
A Comparative Study of Biocompatibility in Rat Connective Tissue of a New Mineral Trioxide Compound (Theracal) versus MTA and a Bioactive G3 Glass

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Anaesthesia
2.3. Surgical Protocol
2.4. Sacrifice and Histological Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ozbas, H.; Yaltirik, M.; Bilgic, B.; Issever, H. Reactions of connective tissue to compomers, composite and amalgam root-end filling materials. Int. Endod. J. 2003, 36, 281–287. [Google Scholar] [CrossRef]
- Mohammadi, Z.; Modaresi, J.; Yazdizadeh, M. Evaluation of the antifungal effects of mineral trioxide aggregate materials. Aust. Endod. J. 2006, 32, 120–122. [Google Scholar] [CrossRef]
- Torabinejad, M.; Ford, T.R.P.; McKendry, D.J.; Abedi, H.R.; Miller, D.A.; Kariyawasam, S.P. Histologic assessment of mineral trioxide aggregate as a root-end filling in monkeys. J. Endod. 1997, 23, 225–228. [Google Scholar] [CrossRef]
- Torabinejad, M.; Ford, T.R.P.; Abedi, H.R.; Kariyawasam, S.P.; Tang, H.-M. Tissue reaction to implanted root-end filling materials in the tibia and mandible of guinea pigs. J. Endod. 1998, 24, 468–471. [Google Scholar] [CrossRef]
- Shahi, S.; Rahimi, S.; Lotfi, M.; Yavari, H.; Gaderian, A. A Comparative Study of the Biocompatibility of Three Root-end Filling Materials in Rat Connective Tissue. J. Endod. 2006, 32, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Yaltirik, M.; Ozbas, H.; Bilgic, B.; Issever, H. Reactions of Connective Tissue to Mineral Trioxide Aggregate and Amalgam. J. Endod. 2004, 30, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Holland, R.; de Souza, V.; Nery, M.J.; Filho, J.A.O.; Bernabé, P.F.; Dezan, E. Reaction of rat connective tissue to implanted dentin tubes filled with mineral trioxide aggregate or calcium hydroxide. J. Endod. 1999, 25, 161–166. [Google Scholar] [CrossRef]
- Abedi, H.R.; Ingle, J. Mineral trioxide aggregate: A review of a new cement. J. Calif. Dent. Assoc. 1995, 23, 39. [Google Scholar]
- Economides, N.; Pantelidou, O.; Kokkas, A.; Tziafas, D. Short-term periradicular tissue response to mineral trioxide aggregate (MTA) as root-end filling material. Int. Endod. J. 2003, 36, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Thomson, T.S.; Berry, J.; Somerman, M.J.; Kirkwood, K.L. Cementoblasts Maintain Expression of Osteocalcin in the Presence of Mineral Trioxide Aggregate. J. Endod. 