
Head and Neck Cutaneous Soft-Tissue Sarcoma Demonstrate Sex and Racial/Ethnic Disparities in Incidence and Socioeconomic Disparities in Survival
 , ,
, ,
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Demographics and Clinical Characteristics
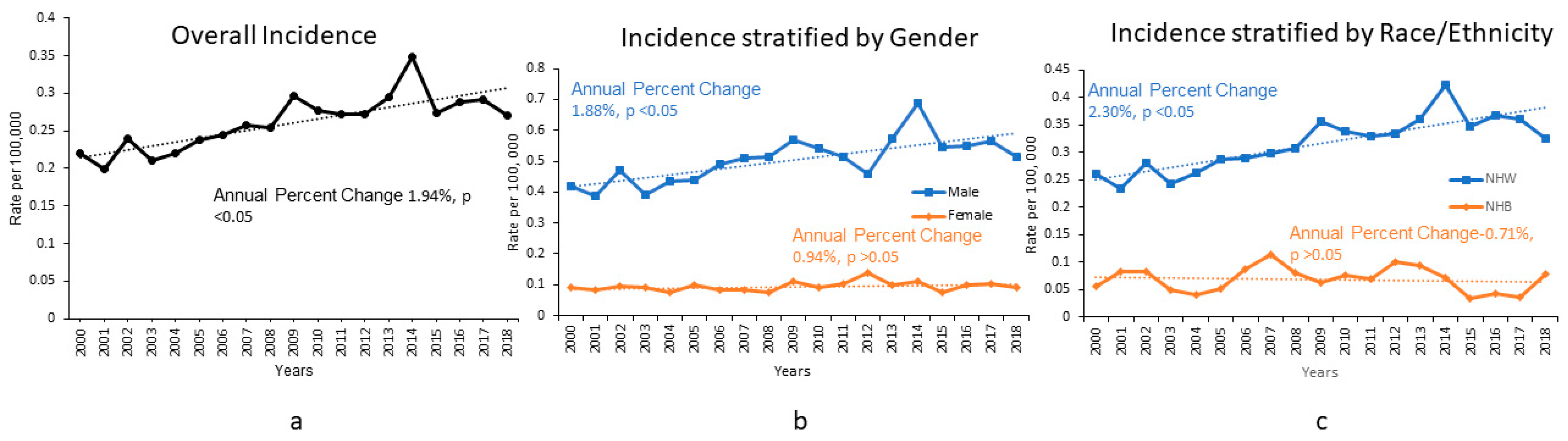
3.2. Incidence: Sex and Racial/Ethnic Disparities
3.3. Survival and Univariable Analysis
3.4. Multivariable Analysis: Independent Predictors of Overall Survival
4. Discussion
4.1. Previous Literature
4.2. Sex and Racial/Ethnic Disparities in Incidence
4.3. Prognostic Factors
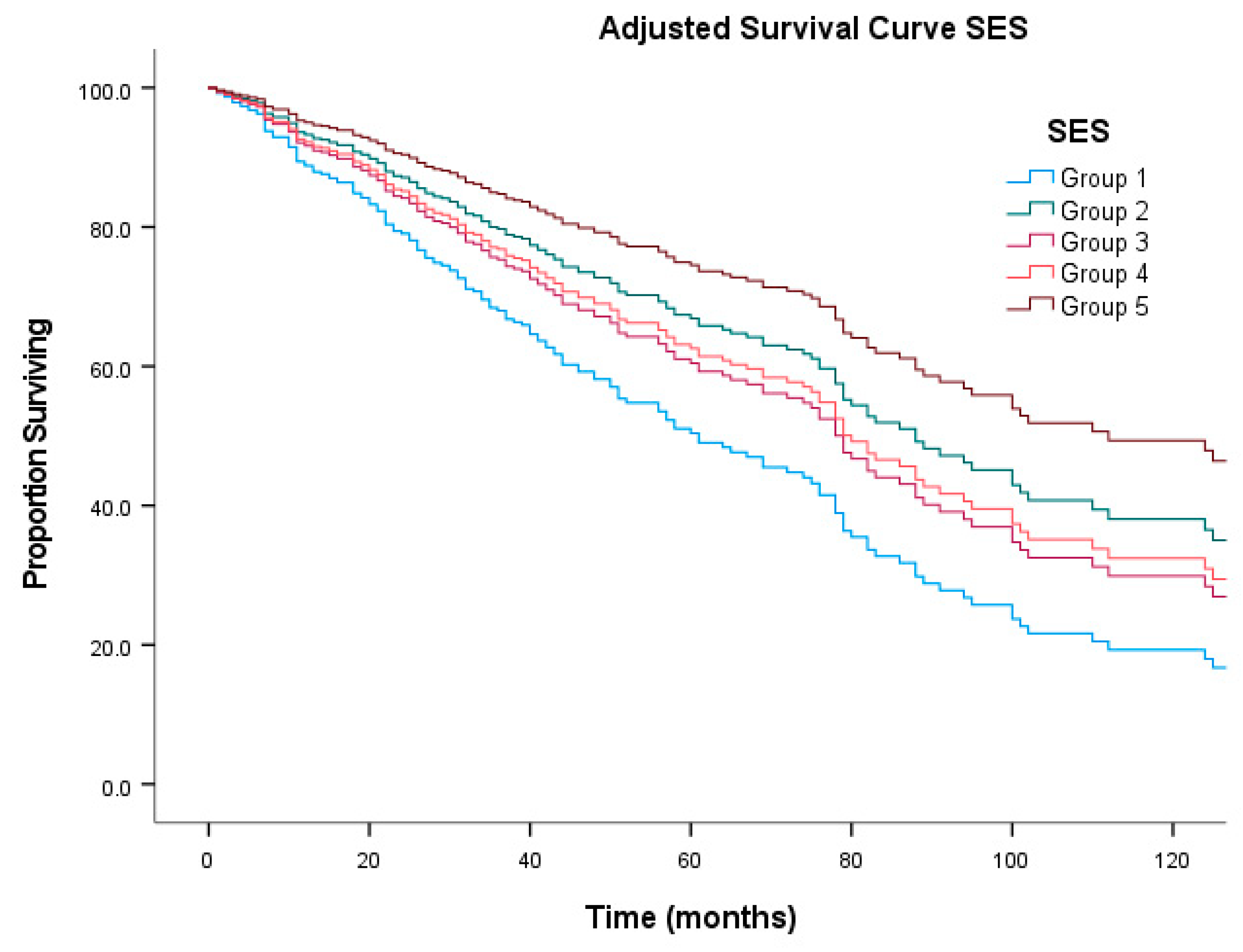
4.4. SES Disparities in Outcomes
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tillman, B.N.; Liu, J.C. Cutaneous Sarcomas. Otolaryngol. Clin. N. Am. 2021, 54, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, M.D.; Nambudiri, V.E. Cutaneous Sarcomas. Hematol. Oncol. Clin. N. Am. 2019, 33, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Farhood, A.I.; Hajdu, S.I.; Shiu, M.H.; Strong, E.W. Soft tissue sarcomas of the head and neck in adults. Am. J. Surg. 1990, 160, 365–369. [Google Scholar] [CrossRef]
- Le Vay, J.; O’Sullivan, B.; Catton, C.; Cummings, B.; Fornasier, V.; Gullane, P.; Simm, J. An assessment of prognostic factors in soft-tissue sarcoma of the head and neck. Arch. Otolaryngol. Head Neck Surg. 1994, 120, 981–986. [Google Scholar] [CrossRef] [PubMed]
- LeVay, J.; O’Sullivan, B.; Catton, C.; Bell, R.; Fornasier, V.; Cummings, B.; Hao, Y.; Warr, D.; Quirt, I. Outcome and prognostic factors in soft tissue sarcoma in the adult. Int. J. Radiat. Oncol. Biol. Phys. 1993, 27, 1091–1099. [Google Scholar] [CrossRef]
- Rouhani, P.; Fletcher, C.D.; Devesa, S.S.; Toro, J.R. Cutaneous soft tissue sarcoma incidence patterns in the U.S.: An analysis of 12,114 cases. Cancer 2008, 113, 616–627. [Google Scholar] [CrossRef] [PubMed]
- Peng, K.A.; Grogan, T.; Wang, M.B. Head and neck sarcomas: Analysis of the SEER database. Otolaryngol. Head Neck Surg. 2014, 151, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Eppsteiner, R.W.; DeYoung, B.R.; Milhem, M.M.; Pagedar, N.A. Leiomyosarcoma of the head and neck: A population-based analysis. Arch. Otolaryngol. Head Neck Surg. 2011, 137, 921–924. [Google Scholar] [CrossRef] [PubMed]
