
Is Computer-Assisted Tissue Image Analysis the Future in Minimally Invasive Surgery? A Review on the Current Status of Its Applications

 , and
, and
Abstract
:1. Introduction
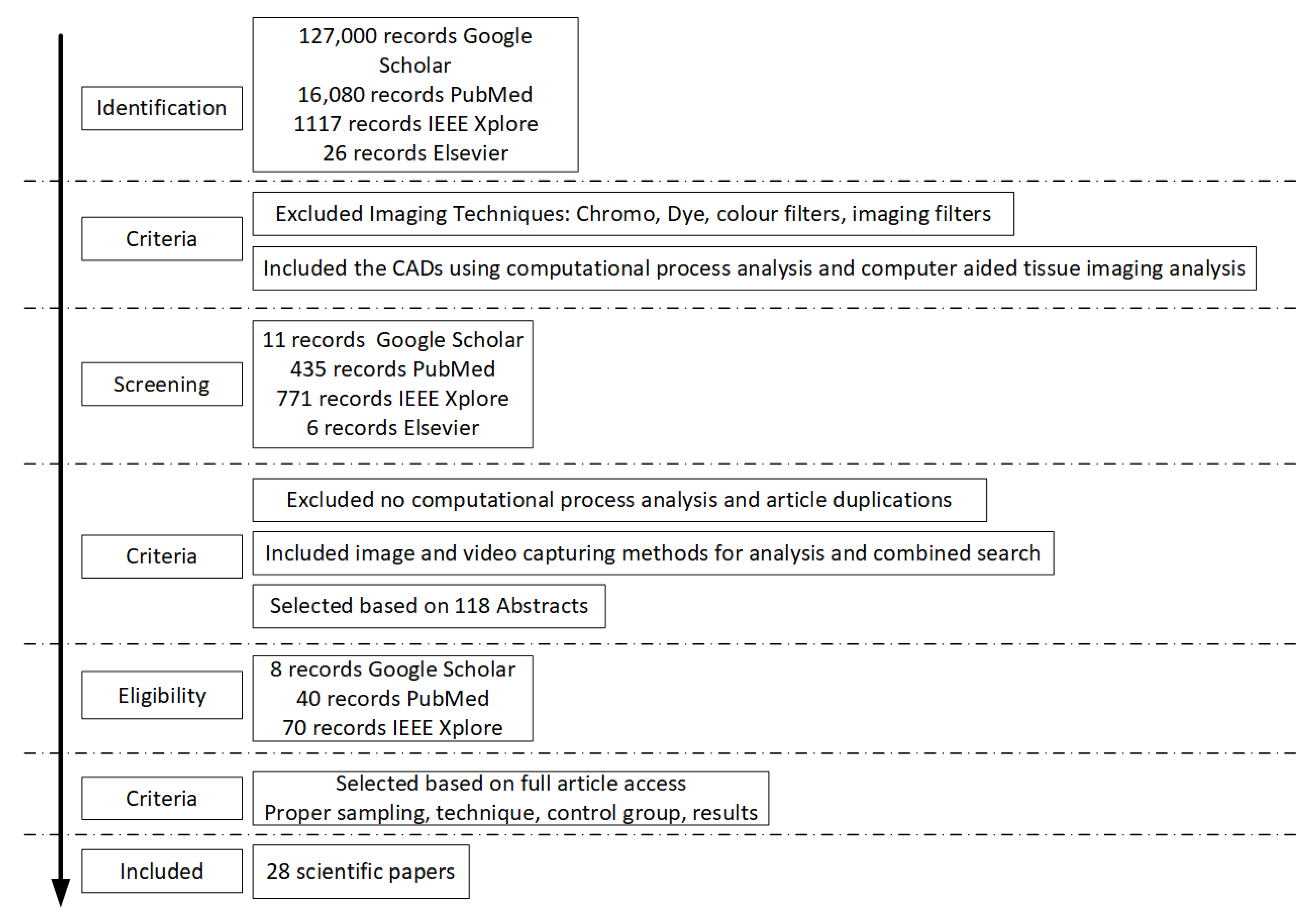
2. Materials and Methods
3. Results
3.1. Assessing Dermatological Abnormalities
3.2. Assessing Gastrointestinal Track Abnormalities
3.3. Assessing Endometrial Hyperplasia and Cancer and Ovarian Malignancies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neofytou, M.S.; Tanos, V.; Constantinou, I.; Pattichis, M.S.; Kyriacou, E.C.; Pattichis, C.S. Computer–Aided Diagnosis in Hysteroscopic Imaging. IEEE J. Biomed. Health Inform. 2015, 19, 1129–1136. [Google Scholar] [CrossRef]
- Efthymiou, M.; Allen, P.B.; Taylor, A.C.F.; Desmond, P.V.; Jayasakera, C.; de Cruz, P.; Kamm, M.A. Chromoendoscopy versus Narrow Band Imaging for Colonic Surveillance in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2013, 19, 2132–2138. [Google Scholar] [CrossRef] [PubMed]
- Atasoy, S.; Mateus, D.; Meining, A.; Yang, G.; Navab, N. Endoscopic Video Manifolds for Targeted Optical Biopsy. IEEE Trans. Med. Imaging 2012, 31, 637–653. [Google Scholar] [CrossRef] [Green Version]
- Chao, Z.; Tsung-Han, T.; Hsiang-Chieh, L.; Tejas, K.; Figueiredo, M.; Yuankai, T.K.; Osman, A.O.; Desmond, A.C.; Schmitt, J.M.; Qin, H.; et al. Characterization of Buried Glands before and after Radiofrequency Ablation by Using 3-Dimensional Optical Coherence Tomography (with Videos). Gastrointest. Endosc. 2012, 76, 32–40. [Google Scholar]
- Abdul-Wadood, D.N.; Loay, E.G.; Nabeel, A.R. Diagnosis of skin cancer using image texture analysis. Int. J. Sci. Eng. Res. 2014, 5, 155. [Google Scholar]
- Bodanese, B.; Silveira, L.F.; Zangaro Amaro, R.; Pacheco, T.T.M.; Pasqualucci, A.C., Jr.; Silveira, L. Discrimination of basal cell carcinoma and melanoma from normal skin biopsies in vitro through Raman spectroscopy and principal component analysis. Photomed. Laser Surg. 2012, 30, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silveira, F.L.; Pacheco, T.T.M.; Bodanese, B.; Pasqualucci, A.C.; Zangaro, A.R., Jr.; Landullfo, S. Discrimination of non-melanoma skin lesions from non-tumor human skin tissues in vivo using Raman spectroscopy and multivariate statistics. Lasers Surg. Med. 2015, 47, 6–16. [Google Scholar] [CrossRef]
- Amelard, R.; Glaister, J.; Wong, A.; Clausi, D.A. Melanoma decision support using lighting-corrected intuitive feature models. In Computer Vision Techniques for the Diagnosis of Skin Cancer; Springer: Berlin/Heidelberg, Germany, 2014; pp. 193–219. [Google Scholar]
