
Comparison of Endoscopic Submucosal Dissection and Radical Surgery for Early Gastric Cancer in Remnant Stomach
 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Evaluation Index
2.3. ESD Technique
2.4. Surgical Technique
2.5. Post-operative Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Baseline and Clinicopathologic Characteristics
3.2. Short-Term Outcomes
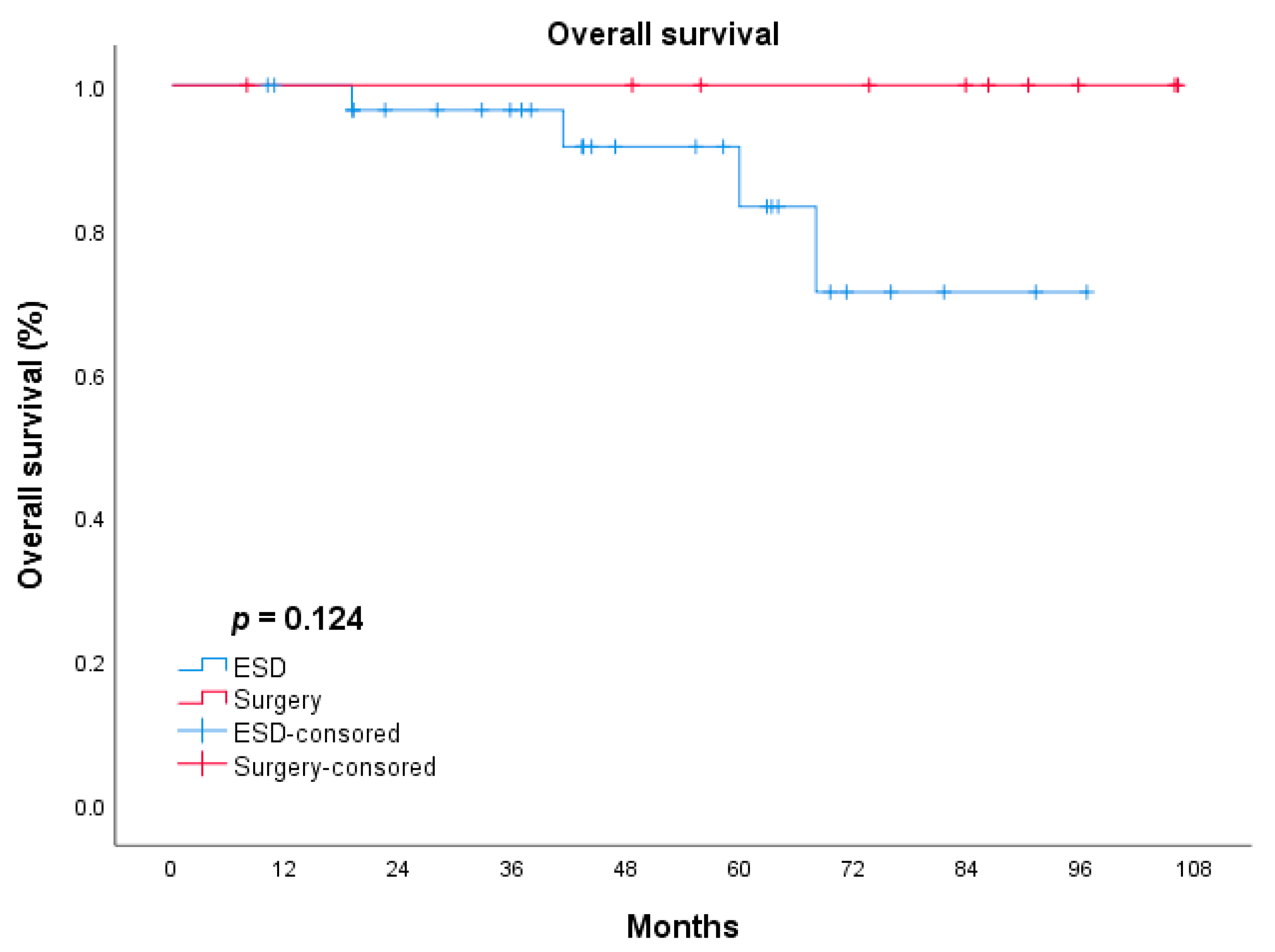
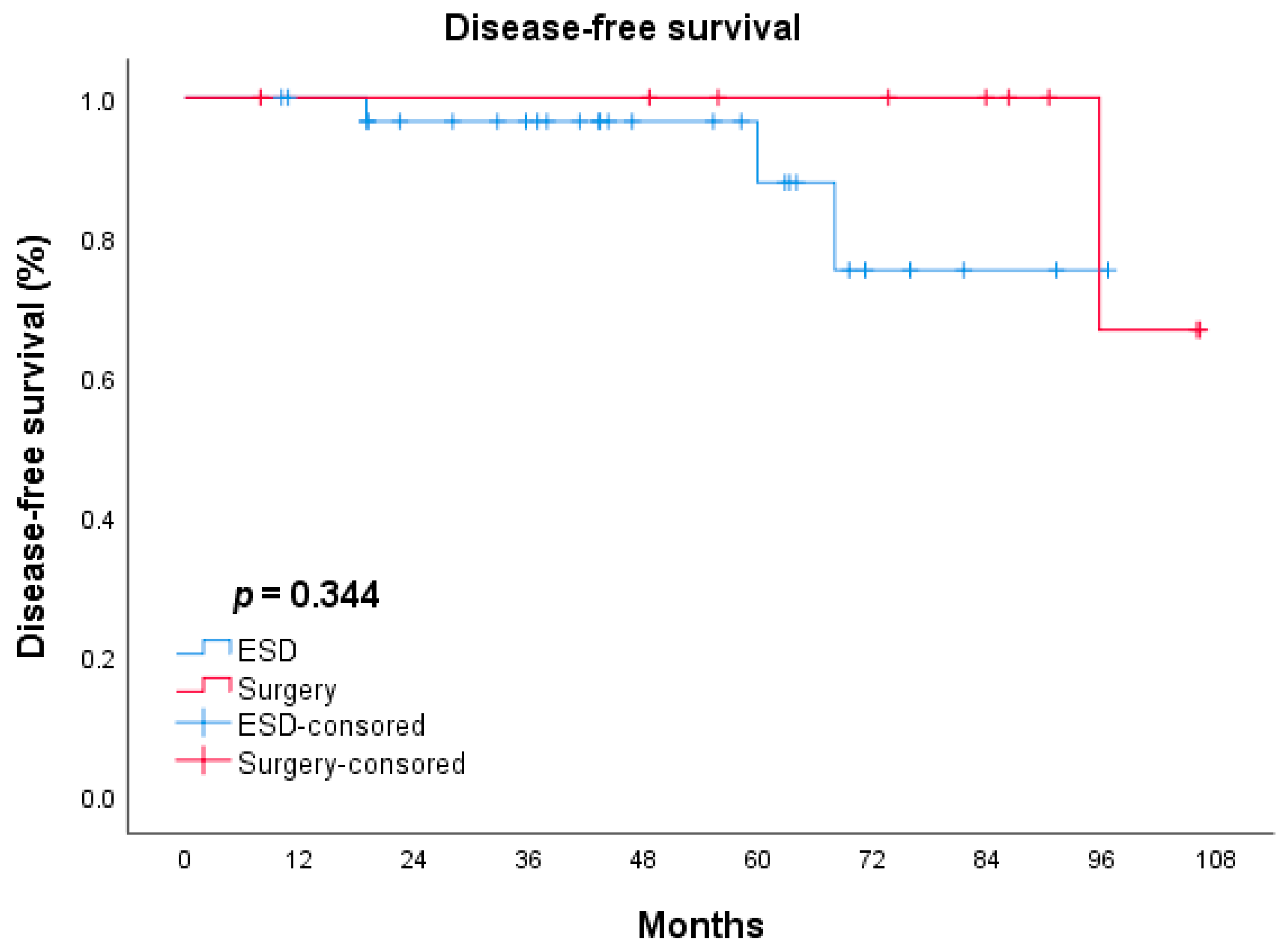
3.3. Long-Term Survival Outcomes
3.4. Comparison of the QOL Scores of the ESD and Surgery Groups
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ohashi, M.; Katai, H.; Fukagawa, T.; Gotoda, T.; Sano, T.; Sasako, M. Cancer of the Gastric Stump Following Distal Gastrectomy for Cancer. Br. J. Surg. 2007, 94, 92–95. [Google Scholar] [CrossRef]
- Kaneko, K.; Kondo, H.; Saito, D.; Shirao, K.; Yamaguchi, H.; Yokota, T.; Yamao, G.; Sano, T.; Sasako, M.; Yoshida, S. Early Gastric Stump Cancer Following Distal Gastrectomy. Gut 1998, 43, 342–344. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, Y.; Saku, M.; Kishihara, F.; Maehara, Y. Effective Follow-up for Recurrence or a Second Primary Cancer in Patients with Early Gastric Cancer. Br. J. Surg. 2005, 92, 235–239. [Google Scholar] [CrossRef]
- Ojima, T.; Iwahashi, M.; Nakamori, M.; Nakamura, M.; Naka, T.; Katsuda, M.; Iida, T.; Tsuji, T.; Hayata, K.; Takifuji, K.; et al. Clinicopathological Characteristics of Remnant Gastric Cancer after a Distal Gastrectomy. J. Gastrointest. Surg. 2010, 14, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Nonaka, S.; Oda, I.; Sato, C.; Abe, S.; Suzuki, H.; Yoshinaga, S.; Hokamura, N.; Igaki, H.; Tachimori, Y.; Taniguchi, H.; et al. Endoscopic Submucosal Dissection for Gastric Tube Cancer after Esophagectomy. Gastrointest. Endosc. 2014, 79, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.H.; Kim, J.W.; Yoo, M.W.; Park, D.J.; Lee, H.J.; Lee, K.U.; Yang, H.K. Clinicopathological Features and Surgical Outcomes of Patients with Remnant Gastric Cancer after a Distal Gastrectomy. Ann. Surg. Oncol. 2008, 15, 1632–1639. [Google Scholar] [CrossRef]
