
Predictors of Progression and Mortality in Patients with Prevalent Rheumatoid Arthritis and Interstitial Lung Disease: A Prospective Cohort Study

 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Design
2.2. Study Population
2.3. Protocol
2.4. Working Definitions and Endpoints
2.5. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
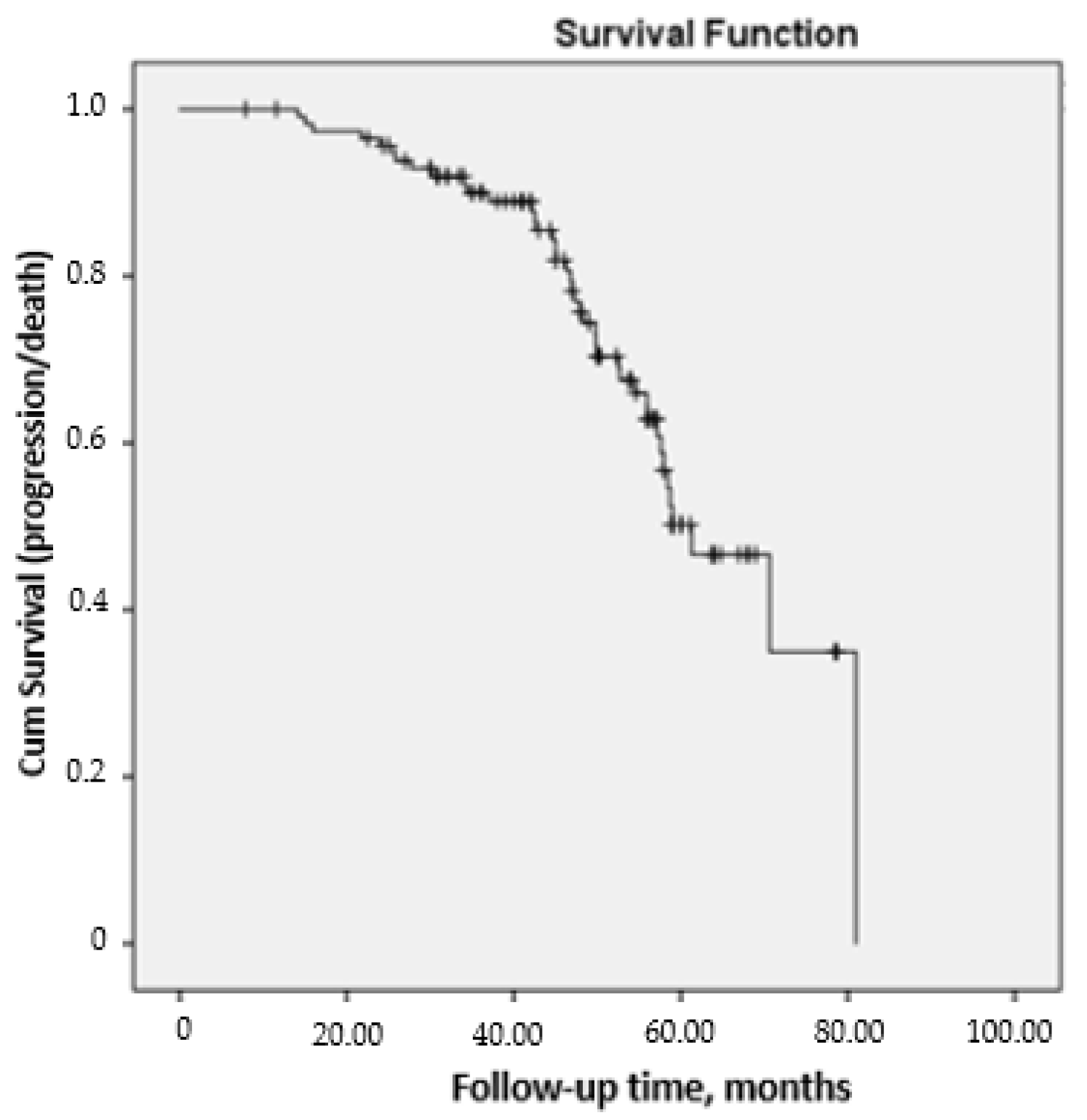
3.2. Course of ILD after 60 Months of Follow-Up
3.3. Factors Associated with Progression and Mortality of ILD after 60 Months of Follow-Up
3.4. Adverse Events
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robles-Pérez, A.; Luburich, P.; Bolivar, S.; Dorca, J.; Nolla, J.M.; Molina-Molina, M.; Narváez, J. A prospective study of lung disease in a cohort of early rheumatoid arthritis patients. Sci. Rep. 2020, 10. [Google Scholar] [CrossRef]
- Kim, D.; Cho, S.-K.; Choi, C.-B.; Choe, J.-Y.; Chung, W.T.; Hong, S.-J.; Jun, J.-B.; Jung, Y.O.; Kim, T.-H.; Kim, T.-J.; et al. Impact of interstitial lung disease on mortality of patients with rheumatoid arthritis. Rheumatol. Int. 2017, 37, 1735–1745. [Google Scholar] [CrossRef] [PubMed]
- Hyldgaard, C.; Hilberg, O.; Pedersen, A.B.; Ulrichsen, S.P.; Løkke, A.; Bendstrup, E.; Ellingsen, T. A population-based cohort study of rheu-matoid arthritis-associated interstitial lung disease: Comorbidity and mortality. Ann. Rheum. Dis. 2017, 76, 1700–1706. [Google Scholar] [CrossRef]
- Koduri, G.; Norton, S.; Young, A.; Cox, N.; Davies, P.; Devlin, J.; Dixey, J.; Gough, A.; Prouse, P.; Winfield, J.; et al. Interstitial lung disease has a poor prognosis in rheumatoid arthritis: Results from an inception cohort. Rheumatology 2010, 49, 1483–1489. [Google Scholar] [CrossRef] [Green Version]
- Kakutani, T.; Hashimoto, A.; Tominaga, A.; Kodama, K.; Nogi, S.; Tsuno, H.; Ogihara, H.; Nunokawa, T.; Komiya, A.; Furukawa, H.; et al. Related factors, increased mortality and causes of death in patients with rheumatoid arthritis-associated interstitial lung disease. Mod. Rheumatol. 2019, 30, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.J.; Ryu, J.; Tazelaar, H.; Myers, J.L.; Tuder, R.; Cool, C.; Swigris, J.J.; Brown, K.K. Fibrosing interstitial pneumonia predicts survival in patients with rheumatoid arthritis-associated interstitial lung disease (RA-ILD). In Proceedings of the American Thoracic Society 2011 International Conference, Denver, CO, USA, 13–18 May 2011. Respir. Med. 2011, 107, 1247–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.A.; Lee, J.S.; Park, J.K.; Lee, E.Y.; Song, Y.W. Clinical characteristics associated with occurrence and poor prognosis of interstitial lung disease in rheumatoid arthritis. Korean J. Intern. Med. 2019, 34, 434–441. [Google Scholar] [CrossRef]
- Kim, E.J.; Elicker, B.M.; Maldonado, F.; Webb, W.R.; Ryu, J.H.; Van Uden, J.H.; Lee, J.S.; King, T.E.; Collard, H.R. Usual interstitial pneumonia in rheumatoid arthri-tis-associated interstitial lung disease. Eur. Respir. J. 2010, 35, 1322–1328. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.C.; Choi, K.H.; Jacob, J.; Song, J.W. Prognostic role of blood KL-6 in rheumatoid arthritis—Associated interstitial lung disease. PLoS ONE 2020, 15, e0229997. [Google Scholar] [CrossRef]
- Zamora-Legoff, J.A.; Krause, M.L.; Crowson, C.S.; Ryu, J.H.; Matteson, E.L. Patterns of interstitial lung disease and mortality in rheumatoid arthritis. Rheumatology 2017, 56, 344–350. [Google Scholar] [CrossRef] [Green Version]
- Singh, N.; Varghese, J.; England, B.R.; Solomon, J.J.; Michaud, K.; Mikuls, T.R.; Healy, H.S.; Kimpston, E.M.; Schweizer, M.L. Impact of the pattern of interstitial lung disease on mortality in rheumatoid arthritis: A systematic literature review and meta-analysis. Semin. Arthritis Rheum. 2019, 49, 358–365. [Google Scholar] [CrossRef]
