
Is Neoadjuvant Treatment Justified in Clinical T1 Pancreatic Ductal Adenocarcinoma?

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
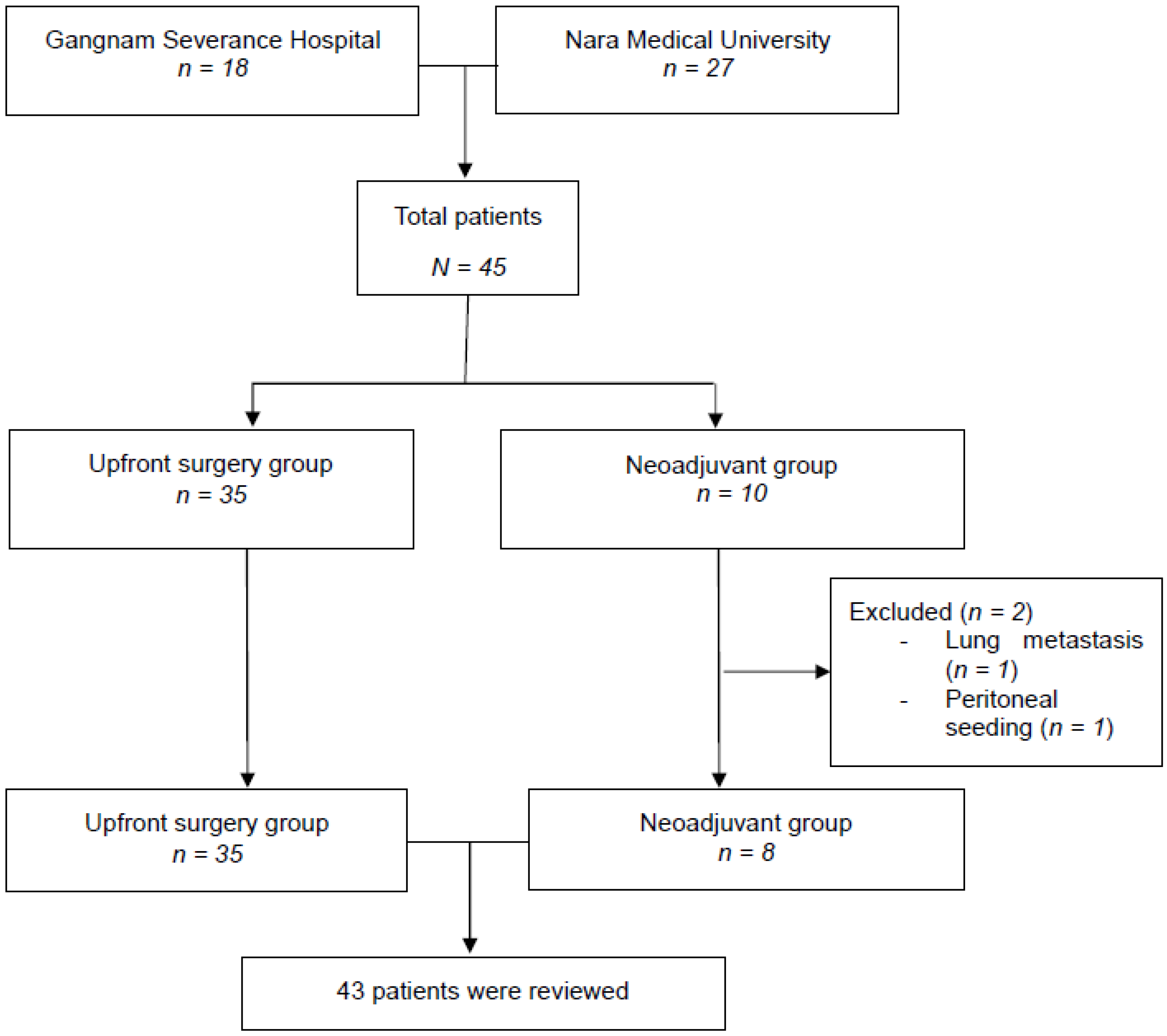
2.1. Patients
2.2. Tumor Assessment
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients with Pancreatic Cancer
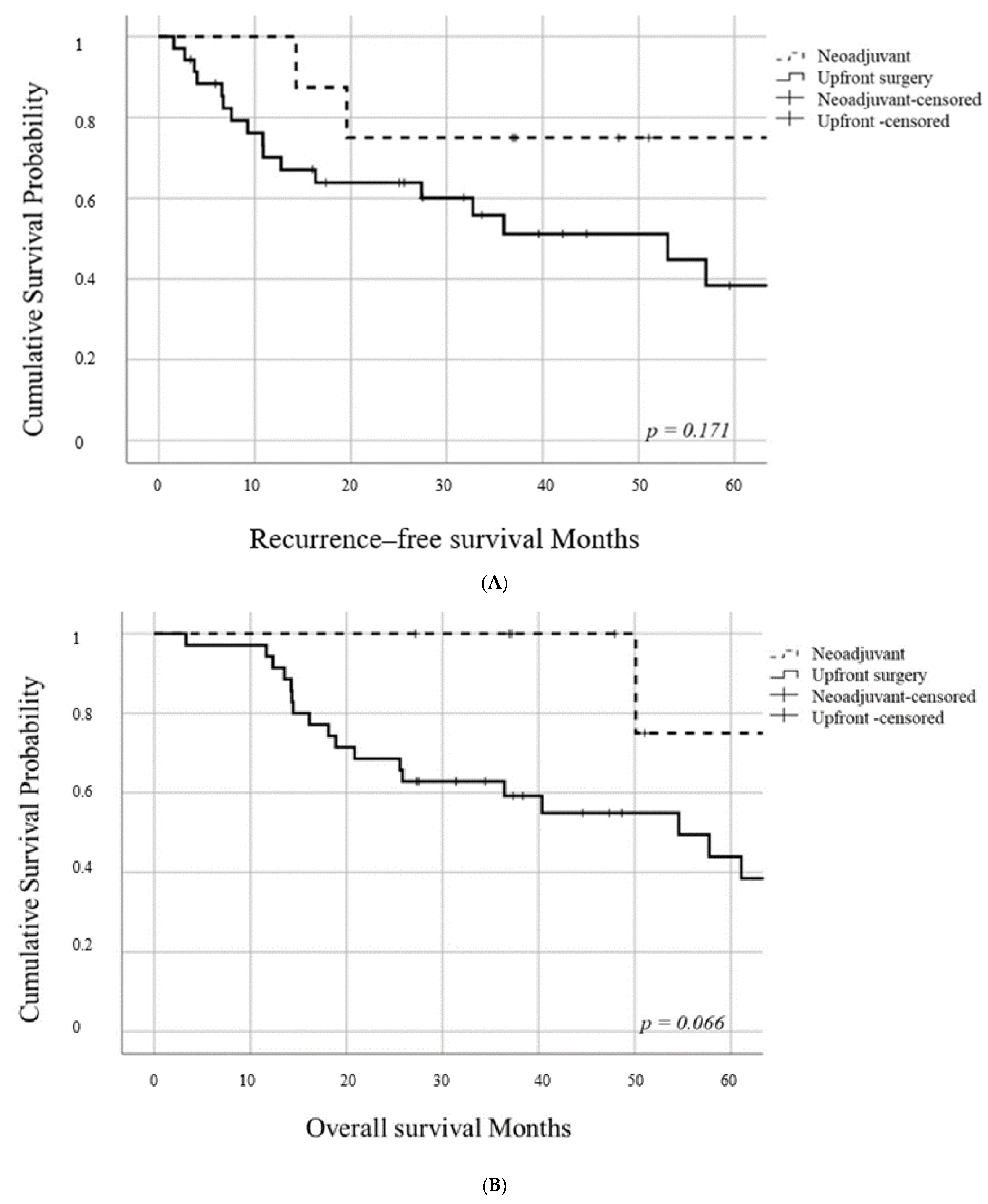
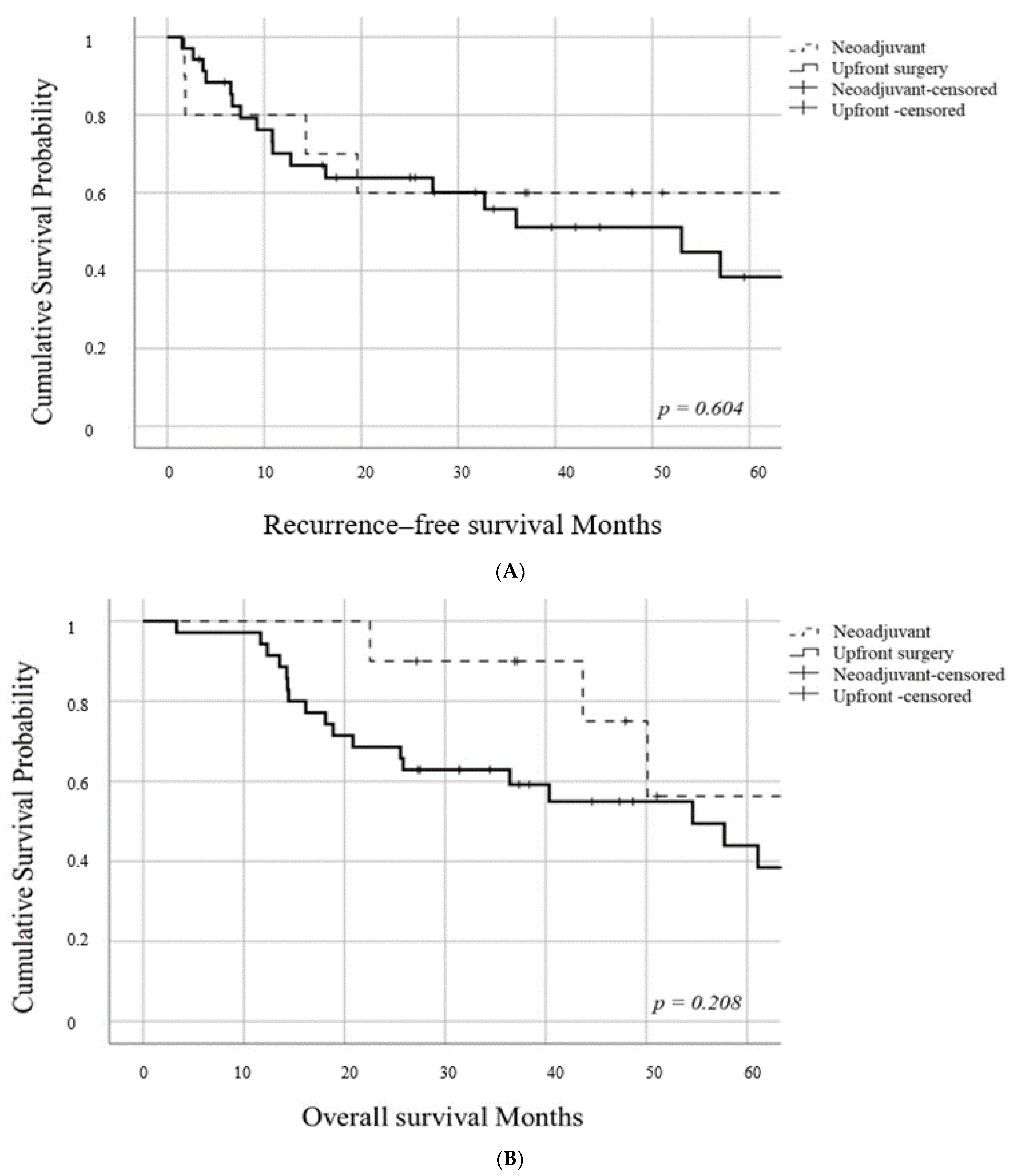
3.2. RFS and OS in Patients with Pancreatic Cancer
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.; Ward, E.; Brawley, O.; Jemal, A. Cancer statistics, 2011: The impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J. Clin. 2011, 61, 212–236. [Google Scholar] [CrossRef] [PubMed]
- Kleeff, J.; Reiser, C.; Hinz, U.; Bachmann, J.; Debus, J.; Jaeger, D.; Friess, H.; Buchler, M.W. Surgery for recurrent pancreatic ductal adenocarcinoma. Ann. Surg. 2007, 245, 566–572. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Stocken, D.D.; Friess, H.; Bassi, C.; Dunn, J.A.; Hickey, H.; Beger, H.; Fernandez-Cruz, L.; Dervenis, C.; Lacaine, F.; et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. New Engl. J. Med. 2004, 350, 1200–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oettle, H.; Neuhaus, P.; Hochhaus, A.; Hartmann, J.T.; Gellert, K.; Ridwelski, K.; Niedergethmann, M.; Zulke, C.; Fahlke, J.; Arning, M.B.; et al. Adjuvant Chemotherapy With Gemcitabine and Long-term Outcomes Among Patients With Resected Pancreatic Cancer The CONKO-001 Randomized Trial. Jama-J. Am. Med. Assoc. 2013, 310, 1473–1481. [Google Scholar] [CrossRef] [Green Version]