- Gadermayr, M.; Kogler, H.; Maximilian, K.; Merhof, D.; Uhl, A.; Vecsei, A. Computer-Aided Texture Analysis Combined with Experts’ Knowledge: Improving Endoscopic Celiac Disease Diagnosis. World J. Gastroenterol. 2016, 22, 7124–7134. [Google Scholar] [CrossRef]
- Neofytou, M.S.; Pattichis, C.S.; Pattichis, M.S.; Tanos, V.; Kyriacou, E.C.; Koutsouris, D. A Standardised Protocol for Texture Feature Analysis of Endoscopic Images in Gynaecological Cancer. BioMed. Eng. OnLine 2007, 6, 44. Available online: http://www.biomedical-engineering-online.com/content/6/1/44 (accessed on 30 November 2021). [CrossRef] [PubMed] [Green Version]
- Neves, A.A.; Di Pietro, M.; O’Donovan, M.; Waterhouse, J.D.; Bohndiek, E.S.; Brindle, M.K.; Fitzgerald, C.R. Detection of early neoplasia in Barrett’s esophagus using lectin-based near-infrared imaging: An ex vivo study on human tissue. Endoscopy 2018, 50, 618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbosa, D.C.; Roupar, D.B.; Ramos, J.C.; Tavares, A.C.; Lima, C.S. Automatic small bowel tumor diagnosis by using multi-scale wavelet-based analysis in wireless capsule endoscopy images. Biomed. Eng. Online 2012, 11, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, L.R.; Antani, S.; Jeronimo, J.; Schiffman, M.; Bopf, M.; Neve, L.; Cornwell, C.; Budihas, S.R.; Thoma, G.R. Technology for medical education, research, and disease screening by exploitation of biomarkers in a large collection of uterine cervix images. In Proceedings of the 19th IEEE Symposium on Computer-Based Medical Systems (CBMS’06), Salt Lake City, UT, USA, 22–23 June 2006; IEEE, 2006; pp. 826–831. [Google Scholar]
- Munzenmayer, C.; Winter, C.; Rupp, S.; Kage, A.; Wittenberg, T. Texture-based computer-assisted diagnosis for fiberscopic images. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009. [Google Scholar]
- Scharcanski, J.; Gaviao, W. Hierarchical Summarization of Diagnostic Hysteroscopy Videos. In Proceedings of the IEEE International Conference on Image Processing, Atlanta, GA, USA, 8–11 October 2006; pp. 129–132. [Google Scholar]
- Terry, B.S.; Ruppert, A.D.; Steinhaus, K.R.; Schoen, J.A.; Rentschler, M.E. An integrated port camera and display system for laparoscopy. IEEE Trans. Biomed. Eng. 2010, 57, 1191–1197. [Google Scholar] [CrossRef]
- Cals, F.L.J.; Schut, T.C.B.; Caspers, P.J.; Baatenburg de Jong, R.J.; Koljenović, S.; Puppels, G.J. Raman spectroscopic analysis of the molecular composition of oral cavity squamous cell carcinoma and healthy tongue tissue. Analyst 2018, 143, 4090–4102. [Google Scholar] [CrossRef] [PubMed]
