
Root Canal Filling Quality Comparison of a Premixed Calcium Silicate Endodontic Sealer and Different Carrier-Based Obturation Systems

 , ,
, ,  , and
, and
Abstract
:1. Introduction
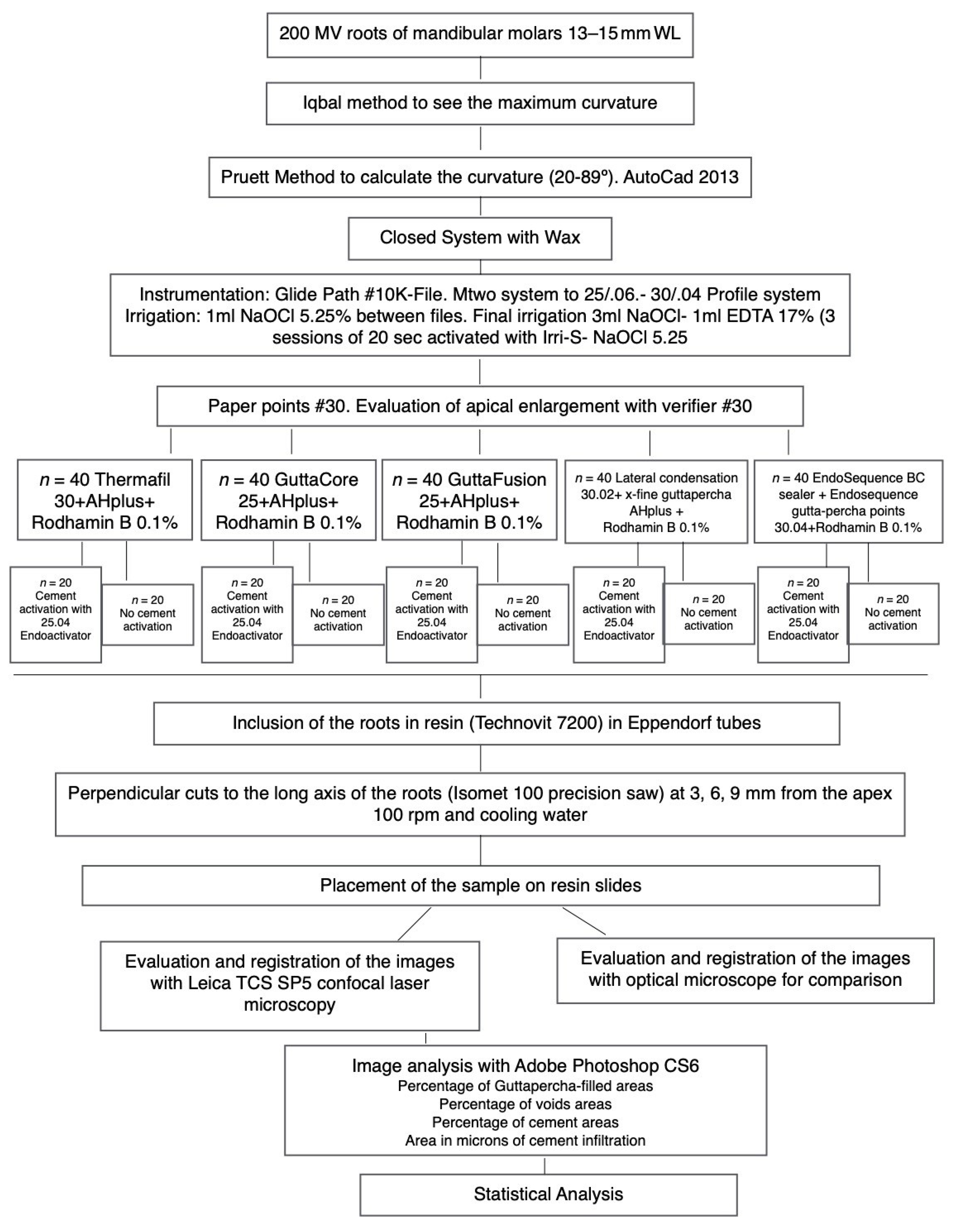
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siqueira, J.F., Jr. Aetiology of root canal treatment failure: Why well-treated teeth can fail. Int. Endod. J. 2001, 34, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siqueira, J.F., Jr.; Araujo, M.C.; Garcia, P.F.; Fraga, R.C.; Dantas, C.J. Histological evaluation of the effectiveness of five instrumentation techniques for cleaning the apical third of root canals. J. Endod. 1997, 23, 499–502. [Google Scholar] [CrossRef]
- Heeren, T.J.; Levitan, M.E. Effect of canal preparation on fill length in straight root canals obturated with RealSeal 1 and Thermafil Plus. J. Endod. 2012, 38, 1380–1382. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.B. A new gutta-percha technique. J. Endod. 1978, 4, 184–188. [Google Scholar] [CrossRef]
- Alfayate, R.P.; Pinilla, J.A.; Pereda, A.A.; Bellido, M.M.; Stincone, S.; Cabello, R.C. In vitro randomized-trial on the sealing ability of carrier-based systems in curved root canals. Endodoncia 2018, 35, 65–75. [Google Scholar]
- Zhou, H.M.; Shen, Y.; Zheng, W.; Li, L.; Zheng, Y.F.; Haapasalo, M. Physical properties of 5 root canal sealers. J. Endod. 2013, 39, 1281–1286. [Google Scholar] [CrossRef]
- Candeiro, G.T.; Correia, F.C.; Duarte, M.A.; Ribeiro-Siqueira, D.C.; Gavini, G. Evaluation of radiopacity, pH, release of calcium ions, and flow of a bioceramic root canal sealer. J. Endod. 2012, 38, 842–845. [Google Scholar] [CrossRef] [Green Version]
- Loushine, B.A.; Bryan, T.E.; Looney, S.W.; Gillen, B.M.; Loushine, R.J.; Weller, R.N.; Pashley, D.H.; Tay, F.R. Setting properties and cytotoxicity evaluation of a premixed bioceramic root canal sealer. J. Endod. 2011, 37, 673–677. [Google Scholar] [CrossRef]
- Han, L.; Okiji, T. Bioactivity evaluation of three calcium silicate-based endodontic materials. Int. Endod. J. 2013, 46, 808–814. [Google Scholar] [CrossRef]
- Kim, J.A.; Hwang, Y.C.; Rosa, V.; Yu, M.K.; Lee, K.W.; Min, K.S. Root Canal Filling Quality of a Premixed Calcium Silicate Endodontic Sealer Applied Using Gutta-percha Cone-mediated Ultrasonic Activation. J. Endod. 2018, 44, 133–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, M.; Kupper, K.; Reimann, S.; Bourauel, C.; Frentzen, M. 3D analyses of interface voids in root canals filled with different sealer materials in combination with warm gutta-percha technique. Clin. Oral Investig. 2014, 18, 155–161. [Google Scholar] [CrossRef]
- Pruett, J.P.; Clement, D.J.; Carnes, D.L., Jr. Cyclic fatigue testing of nickel-titanium endodontic instruments. J. Endod. 1997, 23, 77–85. [Google Scholar] [CrossRef]