- Kelly, C.A.; Saravanan, V.; Nisar, M.; Arthanari, S.; Woodhead, F.A.; Price-Forbes, A.N.; Dawson, J.; Sathi, N.; Ahmad, Y.; Koduri, G.; et al. Rheumatoid arthritis-related interstitial lung disease: Associations, prognostic factors and physiological and radiological characteristics—A large multicentre UK study. Rheumatology 2014, 53, 1676–1682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, Q.; Wang, L.; Li, L.; Li, Y.; Liu, R.; Zheng, Y. Risk factors for progression and prognosis of rheumatoid arthritis-associated inter-stitial lung disease: Single center study with a large sample of Chinese population. Clin. Rheumatol. 2019, 38, 1109–1116. [Google Scholar] [CrossRef]
- Hozumi, H.; Nakamura, Y.; Johkoh, T.; Sumikawa, H.; Colby, T.V.; Kono, M.; Hashimoto, D.; Enomoto, N.; Fujisawa, T.; Inui, N.; et al. Acute exacerbation in rheumatoid arthri-tis-associated interstitial lung disease: A retrospective case control study. BMJ Open 2013, 3, e003132. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.; Song, J.W.; Yoon, H.-Y.; Cross, G.; Barnett, J.; Woo, W.L.; Adams, F.; Kokosi, M.; Devaraj, A.; Renzoni, E.; et al. Prevalence and Effects of Emphysema in Never-Smokers with Rheumatoid Arthritis Interstitial Lung Disease. EBioMedicine 2018, 28, 303–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.-K.; Kim, D.S.; Yoo, B.; Seo, J.B.; Rho, J.-Y.; Colby, T.V.; Kitaichi, M. Histopathologic pattern and clinical features of rheumatoid arthri-tis-associated interstitial lung disease. Chest 2005, 127, 2019–2027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nurmi, H.M.; Purokivi, M.K.; Kärkkäinen, M.S.; Kettunen, H.-P.; Selander, T.A.; Kaarteenaho, R.L. Variable course of disease of rheu-matoid arthritis-associated usual interstitial pneumonia compared to other subtypes. BMC Pulm. Med. 2016, 16, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas-Serrano, J.; Herrera-Bringas, D.; Pérez-Román, D.I.; Pérez-Dorame, R.; Mateos-Toledo, H.; Mejía, M. Rheumatoid arthri-tis-related interstitial lung disease (RA-ILD): Methotrexate and the severity of lung disease are associated to prognosis. Clin. Rheumatol. 2017, 36, 1493–1500. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.J.; Chung, J.H.; Cosgrove, G.P.; Demoruelle, M.K.; Fernandez-Perez, E.R.; Fischer, A.; Frankel, S.K.; Hobbs, S.B.; Huie, T.J.; Ketzer, J.; et al. Predictors of mortality in rheu-matoid arthritis-associated interstitial lung disease. Eur. Respir. J. 2016, 47, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, Y.; Takayanagi, N.; Sugiura, H.; Miyahara, Y.; Tokunaga, D.; Kawabata, Y.; Sugita, Y. Lung diseases directly associated with rheumatoid arthritis and their relationship to outcome. Eur. Respir. J. 2010, 37, 1411–1417. [Google Scholar] [CrossRef] [Green Version]
- Saketkoo, L.A.; Espinoza, L.R. Rheumatoid arthritis interstitial lung disease: Mycophenolate mofetil as an antifibrotic and dis-ease-modifying antirheumatic drug. Arch. Intern. Med. 2008, 168, 1718–1719. [Google Scholar] [PubMed]
- Oldham, J.M.; Lee, C.; Valenzi, E.; Witt, L.J.; Adegunsoye, A.; Hsu, S.; Chen, L.; Montner, S.; Chung, J.H.; Noth, I.; et al. Azathioprine response in patients with fibrotic connective tissue disease-associated interstitial lung disease. Respir. Med. 2016, 121, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Barnes, H.; Holland, A.E.; Westall, G.P.; Goh, N.S.; Glaspole, I.N. Cyclophosphamide for connective tissue disease-associated interstitial lung disease. Cochrane Database Syst. Rev. 2018, 1, 010908. [Google Scholar] [CrossRef]
- Flaherty, K.R.; Wells, A.U.; Cottin, V.; Devaraj, A.; Walsh, S.L.; Inoue, Y.; Richeldi, L.; Kolb, M.; Tetzlaff, K.; Stowasser, S.; et al. Nintedanib in Progressive Fibrosing Interstitial Lung Diseases. N. Engl. J. Med. 2019, 381, 1718–1727. [Google Scholar] [CrossRef] [Green Version]
- Ibfelt, E.H.; Jacobsen, R.K.; Kopp, T.I.; Cordtz, R.L.; Jakobsen, A.S.; Seersholm, N.; Shaker, S.B.; Dreyer, L. Methotrexate and risk of interstitial lung disease and respiratory failure in rheumatoid arthritis: A nationwide population-based study. Rheumatology 2021, 60, 346–352. [Google Scholar] [CrossRef]