- Greene, F.L. Management of Gastric Remnant Carcinoma Based on the Results of a 15-Year Endoscopic Screening Program. Ann. Surg. 1996, 223, 701–706. [Google Scholar] [CrossRef]
- Kim, I.Y.; Kim, Y.A.; Kim, C.G.; Ryu, K.W.; Kim, Y.W.; Sim, J.A.; Yun, Y.H.; Choi, I.J. Serial Intermediate-Term Quality of Life Comparison after Endoscopic Submucosal Dissection Versus Surgery in Early Gastric Cancer Patients. Surg. Endosc. 2018, 32, 2114–2122. [Google Scholar] [CrossRef]
- Choi, H.J.; Kim, E.S.; Lee, Y.J.; Cho, K.B.; Park, K.S.; Jang, B.K.; Chung, W.J.; Hwang, J.S.; Ryu, S.W. Comparison of Quality of Life and Worry of Cancer Recurrence between Endoscopic and Surgical Treatment for Early Gastric Cancer. Gastrointest. Endosc. 2015, 82, 299–307. [Google Scholar] [CrossRef]
- Choi, J.I.; Lee, J.H.; Kim, Y.I.; Kim, C.G.; Cho, S.J.; Lee, J.Y.; Ryu, K.W.; Nam, B.H.; Kook, M.C.; Kim, Y.W. Long-Term Outcome Comparison of Endoscopic Resection and Surgery in Early Gastric Cancer Meeting the Absolute Indication for Endoscopic Resection. Gastrointest. Endosc. 2015, 81, 333–341.e1. [Google Scholar] [CrossRef]
- Hirasaki, S.; Kanzaki, H.; Matsubara, M.; Fujita, K.; Matsumura, S.; Suzuki, S. Treatment of Gastric Remnant Cancer Post Distal Gastrectomy by Endoscopic Submucosal Dissection Using an Insulation-Tipped Diathermic Knife. World J. Gastroenterol. 2008, 14, 2550–2555. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, R.; Kawahara, Y.; Okada, H.; Tsuzuki, T.; Yagi, S.; Kato, J.; Ohara, N.; Yoshino, T.; Imagawa, A.; Fujiki, S.; et al. Endoscopic Submucosal Dissection for Cancers of the Remnant Stomach after Distal Gastrectomy. Gastrointest. Endosc. 2008, 67, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Yamashina, T.; Uedo, N.; Dainaka, K.; Aoi, K.; Matsuura, N.; Ito, T.; Fujii, M.; Kanesaka, T.; Yamamoto, S.; Akasaka, T.; et al. Long-Term Survival after Endoscopic Resection for Early Gastric Cancer in the Remnant Stomach: Comparison with Radical Surgery. Ann. Gastroenterol. 2015, 28, 66–71. [Google Scholar] [PubMed]
- Fukui, Y.; Shindoh, J.; Inoshita, N.; Mizuno, A.; Haruta, S.; Udagawa, H.; Hoteya, S.; Tsunoda, S.; Miyamoto, S.; Ozawa, R.; et al. Efficacy of Endoscopic Management for Early Remnant Gastric Cancer: Is Completion Gastrectomy Truly Necessary in Cases with Marginally Noncurative Histopathologic Features? Ann. Surg. Oncol. 2018, 25, 1608–1615. [Google Scholar] [CrossRef]