- Woods, R.H.; Potter, J.A.; Reid, J.L.; Louise, J.; Bessen, T.; Farshid, G.; Neuhaus, S.J. Patterns of head and neck sarcoma in Australia. ANZ J. Surg. 2018, 88, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Nimhd. Nimhd Minority Health and Health Disparities Research. Available online: https://www.nimhd.nih.gov/about/overview/research-framework/ (accessed on 11 October 2021).
- NCI. Surveillance, Epidemiology and End Result (SEER). 2021. Available online: https://seer.cancer.gov (accessed on 11 October 2021).
- Morris, A.M.; Rhoads, K.F.; Stain, S.C.; Birkmeyer, J.D. Understanding racial disparities in cancer treatment and outcomes. J. Am. Coll. Surg. 2010, 211, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Shavers, V.L.; Brown, M.L. Racial and ethnic disparities in the receipt of cancer treatment. J. Natl. Cancer Inst. 2002, 94, 334–357. [Google Scholar] [CrossRef] [PubMed]
- Meara, J.G.; Leather, A.J.; Hagander, L.; Alkire, B.C.; Alonso, N.; Ameh, E.A.; Bickler, S.W.; Conteh, L.; Dare, A.J.; Davies, J.; et al. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Lancet 2015, 386, 569–624. [Google Scholar] [CrossRef]
- Murphy, M.M.; Tseng, J.F.; Shah, S.A. Disparities in cancer care: An operative perspective. Surgery 2010, 147, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Tatalovich, Z.; Gibson, J.T.; Cronin, K.A. Using a composite index of socioeconomic status to investigate health disparities while protecting the confidentiality of cancer registry data. Cancer Causes Control 2014, 25, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Diessner, B.J.; Weigel, B.J.; Murugan, P.; Zhang, L.; Poynter, J.N.; Spector, L.G. Associations of Socioeconomic Status, Public vs. Private Insurance, and Race/Ethnicity With Metastatic Sarcoma at Diagnosis. JAMA Netw. Open 2020, 3, e2011087. [Google Scholar] [CrossRef] [PubMed]
