
Inner Ear Diagnostics and Drug Delivery via Microneedles

 , , and
, , and
Abstract
:1. Introduction
2. Properties of the Round Window Membrane
3. Microneedle Design and Testing
3.1. Design for RWM Perforation
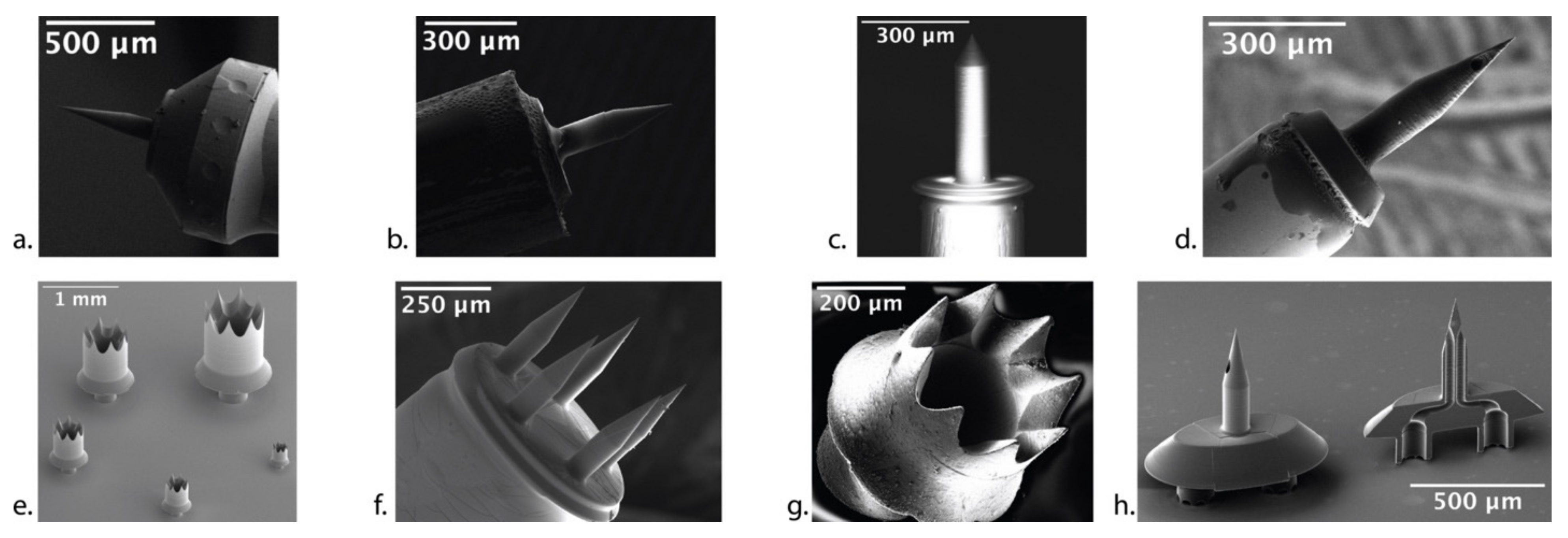
3.2. Microneedle Fabrication
3.3. Anatomical and Functional Consequences of Perforation
3.4. Design Freedom in Microneedle Synthesis
4. Clinical Applications of Microneedles
4.1. Hollow Microneedles for Aspiration
4.2. Microneedles for Diffusion and Injection
4.3. Office-Based Diagnostic and Therapeutic Intervention
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lucas, J.W.; Zelaya, C.E. Hearing difficulty, vision trouble, and balance problems among male veterans and nonveterans. Natl. Health Stat. Rep. 2020, 142, 1–8. [Google Scholar]
- Ahmed, H.; Shubina-Oleinik, O.; Holt, J.R. Emerging Gene Therapies for Genetic Hearing Loss. JARO 2017, 18, 649–670. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, M.E.; Allen, K.; Kopke, R.D.; Weisskopf, P.; Gottshall, K.; Wester, D. Transtympanic versus sustained-release administration of gentamicin: Kinetics, morphology, and function. Laryngoscope 2001, 111, 1343–1357. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Xu, Y.; Cao, W.; Xie, S.; Wen, L.; Chen, G. Understanding the translocation mechanism of PLGA nanoparticles across round window membrane into the inner ear: A guideline for inner ear drug delivery based on nanomedicine. Int. J. Nanomed. 2018, 13, 479–492. [Google Scholar] [CrossRef] [PubMed]
- Paulson, D.P.; Abuzeid, W.; Jiang, H.; Oe, T.; O’Malley, B.W.; Li, D. A novel controlled local drug delivery system for inner ear disease. Laryngoscope 2008, 118, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Ren, J.; Yin, T.; Liu, W. Intratympanic dexamethasone perfusion versus injection for treatment of refractory sudden sensorineural hearing loss. Eur. Arch. Otorhinolaryngol. 2012, 270, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Lambert, P.R.; Carey, J.; Mikulec, A.A.; LeBel, C.; on behalf of the Otonomy Ménière’s Study Group. Intratympanic Sustained-Exposure Dexamethasone Thermosensitive Gel for Symptoms of Ménière’s Disease: Randomized Phase 2b Safety and Efficacy Trial. Otol. Neurotol. 2016, 37, 1669–1676. [Google Scholar] [CrossRef]
- Staecker, H.; Jokovic, G.; Karpishchenko, S.; Kienle-Gogolok, A.; Krzyzaniak, A.; Lin, C.-D.; Navratil, P.; Tzvetkov, V.; Wright, N.; Meyer, T. Efficacy and Safety of AM-111 in the Treatment of Acute Unilateral Sudden Deafness-A Double-blind, Randomized, Placebo-controlled Phase 3 Study. Otol. Neurotol. 2019, 40, 584–594. [Google Scholar] [CrossRef]