- Tanaka, S.; Toyonaga, T.; Morita, Y.; Fujita, T.; Yoshizaki, T.; Kawara, F.; Wakahara, C.; Obata, D.; Sakai, A.; Ishida, T.; et al. Endoscopic Submucosal Dissection for Early Gastric Cancer in Anastomosis Site after Distal Gastrectomy. Gastric. Cancer 2014, 17, 371–376. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese Classification of Gastric Carcinoma: 3rd English Edition. Gastric. Cancer 2011, 14, 101–112. [Google Scholar] [CrossRef]
- Charlson, E.M.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Clavien, A.P.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo Classification of Surgical Complications: Five-Year Experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2018 (5th Edition). Gastric. Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef]
- Iwata, Y.; Ito, S.; Misawa, K.; Ito, Y.; Komori, K.; Abe, T.; Shimizu, Y.; Tajika, M.; Niwa, Y.; Yoshida, K.; et al. Incidence and Treatment of Metachronous Gastric Cancer after Proximal Gastrectomy. Surg. Today 2018, 48, 552–557. [Google Scholar] [CrossRef]
- Nonaka, S.; Oda, I.; Makazu, M.; Haruyama, S.; Abe, S.; Suzuki, H.; Yoshinaga, S.; Nakajima, T.; Kushima, R.; Saito, Y. Endoscopic Submucosal Dissection for Early Gastric Cancer in the Remnant Stomach after Gastrectomy. Gastrointest. Endosc. 2013, 78, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Min, B.H.; Lee, J.G.; Noh, D.; Lee, J.H.; Rhee, P.L.; Kim, J.J. Endoscopic Submucosal Dissection for Early Gastric Neoplasia Occurring in the Remnant Stomach after Distal Gastrectomy. Clin. Endosc. 2016, 49, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Song, G.B.; Kim, G.H. Endoscopic Submucosal Dissection of Gastric Epithelial Neoplasms after Partial Gastrectomy: A Single-Center Experience. Gastroenterol. Res. Pract. 2017, 2017, 6395283. [Google Scholar] [CrossRef] [PubMed]
- Yabuuchi, Y.; Kakushima, N.; Takizawa, K.; Tanaka, M.; Kawata, N.; Yoshida, M.; Kishida, Y.; Ito, S.; Imai, K.; Ishiwatari, H.; et al. Short- and Long-Term Outcomes of Endoscopic Submucosal Dissection for Early Gastric Cancer in the Remnant Stomach after Gastrectomy. J. Gastroenterol. 2019, 54, 511–520. [Google Scholar] [CrossRef]