- Yost, K.; Perkins, C.; Cohen, R.; Morris, C.; Wright, W. Socioeconomic status and breast cancer incidence in California for different race/ethnic groups. Cancer Causes Control 2001, 12, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Bleyer, A. Young adult oncology: The patients and their survival challenges. CA Cancer J. Clin. 2007, 57, 242–255. [Google Scholar] [CrossRef] [PubMed]
- Adolescent Group YAOPR. Closing the Gap: Research and Care Imperatives for Adolescents and Young Adults with Cancer; NIH Publication No. 06-6067; Department of Health and Human Services, National Institutes of Health, National Cancer Institute, and the LIVESTRONG Young Adult Alliance: Bethesda, MD, USA, 2006. [Google Scholar]
- Jawad, M.U.; Cheung, M.C.; Min, E.S.; Schneiderbauer, M.M.; Koniaris, L.G.; Scully, S.P. Ewing sarcoma demonstrates racial disparities in incidence-related and sex-related differences in outcome: An analysis of 1631 cases from the SEER database, 1973–2005. Cancer 2009, 115, 3526–3536. [Google Scholar] [CrossRef] [PubMed]
- Cates, J.M.M. The AJCC 8th Edition Staging System for Soft Tissue Sarcoma of the Extremities or Trunk: A Cohort Study of the SEER Database. J. Natl. Compr. Cancer Netw. 2018, 16, 144–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, C.D.; Unni, K.; Mertens, F. (Eds.) World Health Organization Classification of Tumors: Pathology and Genetics of Tumors of Soft Tissue and Bone; IARC Press: Lyon, France, 2002. [Google Scholar]



{kind=link}
{kind=link}
| Demographics and Clinical Characteristics of the Entire Cohort | Number of Patients | Valid 100% of Total | |
|---|---|---|---|
| Total Patients | 4253 | 100 | |
| Age | |||
| 00–14 years | 27 | 0.6 | |
| 15–39 years | 301 | 7.1 | |
| 40–64 years | 763 | 17.9 | |
| ≥65 years | 3162 | 74.3 | |
| Sex | |||
| Male | 3398 | 79.9 | |
| Female | 855 | 20.1 | |
| Race/Ethnicity | |||
| NH White | 3643 | 89.2 | |
| NH Black | 119 | 2.9 | |
| NHAPI | 12 | 0.3 | |
| NHAIAN | 98 | 2.4 | |
| Hispanic | 210 | 5.1 | |
| Grade | |||
| Well Differentiated | 80 | 10.2 | |
| Moderate | 182 | 23.2 | |
| Poorly | 229 | 29.1 | |
| Undifferentiated | 295 | 37.5 | |
| Stage | |||
| Localized | 2725 | 78.6 | |
| Regional | 659 | 19 | |
| Distant | 81 | 2.3 | |
| Size | |||
| <5 cm | 1397 | 80.2 | |
| ≥5 cm | 344 | 19.8 | |
| Histology | |||
