Patcharatrakul, T.; Gonlachanvit, S. Technique of Functional and Motility Test: How to Perform Antroduodenal Manometry. J. Neurogastroenterol. Motil. 2013, 19, 395–404. [Google Scholar] [CrossRef]
- Drolet, B.; Rousseau, G.; Daleau, P.; Cardinal, R.; Turgeon, J. Domperidone Should Not Be Considered a No-Risk Alternative to Cisapride in the Treatment of Gastrointestinal Motility Disorders. Circulation 2000, 102, 1883–1885. [Google Scholar] [CrossRef]
- Lacy, B.E.; Tack, J.; Gyawali, C.P. AGA Clinical Practice Update on Management of Medically Refractory Gastroparesis: Expert Review. Clin. Gastroenterol. Hepatol. 2022, 20, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Bharucha, A.E.; Kudva, Y.C.; Prichard, D.O. Diabetic Gastroparesis. Endocr. Rev. 2019, 40, 1318–1352. [Google Scholar] [CrossRef] [PubMed]
- Frías Ordoñez, J.S.; Otero Regino, W. Chronic diarrhea in the diabetic. A review of the literature. Rev. Gastroenterol. Peru 2016, 36, 340–349. [Google Scholar] [PubMed]
- Reszczyńska, M.; Marczak-Karpina, B. Dysfunction of the Lower Gastrointestinal Tract as a Complication of Diabetes—A Problematic Issue in the Diabetic Care. Clin. Diabetol. 2016, 5, 95–99. [Google Scholar] [CrossRef]
- Gatopoulou, A.; Papanas, N.; Maltezos, E. Diabetic Gastrointestinal Autonomic Neuropathy: Current Status and New Achievements for Everyday Clinical Practice. Eur. J. Intern. Med. 2012, 23, 499–505. [Google Scholar] [CrossRef]
- Ojetti, V.; Pitocco, D.; Scarpellini, E.; Zaccardi, F.; Scaldaferri, F.; Gigante, G.; Gasbarrini, G.; Ghirlanda, G.; Gasbarrini, A. Small Bowel Bacterial Overgrowth and Type 1 Diabetes. Eur. Rev. Med. Pharm. Sci. 2009, 13, 419–423. [Google Scholar]
- Phillips, L.K.; Rayner, C.K.; Jones, K.L.; Horowitz, M. An Update on Autonomic Neuropathy Affecting the Gastrointestinal Tract. Curr. Diab. Rep. 2006, 6, 417–423. [Google Scholar] [CrossRef]
- Jung, H.-K.; Kim, D.-Y.; Moon, I.-H.; Hong, Y.-S. Colonic Transit Time in Diabetic Patients--Comparison with Healthy Subjects and the Effect of Autonomic Neuropathy. Yonsei Med. J. 2003, 44, 265–272. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The Diagnosis and Management of Non-Alcoholic Fatty Liver Disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef]
- Lonardo, A.; Nascimbeni, F.; Mantovani, A.; Targher, G. Hypertension, Diabetes, Atherosclerosis and NASH: Cause or Consequence? J. Hepatol. 2018, 68, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Pal, D.; Dasgupta, S.; Kundu, R.; Maitra, S.; Das, G.; Mukhopadhyay, S.; Ray, S.; Majumdar, S.S.; Bhattacharya, S. Fetuin-A Acts as an Endogenous Ligand of TLR4 to Promote Lipid-Induced Insulin Resistance. Nat. Med. 2012, 18, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Meex, R.C.; Hoy, A.J.; Morris, A.; Brown, R.D.; Lo, J.C.Y.; Burke, M.; Goode, R.J.A.; Kingwell, B.A.; Kraakman, M.J.; Febbraio, M.A.; et al. Fetuin B Is a Secreted Hepatocyte Factor Linking Steatosis to Impaired Glucose Metabolism. Cell Metab. 2015, 22, 1078–1089. [Google Scholar] [CrossRef] [PubMed]
- Norseen, J.; Hosooka, T.; Hammarstedt, A.; Yore, M.M.; Kant, S.; Aryal, P.; Kiernan, U.A.; Phillips, D.A.; Maruyama, H.; Kraus, B.J.; et al. Retinol-Binding Protein 4 Inhibits Insulin Signaling in Adipocytes by Inducing Proinflammatory Cytokines in Macrophages through a c-Jun N-Terminal Kinase- and Toll-Like Receptor 4-Dependent and Retinol-Independent Mechanism. Mol. Cell. Biol. 2012, 32, 2010–2019. [Google Scholar] [CrossRef]
- Misu, H.; Takamura, T.; Takayama, H.; Hayashi, H.; Matsuzawa-Nagata, N.; Kurita, S.; Ishikura, K.; Ando, H.; Takeshita, Y.; Ota, T.; et al. A Liver-Derived Secretory Protein, Selenoprotein P, Causes Insulin Resistance. Cell Metab. 2010, 12, 483–495. [Google Scholar] [CrossRef]