- Nishide, N.; Ono, H.; Kakushima, N.; Takizawa, K.; Tanaka, M.; Matsubayashi, H.; Yamaguchi, Y. Clinical Outcomes of Endoscopic Submucosal Dissection for Early Gastric Cancer in Remnant Stomach or Gastric Tube. Endoscopy 2012, 44, 577–583. [Google Scholar] [CrossRef]
- Hahn, Y.K.; Park, C.H.; Lee, Y.K.; Chung, H.; Park, J.C.; Shin, S.K.; Lee, Y.C.; Kim, H.I.; Cheong, J.H.; Hyung, W.J.; et al. Comparative Study between Endoscopic Submucosal Dissection and Surgery in Patients with Early Gastric Cancer. Surg. Endosc. 2018, 32, 73–86. [Google Scholar] [CrossRef]
- Cho, H.J.; Cha, S.W.; Kim, H.G.; Lee, T.H.; Cho, J.Y.; Ko, W.J.; Jin, S.Y.; Park, S. Long-Term Outcomes of Endoscopic Submucosal Dissection for Early Gastric Cancer: A Comparison Study to Surgery Using Propensity Score-Matched Analysis. Surg. Endosc. 2016, 30, 3762–3773. [Google Scholar] [CrossRef]
- Takahashi, M.; Terashima, M.; Kawahira, H.; Nagai, E.; Uenosono, Y.; Kinami, S.; Nagata, Y.; Yoshida, M.; Aoyagi, K.; Kodera, Y.; et al. Quality of Life after Total Vs Distal Gastrectomy with Roux-En-Y Reconstruction: Use of the Postgastrectomy Syndrome Assessment Scale-45. World J. Gastroenterol. 2017, 23, 2068–2076. [Google Scholar] [CrossRef]
- Park, S.; Chung, H.Y.; Lee, S.S.; Kwon, O.; Yu, W. Serial Comparisons of Quality of Life after Distal Subtotal or Total Gastrectomy: What Are the Rational Approaches for Quality of Life Management? J. Gastric. Cancer 2014, 14, 32–38. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, H.J.; Choi, Y.S.; Kim, T.H.; Huh, Y.J.; Suh, Y.S.; Kong, S.H.; Yang, H.K. Postoperative Quality of Life after Total Gastrectomy Compared with Partial Gastrectomy: Longitudinal Evaluation by European Organization for Research and Treatment of Cancer-Og25 and Sto22. J. Gastric. Cancer 2016, 16, 230–239. