
Efficacy of Removing Thermafil and GuttaCore from Straight Root Canal Systems Using a Novel Non-Surgical Root Canal Re-Treatment System: A Micro-Computed Tomography Analysis

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Experimental Procedure
2.3. Micro-CT Scanning
2.4. Measurement Procedure
2.5. Statistical Tests
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mareschi, P.; Taschieri, S.; Corbella, S. Long-Term Follow-Up of Nonsurgical Endodontic Treatments Performed by One Spe-cialist: A Retrospective Cohort Study about Tooth Survival and Treatment Success. Int. J. Dent. 2020, 2020, 8855612. [Google Scholar] [CrossRef]
- Pontoriero, D.; Grandini, S.; Spagnuolo, G.; Discepoli, N.; Benedicenti, S.; Maccagnola, V.; Mosca, A.; Cagidiaco, E.F.; Ferrari, M. Clinical Outcomes of Endodontic Treatments and Restorations with and without Posts Up to 18 Years. J. Clin. Med. 2021, 10, 908. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr. Aetiology of root canal treatment failure: Why well-treated teeth can fail. Int. Endod. J. 2001, 34, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torabinejad, M.; Corr, R.; Handysides, R.; Shabahang, S. Outcomes of nonsurgical retreatment and endodontic surgery: A sys-tematic review. J. Endod. 2009, 35, 930–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siqueira, J.F., Jr.; Rôças, I.N.; Ricucci, D.; Hülsmann, M. Causes and management of post-treatment apical periodontitis. Br. Dent. J. 2014, 216, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Salehrabi, R.; Rotstein, I. Epidemiologic Evaluation of the Outcomes of Orthograde Endodontic Retreatment. J. Endod. 2010, 36, 790–792. [Google Scholar] [CrossRef]
- Nudera, W.J. Selective Root Retreatment: A Novel Approach. J. Endod. 2015, 41, 1382–1388. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, G.; Patel, S.; Durán-Sindreu, F.; Roig, M.; Abella, F. Influence of Cone-beam Computed Tomography on Endodontic Retreatment Strategies among General Dental Practitioners and Endodontists. J. Endod. 2017, 43, 1433–1437. [Google Scholar] [CrossRef] [PubMed]