- Oneda, E.; Zaniboni, A. Are We Sure that Adjuvant Chemotherapy is the Best Approach for Resectable Pancreatic Cancer? Are We in the Era of Neoadjuvant Treatment? A Review of Current Literature. J. Clin. Med. 2019, 8, 1922. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Heo, J.S.; Choi, S.H.; Choi, D.W. Extended versus peripancreatic lymph node dissection for the treatment of left-sided pancreatic cancer. Ann. Surg. Treat. Res. 2017, 92, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Chone, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. New Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef]
- Jang, J.Y.; Han, Y.; Lee, H.; Kim, S.W.; Kwon, W.; Lee, K.H.; Oh, D.Y.; Chie, E.K.; Lee, J.M.; Heo, J.S.; et al. Oncological Benefits of Neoadjuvant Chemoradiation With Gemcitabine Versus Upfront Surgery in Patients With Borderline Resectable Pancreatic Cancer A Prospective, Randomized, Open-label, Multicenter Phase 2/3 Trial. Ann. Surg. 2018, 268, 215–222. [Google Scholar] [CrossRef]
- Egawa, S.; Toma, H.; Ohigashi, H.; Okusaka, T.; Nakao, A.; Hatori, T.; Maguchi, H.; Yanagisawa, A.; Tanaka, M. Japan Pancreatic Cancer Registry; 30th Year Anniversary Japan Pancreas Society. Pancreas 2012, 41, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.M.; Cameron, J.L.; Campbell, K.A.; Arnold, M.A.; Chang, D.C.; Coleman, J.; Hodgin, M.B.; Sauter, P.K.; Hruban, R.H.; Riall, T.S.; et al. 1423 pancreaticoduodenectomies for pancreatic cancer: A single-institution experience. J. Gastrointest. Surg. 2006, 10, 1199–1210. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Marchegiani, G.; Hong, T.S.; Ryan, D.P.; Deshpande, V.; McDonnell, E.I.; Sabbatino, F.; Santos, D.D.; Allen, J.N.; Blaszkowsky, L.S.; et al. Radiological and Surgical Implications of Neoadjuvant Treatment with FOLFIRINOX for Locally Advanced and Borderline Resectable Pancreatic Cancer. Ann. Surg. 