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.S.; Chung, H.Y.; Kwon, O.K.; Yu, W. Long-Term Quality of Life after Distal Subtotal and Total Gastrectomy: Symptom- and Behavior-Oriented Consequences. Ann. Surg. 2016, 263, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Ojima, T.; Takifuji, K.; Nakamura, M.; Nakamori, M.; Katsuda, M.; Iida, T.; Hayata, K.; Iwahashi, M.; Yamaue, H. Endoscopic Submucosal Dissection for Gastric Tumors in Various Types of Remnant Stomach. Endoscopy 2014, 46, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Dou, L.; Zhang, Y.; He, S.; Liu, Y.; Lei, H.; Wang, G. Safety and Efficacy of Endoscopic Submucosal Dissection for Metachronous Early Cancer or Precancerous Lesions Emerging at the Anastomotic Site after Curative Surgical Resection of Colorectal Cancer. Ann. Transl. Med. 2020, 8, 1411. [Google Scholar] [CrossRef] [PubMed]
- Ramos, M.F.K.P.; Pereira, M.C.M.; Oliveira, Y.S.; Pereira, M.A.; Barchi, L.C.; Dias, A.R.; Zilberstein, B.; Junior, U.R.; Cecconello, I. Surgical Results of Remnant Gastric Cancer Treatment. Rev. Col. Bras. Cir. 2020, 47, e20202703. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ESD (n = 48) | Surgery (n = 25) | p Value | |
|---|---|---|---|
| Gender, number (%) | 0.295 | ||
| Male | 43 (89.6%) | 20(80.0%) | |
| Female | 5 (10.4%) | 5(20.0%) | |
| Age, mean (SD), y | 64.88 (8.30) | 57.44(9.64) | 0.001 |
| Reasons of previous operation, number (%) | 0.786 | ||
| Gastric cancer | 36 (75.0%) | 17(68.0%) | |
| Benign gastric ulcer | 1 (2.1%) | 6(24.0%) | |
| Esophageal cancer | 10 (20.8%) | 0(0%) | |
| Other (mesenchymoma/leiomyoma) | 1 (2.1%) | 2 (8.0%) | |
| Type of previous operation, n (%) | 0.037 | ||
| Distal gastrectomy | |||
| Billroth-I | 14 (29.2%) | 14(56.0%) | |
| Billroth-II | 9 (18.8%) | 5(20.0%) | |
| Proximal gastrectomy | 15 (31.3%) | 6(24.0%) | |
| Esophagectomy | 10 (20.8%) | 0(0%) | |
| Tumor location, n (%) | 0.023 | ||
| Fundus | 1 (2.1%) | 1(4.0%) | |
| Body | 14 (29.2%) | 8(32.0%) | |
| Antrum | 15 (31.3%) | 2(8.0%) | |
| Cardia | 17 (35.4%) | 10(40.0%) | |
| Anastomosis site | 1 (2.1%) | 4(16.0%) | |
| Tumor size, mm | |||
| Median (P25,P75) | 20.00 (10.25, 30.00) | 25.00(18.50,35.00) | 0.077 |
| Macroscopic type, n (%) | 0.097 | ||
| 0-I | 4 (8.4%) | 10(40.0%) | |
| 0-IIa | 15 (31.3%) | 1(4.0%) | |
| 0-IIb | 3 (6.3%) | 5(20.0%) | |
| 0-IIc | 7 (14.6%) | 3(12.0%) | |
