
Should Ultrasound-Guided High Frequency Focused Ultrasound Be Considered as an Alternative Non-Surgical Treatment of Uterine Fibroids in Non-Asiatic Countries? An Opinion Paper

 , ,
, ,
Abstract
:1. Introduction
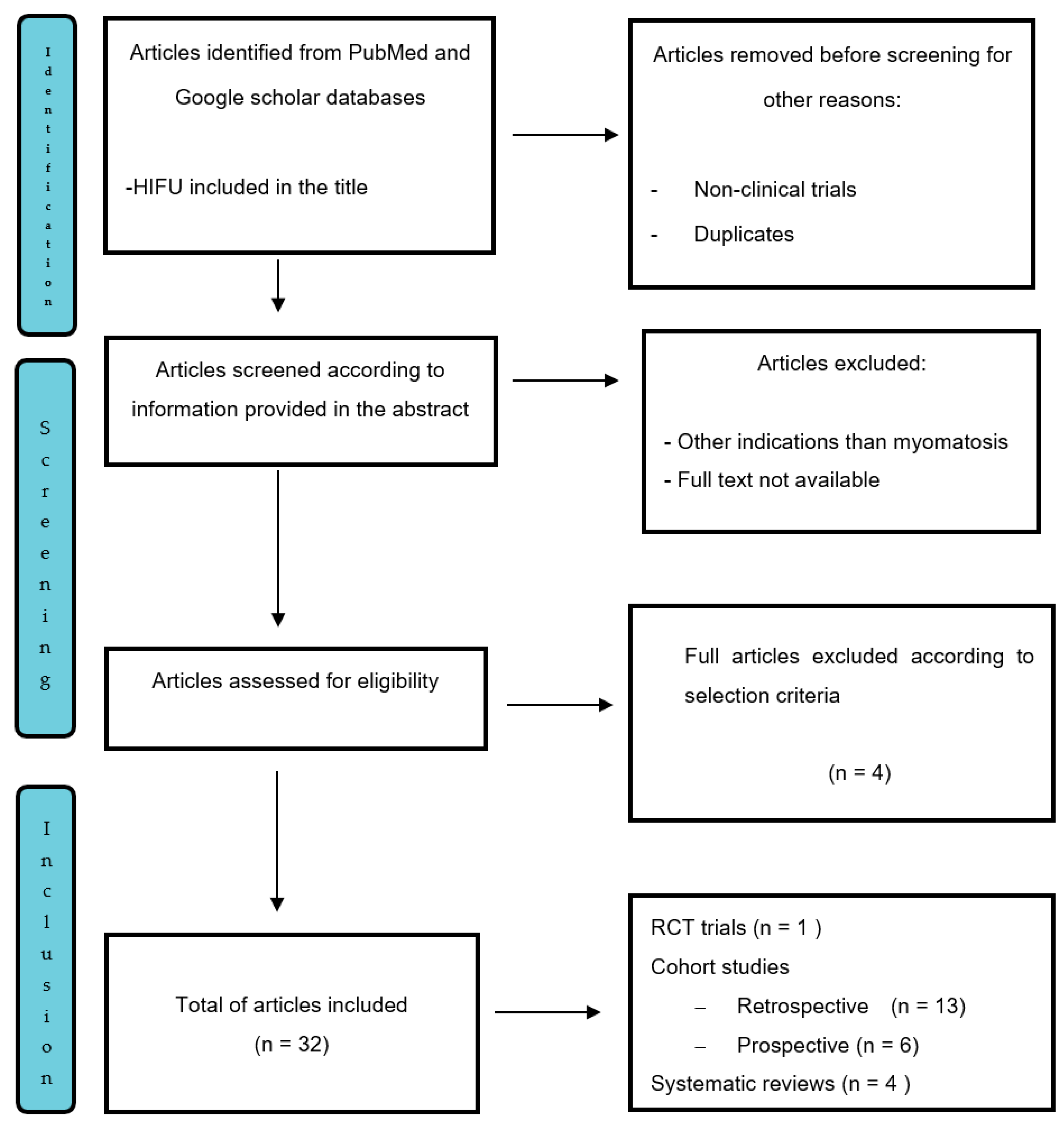
2. Materials and Methods
3. Results
3.1. Ethnicity
3.2. Non-Perfused Volume Ratio
3.3. Thickness of Abdominal Subcutaneous Tissues
3.4. Perfusion of Fibroids
3.5. Energy Efficiency Factor
3.6. Resolution of Symptoms, Quality of Life and Hospital Stay

{kind=link}
{kind=link}
| Author [Ref] | UFS before Therapy | UFS after Therapy | p-Value | QoL Score before Therapy | QoL Score after Therapy | p-Value |
|---|---|---|---|---|---|---|
| Jeng CJ et al., 2020 [3] | 63.9 ± 29.9 | 45.3 ± 26.9 | 0.000 | NA | ||
| Chen J et al., 2018 [37] | HIFU: 19.89 ± 14.29 LM: 15.34 ± 13.34 | 6 months: HIFU: 10.20 ± 10.18 LM: 7.09 ± 8.25 | 0.000 | Baseline HIFU: 72.75 ± 16.33 LM: 72.85 ± 14.46 | 6 months: HIFU 82.48 ± 12.94 LM: 80.44 ± 12.41 | 0.000 |
| 12 months: HIFU: 7.73 ± 9.65, MYO: 5.77 ± 7.77 | NA | 12 months: HIFU: 85.84 ± 12.22 LM: 83.45 ± 11.28 | 0.000 | |||
| Cheung VYT et al., 2019 [14] | USgHIFU: 27 (21–33) | 3 months: 16.5 (11–23) | 0.0001 | NA | ||
| 6 months: 16 (8–21) | 0.0002 | |||||
| 12 months: 14.5 (8–30) | 0.0002 | |||||
| Wang Y et al., 2020 [15] | tSSS: 34 (10–60) | tSSS: 40 (12–66) | 0.178 | |||
| Laughlin-Tommaso SL et al., 2020 [16] | MRgHIFU: 53.9 (19.8) | 6 months MRgHIFU: 31.3 (18.7) | <0.001 | 77.0 QoL score | <0.001 | |
| UAE: 53.1(19.8) | UAE:13.2 (10.2) | 91.2 QoL score | ||||
| 12 months: MRgHIFU:34.1 (24.7) | <0.001 | 72.8 QoL score | <0.001 | |||
| UAE:13.8 (12.8) | 93.0 QoL score | |||||
| He M et al., 2018 [17] | 56.3 ± 16.7 | 1 months: 40.5 ± 17.2 | NA | 41.3 ± 21.2 | 1 month: 60.6 ± 19.7 | NA |
| 3 months: 31.0 ± 15.1 | NA | 3 months: 72.3 ± 18.1 | ||||
| 6 months: 20.6 ± 14.2 | NA | 6 months: 73.4 ± 19.2 | ||||
| Lee JY et al., 2019, JY [18] | USgHIFU 93.1 ± 32.5 | 72.6 ± 26.6 | 0.0001 | |||
| Verpalena IM et al., 2019 [32] | MRgHIFU 46.1 (33.7–58.4) | NA | 6-months: 56.1 (50.0–62.2) | NA | ||
| NA | 12-months: 53.6 (41.8–65.5) | NA | ||||
| Lozinski T et al., 2021 [19] | NA | 3 months: NA 6 months: 87.44 ± 1.96% | NA | NA | 3 months: Better 61% Much better: 8% 6 months: Better: 53% Much better: 23% | NA |
3.7. Adverse Events
| Author [Ref] | Minor Adverse Event | (%) |
|---|---|---|
| Jeng CJ et al., 2020 [3] | Vaginal secretion | 0.086 |
| Low abdominal pain | 0.022 | |
| Leg and buttock pain | 0.0072 | |
| Hematuria | 0.0053 | |
| Uterine bleeding | 0.0022 | |
| Blurred vision | 0.0001 | |
| He M et al., 2017 [17] | Transient leg pain | 0.13 |
| Buttock pain | 0.43 | |
| Skin burning sensation | 0.61 | |
| Lower abdominal pain | 0.60 | |
| Abnormal vaginal discharge | 0.6 | |
| Cheung VYT et al., 2019 [14] | Second degree skin burn | 0.05 |
| Urinary tract infection | 0.05 | |
| Pelvic and back pain | 0.35 | |
| Intense lower abdominal pain | 0.05 | |
| Yin N et al., 2018 [13] | Lower abdominal pain | 0.38 |
| Buttock pain | 0.19 | |
| Vaginal bleeding and discharge | 0.16 | |
| Lower limb paresthesia | 0.048 | |
| Urinary retention | 0.003 | |
| Fever | 0.006 | |
| Hematuria | 0.0056 | |
| Chen J et al., 2017 [37] | Lumbar and back pain | 0.011 |
| Numbness and pain in lower limb | 0.025 | |
| Weakness in lower limb | 0.0066 | |
| Pain and distension of anus | 0.008 | |
| Uterine bleeding | 0.065 | |