| Soft Tissue Sarcoma | 673 | 15.8 | |
| Fibromatous Sarcoma | 2738 | 64.4 | |
| Myxo-, Lipo-, Complex Mix Sarcoma | 31 | 0.7 | |
| Myomatous Sarcoma | 296 | 7 | |
| Vascular Sarcoma | 515 | 12.1 | |
| Surgery | |||
| Surgery | 3414 | 81.2 | |
| No Surgery | 789 | 18.8 | |
| Surgical Procedure | |||
| Skin Biopsy Including Mohs’ | 2666 | 78.1 | |
| Wide Excision Including Amputation | 748 | 21.9 | |
| Radiation Therapy | |||
| Radiotherapy | 1040 | 24.5 | |
| None | 3200 | 75.5 | |
| Chemotherapy | |||
| Chemotherapy | 165 | 4.5 | |
| None | 3509 | 95.5 | |
| Insurance | |||
| Insurance | 2357 | 95.2 | |
| No Insurance/MedicAid | 119 | 4.8 | |
| SES | |||
| Group 1 | 351 | 10.2 | |
| Group 2 | 581 | 16.9 | |
| Group 3 | 659 | 19.2 | |
| Group 4 | 822 | 23.9 | |
| Group 5 | 1026 | 29.8 | |
| Rurality Index | |||
| Rural | 374 | 10.8 | |
| Urban | 3095 | 89.2 | |
| Year of Diagnosis | |||
| 2000–2010 | 2093 | 49.2 | |
| 2011–2018 | 2160 | 50.8 | |
| Overall Survival According to Demographic and Clinical Characteristics (Proportion Surviving) | 5 Years Survival | 10 Years Survival | p-Value | |
|---|---|---|---|---|
| Overall | 0.44 | 0.27 | n/a | |
| Age | ||||
| 00–14 years | 0.95 | 0.95 | ||
| 15–39 years | 0.94 | 0.91 | ||
| 40–64 years | 0.78 | 0.63 | ||
| ≥65 years | 0.3 | 0.12 | <0.001 | |
| Sex | ||||
| Male | 0.41 | 0.23 | ||
| Female | 0.56 | 0.43 | <0.001 | |
| Race/Ethnicity | ||||
| NH White | 0.4 | 0.23 | ||
| NH Black | 0.76 | 0.64 | ||
| NHAPI | 0.54 | 0.45 | ||
| NHAIAN | 0.65 | 0.65 | ||
| Hispanic | 0.67 | 0.58 | <0.001 | |
| Grade | ||||
| Well Differentiated | 0.52 | 0.3 | ||
| Moderate | 0.43 | 0.27 | ||
| Poorly | 0.26 | 0.11 | ||
| Undifferentiated | 0.31 | 0.13 | <0.001 | |
| Stage | ||||
| Localized | 0.44 | 0.25 | ||
| Regional | 0.48 | 0.36 | ||
| Distant | 0.16 | 0.12 | <0.001 | |
| Size | ||||
| <5 cm | 0.43 | 0.28 | ||
| ≥5 cm | 0.37 | 0.24 | 0.04 | |
| Histology | ||||
| Soft Tissue Sarcoma | 0.37 | 0.23 | ||
| Fibromatous Sarcoma | 0.51 | 0.31 | ||
| Myxo-, Lipo-, Complex Mix Sarcoma | 0.62 | 0.51 | ||
| Myomatous Sarcoma | 0.36 | 0.24 | ||
| Vascular Sarcoma | 0.2 | 0.1 | <0.001 | |