- Kiely, P.; Busby, A.D.; Nikiphorou, E.; Sullivan, K.A.; Walsh, D.; Creamer, P.; Dixey, J.; Young, A. Is incident rheumatoid arthritis interstitial lung disease associated with methotrexate treatment? Results from a multivariate analysis in the ERAS and ERAN inception cohorts. BMJ Open 2019, 9, e028466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cubero, C.C.; Carmona, E.C.; Casasempere, P.V. Systematic Review of the Impact of Drugs on Diffuse Interstitial Lung Disease Associated with Rheumatoid. Arthritis Reumatol. Clin. 2020. [Google Scholar] [CrossRef]
- Narváez, J.; Robles-Pérez, A.; Molina-Molina, M.; Vicens-Zygmunt, V.; Luburich, P.; Yañez, M.A.; Alegre, J.J.; Nolla, J.M. Real-world clinical effec-tiveness of rituximab rescue therapy in patients with progressive rheumatoid arthritis-related interstitial lung disease. Semin. Arthritis Rheum. 2020, 50, 902–910. [Google Scholar] [CrossRef]
- Md Yusof, M.Y.; Kabia, A.; Darby, M.; Lettieri, G.; Beirne, P.; Vital, E.M.; Dass, S.; Emery, P. Effect of rituximab on the progression of rheumatoid arthritis-related interstitial lung disease: 10 years’ experience at a single centre. Rheumatology 2017, 8, 1348–1357. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Díaz, C.; Loricera, J.; Castañeda, S.; López-Mejías, R.; Ojeda-García, C.; Olivé, A.; Rodríguez-Muguruza, S.; Carreira, P.E.; Pérez-Sandoval, T.; Retuerto, M.; et al. Abatacept in patients with rheumatoid arthritis and interstitial lung disease: A national multicenter study of 63 patients. Semin. Arthritis Rheum. 2018, 48, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Díaz, C.; Castañeda, S.; Melero-González, R.B.; Ortiz-Sanjuán, F.; Juan-Mas, A.; Carrasco-Cubero, C.; Casafont-Solé, I.; Olivé, A.; Rodríguez-Muguruza, S.; Almodóvar-González, R.; et al. Abatacept in interstitial lung disease associated with rheumatoid arthritis: National multicenter study of 263 patients. Rheumatology 2020, 59, 3906–3916. [Google Scholar] [CrossRef]
- Manfredi, A.; Cassone, G.; Furini, F.; Gremese, E.; Venerito, V.; Atzeni, F.; Arrigoni, E.; Della Casa, G.; Cerri, S.; Govoni, M.; et al. Tocilizumab therapy in rheumatoid arthritis with interstitial lung disease: A multicenter retrospective study. Intern. Med. J. 2019, 50, 1085–1090. [Google Scholar] [CrossRef]
- Mena-Vázquez, N.; Godoy-Navarrete, F.J.; Manrique-Arija, S.; Aguilar-Hurtado, M.C.; Romero-Barco, C.M.; Ureña-Garnica, I.; Espildora, F.; Añón-Oñate, I.; Pérez-Albaladejo, L.; Gomez-Cano, C.; et al. Non-anti-TNF biologic agents are associated with slower worsening of interstitial lung disease secondary to rheumatoid ar-thritis. Clin. Rheumatol. 2020, 40, 133–142. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., III; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Socie-ty/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic inter-stitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Gaujoux-Viala, C.; Mouterde, G.; Baillet, A.; Claudepierre, P.; Fautrel, B.; Le Loët, X.; Maillefert, J.-F. Evaluating disease activity in rheumatoid arthritis: Which composite index is best? A systematic literature analysis of studies comparing the psychometric properties of the DAS, DAS28, SDAI and CDAI. Jt. Bone Spine 2012, 79, 149–155. [Google Scholar] [CrossRef]
- Maska, L.; Anderson, J.; Michaud, K. Measures of functional status and quality of life in rheumatoid arthritis: Health Assessment Questionnaire Disability Index (HAQ), Modified Health Assessment Questionnaire (MHAQ), Multidimensional Health Assessment Questionnaire (MDHAQ), Health Assessment. Arthritis Rheum. 2011, 63, S4–S13. [Google Scholar] [CrossRef]
- Agencia Española de Medicamentos y Productos Sanitarios. Información para las notificaciones de sospechas de reacciones adversas a medicamentos por parte de profesionales sanitarios. Available online: https://www.aemps.gob.es/vigilancia/medicamentosUsoHumano/SEFVH/NRA-SEFV-H/notificaSospechas-RAM-profSanitarios.htm#NSRAPSqueRAM2015 (accessed on 20 January 2021).