| 0-IIc + IIa | 19 (39.6%) | 3(24.0%) | |
| Histologic type, n (%) | 0.016 | ||
| Differentiated | 34 (70.8%) | 12(48.0%) | |
| Undifferentiated | 14 (29.2%) | 13(52.0%) | |
| Depth of tumor invasion, n (%) | 0.008 | ||
| M | 40 (83.4%) | 17 (68%) | |
| SM1 | 4 (8.3%) | 2 (8.0%) | |
| SM2 | 4 (8.3%) | 6 (24.0%) | |
| Lymphovascular invasion, n (%) | 0.331 | ||
| Present | 2 (4.2%) | 3 (12.0%) | |
| Absent | 46 (95.8%) | 22 (88.0%) | |
| Neural invasion, n (%) | 0.547 | ||
| Present | 1 (2.1%) | 2 (8.0%) | |
| Absent | 47 (97.9%) | 23 (92.0%) | |
| ESD (n = 48) | Surgery (n = 25) | p Value | ||
|---|---|---|---|---|
| Short-term outcomes | ||||
| Operation time, median (SD), minute | 39.5 (31.6) | 255.0 (107.8) | 0.000 | |
| Hospital stays after surgery, median (SD), day | 6.0 (1.24) | 15.0 (11.07) | 0.002 | |
| Peri-operative complication, number (%) | 6 (12.5%) | 12 (48%) | 0.001 | |
| bleeding | 5 | 1 | ||
| perforation | 0 | 0 | ||
| stenosis | 1 | - | ||
| pleural effusion | - | 1 | ||
| anastomotic fistula | - | 4 | ||
| wound infection | - | 3 | ||
| Other | - | 3 | ||
| Clavien–Dindo, number (%) | ||||
| I–II | 3 (6.25%) | 7 (28%) | ||
| III–IV | 3 (6.25%) | 5 (20%) | ||
| V | 0 | 0 | ||
| Treatment efficacy, number (%) | ||||
| R0 resection | 44 (91.7%) | - | - | |
| En bloc resection | 48 (100%) | - | ||
| Curative resection | 39 (73.9%) | - | ||
| Lymph node metastasis | - | 2 (8.0%) | - | |
| Long-term outcomes | ||||
| Length of follow-up, median (SD), month | 41.7 (23.29) | 73.6 (36.62) | 0.684 | |
| Recurrence, number (%) | 5 (10.4%) | 3 (12.0%) | ||
| Gastric cancer-related deaths, number (%) | 4 (8.3%) | 3 (12.0%) | ||
| Time after treatment to recurrence, median (SD), month | 36.0 (78.56) | 69.0 (142.48) | ||
| Case | Age | Reason of Previous Operation | TNM Staging of Previous Lesions | Type of Secondary Operation | Tumor Characteristics | Location of Recurrence | Additional Treatment for Recurrence | Cause of Death | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Macroscopic Type | Histological Type | Depth of Tumor Invasion | Lymphovascular Invasion | Neural Invasion | Curative Resection | ||||||||