2003, 29, 407–412. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Siboni, F.; Prati, C. Chemical-physical properties of TheraCal, a novel light-curable MTA-like material for pulp capping. Int. Endod. J. 2012, 45, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Suh, B.; Cannon, M.; Martín, D. Polymerizable Dental Pulp Healing, Capping and Lining Material and Method for Use. U.S. Patent Application No. 12/034,093, 25 December 2008. [Google Scholar]
- Lee, B.N.; Lee, B.G.; Chang, H.S.; Hwang, Y.C.; Hwang, I.N.; Oh, W.M. Effects of a novel light-curable material on odontoblastic differentiation of human dental pulp cells. Int. Endod. J. 2017, 50, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Shin, Y.; Kim, S.O.; Lee, H.-S.; Choi, H.-J.; Song, J.S. Comparative Study of Pulpal Responses to Pulpotomy with ProRoot MTA, RetroMTA, and TheraCal in Dogs’ Teeth. J. Endod. 2015, 41, 1317–1324. [Google Scholar] [CrossRef]
- Camilleri, J.; Laurent, P.; About, I. Hydration of biodentine, theracal LC, and a prototype tricalcium silicate-based dentin replacement material after pulp capping in entire tooth cultures. J. Endod. 2014, 40, 1846–1854. [Google Scholar] [CrossRef]
- Camilleri, J. Hydration characteristics of Biodentine and Theracal used as pulp capping materials. Dent. Mater. 2014, 30, 709–715. [Google Scholar] [CrossRef]
- Al-Hyali, N.A. Comparison among Pulp Capping Materials in Calcium Ion Release, pH Change, Solubility and Water Sorption: An In Vitro Study. J. Baghdad Coll. Dent. 2017, 29, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Demirkaya, K.; Can Demirdöğen, B.; Öncel Torun, Z.; Erdem, O.; Çetinkaya, S.; Akay, C. In vivo evaluation of the effects of hydraulic calcium silicate dental cements on plasma and liver aluminium levels in rats. Eur. J. Oral Sci. 2016, 124, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Cannon, M.; Gerodias, N.; Vieira, A.; Percinoto, C.; Jurado, R. Primate Pulpal Healing after Exposure and TheraCal Application. J. Clin. Pediatr. Dent. 2014, 38, 333–337. [Google Scholar] [CrossRef] [PubMed]
- López-Píriz, R.; Solá-Linares, E.; Rodriguez-Portugal, M.; Malpica, B.; Díaz-Güemes, I.; Enciso, S.; Esteban-Tejeda, L.; Cabal, B.; Granizo, J.J.; Moya, J.S.; et al. Evaluation in a dog model of three antimicrobial glassy coatings: Prevention of bone loss around implants and microbial assessments. PLoS ONE 2015, 10, e0140374. [Google Scholar] [CrossRef]