- Dasgeb, B.; Morris, M.; Mehregan, D.; Siegel, E. Quantified Ultrasound Elastography in the Assessment of Cutaneous Carcinoma. Br. J. Radiol. 2015, 88, 20150344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Venkataraman, S.; Gustafsson, U.; Oyama, C.J.; Ferris, G.D.; Lieberman, W.R. Using acetowhite opacity index for detecting cervical intraepithelial neoplasia. J. Biomed. Opt. 2009, 14, 014020. [Google Scholar] [CrossRef]
- Vlachokosta, A.A.; Asvestas, P.A.; Gkrozou, F.; Lavasidis, L.; Matsopoulos, G.K.; Paschopoulos, M. Classification of hysteroscopical images using texture and vessel descriptors. Med. Biol. Eng. Comput. 2013, 51, 859–867. [Google Scholar] [CrossRef]
- Fujimoto, J.G.; Pitris, C.; Boppart, S.A.; Brezinski, M.E. Optical coherence tomography: An emerging technology for biomedical imaging and optical biopsy. Neoplasia 2000, 2, 9–25. [Google Scholar] [CrossRef] [Green Version]
- Metin, G.N.; Laura, B.E.; Ali, C.; Madabhushi, R.M.N.; Yener, B. Histopathological image analysis: A review. IEEE Rev. Biomed. Eng. 2009, 2, 147–171. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Wirkert, S.J.; Iszatt, J.; Hannes Kenngott, M.W.; Mayer, B.; Stock, C.; Clancy NTElson, D.S.; Maier-Hein, L. Tissue classification for laparoscopic image understanding based on multispectral texture analysis. J. Med. Imaging 2017, 4, 015001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boustany, N.; Boppart, S.; Backman, V. Microscopic imaging and spectroscopy with scattered light. Annu. Rev. Biomed. Eng. 2010, 12, 285–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczypinski, P.; Klepaczko, A.; Pazurek, M.; Daniel, P. Texture and colour based image segmentation and pathology detection in capsule endoscopy videos. Comput. Methods Programs Biomed. 2014, 113, 396–411. [Google Scholar] [CrossRef]
- Chenzhou, W.; Gleysteen, J.; Nutte, T.T.; Yi, L.; Eben, R. In-vivo optical imaging in head and neck oncology: Basic principles, clinical applications and future directions. Int. J. Oral Sci. 2018, 10, 10. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.-H.; Qi, J.; Lu, J.; Wang, S.; Wu, C.; Shih, W.-C.; Larin, K.V. Improvement of tissue analysis and classification using optical coherence tomography combined with Raman spectroscopy. J. Innov. Opt. Health Sci. 2015, 8, 2015. [Google Scholar] [CrossRef]
- STORZ Telescopes. Available online: https://www.karlstorz.com/ (accessed on 30 November 2021).