| Urinary retention | 0.0015 | |
| Hematuria | 0.002 | |
| Fever | 0.0012 | |
| Respiratory tract infection | 0.0007 | |
| Skin burn (1st and 2nd degree) | 0.0012 | |
| Nausea and vomiting | 0.0155 | |
| Dizziness and headache | 0.0014 | |
| Blurred vision | 0.0073 | |
| Zhang CHJ et al., 2017 [4] | Lower abdominal pain | 0.69 |
| Sciatic/buttock pain | 0.57 | |
| Skin burns | 0.38 | |
| Transient leg pain | 0.34 | |
| Vaginal bleeding after HIFU | 0.15 | |
| Lozinski T et al., 2021 [19] | Abdominal pain | 4.16 |
| Low-grade fever Flu-like symptomsmalaise, chills | 2.43 | |
| Hematuria | 2.77 | |
| Panic (claustrophobia) | 0.33 | |
| Wang Y et al., 2018 [22] | MRgHIFU: | |
| Abnormal vaginal discharge | 0.046 | |
| Lower abdominal pain | 0.069 | |
| USgHIFU | ||
| Abnormal vaginal discharge | 0.05 | |
| Lower abdominal pain | 0.039 | |
| Mild lower back pain | 0.019 |
3.8. Fibroid Volume Reduction
| Author [Ref] | Myoma Localization | Myoma Volume before Intervention Mean (cm3) | Myoma Volume Reduction Immediately after Intervention (%) | Myoma Volume Reduction Up to 6 Months (cm3) | Myoma Volume Reduction at Final Follow-Up (cm3) |
|---|---|---|---|---|---|
| Jeng CJ et al., 2020 [3] | Posterior wall 34.7% | 193.9 ± 458.0 | NA | 118.7 ± 240.0 at 3 months | 40.2 ± 21.6 cm3 at 3 months |
| Anterior wall 35.7% | NA | NA | |||
| Fundal 8.7% | NA | NA | |||
| Anterior and posterior wall 20.9% | NA | NA | |||
| Cheung VYT et al., 2019 [37] | Not categorized | 127.0 (18.5–481.2) | 79.8 % (6.6–271.7) at 1 month | 46.9% (8.8–73.1) at 1 month | 75.9% (33.7–99.3) at 12 months |
| He M et al., 2018 [17] | Anterior 127 cases | 1.8–1220.1 | NA | 32.5 ± 24.0% at 1 month | NA |
| Posterior 72 cases | 52.5 ± 36.3%, at 6 months | ||||
| Lateral 67 cases | |||||
| Fundal 80 cases | |||||
| Lee JY et al., 2019 [18] | Anterior 19 cases Posterior 10 case Lateral 14 cases Fundus 10 cases | 5.3 ± 1.5 | NA | 17.3 ± 30.0% at 1 month 33.3 ± 19.3% at 3 months (1st trial) 45.1 ± 25.5% at 5 months (2nd trial) | 33.3 ± 19.3% at 3 months (1st trial) 45.1 ± 25.5% at 5 months (2nd trial) |
| Lozinski T et al., 2021 [19] | 113.18 ± 1.96 | NA | 3 months: 27% | 6 months: 39% |
3.9. Reintervention
| Author | HIFU Cases (n) | Re-Intervened (%) | Reintervention Interval (Months) | Reasons (%) | Further Procedure |
|---|---|---|---|---|---|
| Wang Y et al., 2020 [15] | 245 | 24 (9.80%) | 78 | Symptoms recurred | Myomectomy (n = 8) |
| Hysterectomy (n = 8) | |||||
| HIFU (n = 5) | |||||
| Hormone treatment (n = 3) | |||||
| Li W et al., 2020 [23] | 381 | 79 (20.73%) | 33.7 ± 18.0 | Symptomatic recurred, 63.3% | Myomectomy (n = 46) |
| Psychological factors, 17.7% | Hysterectomy (n = 30) | ||||
| Fertility requirement, 3.8% | USgHIFU (n = 3) | ||||
| Suspected uterine sarcoma, 2.5% | |||||
| Others, 10% | |||||
| He M et al., 2018 [17] | 132 | 2 (1.51%) | 6 | Menstrual bleeding | Myomectomy |
| Cheung VYT et al., 2019 [14] | 20 | 3 (12%) | 10–12 | Symptoms recurred | Myomectomy |
3.10. Pregnancy Outcome
| Author | Approach (n) | Follow Up Duration | Time to Conceive (Months) | No. of Pregnancies | No. of Deliveries | SVD (n) | CS (n) | Complications |
|---|---|---|---|---|---|---|---|---|
| Wu G et al., 2020 [25] | USgHIFU: 219 | 1–8 years | USgHIFU: 13.6 ± 9.5 | USgHIFU: 248 | USgHIFU: 178 | USgHIFU: 91 | USgHIFU: 74 | Fetal distress: USgHIFU: 2.8% LM 1.2% p = 0.468 |
| LM: 224 | LM: 18.9 ± 7.3 | LM: 253 | LM: 173 | LM: 63 | LM: 95 | Fetal growth restriction: USgHIFU: 2.2% LM:0.6%, p = 0.385 | ||