- Moya, J.S.; Martínez, A.; López-Píriz, R.; Guitián, F.; Díaz, L.A.; Esteban-Tejeda, L.; Cabal, B.; Sket, F.; Fernández-García, E.; Tomsia, A.P.; et al. Histological response of soda-lime glass-ceramic bactericidal rods implanted in the jaws of beagle dogs. Sci. Rep. 2016, 6, 31478. [Google Scholar] [CrossRef]
- Martínez Lalis, R.; Esaín, M.L.; Kokubu, G.A.; Willis, J.; Chaves, C.; Grana, D.R. Rat subcutaneous tissue response to modified Portland cement, a new mineral trioxide aggregate. Braz. Dent. J. 2009, 20, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Bramante, C.; Kato, M.M.; Assis, G.; Duarte, M.A.H.; Bernardineli, N.; De Moraes, I.G.; Garcia, R.B.; Ordinola-Zapata, R.; Bramante, A.S. Biocompatibility and setting time of CPM-MTA and white Portland cement clinker with or without calcium sulfate. J. Appl. Oral Sci. 2013, 21, 32–36. [Google Scholar] [CrossRef] [Green Version]
- Sumer, M.; Muglali, M.; Bodrumlu, E.; Guvenc, T. Reactions of Connective Tissue to Amalgam, Intermediate Restorative Material, Mineral Trioxide Aggregate, and Mineral Trioxide Aggregate Mixed With Chlorhexidine. J. Endod. 2006, 32, 1094–1096. [Google Scholar] [CrossRef]
- Close, B.; Banister, K.; Baumans, V.; Bernoth, E.M.; Bromage, N.; Erhardt, W.; Bunyan, J.; Flecknell, P.; Gregory, N.; Hackbarth, H.; et al. Recommendations for euthanasia of experimental animals: Part 2. Lab. Anim. 1997, 31, 1–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taha, N.A.; Safadi, R.A.; Alwedaie, M.S. Biocompatibility Evaluation of EndoSequence Root Repair Paste in the Connective Tissue of Rats. J. Endod. 2016, 42, 1523–1528. [Google Scholar] [CrossRef]
- Parirokh, M.; Torabinejad, M. Mineral Trioxide Aggregate: A Comprehensive Literature Review-Part III: Clinical Applications, Drawbacks, and Mechanism of Action. J. Endod. 2010, 36, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Koh, E.; Torabinejad, M.; Pitt Ford, T.; Brady, K.; McDonald, F. Mineral trioxide aggregate stimulates a biological response in human osteoblasts. J. Biomed. Mater. Res. 1997, 37, 432–439. [Google Scholar] [CrossRef]