{kind=link}
| Image Processing Evaluation: Manual or automated image interpretation that filters artefacts from a database of images, e.g., endoscopic surgery video summary. |
| Colour-spectrum, Characterization and Filtering: Image colour texture content of the region of interest (ROI). Colour texture features are extracted over different colour spaces or hue saturation values (HSV). (1) Red green blue (RGB), (2) Luminance (Y), (3) Chrominance (red-yellow)/chrominance (blue-yellow) (YCrCb). For each colour space component, a standard grayscale feature is used and can be widely applied for texture characterization according to different texture features. |
| Tissue image features There are 26 texture features from each colour component. (i) Statistical Features (SF): (1) Mean, (2) Variance, (3) Median, (4) Energy, (5) Skewness, (6) Kurtosis, (7) Mode, (8) Entropy. (ii) Spatial Gray Level Dependence Matrices (SGLDM) (1) Angular second moment, (2) Contrast, (3) Correlation, (4) Homogeneity, (5) Variance, (6) Entropy, (7) Sum Entropy, (8) Sum Average, (9) Sum Variance, (10) Difference Entropy, (11) Difference Variance, (12) Information Measurement of Correlation 1, (13) Information Measurement of Correlation 2. (iii) Gray Level Difference Statistics (GLDS): (1) Mean, (2) Entropy, (3) Contrast, (4) Homogeneity, (5) Energy. |
| Algorithm and Statistical evaluation Training and testing to distinguish normal from abnormal Regions of Interest (ROI). CATIA system performance was evaluated using SVM algorithm and probabilistic neural networks (PNN). C-SVM network was used to investigate the Gaussian radial basis function (RBF) kernel and the linear kernel. Principal component analysis (PCA) reforms a dataset into a bilinear model of linear independent variables and uses a mathematical equation to explain the variation within the dataset. Vectors within the matrix are reshaped into images that show the spatial distribution forming abundance images, which represent the abundance of each vector for each pixel. Abundance images are then plotted in a colour-scaled image and can be combined with prominent differences between the samples highlighted. Partial least squares discriminant analysis (PLS-DA) is a supervised data reduction technique. It uses a versatile algorithm that can predict and describe modelling as well as select discriminative variables. |
| Journal | Technique | Aim | Sample | Methodology | Results | Critical comments |
|---|---|---|---|---|---|---|
| Intl J of Scient & Engineering Research (IJSER) [5] | CATTA of microscopic images | Skin Cancer Dg (Squamous and Basal cell Carcinomas) | 80 images of skin BMP 24 bit/pixel 1280 × 1024 pixels Blocks Size = 75–225 pixels | Compare normal and abnormal tissue (1) Pre-processing: RGB 2 GRAY - liner image stretching (2) Image ROIs partitioning (3) Discriminating texture features Fifty samples used for training the minimum distance classifier method | Combinations of textural types of features 200 × 200 pixels recognition provided 89.92% for allocation accuracy 93.75% for diagnosis accuracy | Small number of samples Image Stretching = loss of imaging info Partitioning = increase processing time and computational resources Image segmentation may increase the diagnostic accuracy |
| Photomed Laser Surgery, 2012 [6] | Raman spectroscopy and PCA algorithm | Discrimination of BCC and melanoma from normal skin biopsies in vitro | Histo skin images: 145 spectra Normal 30 BCC 96 Melanoma 19 | Raman spectroscopy coupled to a fiber optic Raman probe. PCA and Elucidation distance classify samples according to histopathology | Differentiate normal from BCC and melanoma with accuracy 92.4%, sensitivity 99.1%, and specificity 93.3% | Raman spectroscopy can discriminate colour band frequency and can possibly be combined with any CATIA method adding to the sensitivity of the test. However, the technical complexity and procedural approach seem to be the main obstacles to its implementation. |