| Large infant: USgHIFU: 7.9% LM: 5.8%, p = 0.439 | ||||||||
| Placental abruption: USgHIFU: 3.9%, LM: 4.6%, p = 0.74 | ||||||||
| Placenta increta: USgHIFU: 1.1%, LM: 6.4%, p = 0.009 | ||||||||
| Placenta previa: USgHIFU: 2.8%, LM: 8.7%, p = 0.018 | ||||||||
| Uterine rupture: USgHIFU: 0.6%, LM: 0.6%, p = 1.000 | ||||||||
| Jeng CJ et al., 2020 [3] | 546 | 3–38 months | NA | 12 | 5 | 3 | 2 | NA |
| Liu X et al., 2018 [26] | 174 | 76 months | 16 (1–66) | 88 | Not available | 37 | 37 | Placenta previa: 1 |
| Pregnancy induced hypertension: 1 | ||||||||
| Fetal intrauterine growth retardation: 1 | ||||||||
| Low birth weight: 2 | ||||||||
| Malpresentation: 4 | ||||||||
| Postpartum hemorrhage: 2 | ||||||||
| He M et al., 2018 [17] | 1 | 6 months | 3 | 1 | 1 | 1 | 0 | NA |
| Liu L et al., 2020 [8] | 157 | 6–61.9 months | NA | 18 | NA | NA | NA | NA |
| Anneveldt KJ et al., 2021 [35] | MRgHIFU: 114 | 6 months | MRgHIFU: 0–30 | MRgHIFU: 124 | MRgHIFU: 90 | MRgHIFU: 71 | MRgHIFU: 19 | Placenta previa: MRgHIFU: 2/124 USgHIFU: 6/266 |
| USgHIFU: 325 | 1–8 years | USgHIFU: 1–66 | USgHIFU: 336 | USgHIFU: 248 | USgHIFU: 64 | USgHIFU: 184 | Still births: MRgHIFU: 0 USgHIFU: 1 |
3.11. Risk of Uterine Sarcoma
4. Discussion
5. Key Points to Consider in Clinical Practice
- Localization, size and benign radiological appearance of the uterine masses are accurately assessed prior to ablation. It is more difficult to ablate myomata with long distance from its ventral side to skin, in retroverted uterus, significant enhancement on T1WI, hyperintensity SI on T2WI (MRI), small size, transmural type and posterior location;
- Myoma perfusion (volume blood flow and velocity) is evaluated before procedure, e.g., by contrast enhanced ultrasound. The higher the perfusion, the higher the resistance towards ablation;
- Beam intensity and total treatment time is modulated according to myoma characteristics and subcutaneous abdominal fat thickness. Obese patients are at a higher risk of thermal damage in abdominal wall structures;
- An adequate acoustic window is assured before ablation. Bowel injuries can occur when the bowel is in the acoustic pathway or when fibroids are over treated;
- Patients presenting recurrent symptomatic uterine fibroids after myomectomy benefit from ablation. Most of them do not require further surgery;
- Patients are informed that discharged necrotic tissue will appear in the first cycle after therapy and resolve spontaneously within six to eight months;
- Patients are informed that fibroid volume shrinkage is achieved months after first ablation (mean 6 m);
- Patients are informed that reintervention is mostly required in younger women, when baseline anti-müllerian hormone level is >0.3 ng/mL or when fibroma volume is >300 cm3;
- Patients seeking to be pregnant are informed that average times to pregnancy are longer than after myomectomy, but pregnancy outcomes are similar and caesarean section as mode of delivery is not mandatory;
- Patients undergoing USgHIFU are informed that radiologist and sedation are not mandatory, therefore they give feedback to the physician about pain during procedure eventually to relocate the beam or to modulate its intensity;
- Patients are informed about potential AE, such as skin redness, abdominal pain or discomfort and sciatic nerve paresthesia or simply leg pain, skin burn, and in very seldom cases, nearby organs injury;