- Torabinejad, M.; White, S.N. Endodontic treatment options after unsuccessful initial root canal treatment: Alternatives to single-tooth implants. J. Am. Dent. Assoc. 2016, 147, 214–220. [Google Scholar] [CrossRef]
- Hülsmann, M.; Stotz, S. Efficacy, cleaning ability and safety of different devices for gutta-percha removal in root canal re-treatment. Int. Endod. J. 1997, 30, 227–233. [Google Scholar] [CrossRef]
- Silva, E.J.; Orlowsky, N.B.; Herrera, D.R.; Machado, R.; Krebs, R.L.; Coutinho-Filho Tde, S. Effectiveness of rotatory and reciprocating movements in root canal filling material removal. Braz. Oral Res. 2015, 29, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Rödig, T.; Reicherts, P.; Konietschke, F.; Dullin, C.; Hahn, W.; Hülsmann, M. Efficacy of reciprocating and rotary NiTi instruments for retreatment of curved root canals assessed by micro-CT. Int. Endod. J. 2014, 47, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Zamin, C.; Silva-Sousa, Y.T.C.; Souza-Gabriel, A.E.; Messias, D.F.; Sousa-Neto, M.D. Fracture susceptibility of endodontically treated teeth. Dent. Traumatol. 2011, 28, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Stabholz, A.; Friedman, S. Endodontic retreatment—Case selection and technique. Part 2: Treatment planning for retreatment. J. Endod. 1988, 14, 607–614. [Google Scholar] [CrossRef]
- Marques da Silva, B.; Baratto-Filho, F.; Leonardi, D.P.; Henrique Borges, A.; Volpato, L.; Branco Barletta, F. Effectiveness of ProTa-per, D-RaCe, and Mtwo retreatment files with and without supplementary instruments in the removal of root canal filling material. Int. Endod. J. 2012, 45, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.Y.; Al-Hadlaq, S.M.; Al-Katheeri, N.H. Efficacy of Two Rotary NiTi Instruments in the Removal of Gutta-Percha During Root Canal Retreatment. J. Endod. 2007, 33, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Rossi-Fedele, G.; Ahmed, H.M. Assessment of Root Canal Filling Removal Effectiveness Using Micro-computed Tomogra-phy: A Systematic Review. J Endod. 2017, 43, 520–526. [Google Scholar] [CrossRef]