| Lasers in Surgery and Medicine, 2015 [7] | Raman spectroscopy and multivariate statistics | Discrimination between Mg and Bg skin lesions prior to surgery | In vivo image results compared to histopathology 250 normal images and 14 Bg, 133 BCC 30 SCC, 57 AK | PCA/DA and PLS/DA based on Euclidean Quadratic space distances were used to discriminate between Bg and Mg tissues using RS | Non melanoma versus normal and Bg precancerous lesions; the discrimination accuracy was 91.9% and 82.8%, respectively | Standard methodology microscopy Histopathological sections analysis |
| Series in Bio Engineering [8] | Illumination correction and feature extraction on skin lesion images | Skin lesion analysis Melanoma and nevi | Overall 206 standard camera images ROI 200 × 200 pixels 119 malignant melanomas and 87 nevi | (1) Multistage illumination correction algorithm (2) Histogram equalization (3) Feature extraction method (4) SVM model | Accuracy 72.52–81.26% for 3 different feature sets Combination between the features and framework provide better results | Data set is fair Conclusions are confusing Weak methodology (ground truth values, algorithms for nevi versus melanoma are not acknowledged) Insufficient data analysis Discrimination between malignant melanoma and nevi is not clear |
| Journal | Targeted Organ | Technique | Aim | Sample | Methodology | Results | Critical Comments |
|---|---|---|---|---|---|---|---|
| Alinent Pharmacol Ther [2] | Colon | Colonoscopy vs. chromo endoscopy | Dg of dysplasia in patients with IBD | 6 studies 1277 patients with IBD (Review paper) | Comparison of std colo/py to Chromo endoscopy to detect dysplasia controlled by histo Meta-analysis | 91.3% specificity, 93.9% sensitivity for tumor detection | Not reported 1. Tu size detection ability 2. Texture features values 3. Small no of frames |
| World Journal of Gastrology [9] | Celiac Disease Diagnosis | Endoscopy and Computer Aided Texture Analysis (CATTA) | Detection of Intestinal mucosa alterations due to celiac disease | 290 children 2835 duodenum | Endoscopic images recorded tissue alteration by modified immersion technique compared to histopathology Bx | CATTA reduced Dg error up to 31% Dg accuracy improved by 10% | Small patient numbers Low statistical power analysis Weak study design |
| BioMedical Engineering OnLine [10] | Colon polyps and colitis | Chromo endoscopy | Detection Rate of polyp and ulcerative colitis Procedure time | 75 patients 586 images | White light endoscopy (WLE) followed by CE (Indigo Carmine) colonoscopy for UC surveillance | ×30 ability to detect metaplasia 72% in pre-CE-IM and 63% in post-CE-IM | CATTA improves diagnostic accuracy Well designed study |
| Gastrointest Endosc. [11] | Esophagus | 3D optical coherence tomography for CE-IM | Detection of esophageal metaplasia | patients 18 pre-treatment 16 post-RFA tx | Identification of metaplasia before and after therapy | Chromo endoscopy is superior to light endoscopy by 7% detecting dysplastic lesions | Heterogeneous samples More studies needed |
| BioMedEng OnLine [12] | Small bowel | Endoscopic capsule video multiscale wavelet | Detection of small Bg or Mg bowel tumors | 14 patients 700 frames | Multiscale texture features analysis Wavelet transformation Image Classification | Dysplasia detected by WLE at 9.3% and WLE and CE at 21.3%. Improved Median colo/copy withdrawal time | high rates of polyp detection enhanced dysplasia detection |