- Baumeier, C.; Schlüter, L.; Saussenthaler, S.; Laeger, T.; Rödiger, M.; Alaze, S.A.; Fritsche, L.; Häring, H.-U.; Stefan, N.; Fritsche, A.; et al. Elevated Hepatic DPP4 Activity Promotes Insulin Resistance and Non-Alcoholic Fatty Liver Disease. Mol. Metab. 2017, 6, 1254–1263. [Google Scholar] [CrossRef]
- Wu, H.-T.; Ou, H.-Y.; Hung, H.-C.; Su, Y.-C.; Lu, F.-H.; Wu, J.-S.; Yang, Y.-C.; Wu, C.-L.; Chang, C.-J. A Novel Hepatokine, HFREP1, Plays a Crucial Role in the Development of Insulin Resistance and Type 2 Diabetes. Diabetologia 2016, 59, 1732–1742. [Google Scholar] [CrossRef]
- Xia, M.-F.; Bian, H.; Gao, X. NAFLD and Diabetes: Two Sides of the Same Coin? Rationale for Gene-Based Personalized NAFLD Treatment. Front. Pharmacol. 2019, 10. [Google Scholar] [CrossRef]
- Caturano, A.; Acierno, C.; Nevola, R.; Pafundi, P.C.; Galiero, R.; Rinaldi, L.; Salvatore, T.; Adinolfi, L.E.; Sasso, F.C. Non-Alcoholic Fatty Liver Disease: From Pathogenesis to Clinical Impact. Processes 2021, 9, 135. [Google Scholar] [CrossRef]
- Rinaldi, L.; Pafundi, P.C.; Galiero, R.; Caturano, A.; Morone, M.V.; Silvestri, C.; Giordano, M.; Salvatore, T.; Sasso, F.C. Mechanisms of Non-Alcoholic Fatty Liver Disease in the Metabolic Syndrome. A Narrative Review. Antioxidants 2021, 10, 270. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-Alcoholic Fatty Liver Disease and Risk of Incident Cardiovascular Disease: A Meta-Analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Bertolini, L.; Padovani, R.; Poli, F.; Scala, L.; Tessari, R.; Zenari, L.; Falezza, G. Increased Prevalence of Cardiovascular Disease in Type 2 Diabetic Patients with Non-Alcoholic Fatty Liver Disease. Diabet. Med. 2006, 23, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Csermely, A.; Lonardo, A.; Schattenberg, J.M.; Tilg, H.; Byrne, C.D.; Targher, G. Non-Alcoholic Fatty Liver Disease and Risk of Incident Chronic Kidney Disease: An Updated Meta-Analysis. Gut 2022, 71, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Ciardullo, S.; Ballabeni, C.; Trevisan, R.; Perseghin, G. Liver Fibrosis Assessed by Transient Elastography Is Independently Associated with Albuminuria in the General United States Population. Dig. Liver Dis. 2021, 53, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Portillo-Sanchez, P.; Bril, F.; Maximos, M.; Lomonaco, R.; Biernacki, D.; Orsak, B.; Subbarayan, S.; Webb, A.; Hecht, J.; Cusi, K. High Prevalence of Nonalcoholic Fatty Liver Disease in Patients with Type 2 Diabetes Mellitus and Normal Plasma Aminotransferase Levels. J. Clin. Endocrinol. Metab. 2015, 100, 2231–2238. [Google Scholar] [CrossRef]
- Masarone, M.; Rosato, V.; Aglitti, A.; Bucci, T.; Caruso, R.; Salvatore, T.; Sasso, F.C.; Tripodi, M.F.; Persico, M. Liver Biopsy in Type 2 Diabetes Mellitus: Steatohepatitis Represents the Sole Feature of Liver Damage. PLoS ONE 2017, 12, e0178473. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease-Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The Global Epidemiology of NAFLD and NASH in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- de Vries, M.; El-Morabit, F.; van Erpecum, K.J.; Westerink, J.; Bac, S.T.; Kaasjager, H.A.H.; de Valk, H.W. Non-Alcoholic Fatty Liver Disease: Identical Etiologic Factors in Patients with Type 1 and Type 2 Diabetes. Eur. J. Intern. Med. 2022, 100, 77–82. [Google Scholar] [CrossRef]