- Close follow-up of patient regarding the risk of development of a uterine sarcoma, as the uterine fibroids are not previously sampled for a histological diagnosis.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Wang, Y.; Zhang, S.; Li, C.; Bo, L.; Ouyang, L. Minimally invasive surgery for uterine fibroids. Ginekol. Pol. 2020, 91, 149–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izadifar, Z.; Chapman, D.; Babyn, P. An introduction to high intensity focused ultrasound: A systematic review on principles, devices and clinical applications. J. Clin. Med. 2020, 9, 460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeng, C.J.; Ou, K.Y.; Long, C.Y.; Chuang, L.; Ker, C.R. 500 cases of high intensity focused ultrasound HIFU ablated uterine fibroids and adenomyosis. Taiwan J. Obstet. Gynecol. 2020, 59, 865–871. [Google Scholar] [CrossRef]
- Zhang, C.H.J.; Ngobese, Z.E.; Setzen, Z. Efficacy and safety of ultrasound guided high intensity focused ultrasound ablation of symptomatic uterine fibroids in black women: A preliminary study. BJOG 2017, 124, 36–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duc, N.M.; Huy, Q.H.; Keserci, B. Adverse events of focused ultrasound surgery for uterine fibroids and adenomyosis. Rep. Med. Imaging 2018, 11, 15–26. [Google Scholar]
- Liu, Y.; Ran, W.; Shen, Y.; Feng, W.; Yi, J. High intensity focused ultrasound and laproscopic myomectomy in the treatment of uterine fibroids: A comparative study. BJOG 2017, 124, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Geng, J.; Bao, H.; Dong, J.; Shi, J.; Xi, Q. Comparative effectiveness and safety of high intensity focused ultrasound for uterine fibroids: A meta analysis. Front. Oncol. 2021, 11, 484. [Google Scholar]
- Liu, L.; Wang, T.; Lei, B. Uterine artery embolization compared with high intensity focused ultrasound ablation for the treatment of symptomatic uterine myomas: A systemic review and meta analysis. JMIG 2020, 28, 218–227. [Google Scholar] [CrossRef]
- Torres-de la Roche, L.A.; Becker, S.; Cezar, C.; Hermann, A.; Larbig, A.; Leicher, L.; Di Spiezio, S.A.; Tanos, V.; Wallwiener, M.; Verhoeven, H.; et al. Pathobiology of myomatosis uteri: The underlying knowledge to support our clinical practice. Arch Gynecol Obstet. 2017, 296, 701–707. [Google Scholar] [CrossRef]
- Suomi, V.; Komar, G.; Sainio, T.; Joronen, K.; Perheentupa, A.; Sequeiros, R.B. Comprehensive feature selection for classifying the treatment outcome of high intensity ultrasound therapy in uterine fibroids. Sci. Rep. 2019, 9, 10907. [Google Scholar] [CrossRef] [Green Version]
- Fan, H.J.; Cun, J.P.; Zhao, W.; Huang, J.Q.; Yi, G.F.; Yao, R.H.; Gao, B.L.; Li, X.H. Factors affecting effects of ultrasound guided high intensity focused ultrasound for single uterine fibroids: A retrospective analysis. Int. J. Hyperth. 2018, 35, 534–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.J.; Zhang, P.H.; Zhang, R.; An, P.L. Predictive value of Quantitative uterine fibroids perfusion parametres from contrast enhanced ultrasound for the therapeutic effect of high intensity focused ultrasound ablation. J. Ultrasound Med. 2018, 38, 1511–1517. [Google Scholar] [CrossRef] [PubMed]