- Oliveira, M.; Xavier, C.; Demarco, F.; Pinheiro, A.; Costa, A.; Pozza, D. Comparative chemical study of MTA and Portland cements. Braz. Dent. J. 2007, 18, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Parirokh, M.; Mirsoltani, B.; Raoof, M.; Tabrizchi, H.; Haghdoost, A. Comparative study of subcutaneous tissue responses to a novel root-end filling material and white and grey mineral trioxide aggregate. Int. Endod. J. 2010, 44, 283–289. [Google Scholar] [CrossRef]
- Moretton, T.R.; Brown, C.E.; Legan, J.J.; Kafrawy, A.H. Tissue reactions after subcutaneous and intraosseous implantation of mineral trioxide aggregate and ethoxybenzoic acid cement. J. Biomed. Mater. Res. 2000, 52, 528–533. [Google Scholar] [CrossRef]
- Aguilar, F.G.; Garcia, L.F.R.; Pires-de-Souza, F.C.P. Biocompatibility of New Calcium Aluminate Cement (EndoBinder). J. Endod. 2012, 38, 367–371. [Google Scholar] [CrossRef]
- Poggio, C.; Arciola, C.R.; Beltrami, R.; Monaco, A.; Dagna, A.; Lombardini, M.; Visai, L. Cytocompatibility and Antibacterial Properties of Capping Materials. Sci. World J. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Torneck, C.; Moe, H.; Howley, T. The effect of calcium hydroxide on porcine pulp fibroblasts in vitro. J. Endod. 1983, 9, 131–136. [Google Scholar] [CrossRef]
- Abedi-Amin, A.; Luzi, A.; Giovarruscio, M.; Paolone, G.; Darvizeh, A.; Agullo, V.V.; Sauro, S. Innovative root-end filling materials based on calcium-silicates and calcium-phosphates. J. Mater. Sci. Mater. Med. 2017, 28, 31. [Google Scholar] [CrossRef] [PubMed]
- Hinata, G.; Yoshiba, K.; Han, L.; Edanami, N.; Yoshiba, N.; Okiji, T. Bioactivity and biomineralization ability of calcium silicate-based pulp-capping materials after subcutaneous implantation. Int. Endod. J. 2017, 50, e40–e51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okiji, T.; Yoshiba, K. Reparative Dentinogenesis Induced by Mineral Trioxide Aggregate: A Review from the Biological and Physicochemical Points of View. Int. J. Dent. 2009, 2009, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Watts, A.; Paterson, R.C. Initial biological testing of root canal sealing materials—A critical review. J. Dent. 1992, 20, 259–265. [Google Scholar] [CrossRef]
- Stanford, J.W. Recommended standard practices for biological evaluation of dental materials. Federation Dentaire International, Commission of Dental Materials, Instruments, Equipment and Therapeutics. Int. Dent. J. 1980, 30, 140–188. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | |||||||
|---|---|---|---|---|---|---|---|