| Surgery | ||||
| Surgery | 0.46 | 0.29 | ||
| No Surgery | 0.35 | 0.21 | <0.001 | |
| Surgical Procedure | ||||
| Skin Biopsy Including Mohs’ | 0.45 | 0.28 | ||
| Wide Excision Including Amputation | 0.48 | 0.3 | 0.025 | |
| Radiation Therapy | ||||
| Radiotherapy | 0.4 | 0.23 | ||
| None | 0.45 | 0.28 | <0.001 | |
| Chemotherapy | ||||
| Chemotherapy | 0.17 | 0.13 | ||
| None | 0.44 | 0.27 | <0.001 | |
| Insurance | ||||
| Insurance | 0.4 | 0.33 | ||
| No Insurance/MedicAid | 0.51 | 0.43 | 0.085 | |
| SES | ||||
| Group 1 | 0.46 | 0.28 | ||
| Group 2 | 0.44 | 0.27 | ||
| Group 3 | 0.4 | 0.24 | ||
| Group 4 | 0.41 | 0.26 | ||
| Group 5 | 0.44 | 0.29 | 0.01 | |
| Rurality Index | ||||
| Rural | 0.39 | 0.25 | ||
| Urban | 0.43 | 0.27 | 0.038 | |
| Year of Diagnosis | ||||
| 2000–2010 | 0.43 | 0.27 | ||
| 2011–2018 | 0.51 | ~ | 0.197 | |
| Multivariable Analysis | Number of Patients | Hazard Ratio | 95% CI | p-Value | |
|---|---|---|---|---|---|
| Age | |||||
| 00–14 years | ~ | ~ | ~ | ~ | |
| 15–39 years | 10 | 0 | 0–2.82 × 10167 | 0.946 | |
| 40–64 years | 50 | 0.245 | 0.139–0.433 | <0.001 | |
| ≥65 years | 233 | Reference Group | |||
| Sex | |||||
| Male | 236 | 0.706 | 0.460–1.083 | 0.111 | |
| Female | 57 | Reference Group | |||
| Race/Ethnicity | |||||
| NH White | 257 | 1.184 | 0.571–2.456 | 0.649 | |
| NH Black | 6 | 0.46 | 0.139–1.526 | 0.205 | |
| NHAPI | 13 | 2.057 | 0.715–5.923 | 0.619 | |
| NHAIAN | 1 | 1.785 | 0.182–17.471 | 0.181 | |
| Hispanic | 16 | Reference Group | |||
| Grade | |||||
| Well Differentiated | 29 | 0.947 | 0.522–1.718 | 0.857 | |
| Moderate | 71 | 0.804 | 0.515–1.256 | 0.338 | |
| Poorly | 90 | 0.996 | 0.679–1.461 | 0.985 | |
| Undifferentiated | 103 | Reference Group | |||
| Stage | |||||
| Localized | 184 | 0.256 | 0.113–0.582 | 0.001 | |
| Regional | 100 | 0.356 | 0.159–0.799 | 0.012 | |
| Distant | 9 | Reference Group | |||
| Size | |||||
| <5 cm | 227 | 0.804 | 0.55–1.175 | 0.259 | |
| ≥5 cm | 66 | Reference Group | |||
| Histology | |||||
| Soft Tissue Sarcoma | 73 | 0.675 | 0.408–1.116 | 0.126 | |
| Fibromatous Sarcoma | 104 | 0.587 | 0.374–0.922 | 0.021 | |