- Hahn, H.; Salt, A.N.; Biegner, T.; Kammerer, B.; Delabar, U.; Hartsock, J.; Plontke, K.K. Dexamethasone levels and base to apex concentration gradients in scala tympani perilymph following intracochlear delivery in the guinea pig. Otol. Neurotol. 2012, 33, 660–665. [Google Scholar] [CrossRef]
- Liu, H.; Hao, J.; Li, K.S. Current strategies for drug delivery to the inner ear. Acta Pharm. Sin. B 2013, 3, 86–96. [Google Scholar] [CrossRef]
- Derby, M.L.; Sena-Esteves, M.; Breakefield, X.O.; Corey, D.P. Gene transfer into the mammalian inner ear using HSV-1 and vaccinia virus vectors. Hear. Res. 1999, 134, 1–8. [Google Scholar] [CrossRef]
- Komeda, M.; Roessler, B.J.; Raphael, Y. The influence of interleukin-1 receptor antagonist transgene on spiral ganglion neurons. Hear. Res. 1999, 131, 1–8. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, W.; Johnston, A.H.; Newman, T.A.; Pyykk, I.; Zou, J. Comparison of the distribution pattern of PEG-b-PCL polymersomes delivered into the rat inner ear via different methods. Acta Otolaryngol. 2011, 131, 1249–1256. [Google Scholar] [CrossRef]
- Wareing, M.; Mhatre, A.N.; Pettis, R.; Han, J.J.; Haut, T.; Pfister, M.H.; Hong, K.; Zheng, W.W.; Lalwani, A.K. Cationic liposome mediated transgene expression in the guinea pig cochlea. Hear. Res. 1999, 128, 61–69. [Google Scholar] [CrossRef]
- Han, J.J.; Mhatre, A.N.; Wareing, M.; Pettis, R.; Gao, W.Q.; Zufferey, R.N.; Trono, D.; Lalwani, A.K. Transgene expression in the guinea pig cochlea mediated by a lentivirus-derived gene transfer vector. Hum. Gene Ther. 1999, 10, 1867–1873. [Google Scholar] [CrossRef]
- Carvalho, G.J.; Lalwani, A.K. The effect of cochleostomy and intracochlear infusion on auditory brain stem response threshold in the guinea pig. Am. J. Otol. 1999, 20, 87–90. [Google Scholar]
- Jero, J.; Tseng, C.J.; Mhatre, A.N.; Lalwani, A.K. A surgical approach appropriate for targeted cochlear gene therapy in the mouse. Hear. Res. 2001, 151, 106–114. [Google Scholar] [CrossRef]
- Horváth, M.; Ribári, O.; Répássy, G.; Tóth, I.E.; Boldogkõi, Z.; Palkovits, M. Intracochlear injection of pseudorabies virus labels descending auditory and monoaminerg projections to olivocochlear cells in guinea pig. Eur. J. Neurosci. 2003, 18, 1439–1447. [Google Scholar] [CrossRef]
- Plontke, S.K.; Hartsock, J.J.; Gill, R.M.; Salt, A.N. Intracochlear Drug Injections through the Round Window Membrane: Measures to Improve Drug Retention. Audiol. Neurotol. 2016, 21, 72–79. [Google Scholar] [CrossRef]
- Plontke, S.K.; Götze, G.; Rahne, T.; Liebau, A. Intracochlear drug delivery in combination with cochlear implants. HNO 2017, 65, 19–28. [Google Scholar] [CrossRef]