2015, 261, 12–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagakawa, Y.; Sahara, Y.; Hosokawa, Y.; Murakami, Y.; Yamaue, H.; Satoi, S.; Unno, M.; Isaji, S.; Endo, I.; Sho, M.; et al. Clinical Impact of Neoadjuvant Chemotherapy and Chemoradiotherapy in Borderline Resectable Pancreatic Cancer: Analysis of 884 Patients at Facilities Specializing in Pancreatic Surgery. Ann. Surg. Oncol. 2019, 26, 1629–1636. [Google Scholar] [CrossRef]
- White, R.R.; Hurwitz, H.I.; Morse, M.A.; Lee, C.; Anscher, M.S.; Paulson, E.K.; Gottfried, M.R.; Baillie, J.; Branch, M.S.; Jowell, P.S.; et al. Neoadjuvant chemoradiation for localized adenocarcinoma of the pancreas. Ann. Surg. Oncol. 2001, 8, 758–765. [Google Scholar] [CrossRef]
- Bradley, A.; Van Der Meer, R. Upfront Surgery versus Neoadjuvant Therapy for Resectable Pancreatic Cancer: Systematic Review and Bayesian Network Meta-analysis. Sci. Rep. 2019, 9, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvo, F.A.; Matute, R.; Garcia-Sabrido, J.L.; Gomez-Espi, M.; Martinez, N.E.; Lozano, M.A.; Herranz, R. Neoadjuvant chemoradiation with Tegafur in cancer of the pancreas—Initial analysis of clinical tolerance and outcome. Am. J. Clin. Oncol. 2004, 27, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Chawla, A.; Ferrone, C.R. Neoadjuvant Therapy for Resectable Pancreatic Cancer: An Evolving Paradigm Shift. Front.Oncol. 2019, 9, 1085. [Google Scholar] [CrossRef] [Green Version]
- Ettrich, T.J.; Berger, A.W.; Perkhofer, L.; Daum, S.; Konig, A.; Dickhut, A.; Wittel, U.; Wille, K.; Geissler, M.; Algul, H.; et al. Neoadjuvant plus adjuvant or only adjuvant nab-paclitaxel plus gemcitabine for resectable pancreatic cancer—The NEONAX trial (AIO-PAK-0313), a prospective, randomized, controlled, phase II study of the AIO pancreatic cancer group. BMC Cancer 2018, 18. [Google Scholar] [CrossRef]