- Sviklāne, L.; Olmane, E.; Dzērve, Z.; Kupčs, K.; Pīrāgs, V.; Sokolovska, J. Fatty Liver Index and Hepatic Steatosis Index for Prediction of Non-Alcoholic Fatty Liver Disease in Type 1 Diabetes. J. Gastroenterol. Hepatol. 2018, 33, 270–276. [Google Scholar] [CrossRef]
- Chartampilas, E. Imaging of Nonalcoholic Fatty Liver Disease and Its Clinical Utility. Hormones 2018, 17, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Van Natta, M.L.; Clark, J.; Neuschwander-Tetri, B.A.; Diehl, A.; Dasarathy, S.; Loomba, R.; Chalasani, N.; Kowdley, K.; Hameed, B.; et al. Prospective Study of Outcomes in Adults with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2021, 385, 1559–1569. [Google Scholar] [CrossRef]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver Fibrosis, but No Other Histologic Features, Is Associated with Long-Term Outcomes of Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology 2015, 149, 389–397.e10. [Google Scholar] [CrossRef] [PubMed]
- Ciardullo, S.; Perseghin, G. Prevalence of Elevated Liver Stiffness in Patients with Type 1 and Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabetes Res. Clin. Pract. 2022, 190, 109981. [Google Scholar] [CrossRef] [PubMed]
- EASL–EASD–EASO Clinical Practice Guidelines for the Management of Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2016, 64, 1388–1402. [CrossRef]
- Bril, F.; McPhaul, M.J.; Caulfield, M.P.; Clark, V.C.; Soldevilla-Pico, C.; Firpi-Morell, R.J.; Lai, J.; Shiffman, D.; Rowland, C.M.; Cusi, K. Performance of Plasma Biomarkers and Diagnostic Panels for Nonalcoholic Steatohepatitis and Advanced Fibrosis in Patients with Type 2 Diabetes. Diabetes Care 2019, 43, 290–297. [Google Scholar] [CrossRef]
- Shah, A.G.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J. Nash Clinical Research Network Comparison of Noninvasive Markers of Fibrosis in Patients with Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD Fibrosis Score: A Noninvasive System That Identifies Liver Fibrosis in Patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Rosenberg, W.M.C.; Voelker, M.; Thiel, R.; Becka, M.; Burt, A.; Schuppan, D.; Hubscher, S.; Roskams, T.; Pinzani, M.; Arthur, M.J.P.; et al. Serum Markers Detect the Presence of Liver Fibrosis: A Cohort Study. Gastroenterology 2004, 127, 1704–1713. [Google Scholar] [CrossRef]
- Lin, Z.-H.; Xin, Y.-N.; Dong, Q.-J.; Wang, Q.; Jiang, X.-J.; Zhan, S.-H.; Sun, Y.; Xuan, S.-Y. Performance of the Aspartate Aminotransferase-to-Platelet Ratio Index for the Staging of Hepatitis C-Related Fibrosis: An Updated Meta-Analysis. Hepatology 2011, 53, 726–736. [Google Scholar] [CrossRef]
- Davyduke, T.; Tandon, P.; Al-Karaghouli, M.; Abraldes, J.G.; Ma, M.M. Impact of Implementing a “FIB-4 First” Strategy on a Pathway for Patients with NAFLD Referred from Primary Care. Hepatol. Commun. 2019, 3, 1322–1333. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J.; Gaunt, P.; Aithal, G.P.; Barton, D.; Hull, D.; Parker, R.; Hazlehurst, J.M.; Guo, K.; Abouda, G.; Aldersley, M.A.; et al. Liraglutide Safety and Efficacy in Patients with Non-Alcoholic Steatohepatitis (LEAN): A Multicentre, Double-Blind, Randomised, Placebo-Controlled Phase 2 Study. Lancet 2016, 387, 679–690. [Google Scholar] [CrossRef] [Green Version]
- Sattar, N.; Fitchett, D.; Hantel, S.; George, J.T.; Zinman, B. Empagliflozin Is Associated with Improvements in Liver Enzymes Potentially Consistent with Reductions in Liver Fat: Results from Randomised Trials Including the EMPA-REG OUTCOME® Trial. Diabetologia 2018, 61, 2155–2163. [Google Scholar] [CrossRef]