- Prenzler, N.K.; Salcher, R.; Lenarz, T.; Gaertner, L.; Warnecke, A. Dose-Dependent Transient Decrease of Impedances by Deep Intracochlear Injection of Triamcinolone with a Cochlear Catheter Prior to Cochlear Implantation–1 Year Data. Front. Neurol. 2020, 11, 258. [Google Scholar] [CrossRef]
- Szeto, B.; Chiang, H.; Valentini, C.; Yu, M.; Kysar, J.W.; Lalwani, A.K. Inner ear delivery: Challenges and opportunities. Laryngoscope Investig. Otolaryngol. 2020, 5, 122–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valentini, C.; Szeto, B.; Kysar, J.W.; Lalwani, A.K. Inner ear gene delivery: Vectors and routes. Hear. Balance Commun. 2020, 18, 278–285. [Google Scholar] [CrossRef]
- Cheng, T.; Gan, R.Z. Experimental measurement and modeling analysis on mechanical properties of tensor tympani tendon. Med. Eng. Phys. 2008, 30, 358–366. [Google Scholar] [CrossRef]
- Watanabe, H.; Kysar, J.W.; Lalwani, A.K. Round Window Membrane as a Portal for Inner Ear Therapy. Recent Adv. Otolaryngol. Head Neck Surg. 2017, 6, 39. [Google Scholar]
- Goycoolea, M.V. Clinical aspects of round window membrane permeability under normal and pathological conditions. Acta Oto-Laryngol. 2001, 121, 437–447. [Google Scholar] [CrossRef]
- Nordang, L.; Anniko, M. Hearing loss in relation to round window membrane morphology in experimental otitis media. ORL 2001, 63, 333–340. [Google Scholar] [CrossRef]
- Sahni, R.S.; Paparella, M.M.; Schachern, P.A.; Goycoolea, M.V.; Le, C.T. Thickness of the human round window membrane in different forms of otitis media. Arch Otolaryngol. Head Neck Surg. 1987, 113, 630–634. [Google Scholar] [CrossRef]
- Arriaga, M.; Arteaga, D.N.; Fafalis, D.; Yu, M.; Wang, X.; Kasza, K.E.; Lalwani, A.K.; Kysar, J.W. Membrane curvature and connective fiber alignment in guinea pig round window membrane. Acta Biomater. 2021, 136, 343–362. [Google Scholar] [CrossRef]
- Henry, S.; McAllister, D.V.; Allen, M.G.; Prausnitz, M.R. Microfabricated microneedles: A novel approach to transdermal drug delivery. J. Pharm. Sci. 1999, 88, 948. [Google Scholar] [CrossRef]
- Donnelly, R.F.; Raj Singh, T.R.; Woolfson, A.D. Microneedle-based drug delivery systems: Microfabrication, drug delivery, and safety. Drug Deliv. 2010, 17, 187–207. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, R.F.; Singh, T.R.R.; Tunney, M.M.; Morrow, D.I.J.; McCarron, P.A.; O’Mahony, C.; Woolfson, A.D. Microneedle arrays allow lower microbial penetration than hypodermic needles in vitro. Pharm. Res. 2009, 26, 2513–2522. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-C.; Park, J.-H.; Prausnitz, M.R. Microneedles for drug and vaccine delivery. Adv. Drug Deliv. Rev. 2012, 64, 1547–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Prausnitz, M. Drug delivery using microneedle patches: Not just for skin. Expert Opin. Drug Deliv. 2018, 15, 541–543. [Google Scholar] [CrossRef]