- Iqbal, M.K.; Maggiore, F.; Suh, B.; Edwards, K.R.; Kang, J.; Kim, S. Comparison of apical transportation in four Ni-Ti rotary instrumentation techniques. J. Endod. 2003, 29, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Guinesi, A.S.; Faria, G.; Tanomaru-Filho, M.; Bonetti-Filho, I. Influence of sealer placement technique on the quality of root canal filling by lateral compaction or single cone. Braz. Dent. J. 2014, 25, 117–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Said, H.M.; Bakar, W.Z.; Farea, M.; Husein, A. The effect of different sealer placement techniques on sealing Ability: An in vitro study. J. Conserv. Dent. 2012, 15, 257–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, M.C.; Clement, D.J.; Dove, S.B.; Walker, W.A., 3rd. A comparison of sealer placement techniques in curved canals. J. Endod. 1996, 22, 638–642. [Google Scholar] [CrossRef]
- Wiemann, A.H.; Wilcox, L.R. In vitro evaluation of four methods of sealer placement. J. Endod. 1991, 17, 444–447. [Google Scholar] [CrossRef]
- Kahn, F.H.; Rosenberg, P.A.; Schertzer, L.; Korthals, G.; Nguyen, P.N. An in-vitro evaluation of sealer placement methods. Int. Endod. J. 1997, 30, 181–186. [Google Scholar] [CrossRef]
- Wiesse, P.E.B.; Silva-Sousa, Y.T.; Pereira, R.D.; Estrela, C.; Domingues, L.M.; Pecora, J.D.; Sousa-Neto, M.D. Effect of ultrasonic and sonic activation of root canal sealers on the push-out bond strength and interfacial adaptation to root canal dentine. Int. Endod. J. 2018, 51, 102–111. [Google Scholar] [CrossRef]
- De Gregorio, C.; Estevez, R.; Cisneros, R.; Heilborn, C.; Cohenca, N. Effect of EDTA, sonic, and ultrasonic activation on the penetration of sodium hypochlorite into simulated lateral canals: An in vitro study. J. Endod. 2009, 35, 891–895. [Google Scholar] [CrossRef] [PubMed]
- Gu, L.S.; Kim, J.R.; Ling, J.; Choi, K.K.; Pashley, D.H.; Tay, F.R. Review of contemporary irrigant agitation techniques and devices. J. Endod. 2009, 35, 791–804. [Google Scholar] [CrossRef]
- Guimaraes, B.M.; Amoroso-Silva, P.A.; Alcalde, M.P.; Marciano, M.A.; de Andrade, F.B.; Duarte, M.A. Influence of ultrasonic activation of 4 root canal sealers on the filling quality. J. Endod. 2014, 40, 964–968. [Google Scholar] [CrossRef]
- Retsas, A.; Koursoumis, A.; Tzimpoulas, N.; Boutsioukis, C. Uncontrolled Removal of Dentin during In Vitro Ultrasonic Irrigant Activation in Curved Root Canals. J. Endod. 2016, 42, 1545–1549. [Google Scholar] [CrossRef]
- Arslan, H.; Abbas, A.; Karatas, E. Influence of ultrasonic and sonic activation of epoxy-amine resin-based sealer on penetration of sealer into lateral canals. Clin. Oral Investig. 2016, 20, 2161–2164. [Google Scholar] [CrossRef]
- Schafer, E.; Schrenker, C.; Zupanc, J.; Burklein, S. Percentage of Gutta-percha Filled Areas in Canals Obturated with Cross-linked Gutta-percha Core-carrier Systems, Single-Cone and Lateral Compaction Technique. J. Endod. 2016, 42, 294–298. [Google Scholar] [CrossRef]