- Singal, A.G.; El-Serag, H.B. Rational HCC Screening Approaches for Patients with NAFLD. J. Hepatol. 2022, 76, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Adinolfi, L.E.; Petta, S.; Fracanzani, A.L.; Nevola, R.; Coppola, C.; Narciso, V.; Rinaldi, L.; Calvaruso, V.; Pafundi, P.C.; Lombardi, R.; et al. Reduced Incidence of Type 2 Diabetes in Patients with Chronic Hepatitis C Virus Infection Cleared by Direct-Acting Antiviral Therapy: A Prospective Study. Diabetes Obes. Metab. 2020, 22, 2408–2416. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J. International Consensus Panel MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Konyn, P.; Sandhu, K.K.; Dennis, B.B.; Cheung, A.C.; Ahmed, A. Metabolic Dysfunction-Associated Fatty Liver Disease Is Associated with Increased All-Cause Mortality in the United States. J. Hepatol. 2021, 75, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Lu, L.; Chen, Y.; Xu, L.; Xu, C. A Simpler Definition of MAFLD Better Predicts Long-Term All-Cause Mortality in American Adults. J. Hepatol. 2022, 77, 877–879. [Google Scholar] [CrossRef]
- Méndez-Sánchez, N.; Chavez-Tapia, N.C.; Motola-Kuba, D.; Sanchez-Lara, K.; Ponciano-Rodríguez, G.; Baptista, H.; Ramos, M.H.; Uribe, M. Metabolic Syndrome as a Risk Factor for Gallstone Disease. World J. Gastroenterol. 2005, 11, 1653–1657. [Google Scholar] [CrossRef]
- Méndez-Sánchez, N.; Bermejo-Martínez, L.B.; Viñals, Y.; Chavez-Tapia, N.C.; Graff, I.V.; Ponciano-Rodríguez, G.; Ramos, M.H.; Uribe, M. Serum Leptin Levels and Insulin Resistance Are Associated with Gallstone Disease in Overweight Subjects. World J. Gastroenterol. 2005, 11, 6182–6187. [Google Scholar] [CrossRef]
- Yuan, S.; Gill, D.; Giovannucci, E.L.; Larsson, S.C. Obesity, Type 2 Diabetes, Lifestyle Factors, and Risk of Gallstone Disease: A Mendelian Randomization Investigation. Clin. Gastroenterol. Hepatol. 2022, 20, e529–e537. [Google Scholar] [CrossRef] [PubMed]
- Pagliarulo, M.; Fornari, F.; Fraquelli, M.; Zoli, M.; Giangregorio, F.; Grigolon, A.; Peracchi, M.; Conte, D. Gallstone Disease and Related Risk Factors in a Large Cohort of Diabetic Patients. Dig. Liver Dis. 2004, 36, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Vatten, L.J. Diabetes Mellitus and the Risk of Gallbladder Disease: A Systematic Review and Meta-Analysis of Prospective Studies. J. Diabetes Complicat. 2016, 30, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Li, N. The Association of Gallstone Disease and Diabetes Mellitus. A Meta-Analysis. Saudi Med. J. 2014, 35, 1005–1012. [Google Scholar]
- Gu, J.; Yan, S.; Wang, B.; Shen, F.; Cao, H.; Fan, J.; Wang, Y. Type 2 Diabetes Mellitus and Risk of Gallbladder Cancer: A Systematic Review and Meta-Analysis of Observational Studies. Diabetes Metab. Res. Rev. 2016, 32, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Mahamat-Saleh, Y.; Norat, T.; Riboli, E. Diabetes Mellitus and the Risk of Pancreatitis: A Systematic Review and Meta-Analysis of Cohort Studies. Pancreatology 2020, 20, 602–607. [Google Scholar] [CrossRef]
- Azami, M.; Baradaran, H.R.; Dehghanbanadaki, H.; Kohnepoushi, P.; Saed, L.; Moradkhani, A.; Moradpour, F.; Moradi, Y. Association of Helicobacter Pylori Infection with the Risk of Metabolic Syndrome and Insulin Resistance: An Updated Systematic Review and Meta-Analysis. Diabetol. Metab. Syndr. 2021, 13, 145. [Google Scholar] [CrossRef]
- Zhou, X.; Zhang, C.; Wu, J.; Zhang, G. Association between Helicobacter Pylori Infection and Diabetes Mellitus: A Meta-Analysis of Observational Studies. Diabetes Res. Clin. Pract. 2013, 99, 200–208. [Google Scholar] [CrossRef]
- Mansori, K.; Moradi, Y.; Naderpour, S.; Rashti, R.; Moghaddam, A.B.; Saed, L.; Mohammadi, H. Helicobacter Pylori Infection as a Risk Factor for Diabetes: A Meta-Analysis of Case-Control Studies. BMC Gastroenterol. 2020, 20, 77. [Google Scholar] [CrossRef]