- Spagnolo, P.; Lee, J.S.; Sverzellati, N.; Rossi, G.; Cottin, V. The Lung in Rheumatoid Arthritis: Focus on Interstitial Lung Disease. Arthritis Rheumatol. 2018, 70, 1544–1554. [Google Scholar] [CrossRef] [Green Version]
- Kelly, C.A.; Nisar, M.; Arthanari, S.; Carty, S.; Woodhead, F.A.; Price-Forbes, A.; Middleton, D.; Dempsey, O.; Miller, D.; Basu, N.; et al. Rheumatoid arthritis related interstitial lung disease—Improving outcomes over 25 years: A large multicentre UK study. Rheumatology 2020. [Google Scholar] [CrossRef] [PubMed]
- Farquhar, H.; Vassallo, R.; Edwards, A.L.; Matteson, E.L. Pulmonary Complications of Rheumatoid Arthritis. Semin. Respir. Crit. Care Med. 2019, 40, 194–207. [Google Scholar] [CrossRef]
- Nannini, C.; Ryu, J.H.; Matteson, E.L. Lung disease in rheumatoid arthritis. Curr. Opin. Rheumatol. 2015, 20, 340–346. [Google Scholar] [CrossRef]
- Conway, R.; Low, C.; Coughlan, R.J.; O’Donnell, M.J.; Carey, J.J. Methotrexate and lung disease in rheumatoid arthritis: A meta-analysis of randomized controlled trials. Arthritis Rheumatol. 2015, 66, 803–812. [Google Scholar] [CrossRef]
- Conway, R.; Low, C.; Coughlan, R.J.; O’Donnell, M.J.; Carey, J.J. Leflunomide Use and Risk of Lung Disease in Rheumatoid Arthritis: A Systematic Literature Review and Metaanalysis of Randomized Controlled Trials. J. Rheumatol. 2016, 43, 855–860. [Google Scholar] [CrossRef]
- Perez-Alvarez, R.; Perez-De-Lis, M.; Diaz-Lagares, C.; Pego-Reigosa, J.M.; Retamozo, S.; Bove, A.; Brito-Zeron, P.; Bosch, X.; Ramos-Casals, M. Interstitial Lung Disease Induced or Exacerbated by TNF-Targeted Therapies: Analysis of 122 Cases. Semin. Arthritis Rheum. 2011, 41, 256–264. [Google Scholar] [CrossRef]
- Nakashita, T.; Ando, K.; Takahashi, K.; Motojima, S. Possible effect of abatacept on the progression of interstitial lung disease in rheumatoid arthritis patients. Respir. Investig. 2016, 54, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Kawashiri, S.-Y.; Kawakami, A.; Sakamoto, N.; Ishimatsu, Y.; Eguchi, K. A fatal case of acute exacerbation of interstitial lung disease in a patient with rheumatoid arthritis during treatment with tocilizumab. Rheumatol. Int. 2012, 32, 4023–4026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wendling, D.; Vidon, C.; Godfrin-Valnet, M.; Rival, G.; Guillot, X.; Prati, C. Exacerbation of combined pulmonary fibrosis and em-physema syndrome during tocilizumab therapy for rheumatoid arthritis. Jt. Bone Spine 2013, 80, 670–671. [Google Scholar] [CrossRef]