- Campello, A.F.; Almeida, B.M.; Franzoni, M.A.; Alves, F.R.F.; Marceliano-Alves, M.F.; Rocas, I.N.; Siqueira, J.F., Jr.; Proven-zano, J.C. Influence of solvent and a supplementary step with a finishing instrument on filling material removal from ca-nals connected by an isthmus. Int. Endod. J. 2019, 52, 716–724. [Google Scholar] [CrossRef]
- Kesharani, P.; Kapasi, K.; Kansara, P.; Patil, D.; Kansara, T.; Sheth, S. In vitro comparative evaluation of efficiency of XP-endo shaper, XP-endo finisher, and XP-endo finisher-R files in terms of residual root filling material, preservation of root dentin, and time during retreatment procedures in oval canals—A cone-beam computed tomography analysis. J. Conserv. Dent. 2020, 23, 145–151. [Google Scholar] [CrossRef]
- Fleming, C.H.; Litaker, M.S.; Alley, L.W.; Eleazer, P.D. Comparison of classic endodontic techniques versus contemporary tech-niques on endodontic treatment success. J. Endod. 2010, 36, 414–418. [Google Scholar] [CrossRef]
- Blacher, J.D.; Safavi, K.E.; Aseltine, R.H.; Kaufman, B.M. Defining Endodontic Residents’ Clinical Experiences: A National Survey. J. Dent. Educ. 2019, 83, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Gagliani, M.A.; Cerutti, A.; Bondesan, A.; Colombo, M.; Godio, E.; Giacomelli, G. A 24-month survey on root canal treatment per-formed by NiTi engine driven files and warm gutta-percha filling associated system. Minerva Stomatol. 2004, 53, 543–554. [Google Scholar] [PubMed]
- Gernhardt, C.R.; Krüger, T.; Bekes, K.; Schaller, H.-G. Apical sealing ability of 2 epoxy resin-based sealers used with root canal obturation techniques based on warm gutta-percha compared to cold lateral condensation. Quintessence Int. (Berl. Ger. 1985) 2007, 38, 229–234. [Google Scholar]