- Mills, K.T.; Bellows, C.F.; Hoffman, A.E.; Kelly, T.N.; Gagliardi, G. Diabetes and Colorectal Cancer Prognosis: A Meta-Analysis. Dis. Colon. Rectum 2013, 56, 1304–1319. [Google Scholar] [CrossRef]
- Ali Khan, U.; Fallah, M.; Tian, Y.; Sundquist, K.; Sundquist, J.; Brenner, H.; Kharazmi, E. Personal History of Diabetes as Important as Family History of Colorectal Cancer for Risk of Colorectal Cancer: A Nationwide Cohort Study. Off. J. Am. Coll. Gastroenterol. ACG 2020, 115, 1103–1109. [Google Scholar] [CrossRef]
- Troelsen, F.S.; Sørensen, H.T.; Pedersen, L.; Erichsen, R. Risk of a Post-Colonoscopy Colorectal Cancer in Patients with Type 2 Diabetes: A Danish Population-Based Cohort Study. BMJ Open Gastroenterol. 2021, 8, e000786. [Google Scholar] [CrossRef]
- Phelps, G.; Chapman, I.; Hall, P.; Braund, W.; Mackinnon, M. Prevalence of Genetic Haemochromatosis among Diabetic Patients. Lancet 1989, 2, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Real, J.M.; Ricart-Engel, W.; Arroyo, E.; Balançá, R.; Casamitjana-Abella, R.; Cabrero, D.; Fernández-Castañer, M.; Soler, J. Serum Ferritin as a Component of the Insulin Resistance Syndrome. Diabetes Care 1998, 21, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Li, Q.; Yang, Y.; Ma, L. Iron Metabolism and Type 2 Diabetes Mellitus: A Meta-Analysis and Systematic Review. J. Diabetes Investig. 2020, 11, 946–955. [Google Scholar] [CrossRef]
- Bao, W.; Rong, Y.; Rong, S.; Liu, L. Dietary Iron Intake, Body Iron Stores, and the Risk of Type 2 Diabetes: A Systematic Review and Meta-Analysis. BMC Med. 2012, 10, 119. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Apekey, T.A.; Walley, J.; Kain, K. Ferritin Levels and Risk of Type 2 Diabetes Mellitus: An Updated Systematic Review and Meta-Analysis of Prospective Evidence. Diabetes Metab. Res. Rev. 2013, 29, 308–318. [Google Scholar] [CrossRef]
- Zhao, Z.; Li, S.; Liu, G.; Yan, F.; Ma, X.; Huang, Z.; Tian, H. Body Iron Stores and Heme-Iron Intake in Relation to Risk of Type 2 Diabetes: A Systematic Review and Meta-Analysis. PLoS ONE 2012, 7, e41641. [Google Scholar] [CrossRef]
- Cohn, A.; Sofia, M.A.; Kupfer, S.S. Type 1 Diabetes and Celiac Disease: Clinical Overlap and New Insights into Disease Pathogenesis. Curr. Diab. Rep. 2014, 14, 517. [Google Scholar] [CrossRef]
- Kylökäs, A.; Kaukinen, K.; Huhtala, H.; Collin, P.; Mäki, M.; Kurppa, K. Type 1 and Type 2 Diabetes in Celiac Disease: Prevalence and Effect on Clinical and Histological Presentation. BMC Gastroenterol. 2016, 16, 76. [Google Scholar] [CrossRef]
- Kabbani, T.A.; Kelly, C.P.; Betensky, R.A.; Hansen, J.; Pallav, K.; Villafuerte-Gálvez, J.A.; Vanga, R.; Mukherjee, R.; Novero, A.; Dennis, M.; et al. Patients with Celiac Disease Have a Lower Prevalence of Non-Insulin-Dependent Diabetes Mellitus and Metabolic Syndrome. Gastroenterology 2013, 144, 912–917.e1. [Google Scholar] [CrossRef] [PubMed]
- Kizilgul, M.; Ozcelik, O.; Beysel, S.; Akinci, H.; Kan, S.; Ucan, B.; Apaydin, M.; Cakal, E. Screening for Celiac Disease in Poorly Controlled Type 2 Diabetes Mellitus: Worth It or Not? BMC Endocr. Disord. 2017, 17, 62. [Google Scholar] [CrossRef]
- Rostom, A.; Murray, J.A.; Kagnoff, M.F. American Gastroenterological Association (AGA) Institute Technical Review on the Diagnosis and Management of Celiac Disease. Gastroenterology 2006, 131, 1981–2002. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Tests | Comments |
|---|---|