| 1 | 67 | Esophageal cancer | IB | ESD | II-a + II-c | Differentiated | Mucosa | Negative | Negative | Yes | Bone | Symptomatic treatment | Esophageal cancer-related |
| 2 | 58 | Gastric cancer | IIIA | ESD | II-b | Differentiated | Mucosa | Negative | Negative | Yes | Liver | Chemoradiotherapy | Gastric cancer-related |
| 3 | 56 | Gastric cancer | IIIC | ESD | II-a + II-c | Differentiated | Mucosa | Negative | Negative | Yes | Colon | Symptomatic treatment | Gastric cancer-related |
| 4 | 74 | Gastric cancer | NA | ESD | I-s | Differentiated | Mucosa | Negative | Negative | Yes | - | - | Colon cancer-related |
| 5 | 62 | Gastric cancer | IIIC | ESD | II-a + II-c | Undifferentiated | Mucosa | Negative | Negative | Yes | Bone | Radiotherapy | Gastric cancer-related |
| 6 | 77 | Gastric cancer | NA | ESD | II-a | Differentiated | Mucosa | Negative | Negative | Yes | - | - | Apastia |
| 7 | 58 | Esophageal stromal tumor | NA | ESD | II-c | Undifferentiated | Mucosa | Negative | Negative | No | Liver and retroperitoneal lymph node | Symptomatic treatment | Gastric cancer-related |
| 8 | 57 | Gastric ulcer | - | TG | I-s | Undifferentiated | Submucosa | Negative | Positive | - | Liver and retroperitoneal lymph node | Chemoradiotherapy | Gastric cancer-related |
| 9 | 71 | Gastric ulcer | - | TG | II-b | Differentiated | Mucosa | Negative | Negative | - | - | - | Myocardial infarction |
| 10 | 73 | Gastric cancer | NA | TG | I-s | Differentiated | Mucosa | Negative | Negative | - | Liver and bone | Symptomatic treatment | Gastric cancer-related |
| 11 | 57 | Gastric cancer | NA | TG | I-s | Differentiated | Mucosa | Negative | Negative | - | - | - | Esophageal cancer-related |
| 12 | 45 | Gastric cancer | NA | TG | II-c | Undifferentiated | Mucosa | Negative | Negative | - | Liver and retroperitoneal lymph node | Surgery and Chemoradiotherapy | Gastric cancer-related |
| ESD (n = 32) | Surgery (n = 13) | p-Value | |
|---|---|---|---|
| EORTC-QLQ-C30 functional scales, mean (SD) | |||
| Global health status | 71.58 (15.06) | 61.90 (12.54) | 0.041 |
| Physical functioning | 97.71 (5.25) | 84.29 (16.46) | 0.010 |
| Role functioning | 95.83 (11.20) | 69.05 (14.41) | <0.001 |