- Pirani, C.; Iacono, F.; Gatto, M.R.; FitzGibbon, R.M.; Chersoni, S.; Shemesh, H.; Prati, C. Outcome of secondary root canal treatment filled with Thermafil: A 5-year follow-up of retrospective cohort study. Clin. Oral Investig. 2018, 22, 1363–1373. [Google Scholar] [CrossRef] [PubMed]
- Pirani, C.; Friedman, S.; Gatto, M.R.; Iacono, F.; Tinarelli, V.; Gandolfi, M.G.; Prati, C. Survival and periapical health after root canal treatment with carrier-based root fillings: Five-year retrospective assessment. Int. Endod. J. 2017, 51, e178–e188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirfendereski, M.; Roth, K.; Fan, B.; Dubrowski, A.; Carnahan, H.; Azarpazhooh, A.; Basrani, B.; Torneck, C.D.; Friedman, S. Technique Acquisition in the Use of Two Thermoplasticized Root Filling Methods by Inexperienced Dental Students: A Microcomputed Tomography Analysis. J. Endod. 2009, 35, 1512–1517. [Google Scholar] [CrossRef]
- Baratto Filho, F.; Ferreira, E.L.; Fariniuk, L.F. Efficiency of the 0.04 taper ProFile during the re-treatment of gutta-percha-filled root canals. Int. Endod. J. 2002, 35, 651–654. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, L.R.; Juhlin, J.J. Endodontic retreatment of Thermafil versus laterally condensed gutta-percha. J. Endod. 1994, 20, 115–117. [Google Scholar] [CrossRef]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Roberts, H.W.; Kirkpatrick, T.C.; Bergeron, B.E. Thermal analysis and stability of commercially available endodontic obturation materials. Clin. Oral Investig. 2017, 21, 2589–2602. [Google Scholar] [CrossRef] [PubMed]
- Rödig, T.; Wagner, J.; Wiegand, A.; Rizk, M. Efficacy of the ProTaper retreatment system in removing Thermafil, GuttaCore or vertically compacted gutta-percha from curved root canals assessed by micro-CT. Int. Endod. J. 2018, 51, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Nevares, G.; De Albuquerque, D.S.; Bueno, C.E.D.S.; Cunha, R.S. Is guttacore more easily removed from the root canal than thermafil? An ex-vivo study. J. Can. Dent. Assoc. 2015, 81, f22. [Google Scholar] [PubMed]