| Scintigraphic gastric emptying | The gold standard, most cost-effective, simple, and available technique able to assess liquid and solid emptying; minimal radiation exposure [9] |
| Wireless motility capsule | Measures simultaneously phasic pressure amplitudes, temperature, and Ph as it passes through the GI tract [18] |
| 13 C breath testing | Non-invasive, non-radiation exposure. Acetate breath testing, octanoic acid breath test, or spirulin have been used to assess gastric emptying [19]. |
| Electrogastrography | Noninvasive method that measures gastric myoelectrical activity [20]. |
| Antroduodenal manometry | Invasive procedure requiring expertise to perform and interpret. Assess fasting and postprandial phases [21]. |
| Treatment | Mechanism | Comments |
|---|---|---|
| Metoclopramide (10 mg four times daily) | Improves gastric emptying by enhancing gastric antral contractions and decreasing postprandial fundus relaxation | First line therapy Symptoms improved in 25 to 62% of patients [11] Risk of tardive dyskinesia |
| Domperidone (10 mg three times daily) | Similar with Metoclopramide | Used when symptoms fail to respond to Metoclopramide Risk of cardiac arrhythmias [22] |
| Erythromycin (250 mg three times daily) | Motilin receptor agonist Induces high amplitude gastric propulsive contractions that increase gastric emptying | Used when symptoms fail to respond to Metoclopramide and Domperidone Duration: no more than 4 weeks Risk of tachyphylaxis [23] |
| Tricyclic agents | Reduce perception of pain at different levels of the brain–gut axis | Medication for visceral pain [23] |
| Gastric per-oral endoscopic myotomy (G-POEM) | Induces dumping syndrome | Pooled analysis including open-label and retrospective studies suggest a reduction in post-procedure GCSI scores and improved gastric emptying, with 6.8% overall adverse events Indication: only in refractory gastroparesis in tertiary centers [23] |
| Gastric electrical stimulation | Electric stimulation with high-energy, long-duration pulses | Reserved for compassionate treatment in patients with refractory symptoms (e.g., nausea and vomiting, without pain) [23] |
| Surgery | Pyloroplasty, gastrectomy | Most studies are non-randomized, unblended, or case series [11,24] |
| Biomarker | Formula | Cut-Offs to Rule Out/in Advanced Fibrosis |
|---|---|---|
| FIB-4 index [58] | Age (years) × AST (U/L)/ [PLT (109/ L) × ALT1/2 (U/L) | <1.3/>2.67 |
| NAFLD fibrosis score [59] | −1.675 + 0.037 × age (years) + 0.094 × BMI (kg/m2) + 1.13 × IFG/diabetes (yes = 1, no = 0) + 0.99 × AST/ALT ratio − 0.013 × platelet count (× 109/L) − 0.66 × albumin (g/dL). | <−1.455/>0.676 |
| Enhanced liver fibrosis test (ELF) [60] | Age, hyaluronic acid, aminoterminal propeptide of type III collagen, and tissue inhibitor of matrix metalloproteinase 1 | ≥9.8 |
| Alanine aspartate transferase (AST) to platelet ratio index (APRI) [61] | [(AST/ upper limit of the normal AST range)/platelet count (109/L)] × 100 | <0.5/>1.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mare, R.; Sporea, I. Gastrointestinal and Liver Complications in Patients with Diabetes Mellitus—A Review of the Literature. J. Clin. Med. 2022, 11, 5223. https://doi.org/10.3390/jcm11175223
Mare R, Sporea I. Gastrointestinal and Liver Complications in Patients with Diabetes Mellitus—A Review of the Literature. Journal of Clinical Medicine. 2022; 11(17):5223. https://doi.org/10.3390/jcm11175223
Chicago/Turabian StyleMare, Ruxandra, and Ioan Sporea. 2022. "Gastrointestinal and Liver Complications in Patients with Diabetes Mellitus—A Review of the Literature" Journal of Clinical Medicine 11, no. 17: 5223. https://doi.org/10.3390/jcm11175223