| Journal | Target Organ | Technique | Aim | Sample | Methodology | Results | Critical Comments |
|---|---|---|---|---|---|---|---|
| BioMedical Engineering OnLine, 2007 [10] | A standardized protocol for texture feature analysis of endoscopic images in gynecological cancer | Endoscopy video | Gynecology | Normal 209 vs. 209 abnormal ROIs | Texture Features Colour correction Gamma correction Calibration Viewing conditions | Gamma correction improve the comparison between different viewing conditions. Texture features can differentiate normal vs. abnormal ROIs | More images can be imported for further analysis |
| CBMS, 19th IEEE International Symposium on IEEE, 2006 [13] | Technology for medical education, Research, and Disease Screening by Exploitation of Biomarkers in a Large Collection of Uterine Cervix Images | Cervical images colour features discrimination | Gynecology | Classification using Gaussian mixture model, Lab colour and one geometrical feature to discriminate clinically significant images. | Image pre-processor used to remove specular reflecting artifacts with 90% success rates | New camera projection software with an algorithm to infer the rotation of the lens improved boundary estimation and image conversions | |
| IEEE EMBS 2009 [14] | Texture-based Computer-Assisted Diagnosis for fiberscope Images | GIT endoscopy Fiberscope images | For Improving diagnosis in GIT Endoscopy Images before and after CATA | 350 esophagus 129 gastric mucosa 164 Barret esophagus 158 squamous epithelium | A new CAD system that filters the artifacts first with an image filtering algorithm, then applies a colour texture algorithm. Evaluation is based on an image database with artificially rendered fiber artifacts | Similar to highest accuracy achieved by standard original images and Gabor filter by 80% No improvement after filtered procedure | Insufficient pre-processing More tissue texture feature algorithms can be applied |
| IEEE International Conference on Image Processing, 2006 [15] | Hierarchical Summarization of Diagnostic Hysteroscopy Videos | Hysteroscopy video | Gynecology | 12 hysteroscopy videos | Video summarization Video segmentation | False positive 26% for 11 videos | Small sample More videos |
| IEEE EMBS, 2010 [16] | An Integrated Port Camera and Display System for Laparoscopy | Port camera | Gynecology | The Powered port camera integrating visual system components with a cannula port | Results show that ex vivo tissue identification and acquisition was as good as the traditional methods | New device: (1) reduced the invasiveness of the laparoscopic procedure (2) reduced its cost (3) improved the laparoscopic procedure |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanos, V.; Neofytou, M.; Soliman, A.S.A.; Tanos, P.; Pattichis, C.S. Is Computer-Assisted Tissue Image Analysis the Future in Minimally Invasive Surgery? A Review on the Current Status of Its Applications. J. Clin. Med. 2021, 10, 5770. https://doi.org/10.3390/jcm10245770
Tanos V, Neofytou M, Soliman ASA, Tanos P, Pattichis CS. Is Computer-Assisted Tissue Image Analysis the Future in Minimally Invasive Surgery? A Review on the Current Status of Its Applications. Journal of Clinical Medicine. 2021; 10(24):5770. https://doi.org/10.3390/jcm10245770
Chicago/Turabian StyleTanos, Vasilios, Marios Neofytou, Ahmed Samy Abdulhady Soliman, Panayiotis Tanos, and Constantinos S. Pattichis. 2021. "Is Computer-Assisted Tissue Image Analysis the Future in Minimally Invasive Surgery? A Review on the Current Status of Its Applications" Journal of Clinical Medicine 10, no. 24: 5770. https://doi.org/10.3390/jcm10245770