- Beasley, R.T.; Williamson, A.E.; Justman, B.C.; Qian, F. Time Required to Remove GuttaCore, Thermafil Plus, and Thermoplasticized Gutta-percha from Moderately Curved Root Canals with ProTaper Files. J. Endod. 2013, 39, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Gergi, R.; Sabbagh, C. Effectiveness of two nickel-titanium rotary instruments and a hand file for removing gutta-percha in severely curved root canals during retreatment: An ex vivo study. Int. Endod. J. 2007, 40, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Schirrmeister, J.F.; Wrbas, K.-T.; Schneider, F.H.; Altenburger, M.J.; Hellwig, E. Effectiveness of a hand file and three nickel-titanium rotary instruments for removing gutta-percha in curved root canals during retreatment. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Zandi, H.; Petronijevic, N.; Mdala, I.; Kristoffersen, A.K.; Enersen, M.; Rôças, I.N.; Siqueira, J.F.; Ørstavik, D. Outcome of Endodontic Retreatment Using 2 Root Canal Irrigants and Influence of Infection on Healing as Determined by a Molecular Method: A Randomized Clinical Trial. J. Endod. 2019, 45, 1089–1098.e5. [Google Scholar] [CrossRef]
- Takahashi, C.M.; Cunha, R.S.; de Martin, A.S.; Fontana, C.E.; Silveira, C.F.; da Silveira Bueno, C.E. In vitro evaluation of the effec-tiveness of ProTaper universal rotary retreatment system for gutta-percha removal with or without a solvent. J. Endod. 2009, 35, 1580–1583. [Google Scholar] [CrossRef] [PubMed]
- Solda, C.; Padoim, K.; Rigo, L.; Silva Sousa, Y.T.C.; Hartmann, M.S.M. Assessment of Apical Extrusion using Rotary and Recipro-cating Systems during Root Canal Retreatment. J. Contemp. Dent. Pract. 