| Appearance | Category | Value 0 | Value 1 | Value 2 | Value 3 | Value 4 | Value 5 |
| Inflammation | Kind | Absence of both types (Acute and chronic) | Chronicle | Sharp | Both types | ||
| Intensity (concentration of inflammatory cells per field ×40) | Inflammatory cells are not detected | Less than 25 cells (rare) | Between 25 and 50 cells (mild) | Between 50 and 75 cells (moderate) | More than 75 cells (severe) | ||
| Extension | Inflammatory cells are not detected | Inflammatory cells are located in the superficial layer of the capsule | Inflammatory cells located within the limits of the capsule | Inflammatory cells beyond the capsule | There is no encapsulation. Cells are limited to the contact area | There is no encapsulation. Inflammatory cells spread outside the contact area | |
| Fibroblastic reaction | Connective tissue capsule | Absent | Immature form | Mature, thin form (<150 µm) | Mature, coarse form (≥150 µm) | ||
| Foreign body reaction | Giant cells or foreign body eosinophils | Absence | Presence | ||||
| Capillary reaction | Congestion in blood vessels | Absence | Presence | ||||
| Tissue edema | Absence | Limited areas of tissue edema | Widespread areas of tissue edema | ||||
| Calcification | Absence | Presence | |||||
| Necrosis | Absence | Presence | |||||
| PARAMETER | MATERIAL | DAY 15 | DAY 30 | DAY 45 | p |
|---|---|---|---|---|---|
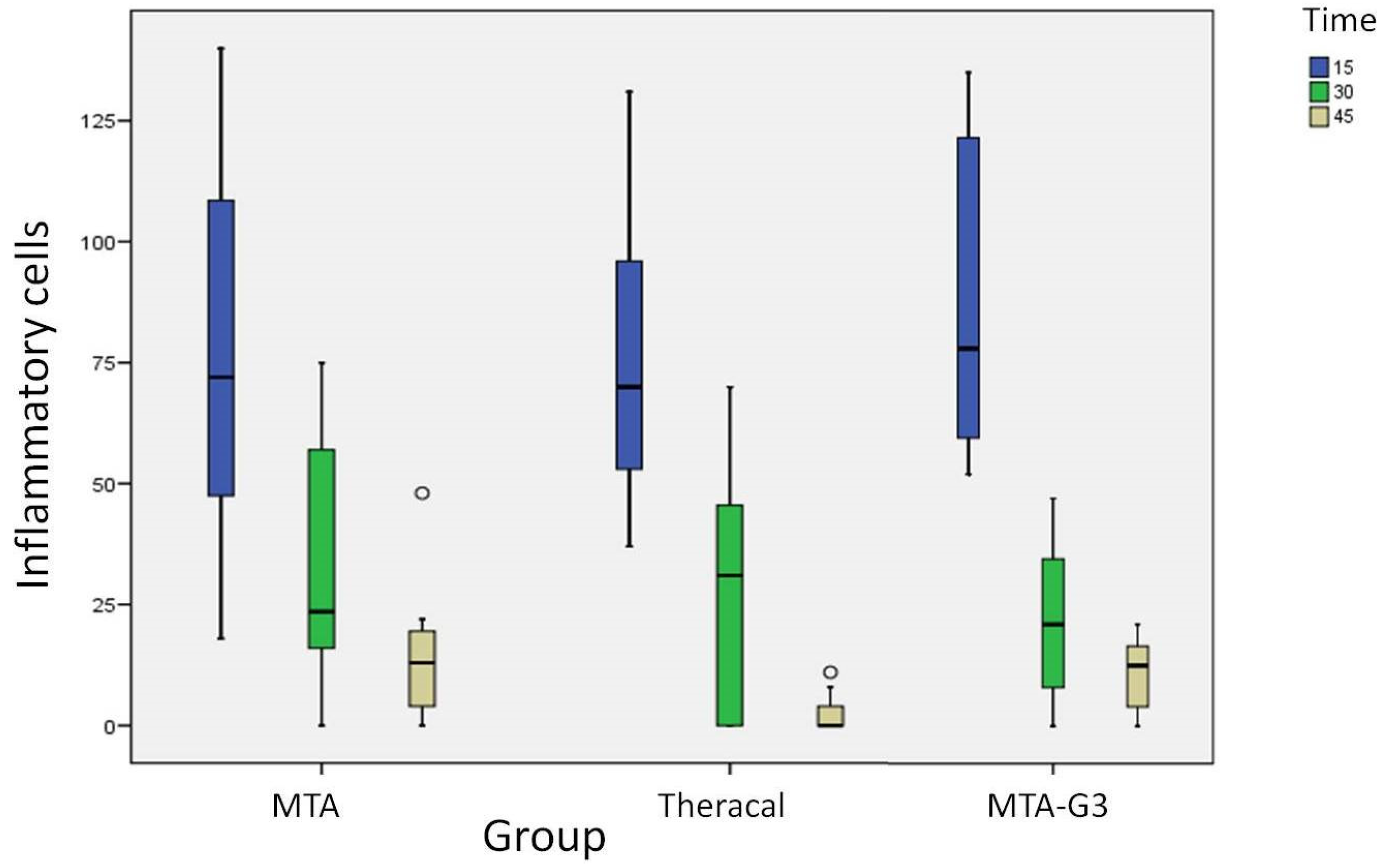
| Number of inflammatory cells Md(RIQ) | MTA | 72 (74.5) | 23.5 (47.5) | 13 (18.75) | 0.004 * |
| MTA-G3 | 78 (70.5) | 21 (35.75) | 12.5 (15.25) | <0.001 * | |
| THER. | 70 (58) | 31 (46.75) | 0 (6) | 0.001 * |
| PARAMETER | DAYS | MTA | THER. | MTA-G3 | p |
|---|---|---|---|---|---|
| Number of inflammatory cells Md(RIQ) | 15 | 72 (74.5) | 70 (58) | 78 (70.5) | 0.916 * |
| 30 | 23, 5 (47.5) | 31 (46.75) | 21 (35.75) | 0.711 * | |
| 45 | 13 (18.75) | 0 (6) | 12.5 (15.25) | 0.021 * |
| PARAMETER | GRADE | MTA | THER. | MTA-G3 | Control | p |
|---|---|---|---|---|---|---|
| Type of inflammation n(%) | Absence | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - |
| Chronic | 8 (100) | 8 (100) | 8 (100) | 8 (100) | ||
| Intensity n(%) | Limited | 1 (12.5) | 0 (0) | 0 (0) | 0 (0) | |
| Mild | 1 (12.5) | 2 (25) | 0 (0) | 0 (0) | 0.551 * | |
| Moderate | 3 (37.5) | 4 (50) | 4 (50) | 5 (62.5) | ||
| Severe | 3 (37.5) | 2 (25) | 4 (50) | 3 (37.5) | ||