- Mori, S.; Koga, Y.; Sugimoto, M. Different risk factors between interstitial lung disease and airway disease in rheumatoid arthritis. Respir. Med. 2012, 106, 1591–1599. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Liu, R.; Zhang, Y.; Zhou, J.; Li, Y.; Xu, Y.; Gao, S.; Zheng, Y. A retrospective study on the predictive implications of clinical characteristics and therapeutic management in patients with rheumatoid arthritis-associated interstitial lung disease. Clin. Rheumatol. 2019, 39, 1457–1470. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Legoff, J.A.; Krause, M.L.; Crowson, C.S.; Ryu, J.H.; Matteson, E.L. Progressive Decline of Lung Function in Rheumatoid Arthritis-Associated Interstitial Lung Disease. Arthritis Rheumatol. 2017, 69, 542–549. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total = 116 |
|---|---|
| Epidemiological characteristics | |
| Female sex, n (%) | 63 (54.3) |
| Caucasian race, n (%) | 113 (97.4) |
| Age, years, mean (SD) | 68.3 (9.9) |
| Clinical and analytical characteristics | |
| Current smoker | – |
| Nonsmoker, n (%) | 57 (49.1) |
| Smoker, n (%) | 23 (19.8) |
| Exsmoker, n (%) | 36 (31.0) |
| Body mass index, mean (SD) | 27.8 (4.1) |
| Time since diagnosis of RA, months, median (25%–75%) | 148.5 (71.5–217.8) |
| Diagnostic delay, months, median (25%–75%) | 8.5 (4.9–16.8) |
| Time since diagnosis of ILD, months, median (25%–75%) | 27.5 (9.8–60.0) |
| Positive rheumatoid factor (>10), n (%) | 111 (95.7) |
| Positive ACPA titer (>20), n (%) | 100 (86.2) |
| High ACPA titer (>340), n (%) | 48 (41.4) |
| Erosive disease, n (%) | 76 (65.5) |
| Sjögren syndrome, n (%) | 18 (15.5) |
| Osteoporosis, n (%) | 51 (44.0) |
| Treatment | |
| Synthetic DMARD | 100 (86.2) |
| Methotrexate, n (%) | 51 (44.0) |
| Leflunomide, n (%) | 30 (25.9) |
| Sulfasalazine, n (%) | 9 (7.8) |
| Hydroxychloroquine, n (%) | 21 (18.1) |
| Biologic DMARD | 50 (43.1) |
| Infliximab, n (%) | 1 (0.9) |
| Etanercept, n (%) | 6 (5.2) |
| Adalimumab, n (%) | 3 (2.6) |
| Golimumab, n (%) | 3 (2.6) |
| Certolizumab, n (%) | 3 (2.6) |
| Tocilizumab, n (%) | 6 (5.2) |
| Abatacept, n (%) | 15 (12.9) |
| Rituximab, n (%) | 13 (11.2) |
| Immunosuppressants | 11 (9.5) |
| Mycophenolate, n (%) | 7 (6.0) |
| Azathioprine, n (%) | 4 (3.4) |
| Antifibrotic agents, nintedanib, n (%) | 1 (0.9) |
| Baseline corticosteroids, n (%) | 69 (60.0) |
| Dose of baseline corticosteroids, median (25%–75%) | 5.0 (0.0–7.5) |
| Variable | UIP, n = 71 | NSIP, n = 41 | p Value |
|---|---|---|---|
| Epidemiological characteristics | |||
| Female sex, n (%) | 31 (43.7) | 30 (73.2) | 0.003 |