- Yin, N.; Hu, L.; Xiao, Z.B.; Liu, C.; Chen, W.Z.; Roberts, N.; Chen, J.; Wang, Z.B. Factors influencing thermal injury to skin and abdominal wall structures in HIFU ablation of uterine fibroids. Int. J. Hyperth. 2018, 34, 1298–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, V.Y.T.; Lam, T.P.W.; Jenkins, C.R.; Lam, S.W.; Cheung, G.K.I.; Chan, S.S.Y.; Choi, W.K.; Cheung, I. Efficacy and safety of ultrasound-guided highintensity focused ultrasound for uterine fibroids: A preliminary experience. J. Obstet. Gynaecol. 2019, 39, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, X.; Wang, W.; Tang, J.; Song, L. Long term clinical outcomes of US-guided high intensity focused ultrasound ablation for symptomatic submucosal fibroids: A retrospective comparison with uterus sparing surgery. Acad Radiol. 2020, 28, 1102–1107. [Google Scholar] [CrossRef] [PubMed]
- Laughlin-Tommaso, S.; Barnard, E.P.; AbdElmagied, A.M.; Vaughan, L.E.; Weaver, A.L.; Hesley, G.K.; Woodrum, D.A.; Jacoby, V.L.; Kohi, M.P.; Price, T.M.; et al. FIRSTT study: Randomized controlled trial of uterine artery embolization vs. focused ultrasound surgery. Am. J. Obstet. Gynecol. 2018, 220, 174.e1–174.e13. [Google Scholar] [CrossRef]
- He, M.; Jacobson, H.; Zhang, C.; Setzen, R.; Zhang, L. A reterospective study of ultrasound guided high intensity focused ultrasound ablation for multiple uterine fibroids in South Africa. Int. J. Hyperth. 2017, 34, 1304–1310. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Choong, H.H.; Kang, S.Y.; Park, E.; Park, D.H.; Son, K.; Han, J.K. Poratble ultrasound guided high intensity focused ultrasound with functions for safe and rapid ablation: Prospective clinical trial for uterine fibroids- short term and long term results. Eur. Radiol. 2019, 34, 1554–1563. [Google Scholar]
- Lozinski, T.; Filipowska, J.; Pyka, M.; Baczkowska, M.; Ciebiera, M. Magnetic resonance-guided high-intensity ultrasound (MR-HIFU) in the treatment of symptomatic uterine fibroids—Five-year experience. Ginekol. Pol. 2021. [Google Scholar] [CrossRef]
- Liu, X.; Dong, X.; Mu, Y.; Huang, G.; HeHu, L. High intensity focused ultrasound for the treatment of uterine fibroids: Does HIFU significantly increase the risk of pelvic adhesion. Int. J. Hyperth. 2020, 37, 1027–1032. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, W.W.; He, M.; Gong, C.; Xie, B.; Wen, X.; Li, D.; Zhang, L. Adverse effect analysis of high intensity focused ultrasound in the treatment of benign uterine diseases. Int. J. Hyperth. 2018, 35, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Wang, Z.B.; Xu, Y.H. Efficacy, Efficiency, and Safety of Magnetic Resonance-Guided High-Intensity Focused Ultrasound for Ablation of Uterine Fibroids: Comparison with Ultrasound-Guided Method. Korean J. Radiol. 2018, 19, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Jiang, Z.; Deng, X.; Xu, D. Long term follow up outcome and reintervention analysis of ultrasound guided focused ultrasound treatment for uterine fibroids. Int. J. Hyperth. 2020, 37, 1046–1051. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Tang, J.; Luo, Y.; Wang, Y.; Song, L.; Wang, W. Comparison of high intensity focused ultrasound ablation and secondary myomectomy for recurrent symptomatic uterine fibroids following myomectomy: A retrospective study. Bjog 2020, 127, 1422–1428. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Li, R.; He, M.; Pu, Y.; Wang, J.; Chen, J.; Qi, H. A comparison of the preganancy outcomes between ultrasound guided high intensity focused ultrasound ablation and laproscopic myomectomy for uterine fibroids: A comaparative study. Int. J. Hyperth. 2020, 37, 617–623. [Google Scholar] [CrossRef]