- Aksit, A.; Arteaga, D.; Arriaga, M.; Wang, X.; Watanabe, H.; Kasza, K.; Lalwani, A.; Kysar, J. In-vitro perforation of the round window membrane via direct 3-D printed microneedles. Biomed. Microdevices 2018, 20, 1–12. [Google Scholar] [CrossRef]
- Yu, M.; Arteaga, D.N.; Aksit, A.; Chiang, H.; Olson, E.S.; Kysar, J.W.; Lalwani, A.K. Anatomical and Functional Consequences of Microneedle Perforation of Round Window Membrane. Otol. Neurotol. 2020, 41, e280–e287. [Google Scholar] [CrossRef]
- Chiang, H.; Yu, M.; Aksit, A.; Wang, W.; Stern-Shavit, S.; Kysar, J.W.; Lalwani, A.K. 3D-printed Microneedles Create Precise Perforations in Human Round Window Membrane in situ. Otol. Neurotol. 2020, 41, 277–284. [Google Scholar] [CrossRef]
- Aksit, A.; Rastogi, S.; Nadal, M.; Parker, A.; Lalwani, A.; West, A.; Kysar, J.W. Drug delivery device for the inner ear: Ultra-sharp fully metallic microneedles. Drug Deliv. Transl. Res. 2020, 11, 214–226. [Google Scholar] [CrossRef]
- Szeto, B.; Aksit, A.; Valentini, C.; Yu, M.; Werth, E.G.; Goeta, S.; Tang, C.; Brown, L.M.; Olson, E.S.; Kysar, J.W.; et al. Novel 3D-printed hollow microneedles facilitate safe, reliable, and informative sampling of perilymph from guinea pigs. Hear. Res. 2021, 400, 108141. [Google Scholar] [CrossRef]
- Watanabe, H.; Cardoso, L.; Lalwani, A.K.; Kysar, J.W. A dual wedge microneedle for sampling of perilymph solution via round window membrane. Biomed. Microdevices 2016, 18, 24. [Google Scholar] [CrossRef]
- Park, J.-H.; Allen, M.G.; Prausnitz, M.R. Polymer Microneedles for Controlled-Release Drug Delivery. Pharm. Res. 2006, 23, 1008–1019. [Google Scholar] [CrossRef]
- Larrañeta, E.; McCrudden, M.T.C.; Courtenay, A.J.; Donnelly, R.F. Microneedles: A New Frontier in Nanomedicine Delivery. Pharm. Res. 2016, 33, 1055–1073. [Google Scholar] [CrossRef]
- Serbin, J.; Egbert, A.; Ostendorf, A.; Chichkov, B.N.; Houbertz, R.; Domann, G.; Schulz, J.; Cronauer, C.; Fröhlich, L.; Popall, M. Femtosecond laser-induced two-photon polymerization of inorganic–organic hybrid materials for applications in photonics. Opt. Lett. 2003, 28, 301–303. [Google Scholar] [CrossRef]
- Kelso, C.M.; Watanabe, H.; Wazen, J.M.; Bucher, T.; Qian, Z.J.; Olson, E.S.; Kysar, J.W.; Lalwani, A.K. Microperforations Significantly Enhance Diffusion Across Round Window Membrane. Otol. Neurotol. 2015, 36, 694–700. [Google Scholar] [CrossRef]
- Creber, N.J.; Eastwood, H.T.; Hampson, A.J.; Tan, J.; O’Leary, S.J. A comparison of cochlear distribution and glucocorticoid receptor activation in local and systemic dexamethasone drug delivery regimes. Hear. Res. 2018, 368, 75–85. [Google Scholar] [CrossRef]