| Caucasian, n (%) | 68 (95.8) | 41 (100) | 0.182 |
| Age, years, mean (SD) | 68.9 (9.4) | 68.0 (10.9) | 0.639 |
| Clinical and analytical characteristics | |||
| Current smoker | 0.815 | ||
| Nonsmoker, n (%) | 32 (45.1) | 21 (51.2) | |
| Smoker, n (%) | 13 (18.3) | 7 (17.1) | |
| Exsmoker, n (%) | 26 (36.6) | 13 (31.7) | |
| Body mass index, mean (SD) | 28.1 (4.3) | 27.5 (4.1) | 0.578 |
| Time since diagnosis of RA, months, median (25%–75%) | 146.1 (69.2–227.9) | 167.7 (87.5–224.2) | 0.987 |
| Diagnostic delay, months, median (25%–75%) | 10.9 (4.9–18.4) | 7.0 (4.9–15.5) | 0.395 |
| Time since diagnosis of ILD, months, mean (SD) | 23.8 (9.6–59.9) | 36.4 (11.3–67.9) | 0.337 |
| Positive rheumatoid factor (>10), n (%) | 69 (97.2) | 38 (92.7) | 0.267 |
| ACPA titer (>20), n (%) | 65 (91.5) | 31 (75.6) | 0.020 |
| Erosive disease, n (%) | 53 (74.6) | 22 (53.7) | 0.023 |
| Sjögren syndrome, n (%) | 11 (15.5) | 7 (17.1) | 0.826 |
| Osteoporosis, n (%) | 32 (45.1) | 17 (41.5) | 0.711 |
| Treatment | |||
| Synthetic DMARD | 60 (84.5) | 37 (90.2) | 0.390 |
| Methotrexate, n (%) | 28 (39.4) | 22 (50.7) | 0.145 |
| Leflunomide, n (%) | 20 (28.2) | 9 (22.0) | 0.469 |
| Sulfasalazine, n (%) | 7 (9.9) | 1 (2.4) | 0.142 |
| Hydroxychloroquine, n (%) | 14 (19.7) | 7 (17.1) | 0.730 |
| Biologic DMARD | 30 (42.3) | 19 (46.3) | 0.674 |
| Infliximab, n (%) | 1 (1.4) | 0 (0.0) | 0.445 |
| Etanercept, n (%) | 3 (4.2) | 3 (4.2) | 0.485 |
| Adalimumab, n (%) | 1 (1.4) | 2 (4.9) | 0.273 |
| Golimumab, n (%) | 2 (2.8) | 1 (2.4) | 0.905 |
| Certolizumab, n (%) | 2 (2.8) | 1 (2.4) | 0.905 |
| Tocilizumab, n (%) | 4 (4.2) | 1 (2.4) | 0.324 |
| Abatacept, n (%) | 9 (12.7) | 6 (14.6) | 0.769 |
| Rituximab, n (%) | 9 (12.7) | 4 (9.8) | 0.642 |
| Immunosuppressants | 7 (9.9) | 4 (9.8) | 0.986 |
| Mycophenolate, n (%) | 5 (7.0) | 2 (4.9) | 0.649 |
| Azathioprine, n (%) | 2 (2.8) | 2 (4.9) | 0.571 |
| Antifibrotic agents, nintedanib, n (%) | 1 (0.9) | 0 (0.0) | 0.045 |
| Corticosteroids at baseline, n (%) | 42 (59.1) | 22 (50.7) | 0.800 |
| Dose of corticosteroids at baseline, median (25%–75%) | 5.0 (0.0–6.0) | 5.0 (0.0–7.5) | 0.140 |
| Variable | Baseline | End of Follow-Up | p Value |
|---|---|---|---|
| Duration of follow-up, mean (SD) | – | 49.1 (14.4) | – |
| Respiratory function | |||
| Oxygen saturation, mean (SD) | 96.1 (2.2) | 95.0 (3.1) | 0.018 |
| Pulmonary function testing | |||
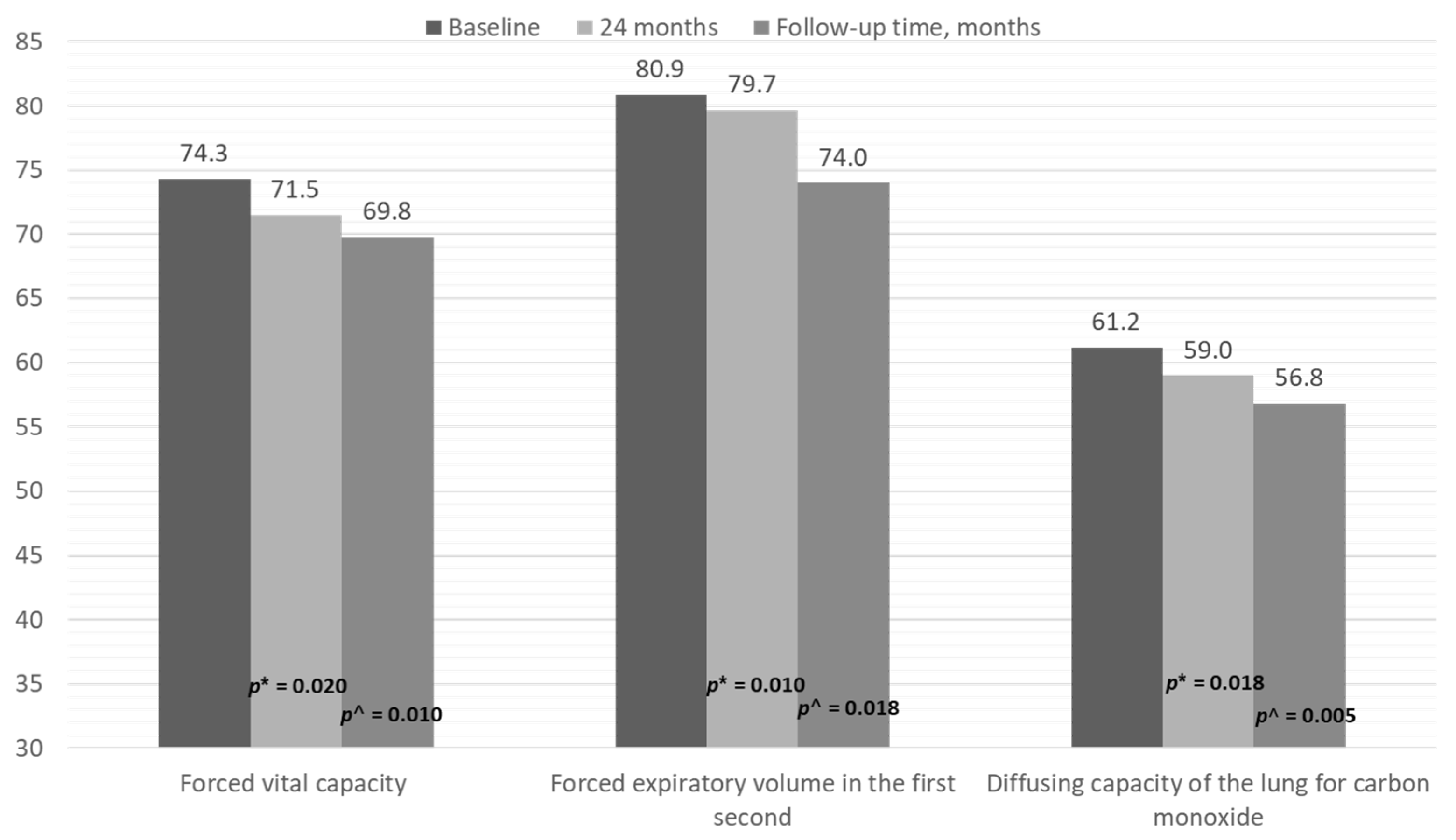
| FVC, mean (SD) | 74.3 (17.3) | 69.8 (23.4) | 0.010 |
| FVC <80%, n (%) | 69 (59.5) | 79 (68.1) | 0.012 |
| FVC ≥80%, n (%) | 47 (40.5) | 37 (31.9) | |