- Liu, X.; Xue, L.; Wang, Y.; Wang, W.; Tang, J. Vaginal delivery outcomes of pregnancies following ultrasound guided high intensity focused ultrasound ablation treatment for uterine fibroids. Int. J. Hyperth. 2018, 35, 510–517. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Wu, X.; Zhu, X.; Wang, J.; Xu, F.; Lin, Z.; Gong, C.; He, M.; Zhang, L. MRI features and clinical outcomes of unexpected uterine sarcomas in patients who underwent high intensity focused ultrasound ablation for presumed uterine fibroids. Int. J. Hyperth. 2021, 38, 39–45. [Google Scholar] [CrossRef]
- Jeng, C.J.; Long, C.Y.; Chuang, L. Comparison of magnetic resonance guided high intensity focused ultrasound with uterine artery embolization for the treatment of uterine myomas: A systemic literature review and meta-analysis. Taiwan J. Obstet. Gynecol. 2020, 59, 691–697. [Google Scholar] [CrossRef]
- Yu, L.; Zhu, S.; Zhang, H.; Wang, A.; Sun, G.; Liang, J.; Wang, X. The efficacy and safety of MRgHIFU and US-HIFU in treating uterine fibroids with volume <300 cm3: A metanalysis. Int. J. Hyperth. 2021, 38, 1126–1132. [Google Scholar] [CrossRef]
- Torkzaban, M.; Machado, P.; Gupta, I.; Forsberg, F.; Hai, Y. Contrast-Enhanced Ultrasound For Monitoring Non-Surgical Treatments Of Uterine Fibroids: A Systematic Review. Ultrasound Med. Biol. 2020, 47, 3–18. [Google Scholar] [CrossRef]
- Sandberg, E.M.; Tummers, F.H.M.P.; Cohen, S.L.; Haak, L.V.D.; Dekkers, O.M.; Jansen, F.W. Reintervention risk and quality of life outcomes after uterine sparing interventions for fibroids: A systemic review and meta-analysis. Fertil. Steril. 2018, 109, 698–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verpalena, I.M.; Anneveldt, K.J.; Nijholta, I.M.; Schutteb, J.M.; Dijkstrab, J.R.; Franxd, A.; Bartelse, L.W.; Moonene, C.T.W.; Edensc, M.A.; Boomsma, M.F. Magnetic resonance-high intensity focused ultrasound (MR-HIFU) therapy of symptomatic uterine fibroids with unrestrictive treatment protocols: A systematic review and meta-analysis. Eur. J. Radiol. 2019, 120, 108700. [Google Scholar] [CrossRef]
- Xu, F.; Deng, L.; Zhang, L.; Hu, H.; Shi, Q. The comparison of myomectomy, UAE and MRgFUS in the treatment of uterine fibroids: A metaanalysis. Int. J. Hyperth. 2021, 38, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Taheri, M.; Galo, L.; Potts, C.; Sakhel, K.; Quinn, D.S. Nonresective treatments for uterine fibroids: A systematic review of uterine and fibroid volume reductions. Int. J. Hyperth. 2019, 36, 294–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anneveldt, K.J.; van ’t Oever, H.J.; Nijholt, I.M.; Dijkstra, J.R.; Hehenkamp, W.J.; Veersema, S.; Huirne, J.A.F.; Schutte, J.M.; Boomsma, M.F. Systematic review of reproductive outcomes after high intensity focused ultrasound treatment of uterine fibroids. Eur. J. Radiol. 2021, 141, 109801. [Google Scholar] [CrossRef]
- Duc, N.M.; Keserci, B. Review of influential clinical factors in reducing the risk of unsuccessful MRI guided HIFU treatment outcome of uterine fibroids. Diagn Interv Radiol. 2018, 24, 283–291. [Google Scholar] [CrossRef]
- Chen, J.; Li, Y.; Wang, Z.; McCulloch, P.; Hu, L.; Chen, W.; Liu, G.; Li, J.; Lang, J. Evaluation of high-intensity focused ultrasound ablation for uterine fibroids: An IDEAL prospective exploration study. Bjog 2018, 125, 354–364. [Google Scholar] [CrossRef] [Green Version]