- Evans, D.B.; Varadhachary, G.R.; Crane, C.H.; Sun, C.C.; Lee, J.E.; Pisters, P.W.T.; Vauthey, J.N.; Wang, H.; Cleary, K.R.; Staerkel, G.A.; et al. Preoperative gemcitabine-based chemoradiation for patients with resectable adenocarcinoma of the pancreatic head. J. Clin. Oncol. 2008, 26, 3496–3502. [Google Scholar] [CrossRef] [Green Version]
- Heinrich, S.; Pestalozzi, B.C.; Schaefer, M.; Weber, A.; Bauerfeind, P.; Knuth, A.; Clavien, P.A. Prospective phase II trial of Neoadjuvant chemotherapy with gemcitabine and cisplatin for resectable adenocarcinoma of the pancreatic head. J. Clin. Oncol. 2008, 26, 2526–2531. [Google Scholar] [CrossRef] [PubMed]
- Hozaeel, W.; Pauligk, C.; Homann, N.; Luley, K.; Kraus, T.W.; Trojan, J.; Bechstein, W.O.; Grimm, K.; Heise, B.; Schmiegel, W.; et al. Randomized multicenter phase II/III study with adjuvant gemcitabine versus neoadjuvant/adjuvant FOLFIRINOX in resectable pancreatic cancer: The NEPAFOX trial. J. Clin. Oncol. 2015, 33. [Google Scholar] [CrossRef]
- Magnin, V.; Moutardier, V.; Giovannini, M.H.; Lelong, B.; Giovannini, M.; Viret, F.; Monges, G.; Bardou, V.J.; Alzieu, C.; Delpero, J.R. Neoadjuvant preoperative chemoradiation in patients with pancreatic cancer. Int. J. Radiat. Oncol. 2003, 55, 1300–1304. [Google Scholar] [CrossRef]
- Murphy, J.E.; Wo, J.Y.; Ryan, D.P.; Clark, J.W.; Jiang, W.Q.; Yeap, B.Y.; Drapek, L.C.; Ly, L.; Baglini, C.V.; Blaszkowsky, L.S.; et al. Total Neoadjuvant Therapy with FOLFIRINOX in Combination With Losartan Followed by Chemoradiotherapy for Locally Advanced Pancreatic Cancer A Phase 2 Clinical Trial. Jama Oncol. 