| FEV1, mean (SD) | 80.9 (20.5) | 74.0 (21.1) | 0.018 |
| DLCO-SB, mean (SD) | 61.2 (16.2) | 56.8 (18.5) | 0.005 |
| HRCT | |||
| Radiological pattern | 0.720 | ||
| UIP, n (%) | 71 (61.2) | 74 (63.7) | |
| NSIP, n (%) | 32 (27.6) | 31 (26.7) | |
| Fibrotic NSIP, n (%) | 9 (7.8) | 7 (6.0) | |
| Other, n (%) | 4 (3.4) | 4 (3.4) | |
| Course | |||
| Progression, n (%) | – | 32 (27.6) | |
| Stabilization, n (%) | – | 77 (66.4) | |
| Improvement, n (%) | – | 7 (6.0) | |
| Progression of lung disease (total) * | |||
| Improvement, n (%) | – | 9 (7.8) | |
| Stabilization, n (%) | – | 66 (56.9) | |
| Worsening, n (%) | – | 23 (19.8) | |
| Death, n (%) | – | 18 (15.5) | |
| Inflammatory activity | |||
| DAS28, median (25%–75%) | 2.8 (2.3–4.0) | 3.0 (3.0–5.2) | 0.627 |
| C-reactive protein, median (25%–75%) | 5.3 (2.9–13.0) | 8.0 (2.0–22.0) | 0.320 |
| ESR, median (25%–75%) | 21.0 (9.7–36.5) | 20.0 (8.0–29.0) | 0.136 |
| HAQ, median (25%–75%) | 1.0 (0.2–1.8) | 1.1 (0.6–1.9) | 0.484 |
| Variable | UIP | NSIP | p Value |
|---|---|---|---|
| Duration of follow-up, mean (SD) | 46.8 (14.5) | 47.5 (14.9) | 0.808 |
| Pulmonary function testing | |||
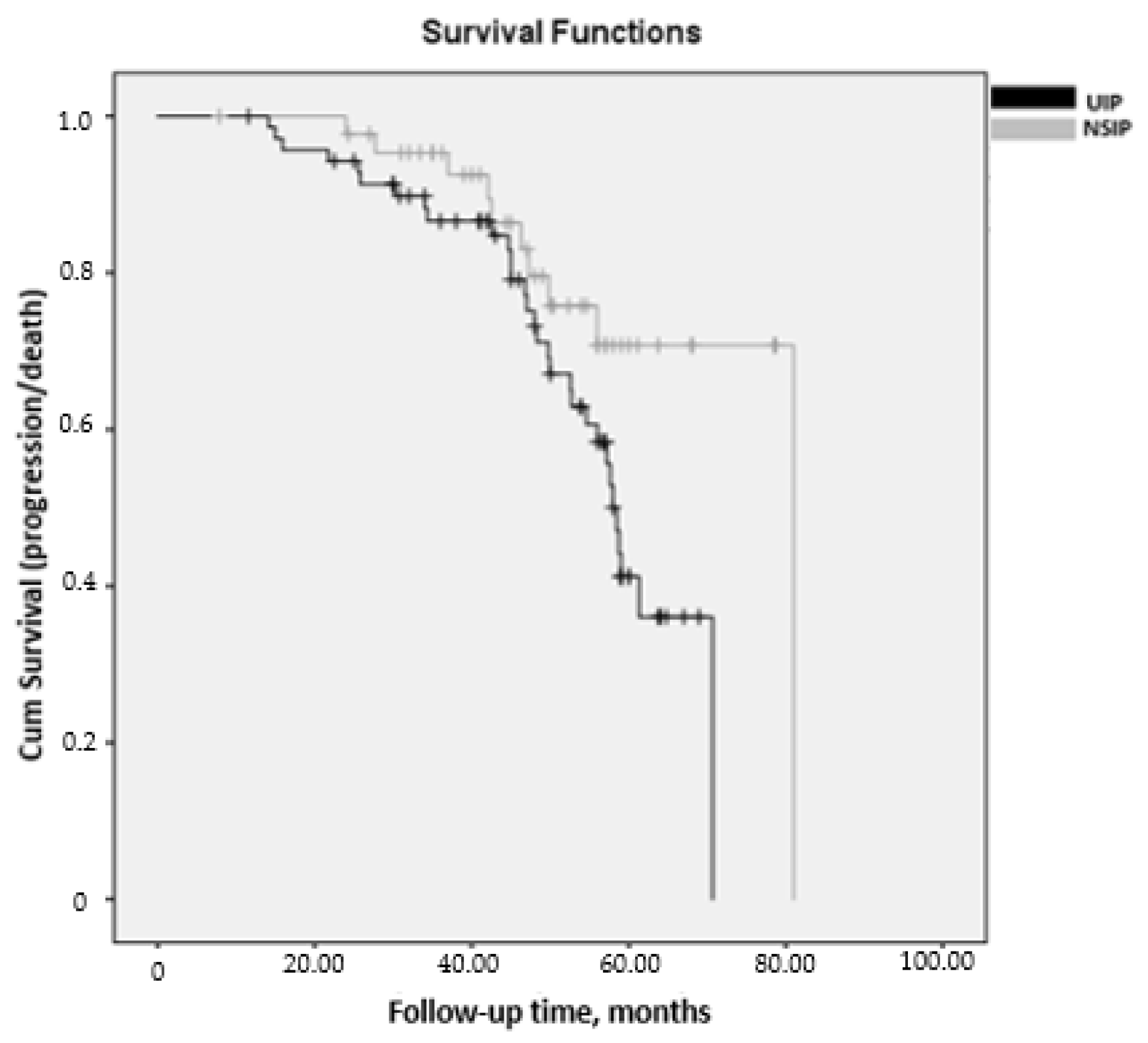
| Last FVC, mean (SD) | 67.6 (22.0) | 78.6 (25.4) | 0.037 |
| Last FEV1<, mean (SD) | 72.1 (21.9) | 78.2 (20.7) | 0.225 |
| Last DLCO, mean (SD) | 66.9 (18.5) | 70.1 (16.7) | 0.235 |
| HRCT | |||
| Course | 0.002 | ||
| Progression, n (%) | 27 (38.0) | 9 (22.0) | |
| Stabilization, n (%) | 44 (62.0) | 26 (63.4) | |
| Improvement, n (%) | 0 (0.0) | 6 (14.6) | |
| Progression of lung disease (total) * | 0.032 | ||
| Improvement, n (%) | 2 (2.8) | 6 (14.6) | |
| Stabilization, n (%) | 38 (53.5) | 25 (61.0) | |
| Worsening, n (%) | 16 (22.5) | 7 (17.1) | |
| Death, n (%) | 15 (21.1) | 3 (7.3) | |
| Inflammatory activity | |||
| Last DAS28, mean (SD) | 3.3 (1.1) | 3.2 (1.4) | 0.428 |
| Last C-reactive protein, mean (SD) | 18.5 (16.9) | 8.6 (7.3) | 0.037 |
| Last ESR, mean (SD) | 26.1 (17.4) | 23.2 (18.2) | 0.823 |
| Last HAQ, mean (SD) | 1.5 (0.7) | 1.2 (0.7) | 0.341 |
| Variable | Univariate HR (95% CI) | Multivariate HR (95% CI) | p Value |
|---|---|---|---|
| Age, years | 1.930 (0.98–1.07) | ||
| Male sex | 1.041 (0.28–2.23) | ||
| History of smoking | 2.204 (1.01–4.85) | 2.543 (1.03–6.24) | 0.042 |
| Radiological pattern, UIP | 2.712 (1.82–7.11) | 2.661 (1.04–6.77) | 0.040 |
| Rheumatoid factor, titer | 1.001 (1.00–1.01) | ||
| High ACPA (>340) | 2.556 (1.17–5.58) | 2.810 (1.17–6.75) | 0.021 |
| Baseline FVC <80 | 2.517 (1.10–5.75) | 3.840 (1.50–6.70) | 0.003 |