- Li, G.H.; Niu, L.N.; Selem, L.C.; Eid, A.A.; Bergeron, B.E.; Chen, J.H.; Pashley, D.H.; Tay, F.R. Quality of obturation achieved by an endodontic core-carrier system with crosslinked gutta-percha carrier in single-rooted canals. J. Dent. 2014, 42, 1124–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beasley, R.T.; Williamson, A.E.; Justman, B.C.; Qian, F. Time required to remove guttacore, thermafil plus, and thermoplasticized gutta-percha from moderately curved root canals with protaper files. J. Endod. 2013, 39, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, K.W.; Schick, A.; Lussi, A. Apical filling characteristics of carrier-based techniques vs. single cone technique in curved root canals. Clin. Oral Investig. 2016, 20, 1631–1637. [Google Scholar] [CrossRef]
- Marciano, M.A.; Ordinola-Zapata, R.; Cunha, T.V.; Duarte, M.A.; Cavenago, B.C.; Garcia, R.B.; Bramante, C.M.; Bernardineli, N.; Moraes, I.G. Analysis of four gutta-percha techniques used to fill mesial root canals of mandibular molars. Int. Endod. J. 2011, 44, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Pedulla, E.; Abiad, R.S.; Conte, G.; La Rosa, G.R.M.; Rapisarda, E.; Neelakantan, P. Root fillings with a matched-taper single cone and two calcium silicate-based sealers: An analysis of voids using micro-computed tomography. Clin. Oral Investig. 2020, 24, 4487–4492. [Google Scholar] [CrossRef] [PubMed]
- Celikten, B.; Uzuntas, C.F.; Orhan, A.I.; Orhan, K.; Tufenkci, P.; Kursun, S.; Demiralp, K.O. Evaluation of root canal sealer filling quality using a single-cone technique in oval shaped canals: An In vitro Micro-CT study. Scanning 2016, 38, 133–140. [Google Scholar] [CrossRef]
- Alsubait, S.; Albader, S.; Alajlan, N.; Alkhunaini, N.; Niazy, A.; Almahdy, A. Comparison of the antibacterial activity of calcium silicate- and epoxy resin-based endodontic sealers against Enterococcus faecalis biofilms: A confocal laser-scanning microscopy analysis. Odontology 2019, 107, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Zapata, R.O.; Bramante, C.M.; de Moraes, I.G.; Bernardineli, N.; Gasparoto, T.H.; Graeff, M.S.; Campanelli, A.P.; Garcia, R.B. Confocal laser scanning microscopy is appropriate to detect viability of Enterococcus faecalis in infected dentin. J. Endod. 2008, 34, 1198–1201. [Google Scholar] [CrossRef] [PubMed]
- Bitter, K.; Paris, S.; Martus, P.; Schartner, R.; Kielbassa, A.M. A Confocal Laser Scanning Microscope investigation of different dental adhesives bonded to root canal dentine. Int. Endod. J. 2004, 37, 840–848. [Google Scholar] [CrossRef]
- Marciano, M.A.; Guimaraes, B.M.; Ordinola-Zapata, R.; Bramante, C.M.; Cavenago, B.C.; Garcia, R.B.; Bernardineli, N.; Andrade, F.B.; Moraes, I.G.; Duarte, M.A. Physical properties and interfacial adaptation of three epoxy resin-based sealers. J. Endod. 2011, 37, 1417–1421. [Google Scholar] [CrossRef]