- Qu, K.; Mao, S.; Li, J.; Wang, J.; Ouyang, G.; Wang, Z.; Wang, Z.; Xiong, Y.; Zhang, L. The impact of ultrasound-guided high-intensity focused ultrasound for uterine fibroids on ovarian reserve. Int. J. Hyperth. 2020, 37, 399–403. [Google Scholar] [CrossRef]
- Li, J.; Chen, X.; Hu, H. High-intensity focused ultrasound for treatment of recurrent uterine leiomyosarcoma: A case report and literature review. J. Int. Med. Res. 2020, 48, 0300060520942107. [Google Scholar] [CrossRef]
- Prachee, I.; Wu, F.; Cranston, D. Oxford’s clinical experience in the development of high intensity focused ultrasound therapy. Int. J. Hyperth. 2021, 32, 81–88. [Google Scholar] [CrossRef]
- Gupta, J.K.; Sinha, A.; Lumsden, M.A.; Hickey, M. Uterine artery embolization for symptomatic uterine fibroids. Cochrane Database Syst. Rev. 2014, 26, CD005073. [Google Scholar] [CrossRef] [Green Version]
- Togioka, B.M.; Tonismae, T. Uterine Rupture. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA.
- Gambacorti-Passerini, Z.M.; Penati, C.; Carli, A.; Accordino, F.; Ferrari, L.; Berghella, V.; Locatelli, A. Vaginal birth after prior myomectomy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 231, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Bohlmann, M.K.; Hoellen, F.; Hunold, P.; David, M. High-Intensity Focused Ultrasound Ablation of Uterine Fibroids—Potential Impact on Fertility and Pregnancy Outcome. Geburtshilfe Frauenheilkd. 2014, 74, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-López, F.R.; Ornat, L.; Ceausu, I.; Depypere, H.; Erel, C.T.; Lambrinoudaki, I.; Schenck-Gustafsson, K.; Simoncini, T.; Tremollieres, F.; EMAS; et al. EMAS position statement: Management of uterine fibroids. Maturitas 2014, 79, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Vilos, G.A.; Vilos, A.; Abu-Rafea, B.; Leyland, N.; Allaire, C.; Laberge, P.Y.; Murji, A.; Singh, S.S.; Thiel, J. Interventional Uterine-Sparing Therapies for Leiomyomas: A Commentary on Myolysis. J. Obstet. Gynaecol. Can. 2020, 42, 169–172. [Google Scholar] [CrossRef] [PubMed]


| Author [Ref] | Study Design | Level of Evidence | Country | Population No. of Patients/Ethnicity | Age of Participants (Years Old) |
|---|---|---|---|---|---|
| Jeng CJ et al., 2020 [3] | Retrospective, cross-sectional | II b | Taiwan | Myomatosis: 404, Adenomyosis: 149 | 40.7 ± 5.9 |
| Zhang C et al., 2017 [4] | Retrospective non comparative | II b | South Africa | 26 Black | 34.4 ± 6.2 |
| Liu Y et al., 2017 [6] | Prospective comparative | II b | China | HIFU: 99, LM: 67 | >20 |
| Suomi V et al., 2019 [10] | Retrospective, non comparative | II b | Finland | 89; White: 80, Black: 6, Asian: 3 | 26–51 |
| Fan HJ et al., 2018 [11] | Retrospective, non comparative | II b | China | 207 | 18–55 |
| Wang YJ et al., 2018 [12] | Retrospective, non comparative | II b | China | 263 | 38.2 ± 5.6 |
| Yin N et al., 2018 [13] | Prospective, non comparative | II b | China | 892 | 39.1 ± 6.4 |
| Cheung VYT et al., 2019 [14] | Prospective, non comparative | II b | Hong Kong | 20 | >40 |
| Wang Y et al., 2020 [15] | Retrospective, comparative | II b | China | HIFU: 245, Uterus sparing surgery: 129 | 25–52; 23–53 |
| Laughlin-Tommaso S et al., 2019 [16] | Randomized control trial | I b | USA | MRgHIFU: 43, UAE: 40 | 44.4 |
| He M et al., 2017 [17] | Retrospective, comparative | II b | South Africa | 176 | 35.3 ± 5.9 |
| Lee JY et al., 2019 [18] | Prospective non comparative | II b | Korea | 36 | 44.9 ± 28.6 |