| Emotional functioning | 91.41 (16.87) | 74.40 (23.68) | 0.008 |
| Cognitive functioning | 97.92 (7.02) | 89.29 (14.03) | 0.044 |
| Social functioning | 94.79 (14.93) | 76.19 (24.21) | 0.016 |
| EORTC-QLQ-C30 symptom scales, mean (SD) | |||
| Fatigue | 6.25 (13.22) | 25.40 (17.66) | <0.001 |
| Nausea and vomiting | 7.81 (15.25) | 14.29 (11.05) | 0.160 |
| Pain | 3.65 (9.21) | 10.71 (14.03) | 0.048 |
| Dyspnea | 11.46 (42.00) | 11.90 (16.57) | 0.970 |
| Insomnia | 13.54 (25.20) | 23.81 (30.46) | 0.239 |
| Appetite loss | 2.08 (8.20) | 45.24 (38.36) | 0.001 |
| Constipation | 14.58 (26.69) | 28.57 (25.68) | 0.105 |
| Diarrhea | 13.54 (22.17) | 23.81 (24.21) | 0.167 |
| Financial difficulties | 5.21 (12.30) | 28.57 (22.10) | <0.001 |
| EORTC-QLQ-STO22 symptom scales, mean (SD) | |||
| Dysphagia | 4.86 (7.95) | 20.63 (12.97) | 0.001 |
| Pain | 7.55 (11.07) | 27.98 (22.55) | <0.001 |
| Reflux symptoms | 15.63 (18.69) | 19.84 (15.21) | 0.462 |
| Eating restrictions | 3.91 (7.92) | 23.81 (19.30) | 0.002 |
| Anxiety | 5.90 (15.71) | 22.22 (27.91) | 0.056 |
| Dry mouth | 3.13 (9.87) | 11.90 (16.57) | 0.082 |
| Taste | 3.13 (13.01) | 9.52 (15.63) | 0.156 |
| Hair loss | 2.08 (8.20) | 14.29 (17.12) | 0.022 |
| Body image | 2.08 (8.20) | 28.57 (22.01) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Chen, Z.; Zhou, H.; Chen, Y.; Dou, L.; Zhang, Y.; Liu, Y.; He, S.; Zhao, D.; Wang, G. Comparison of Endoscopic Submucosal Dissection and Radical Surgery for Early Gastric Cancer in Remnant Stomach. J. Clin. Med. 2022, 11, 5403. https://doi.org/10.3390/jcm11185403
Liu Y, Chen Z, Zhou H, Chen Y, Dou L, Zhang Y, Liu Y, He S, Zhao D, Wang G. Comparison of Endoscopic Submucosal Dissection and Radical Surgery for Early Gastric Cancer in Remnant Stomach. Journal of Clinical Medicine. 2022; 11(18):5403. https://doi.org/10.3390/jcm11185403
Chicago/Turabian StyleLiu, Yi, Zhihao Chen, Hong Zhou, Yingtai Chen, Lizhou Dou, Yueming Zhang, Yong Liu, Shun He, Dongbing Zhao, and Guiqi Wang. 2022. "Comparison of Endoscopic Submucosal Dissection and Radical Surgery for Early Gastric Cancer in Remnant Stomach" Journal of Clinical Medicine 11, no. 18: 5403. https://doi.org/10.3390/jcm11185403