2020, 21, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Fracchia, D.E.; Amaroli, A.; De Angelis, N.; Signore, A.; Parker, S.; Benedicenti, S.; Polesel, A. GuttaCore Pink, Thermafil and Warm Vertically compacted gutta-percha retreatment: Time required and quantitative evaluation by using ProTaper files. Dent. Mater. J. 2020, 39, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Sae-Lim, V.; Rajamanickam, I.; Lim, B.K.; Lee, H.L. Effectiveness of ProFile.04 taper rotary instruments in endodontic retreatment. J. Endod. 2000, 26, 100–104. [Google Scholar] [CrossRef] [Green Version]
- Kfir, A.; Tsesis, I.; Yakirevich, E.; Matalon, S.; Abramovitz, I. The efficacy of five techniques for removing root filling material: Microscopic versus radiographic evaluation. Int. Endod. J. 2011, 45, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Shen, Y.; Haapasalo, M. Root Canal Wall Dentin Structure in Uninstrumented but Cleaned Human Premolars: A Scanning Electron Microscopic Study. J. Endod. 2018, 44, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Fariniuk, L.F.; Azevedo, M.A.D.; Carneiro, E.; Westphalen, V.P.D.; Piasecki, L.; Neto, U.X.D.S. Efficacy of protaper instruments during endodontic retreatment. Indian J. Dent. Res. 2017, 28, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Dhaimy, S.; Kim, H.-C.; Bedida, L.; Benkiran, I. Efficacy of reciprocating and rotary retreatment nickel-titanium file systems for removing filling materials with a complementary cleaning method in oval canals. Restor. Dent. Endod. 2021, 46, 13. [Google Scholar] [CrossRef] [PubMed]
- Pirani, C.; Pelliccioni, G.A.; Marchionni, S.; Montebugnoli, L.; Piana, G.; Prati, C. Effectiveness of three different retreatment tech-niques in canals filled with compacted gutta-percha or Thermafil: A scanning electron microscope study. J. Endod. 2009, 35, 1433–1440. [Google Scholar] [CrossRef] [PubMed]
- Versiani, M.A.; Ordinola-Zapata, R.; Keleş, A.; Alcin, H.; Bramante, C.M.; Pécora, J.D.; Sousa-Neto, M.D. Middle mesial canals in mandibular first molars: A micro-CT study in different populations. Arch. Oral Biol. 2016, 61, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Crozeta, B.M.; Silva-Sousa, Y.T.C.; Leoni, G.B.; Mazzi-Chaves, J.F.; Fantinato, T.; Baratto-Filho, F.; Sousa-Neto, M.D. Micro–Computed Tomography Study of Filling Material Removal from Oval-shaped Canals by Using Rotary, Reciprocating, and Adaptive Motion Systems. J. Endod. 