| Number of inflammatory cells Md(RIQ) | 72 (74.5) | 70 (58) | 78 (70.50) | 74.5 (58.75) | 0.938 ** | |
| Extension n(%) | Not detected | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| On capsule surface | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Inside the capsule | 5 (62.5) | 2 (25) | 0 (0) | 3 (37.5) | ||
| Beyond the capsule | 3 (37.5) | 3 (37.5) | 6 (75) | 5 (62.5) | 0.058 * | |
| In contact area | 0 (0) | 3 (37.5) | 2 (25) | 0 (0) | ||
| Extended | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Capsule n(%) | Absence | 0 (0) | 1 (12.5) | 2 (25) | 0 (0) | |
| Immature | 3 (37.5) | 7 (87.5) | 3 (37.5) | 5 (62.5) | 0.123 * | |
| Fine | 3 (37.5) | 0 (0) | 1 (12.5) | 3 (37.5) | ||
| Thick | 2 (25) | 0 (0) | 2(25) | 0 (0) | ||
| Capsule thickness Md(RIQ) | 128 (188.5) | 0 (0) | 241 (58) | 83 (87) | 0.212 ** | |
| Strange body n(%) | Yes | 4 (50) | 4 (50) | 5 (62.5) | 2 (25) | 0.497 * |
| No | 4 (50) | 4 (50) | 3 (37.5) | 6 (75) | ||
| Calcification n(%) | Yes | 5 (62.5) | 5 (62.5) | 7 (87.5) | 0 (0) | 0.004 * |
| No | 3 (37.5) | 3 (37.5) | 1 (12.5) | 8 (100) | ||
| Congestion n(%) | Yes | 1 (12.5) | 2 (25) | 1 (12.5) | 2 (25) | 0.845 * |
| No | 7 (87.5) | 6 (75) | 7 (87.5) | 6 (75) | ||
| Edema n(%) | Yes | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - |
| No | 8 (100) | 8 (100) | 8 (100) | 8 (100) | ||
| Necrosis n(%) | Yes | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - |
| No | 8 (100) | 8 (100) | 8 (100) | 8 (100) |
| PARAMETER | GRADE | MTA | THER. | MTA-G3 | Control | p |
|---|---|---|---|---|---|---|
| Type of inflammation n(%) | Absence | 1 (12.5) | 3 (37.5) | 2 (25) | 2 (25) | 0.612 |
| Chronic | 7 (87.5) | 5 (62.5) | 6 (75) | 6 (75) | ||
| Intensity n(%) | Limited | 1 (12.5) | 3 (37.5) | 2 (25) | 2 (25) | |
| Mild | 4 (50) | 1 (12.5) | 4 (50) | 4 (50) | 0.532 * | |
| Moderate | 1 (12.5) | 3 (37.5) | 2 (25) | 2 (25) | ||
| Severe | 2 (25) | 1 (12.5) | 0 (0) | 0 (0) | ||
| Number of inflammatory cells Md(RIQ) | 23.5 (47.5) | 31 (46.75) | 21 (35.75) | 38.50 (58) | 0.620 ** | |
| Extension n(%) | Not detected | 1 (12.5) | 3 (37.5) | 2 (25) | 2 (25) | |
| On capsule surface | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Inside the capsule | 5 (62.5) | 1 (12.5) | 6 (75) | 3 (37.5) | ||
| Beyond the capsule | 1 (12.5) | 4 (50) | 0 (0) | 3 (37.5) | 0.166 * | |
| In contact area | 1 (12.5) | 0 (0) | 0 (0) | 0 (0) | ||