2019, 5, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- Unno, M.; Motoi, F.; Matsuyama, Y.; Satoi, S.; Matsumoto, I.; Aosasa, S.; Shirakawa, H.; Wada, K.; Fujii, T.; Yoshitomi, H.; et al. Randomized phase II/III trial of neoadjuvant chemotherapy with gemcitabine and S-1 versus upfront surgery for resectable pancreatic cancer (Prep-02/JSAP-05). J. Clin. Oncol. 2019, 37. [Google Scholar] [CrossRef]
- Greene, F.L. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Cong, L.; Liu, Q.F.; Zhang, R.H.; Cui, M.; Zhang, X.; Gao, X.; Guo, J.C.; Dai, M.H.; Zhang, T.P.; Liao, Q.; et al. Tumor size classification of the 8th edition of TNM staging system is superior to that of the 7th edition in predicting the survival outcome of pancreatic cancer patients after radical resection and adjuvant chemotherapy. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Simoneau, E.; Chiang, Y.J.; Lee, J.E.; Kim, M.P.; Aloia, T.A.; Vauthey, J.N.; Katz, M.H.; Tzeng, C.W.D. Is early-stage pancreatic adenocarcinoma truly early: Stage migration on final pathology with surgery-first versus neoadjuvant therapy sequencing. Hpb 2019, 21, 1203–1210. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Neoadjuvant Group (n = 8) | Upfront Surgery Group (n = 35) | p-Value | ||
|---|---|---|---|---|
| Age | 66.1 ± 6.9 | 66.8 ± 11.5 | 0.860 | |
| Sex | 0.045 | |||
| Men | 7 (87.5%) | 17 (48.6%) | ||
| Women | 1 (12.5%) | 18 (51.4%) | ||
| (yp)T stage | 0.671 | |||
| (yp)Tis | 1 (12.5%) | 3 (8.6%) | ||
| (yp)T1 | 5 (62.5%) | 26 (74.3%) | ||
| (yp)T2 | 2 (25%) | 4 (11.4%) | ||
| (yp)T3 | 0 (0%) | 2 (5.7%) | ||
| (yp)N stage | 0.511 | |||
| (yp)N0 | 7 (87.5%) | 24 (68.6%) | ||