2016, 42, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.J.N.L.; Belladonna, F.G.; Zuolo, A.S.; Rodrigues, E.; Ehrhardt, I.C.; Souza, E.M.; De-Deus, G. Effectiveness of XP-endo Finisher and XP-endo Finisher R in removing root filling remnants: A micro-CT study. Int. Endod. J. 2018, 51, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Alves, F.R.; Marceliano-Alves, M.F.; Sousa, J.C.N.; Silveira, S.B.; Provenzano, J.C.; Siqueira, J.F. Removal of Root Canal Fillings in Curved Canals Using Either Reciprocating Single- or Rotary Multi-instrument Systems and a Supplementary Step with the XP-Endo Finisher. J. Endod. 2016, 42, 1114–1119. [Google Scholar] [CrossRef]
- Aksel, H.; Eren, S.K.; Örs, S.A.; Serper, A.; Ocak, M.; Çelik, H.H. Micro-CT evaluation of the removal of root fillings using the ProTaper Universal Retreatment system supplemented by the XP-Endo Finisher file. Int. Endod. J. 2019, 52, 1070–1076. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
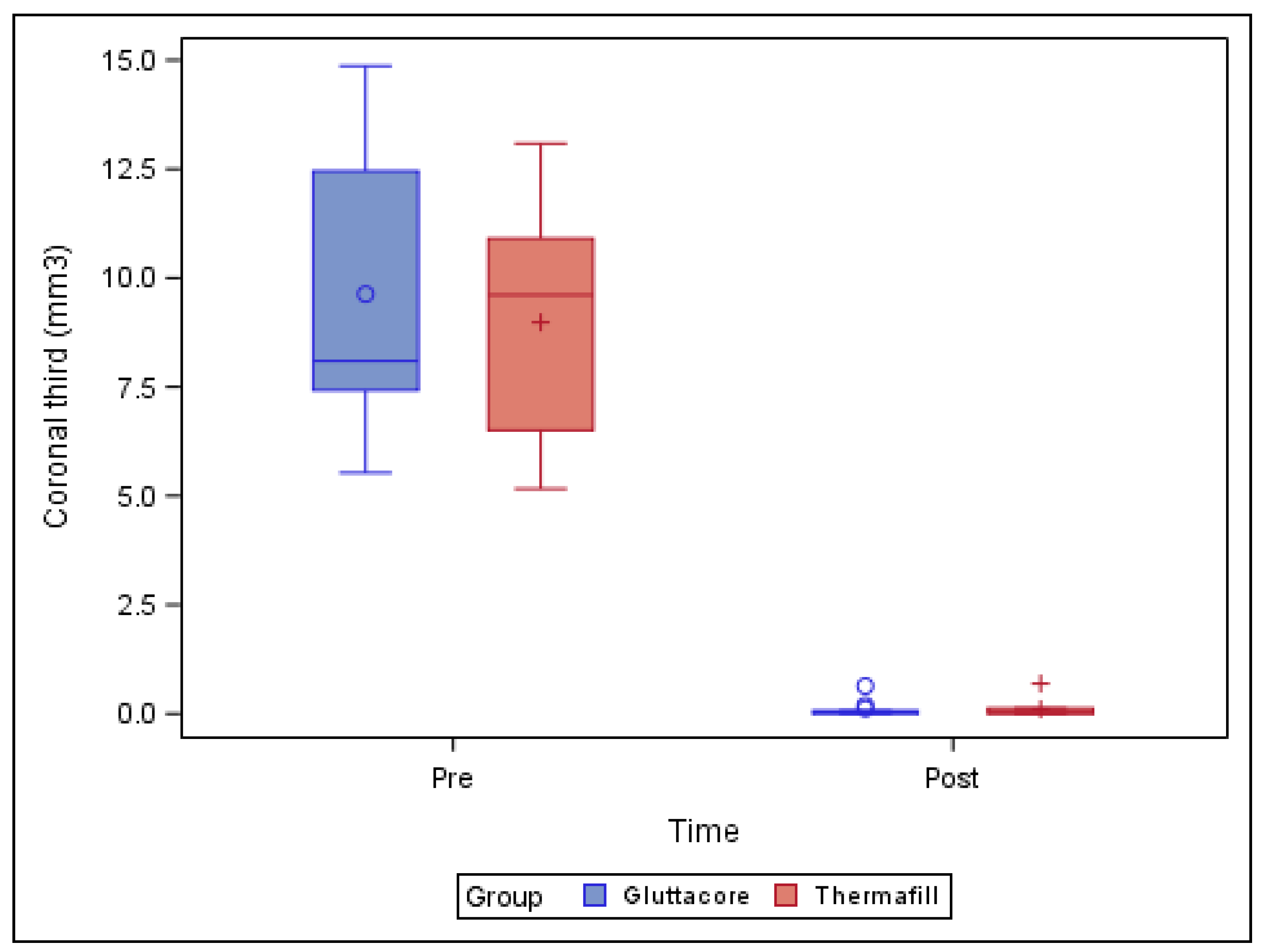
| Study Group | Time | n | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| GuttaCore | Pre-operative | 10 | 9.63 a | 3.16 | 5.53 | 14.87 |
| Post-operative | 9 | 0.12 a | 0.20 | 0.00 | 0.64 | |
| Thermafil | Pre-operative | 10 | 8.98 a | 2.55 | 5.16 | 13.09 |
| Post-operative | 10 | 0.11 a | 0.21 | 0.00 | 00.69 |
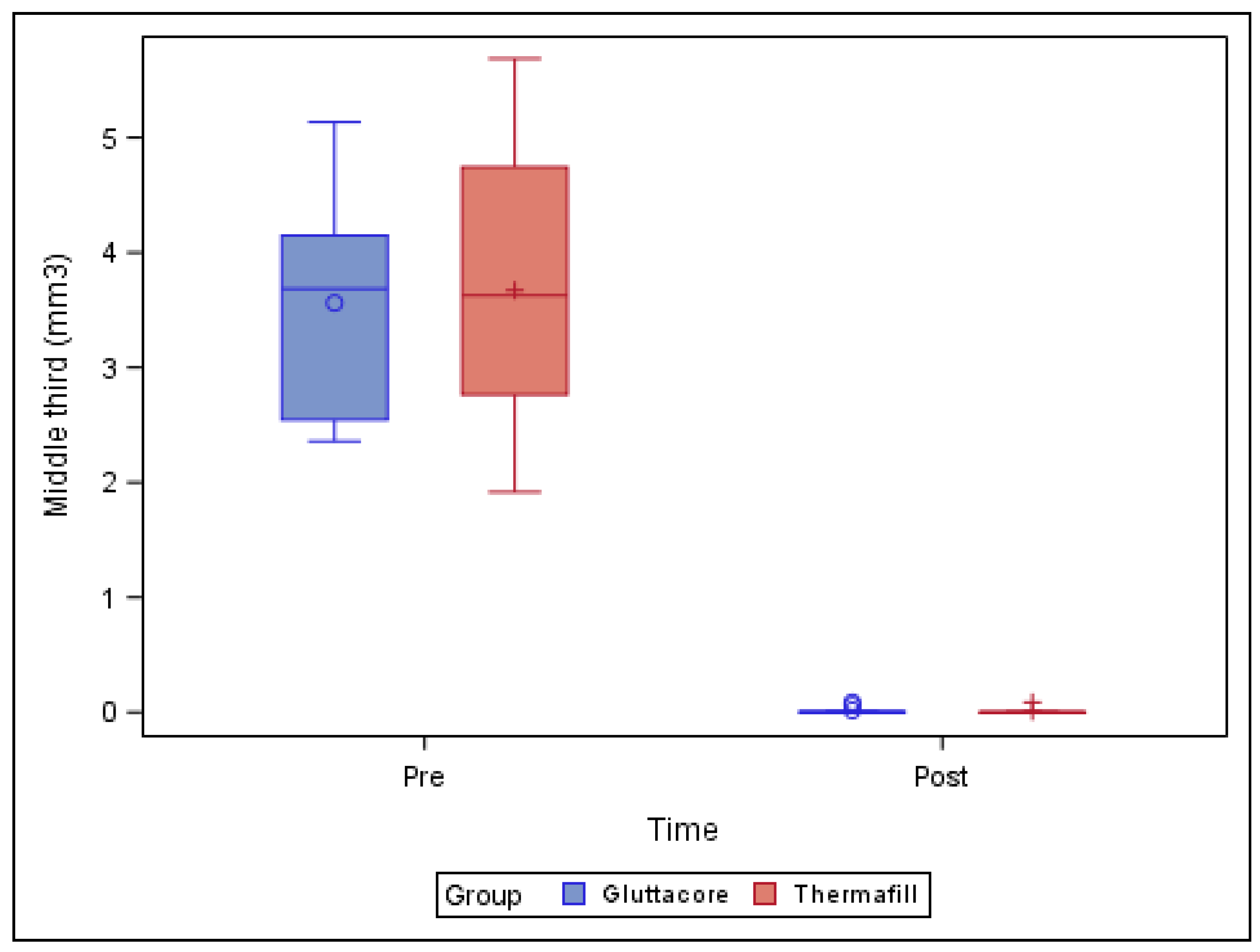
| Study Group | Time | n | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| GuttaCore | Pre-operative | 10 | 3.56 a | 0.94 | 2.36 | 5.14 |
| Post-operative | 9 | 0.02 a | 0.03 | 0.00 | 0.09 | |
| Thermafil | Pre-operative | 10 | 3.67 a | 1.20 | 1.92 | 5.69 |
| Post-operative | 10 | 0.01 a | 0.03 | 0.00 | 0.09 |
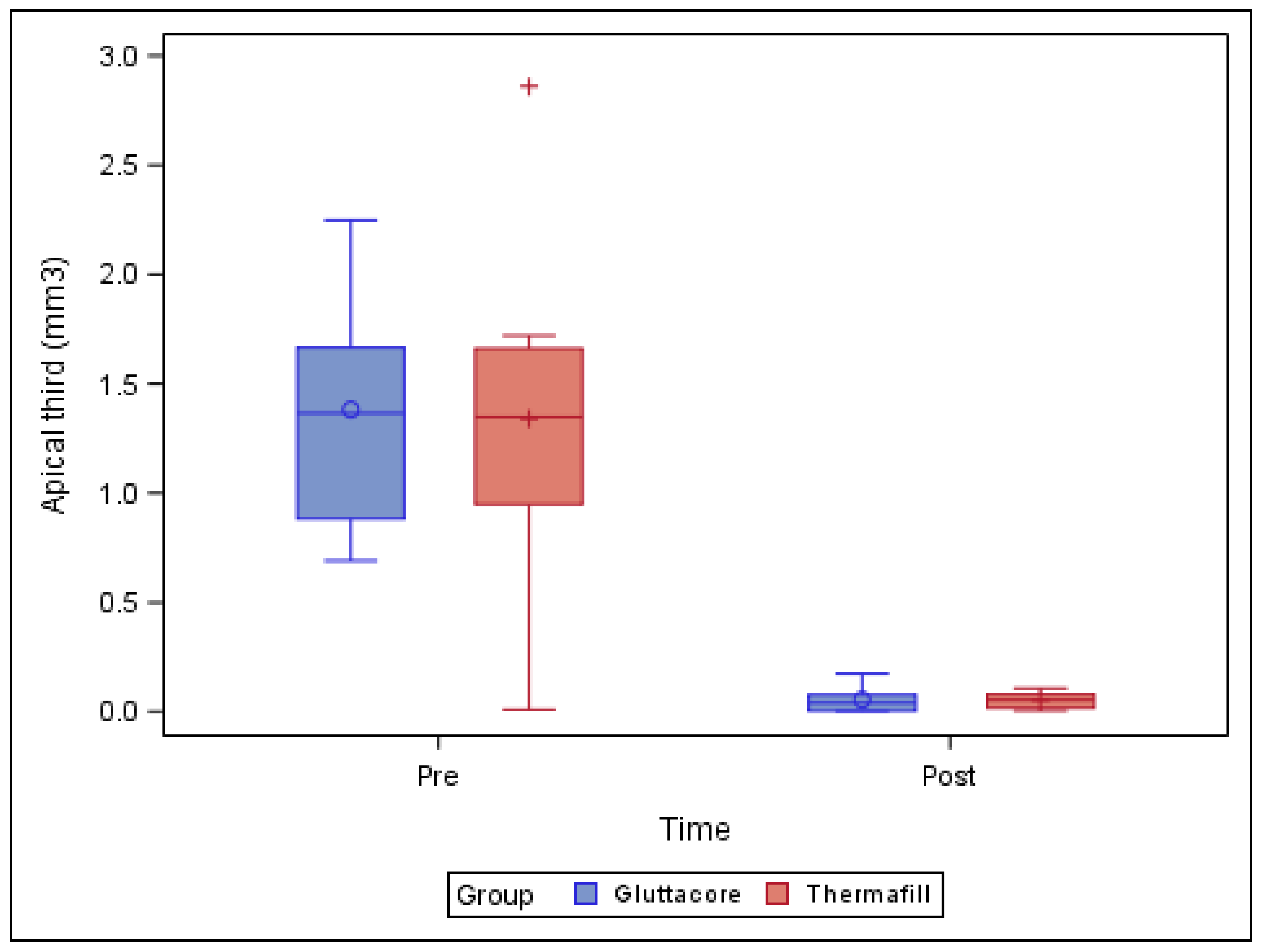