| Baseline DLCO-SB <80 | 2.800 (0.90–8.10) | ||
| Corticosteroids | 1.603 (0.71–3.57) | ||
| DMARDs | 0.662 (0.22–1.93) | ||
| Immunosuppressants | 0.661 (0.16–2.64) | ||
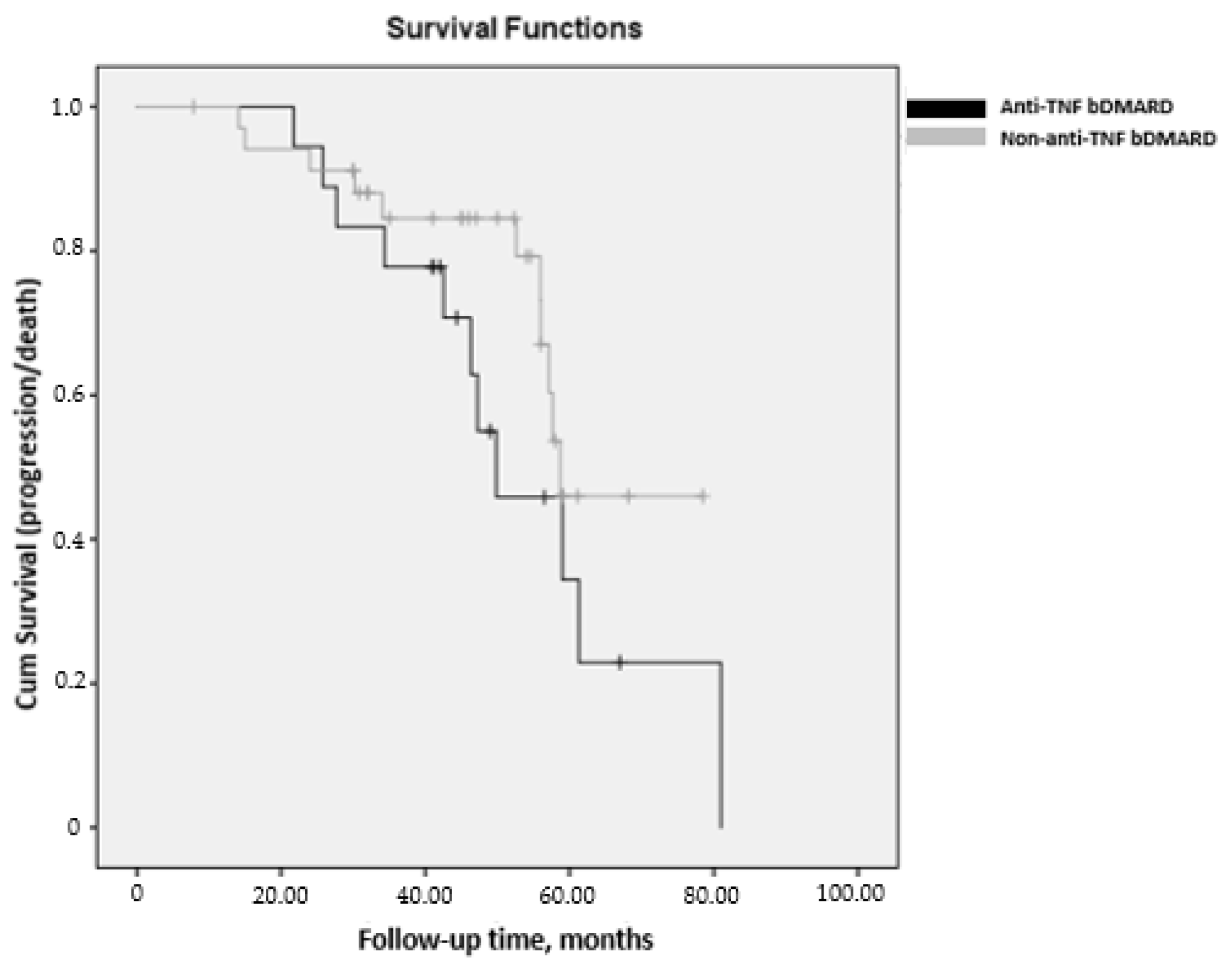
| Anti-TNF | 2.692 (1.02–7.87) | ||
| Non–anti-TNF | 0.618 (0.36–0.89) | 0.472 (0.25–0.86) | 0.014 |
| Variable | Sample = 116 |
|---|---|
| Adverse effects, n (%) | 79 (68.1) |
| Mild adverse effects, n (%) | 48 (41.4) |
| Severe adverse effects, n (%) | 40 (34.4) |
| Incidence of adverse effects (patient-years) | 0.17 |
| Incidence of mild adverse effects (patient-years) | 0.10 |
| Incidence of severe adverse effects (patient-years) | 0.08 |
| Infection, n (%) | 71 (61.2) |
| Respiratory infection, n (%) | 63 (54.3) |
| Other infections, n (%) | 13 (11.2) |
| Cold sore, n (%) | 2 (1.7) |
| Dental infection, n (%) | 1 (0.8) |
| Cutaneous infection, n (%) | 3 (2.5) |
| Urinary infection, n (%) | 7 (6.0) |
| Incidence of infection (patient-years) | 0.15 |
| Incidence of respiratory infection (patient-years) | 0.13 |
| Incidence of other infections (patient-years) | 0.02 |
| Mortality | 18 (15.5) |
| Incidence of mortality (patient-years) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mena-Vázquez, N.; Rojas-Gimenez, M.; Romero-Barco, C.M.; Manrique-Arija, S.; Francisco, E.; Aguilar-Hurtado, M.C.; Añón-Oñate, I.; Pérez-Albaladejo, L.; Ortega-Castro, R.; Godoy-Navarrete, F.J.; et al. Predictors of Progression and Mortality in Patients with Prevalent Rheumatoid Arthritis and Interstitial Lung Disease: A Prospective Cohort Study. J. Clin. Med. 2021, 10, 874. https://doi.org/10.3390/jcm10040874
Mena-Vázquez N, Rojas-Gimenez M, Romero-Barco CM, Manrique-Arija S, Francisco E, Aguilar-Hurtado MC, Añón-Oñate I, Pérez-Albaladejo L, Ortega-Castro R, Godoy-Navarrete FJ, et al. Predictors of Progression and Mortality in Patients with Prevalent Rheumatoid Arthritis and Interstitial Lung Disease: A Prospective Cohort Study. Journal of Clinical Medicine. 2021; 10(4):874. https://doi.org/10.3390/jcm10040874
Chicago/Turabian StyleMena-Vázquez, Natalia, Marta Rojas-Gimenez, Carmen María Romero-Barco, Sara Manrique-Arija, Espildora Francisco, María Carmen Aguilar-Hurtado, Isabel Añón-Oñate, Lorena Pérez-Albaladejo, Rafaela Ortega-Castro, Francisco Javier Godoy-Navarrete, and et al. 2021. "Predictors of Progression and Mortality in Patients with Prevalent Rheumatoid Arthritis and Interstitial Lung Disease: A Prospective Cohort Study" Journal of Clinical Medicine 10, no. 4: 874. https://doi.org/10.3390/jcm10040874