- Al-Haddad, A.; Abu Kasim, N.H.; Che Ab Aziz, Z.A. Interfacial adaptation and thickness of bioceramic-based root canal sealers. Dent. Mater. J. 2015, 34, 516–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rached-Junior, F.A.; Sousa-Neto, M.D.; Bruniera, J.F.; Duarte, M.A.; Silva-Sousa, Y.T. Confocal microscopy assessment of filling material remaining on root canal walls after retreatment. Int. Endod. J. 2014, 47, 264–270. [Google Scholar] [CrossRef]
- Mancino, D.; Kharouf, N.; Cabiddu, M.; Bukiet, F.; Haikel, Y. Microscopic and chemical evaluation of the filling quality of five obturation techniques in oval-shaped root canals. Clin. Oral Investig. 2020, 1–9, online ahead of print. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GROUP | GP % (Mean-SD) | Sealer % (Mean-SD) | Voids % (Mean-SD) | GP % (Mean-SD) | Sealer % (Mean-SD) | Voids % (Mean-SD) | GP % (Mean-SD) | Sealer % (Mean-SD) | Voids % (Mean-SD) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Distance from the apex | 3 mm | 3 mm | 3 mm | 6 mm | 6 mm | 6 mm | 9 mm | 9 mm | 9 mm | |
| No Activation | BC | 69.0–12.2 | 29.8–11.5 | 0.5–1.0 | 61.9 14.2 | 35.7–15.1 | 0.6–1.4 | 56.6–12 | 41.9–11.4 | 2.5–3.3 |
| CL | 75.4–16.2 | 23.7–15.2 | 1.5–2.5 | 79.1–11.0 | 18.1–10.3 | 1.4–1.5 | 82.0–10.9 | 15.6–10.0 | 2.6–2.5 | |
| GC | 76.1–33.6 | 23.1–33 | 1.0–1.6 | 88.5–16.7 | 10.3- 15.7 | 0.3–1.0 | 91.5–4.1 | 7.9–3.5 | 0.6–0.8 | |
| GF | 90.7–7.4 | 8.9–7.6 | 0.1–0.2 | 92.5–7.9 | 6.2–5.9 | 0.8–1.9 | 91.7–5.2 | 7.5–5.0 | 1.7–2.7 | |
| TH | 54.4–46.1 | 43.3–43.5 | 2.1–5.3 | 94.3–5.4 | 4.8–5.1 | 0.3–0.6 | 91.9–7.0 | 6.8–6.2 | 1.3–2.0 | |
| Activation | BC | 60.1–12.4 | 39.3–12.1 | 1.2–1.9 | 60.2–12.9 | 39.3–12.7 | 2.5–4.2 | 56.7–11.4 | 40.8–11.9 | 1.5–4.3 |
| CL | 72.1–15.2 | 26.5–14.8 | 0.9–2.3 | 80.6–7.5 | 18.1–7.2 | 2.8–3.3 | 81.7–13.1 | 15.8–11.8 | 2.4–1.8 | |
| GC | 73.0–34.0 | 26–32.7 | 0.8–1.3 | 83.7–27.7 | 16.0–27.0 | 1.2–2.7 | 91.3–4.9 | 8.0–4.8 | 0.5–1.0 | |
| GF | 91.1–7.1 | 8.8–7 | 0.3–0.9 | 92.9–5.4 | 6.3–4.6 | 1.3–2.8 | 91.7–6.8 | 6.6–5.5 | 0.8–1.8 | |
| TH | 77.8–32.1 | 20.2–28.2 | 2.4–4.5 | 94.0–5.5 | 5.7–5.3 | 1.0–1.8 | 92.7–3.9 | 6.0–3.4 | 1.3–1.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Alfayate, R.; Mercade, M.; Algar-Pinilla, J.; Cisneros-Cabello, R.; Foschi, F.; Cohen, S. Root Canal Filling Quality Comparison of a Premixed Calcium Silicate Endodontic Sealer and Different Carrier-Based Obturation Systems. J. Clin. Med. 2021, 10, 1271. https://doi.org/10.3390/jcm10061271
Pérez-Alfayate R, Mercade M, Algar-Pinilla J, Cisneros-Cabello R, Foschi F, Cohen S. Root Canal Filling Quality Comparison of a Premixed Calcium Silicate Endodontic Sealer and Different Carrier-Based Obturation Systems. Journal of Clinical Medicine. 2021; 10(6):1271. https://doi.org/10.3390/jcm10061271
Chicago/Turabian StylePérez-Alfayate, Ruth, Montse Mercade, Juan Algar-Pinilla, Rafael Cisneros-Cabello, Federico Foschi, and Stephen Cohen. 2021. "Root Canal Filling Quality Comparison of a Premixed Calcium Silicate Endodontic Sealer and Different Carrier-Based Obturation Systems" Journal of Clinical Medicine 10, no. 6: 1271. https://doi.org/10.3390/jcm10061271