| Study Group | Time | n | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| GuttaCore | Pre-operative | 10 | 1.38 a | 0.52 | 0.69 | 2.25 |
| Post-operative | 9 | 0.06 a | 0.06 | 0.00 | 0.17 | |
| Thermafil | Pre-operative | 10 | 1.34 a | 0.72 | 0.01 | 2.86 |
| Post-operative | 10 | 0.05 a | 0.04 | 0.00 | 0.11 |
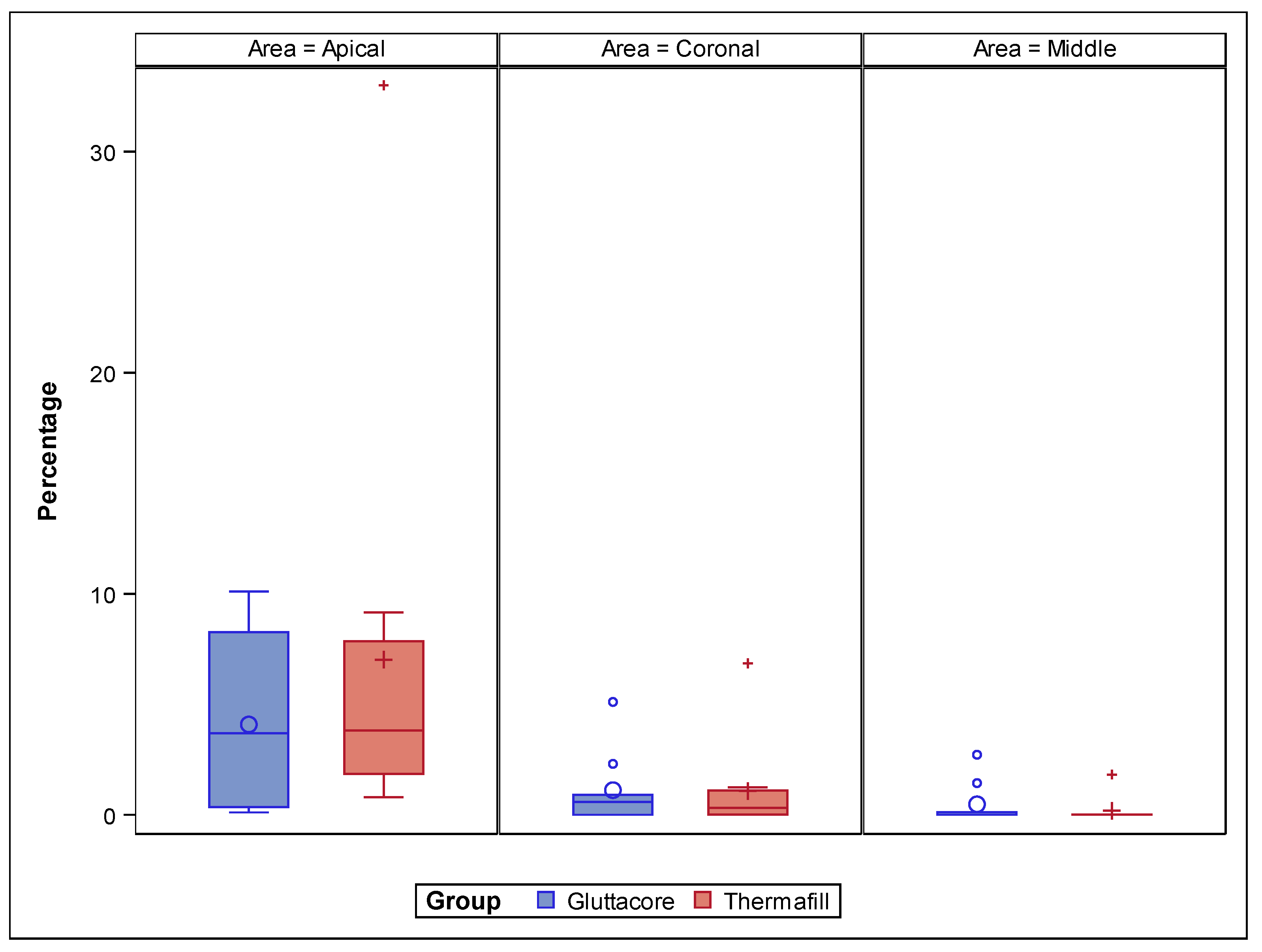
| Study Group | Root Third | Estimate | SD |
|---|---|---|---|
| GuttaCore | Coronal | 1.114 a | 1.491 |
| Middle | 0.473 a | 1.491 | |
| Apical | 4.084 a | 1.491 | |
| Thermafill | Coronal | 1.070 a | 1.415 |
| Middle | 0.184 a | 1.415 | |
| Apical | 7.011 a | 1.415 |
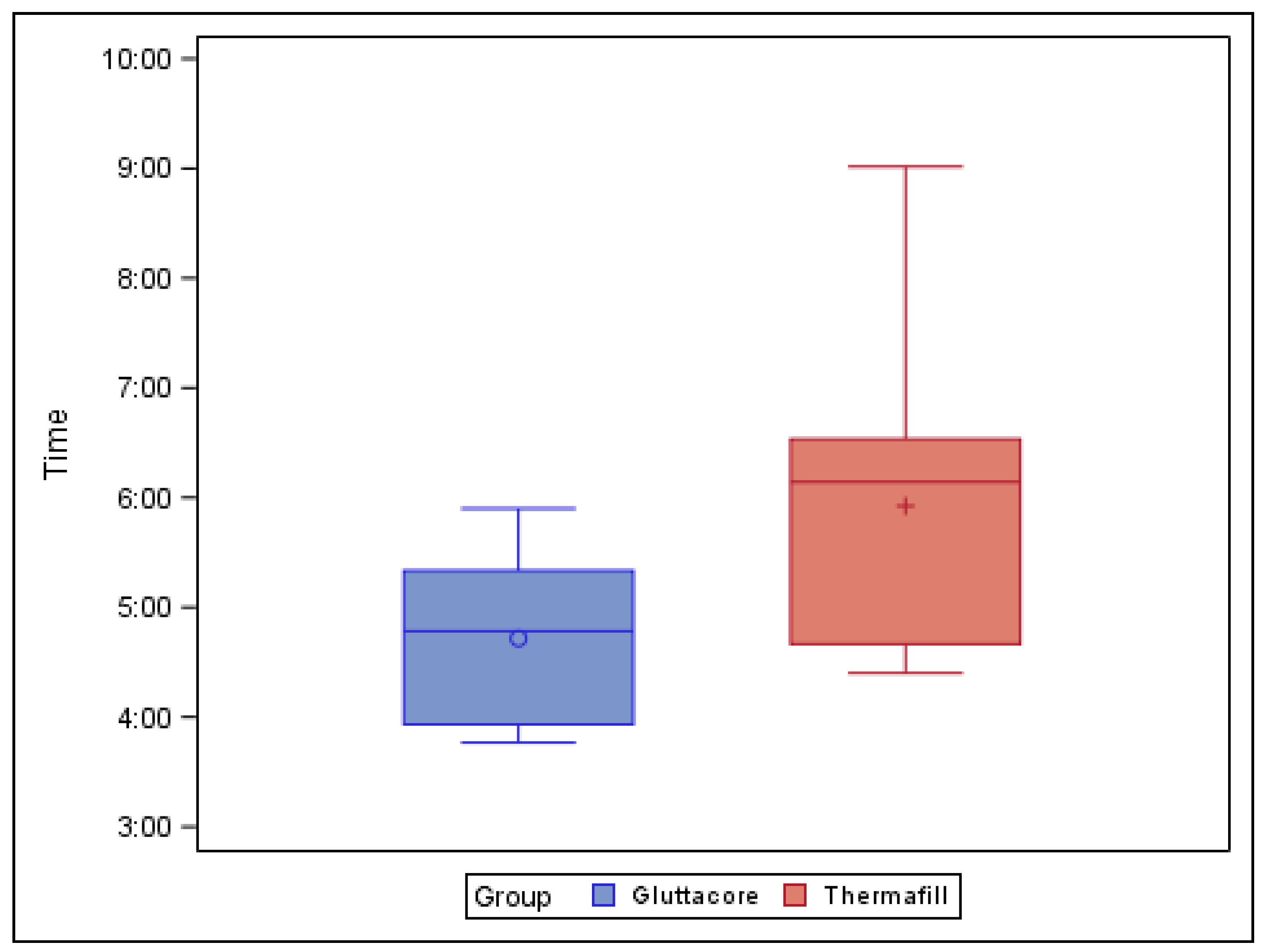
| Study Group | n | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|
| GuttaCore | 9 | 4.72 a | 0.76 | 3.77 | 5.90 |
| Thermafill | 10 | 5.92 b | 1.42 | 4.40 | 9.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faus-Llácer, V.; Pérez, R.L.; Faus-Matoses, I.; Ruiz-Sánchez, C.; Zubizarreta-Macho, Á.; Sauro, S.; Faus-Matoses, V. Efficacy of Removing Thermafil and GuttaCore from Straight Root Canal Systems Using a Novel Non-Surgical Root Canal Re-Treatment System: A Micro-Computed Tomography Analysis. J. Clin. Med. 2021, 10, 1266. https://doi.org/10.3390/jcm10061266
Faus-Llácer V, Pérez RL, Faus-Matoses I, Ruiz-Sánchez C, Zubizarreta-Macho Á, Sauro S, Faus-Matoses V. Efficacy of Removing Thermafil and GuttaCore from Straight Root Canal Systems Using a Novel Non-Surgical Root Canal Re-Treatment System: A Micro-Computed Tomography Analysis. Journal of Clinical Medicine. 2021; 10(6):1266. https://doi.org/10.3390/jcm10061266
Chicago/Turabian StyleFaus-Llácer, Vicente, Rubén Linero Pérez, Ignacio Faus-Matoses, Celia Ruiz-Sánchez, Álvaro Zubizarreta-Macho, Salvatore Sauro, and Vicente Faus-Matoses. 2021. "Efficacy of Removing Thermafil and GuttaCore from Straight Root Canal Systems Using a Novel Non-Surgical Root Canal Re-Treatment System: A Micro-Computed Tomography Analysis" Journal of Clinical Medicine 10, no. 6: 1266. https://doi.org/10.3390/jcm10061266