| Extended | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Capsule n(%) | Absence | 2 (25) | 0 (0) | 2 (25) | 0 (0) | |
| Immature | 2 (25) | 0 (0) | 0 (0) | 0 (0) | 0.016 * | |
| Fine | 0 (0) | 7 (87.5) | 4 (50) | 7 (87.5) | ||
| Thick | 4 (50) | 1 (12.5) | 2 (25) | 1 (12.5) | ||
| Capsule thickness Md(RIQ) | 187 (32.25) | 93 (40.75) | 120.5 (162.5) | 68 (81.5) | 0.047 ** | |
| Strange body n(%) | Yes | 0 (0) | 1 (12.5) | 1 (12.5) | 1 (12.5) | 0.545 * |
| No | 8 (100) | 7 (87.5) | 7 (87.5) | 7 (87.5) | ||
| Calcification n(%) | Yes | 8 (100) | 2 (37.5) | 2 (37.5) | 0 (0) | <0.001 * |
| No | 0 (0) | 6 (75) | 6 (75) | 8 (100) | ||
| Congestion n(%) | Yes | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - |
| No | 8 (100) | 8 (100) | 8 (100) | 8 (100) | ||
| Edema n(%) | Yes | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - |
| No | 8 (100) | 8 (100) | 8 (100) | 8 (100) | ||
| Necrosis n(%) | Yes | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - |
| No | 8 (100) | 8 (100) | 8 (100) | 8 (100) |
| PARAMETER | GRADE | MTA | THER. | MTA-G3 | Control | p |
|---|---|---|---|---|---|---|
| Type of inflammation | Absence | 2 (25) | 6 (75) | 2 (25) | 3 (37.5) | 0.188 * |
| n(%) | Chronic | 6 (75) | 2 (25) | 6 (75) | 5 (62.5) | |
| Absence cells | 2 (25) | 6 (75) | 2 (12.5) | 3 (37.5) | ||
| Intensity | Limited | 5 (62.5) | 2 (25) | 6 (75) | 4 (50) | |
| n(%) | Mild | 1 (12.5) | 0 (0) | 0 (0) | 0 (0) | 0.251 * |
| Moderate | 0 (0) | 0 (0) | 0 (0) | 1 (12.5) | ||
| Severe | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Number of inflammatory cells Md(RIQ) | 13 (18.75) | 0 (6) | 12.5 (15.25) | 12 (19.5) | 0.081 ** | |
| Extension n(%) | Not detected | 2 (25) | 6 (75) | 1 (12.5) | 3 (37.5) | |
| On capsule surface | 0 (0) | 0 (0) | 1 (12.5) | 0 (0) | ||
| Inside the capsule | 4 (50) | 2 (25) | 1 (12.5) | 4 (50) | ||
| Beyond the capsule | 1 (12.5) | 0 (0) | 3 (37.5) | 0 (0) | 0.125 * | |
| In contact area | 1 (12.5) | 0 (0) | 1 (12.5) | 1 (12.5) | ||
| Extended | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Capsule n(%) | Absence | 2 (25) | 0 (0) | 1 (12.5) | ||
| Immature | 0 (0) | 0 (0) | 0 (0) | 0.274 * | ||
| Fine | 4 (50) | 8 (100) | 2 (25) | 7 (87.5) | ||
| Thick | 2 (25) | 0 (0) | 0 (0) | 0 (0) | ||
| Capsule thickness Md(RIQ) | 101.5 (92.25) | 93 (65.25) | 82 (58.25) | 43 (18) | 0.003 ** | |