- Wang, Y.; Han, L.; Diao, T.; Jing, Y.; Wang, L.; Zheng, H.; Ma, X.; Qi, J.; Yu, L. A comparison of systemic and local dexamethasone administration: From perilymph/cochlear concentration to cochlear distribution. Hear. Res. 2018, 370, 1–10. [Google Scholar] [CrossRef]
- Trune, D.R.; Shives, K.D.; Hausman, F.; Kempton, J.B.; MacArthur, C.J.; Choi, D. Intratympanically delivered steroids impact thousands more inner ear genes than systemic delivery. Ann. Otol. Rhinol. Laryngol. 2019, 128 (Suppl. S6), 134S–138S. [Google Scholar] [CrossRef]
- Szeto, B.; Valentini, C.; Aksit, A.; Werth, E.G.; Goeta, S.; Brown, L.M.; Olson, E.S.; Kysar, J.W.; Lalwani, A.K. Impact of Systemic versus Intratympanic Dexamethasone Administration on the Perilymph Proteome. J. Proteom. Res. 2021, 20, 4001–4009. [Google Scholar] [CrossRef]
- Salt, A.N.; Sirjani, D.B.; Hartsock, J.J.; Gill, R.M.; Plontke, S.K. Marker retention in the cochlea following injections through the round window membrane. Hear. Res. 2007, 232, 78–86. [Google Scholar] [CrossRef]
- Poiseuille, J. Ecoulement des Liquides: Societe Philomatique de Paris. Extraits des Proces-Verbaux des Seances Pendant I’Annee 1838, 3, 77–81. [Google Scholar]
- Santimetaneedol, A.; Wang, Z.; Arteaga, D.N.; Aksit, A.; Prevoteau, C.; Yu, M.; Chiang, H.; Fafalis, D.; Lalwani, A.K.; Kysar, J.W. Small molecule delivery across a perforated artificial membrane by thermoreversible hydrogel poloxamer 407. Colloids Surf. B Biointerfaces 2019, 182, 110300. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Ages 18+ | Ages 18–44 | Ages 45–64 | Ages 65–74 | Age 75+ | |
|---|---|---|---|---|---|
| Severe hearing loss | 2.4% (2.0–2.8) | 0.4% (0.2–0.6) | 1.9% (1.5–2.5) | 6.0% (4.2–8.3) | 13.4% (10.2–17.2) |
| Mild–moderate hearing loss | 13.6% (12.7–14.4) | 5.3% (4.6–6.1) | 16.7% (15.3–18.2) | 31.2% (28.0–34.6) | 36.4% (31.2–41.9) |
| Balance issues | 18.7% (17.7–19.7) | 14.2% (12.9–15.6) | 21.1% (19.5–22.7) | 27.1% (24.0–30.4) | 30.1% (25.3–35.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leong, S.; Aksit, A.; Feng, S.J.; Kysar, J.W.; Lalwani, A.K. Inner Ear Diagnostics and Drug Delivery via Microneedles. J. Clin. Med. 2022, 11, 5474. https://doi.org/10.3390/jcm11185474
Leong S, Aksit A, Feng SJ, Kysar JW, Lalwani AK. Inner Ear Diagnostics and Drug Delivery via Microneedles. Journal of Clinical Medicine. 2022; 11(18):5474. https://doi.org/10.3390/jcm11185474
Chicago/Turabian StyleLeong, Stephen, Aykut Aksit, Sharon J. Feng, Jeffrey W. Kysar, and Anil K. Lalwani. 2022. "Inner Ear Diagnostics and Drug Delivery via Microneedles" Journal of Clinical Medicine 11, no. 18: 5474. https://doi.org/10.3390/jcm11185474