| (yp)N1 | 1 (12.5%) | 8 (22.9%) | ||
| (yp)N2 | 0 (0%) | 3 (8.6%) | ||
| (yp)Stage | 0.897 | |||
| (yp)CIS | 1 (12.5%) | 3 (8.6%) | ||
| (yp)IA | 5 (62.5%) | 19 (54.3%) | ||
| (yp)IB | 1 (12.5%) | 3 (8.6%) | ||
| (yp)IIB | 1 (12.5%) | 8 (22.9%) | ||
| (yp)III | 0 (0%) | 2 (5.7%) | ||
| PNI | 0.392 | |||
| Positive | 5 (62.5%) | 27 (77.1%) | ||
| Negative | 3 (37.5%) | 8 (22.9%) | ||
| LVI | 0.985 | |||
| Positive | 5 (62.5%) | 22 (62.9%) | ||
| Negative | 3 (37.5%) | 13 (37.1%) | ||
| Diff | 0.688 | |||
| Well diff | 3 (37.5%) | 9 (25.7%) | ||
| Moderate diff | 5 (62.5%) | 21 (60.0%) | ||
| Poorly diff | 0 (0%) | 3 (8.6%) | ||
| Unknown | 0 (0%) | 2 (5.7%) | ||
| Tumor size | cm | 1.4 ± 0.8 | 1.9 ± 1.7 | 0.445 |
| R0/R1 | 0.489 | |||
| R0 | 8 (100%) | 33 (94.3%) | ||
| R1 | 0 (0%) | 2 (5.7%) | ||
| CA19-9 | U/mL | 93.7 [2–441] | 62.2 [0.8–612] | 0.586 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.S.; Nakagawa, K.; Akahori, T.; Nakamura, K.; Takagi, T.; Sho, M.; Park, J.S.; Yoon, D.S. Is Neoadjuvant Treatment Justified in Clinical T1 Pancreatic Ductal Adenocarcinoma? J. Clin. Med. 2021, 10, 873. https://doi.org/10.3390/jcm10040873
Kim HS, Nakagawa K, Akahori T, Nakamura K, Takagi T, Sho M, Park JS, Yoon DS. Is Neoadjuvant Treatment Justified in Clinical T1 Pancreatic Ductal Adenocarcinoma? Journal of Clinical Medicine. 2021; 10(4):873. https://doi.org/10.3390/jcm10040873
Chicago/Turabian StyleKim, Hyung Sun, Kenji Nakagawa, Takahiro Akahori, Kota Nakamura, Tadataka Takagi, Masayuki Sho, Joon Seong Park, and Dong Sup Yoon. 2021. "Is Neoadjuvant Treatment Justified in Clinical T1 Pancreatic Ductal Adenocarcinoma?" Journal of Clinical Medicine 10, no. 4: 873. https://doi.org/10.3390/jcm10040873