| Strange body | Yes | 0 (0) | 0 (0) | 0 (0) | 1 (12.5) | 0.396 * |
| n(%) | No | 8 (100) | 8 (100) | 8 (100) | 7 (87.5) | |
| Calcification | Yes | 5 (62.5) | 2 (37.5) | 2 (37.5) | 0 (0) | 0.048 * |
| n(%) | No | 3 (37.5) | 6 (75) | 6 (75) | 8 (100) | |
| Congestion | Yes | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - |
| n(%) | No | 8 (100) | 8 (100) | 8 (100) | 8 (100) | |
| Edema | Yes | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - |
| n(%) | No | 8 (100) | 8 (100) | 8 (100) | 8 (100) | |
| Necrosis | Yes | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - |
| n(%) | No | 8 (100) | 8 (100) | 8 (100) | 8 (100) |
| PARAMETER | GRADE | MTA | THER. | MTA-G3 |
|---|---|---|---|---|
| Calcification | Yes | 18 (75) | 9 (37.5) | 11 (45.8) |
| n (%) | No | 6 (25) | 15 (62.5) | 13 (54.2) |
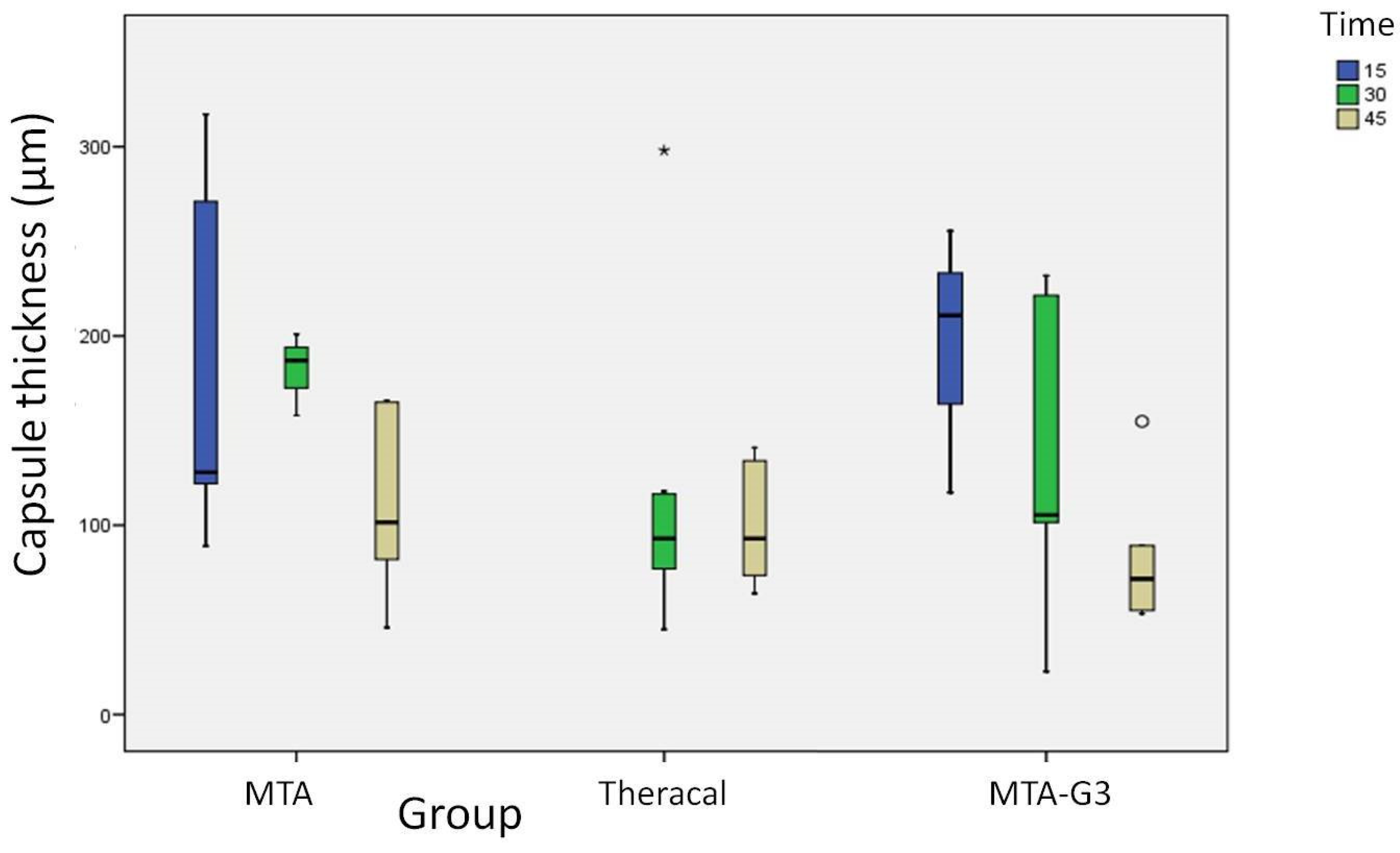
| PARAMETER | MATERIAL | DAY 15 | DAY 30 | DAY 45 | p |
|---|---|---|---|---|---|
| Thickness (µm) Md(RIQ) | MTA | 128 (188.5) | 187 (32.25) | 101.5 (92.25) | 0.08 * |
| THER. | 93 (40.75) | 93 (65.25) | 0.834 ** | ||
| MTA-G3 | 241 (158) | 120.5 (162.5) | 82 (58.25) | 0.068 * |
| PARAMETER | DAYS | MTA | THER. | MTA-G3 |
|---|---|---|---|---|
| Thickness (µm) Md(RIQ) | 15 | 128 (188.5) | 241 (158) | |
| 30 | 187 (32.25) | 93 (40.75) | 120.5 (162.5) | |
| 45 | 101.5 (92.25) | 93 (65.25) | 82 (58.25) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mena-Álvarez, J.; Rico-Romano, C.; Gutiérrez-Ortega, C.; Arias-Sanz, P.; Castro-Urda, J. A Comparative Study of Biocompatibility in Rat Connective Tissue of a New Mineral Trioxide Compound (Theracal) versus MTA and a Bioactive G3 Glass. J. Clin. Med. 2021, 10, 2536. https://doi.org/10.3390/jcm10122536
Mena-Álvarez J, Rico-Romano C, Gutiérrez-Ortega C, Arias-Sanz P, Castro-Urda J. A Comparative Study of Biocompatibility in Rat Connective Tissue of a New Mineral Trioxide Compound (Theracal) versus MTA and a Bioactive G3 Glass. Journal of Clinical Medicine. 2021; 10(12):2536. https://doi.org/10.3390/jcm10122536
Chicago/Turabian StyleMena-Álvarez, Jesús, Cristina Rico-Romano, Carlos Gutiérrez-Ortega, Pablo Arias-Sanz, and Javier Castro-Urda. 2021. "A Comparative Study of Biocompatibility in Rat Connective Tissue of a New Mineral Trioxide Compound (Theracal) versus MTA and a Bioactive G3 Glass" Journal of Clinical Medicine 10, no. 12: 2536. https://doi.org/10.3390/jcm10122536