| Myxo-, Lipo-, Complex Mix Sarcoma | 5 | 0.463 | 0.131–1.640 | 0.233 | |
| Myomatous Sarcoma | 31 | 0.639 | 0.346–1.178 | 0.151 | |
| Vascular Sarcoma | 80 | Reference Group | |||
| Surgical Procedure | |||||
| Skin Biopsy Including Mohs’ | 209 | 0.882 | 0.622–1.250 | 0.481 | |
| Wide Excision Including Amputation | 84 | Reference Group | |||
| Radiation Therapy | |||||
| Radiotherapy | 82 | 0.861 | 0.593–1.248 | 0.429 | |
| None | 211 | Reference Group | |||
| Chemotherapy | |||||
| Chemotherapy | 25 | 1.599 | 0.848–3.014 | 0.147 | |
| None | 268 | Reference Group | |||
| SES | |||||
| Group 1 | 34 | 2.33 | 1.3–4.178 | 0.005 | |
| Group 2 | 50 | 1.368 | 0.821–2.279 | 0.229 | |
| Group 3 | 57 | 1.711 | 1.069–2.738 | 0.025 | |
| Group 4 | 76 | 1.594 | 1.022–2.486 | 0.04 | |
| Group 5 | 76 | Reference Group | |||
| Rurality Index | |||||
| Rural | 37 | 0.746 | 0.438–1.271 | 0.281 | |
| Urban | 256 | Reference Group |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jawad, M.U.; Zeitlinger, L.N.; Bewley, A.F.; O’Donnell, E.F., III; Traven, S.A.; Carr-Ascher, J.R.; Monjazeb, A.M.; Canter, R.J.; Thorpe, S.W.; Randall, R.L. Head and Neck Cutaneous Soft-Tissue Sarcoma Demonstrate Sex and Racial/Ethnic Disparities in Incidence and Socioeconomic Disparities in Survival. J. Clin. Med. 2022, 11, 5475. https://doi.org/10.3390/jcm11185475
Jawad MU, Zeitlinger LN, Bewley AF, O’Donnell EF III, Traven SA, Carr-Ascher JR, Monjazeb AM, Canter RJ, Thorpe SW, Randall RL. Head and Neck Cutaneous Soft-Tissue Sarcoma Demonstrate Sex and Racial/Ethnic Disparities in Incidence and Socioeconomic Disparities in Survival. Journal of Clinical Medicine. 2022; 11(18):5475. https://doi.org/10.3390/jcm11185475
Chicago/Turabian StyleJawad, Muhammad Umar, Lauren N. Zeitlinger, Arnaud F. Bewley, Edmond F. O’Donnell, III, Sophia A. Traven, Janai R. Carr-Ascher, Arta M. Monjazeb, Robert J. Canter, Steven W. Thorpe, and R. Lor Randall. 2022. "Head and Neck Cutaneous Soft-Tissue Sarcoma Demonstrate Sex and Racial/Ethnic Disparities in Incidence and Socioeconomic Disparities in Survival" Journal of Clinical Medicine 11, no. 18: 5475. https://doi.org/10.3390/jcm11185475