| Lozinski T et al., 2021 [19] | Prospective non comparative | II b | Poland | 288 | 36.6 ± 5.3 |
| Liu X et al., 2020 [20] | Retrospective, comparative | II b | China | 96 | 39.15 ± 5.46 |
| Liu Y et al., 2018 [21] | Retrospective, non comparative | II b | China | 17402 | 37–45 |
| Wang Y et al., 2018 [22] | Prospective, comparative | II b | China | MRgHIFU: 3 USgHIFU: 51 | 41.6 ± 5.5, 38.6 ± 7.0 |
| Li W et al., 2020 [23] | Retrospective, non comparative | II b | China | 381 | 40.7 ± 5.1 |
| Liu X et al., 2020 [24] | Retrospective, comparative | II b | China | 188 | 39.3 ± 5.9 |
| Wu G et al., 2020 [25] | Retrospective, comparative | II b | China | HIFU: 320 LM:336 | 22–42 |
| Liu X et al., 2018 [26] | Prospective non comparative | II b | China | 81 | 31.1 ± 3.8 |
| Wang Q et al., 2021 [27] | Retrospective non comparative | II b | China | 15,759 | 40–47 |
| Author [Ref] | Design/ (No. of Studies Included) | Objective | No. of Cases | Age | Results |
|---|---|---|---|---|---|
| Jeng CJ et al., 2020 [28] | Systematic review (4) | Comparison MRgHIFU with UAE for treatment of uterine myomata | HIFU: 207 UAE: 201 | NA | Symptom severity score: I2 = 65.1%; Cochran Q = 5.7; p = 0.057 QoL: I2 = 0%; Cochran Q = 0.7; p = 0.697 Reintervention rate: I2 = 48.8%; Cochran Q: 5.9; p = 0.119 AE: I2 = 62.5%; Cochran Q = 5.3; p = 0.069 |
| Yu L et al., 2021 [29] | Meta-analysis (48) | Efficacy and safety of MRgHIFU and USgHIFU in treatment of uterine fibroids with volume <300 cm3 | MRgHIFU: 2179 USgHIFU: 4068 | NA | mean NPVR: MRgHIFU: 58.92% (95% CI: 46.94–70.89), USgHIFU: 81.07% (95% CI: 77.61–84.53) mean treatment time: MRgHIFU: 178.19 min (95% CI: 140.24–216.15), USgHIFU: 96.9 min (95% CI: 82.20–111.60) Skin thermal injury: USgHIFU: 14.4% (95% CI: 7.3–21.5), MRgHIFU: 4.5% (95% CI: 2.5–6.4), Sciatic nerve pain: MRgHIFU: 8.9% (95% CI: 3.8–12.3), USgHIFU: 15.7% (95% CI: 8.2–23.3), Abdominal pain: MRgHIFU: 37.0% (95% CI: 21.9–52.2), USgHIFU: 31.2% (95% CI: 21.2–41.1), Abnormal vaginal discharge: MRgHIFU: 20.3% (95% CI: 9.2–31.3), USgHIFU: 11.3% (95% CI: 7.7–14.9) Reduction rate of UF: USgHIFU: 3 mo: 42.42% (95% CI: 30.66–54.17), 6 mo: 58.72% (95% CI: 52.26–65.17), 12 mo: 65.55% (95% CI: 49.54–81.56), MRgHIFU: 3 mo: 34.79% (95% CI: 30.76–38.83), 6 mo: 37.79% (95% CI: 26.71–49.23), 12 mo: 36.44% (95% CI: 24.49–48.38). One year reintervention rate: MRgHIFU: 13.4% (95% CI: 5.4–21.4), USgHIFU: 5.2% (95% CI: 2.0–8.4) |
| Wang Y et al., 2021 [7] | Meta-analysis (18) | Compare effectiveness and safety of HIFU with myomectomy and hysterectomy | 33.60–46.54 | Rate of reintervention: HIFU vs. UAE (pooled OR: 11.99, 95% CI: 5.17–27.83, p < 0.01), HIFU vs. MYO (pooled OR: 4.05, 95% CI: 1.82–8.99, p < 0.01), Incidence of abnormal pregnancy: HIFU vs. UAE: (OR: 1.20, 95% CI: 0.42–3.40, p = 0.73), HIFU vs. MYO: (pooled OR: 0.82, 95% CI: 0.46–1.46, p = 0.50). Change of serum sex hormones: HIFU vs. UAE: FSH (MD: −0.20, 95% CI: −0.91–0.51, p = 0.58), LH (MD: 0.10, 95% CI: −0.55–0.75, p = 0.76), and E2 (MD: −1.00, 95% CI: −7.42–5.42, p = 0.76) Days of hospital stay: HIFU vs. MYO: (pooled MD: −4.70, 95% CI: −7.46–1.94, p < 0.01), HIFU vs. HYS: (MD: −6.90, 95% CI: −7.24–6.56, p < 0.01). | |
| Liu L et al., 2020 [8] | Meta-analysis (7) | To compare the clinical effects of uterine artery embolization (UAE) with those of high-intensity focused ultrasound (HIFU) ablation for the treatment of symptomatic uterine fibroids | HIFU: 227 UAE: 4365 | HIFU: 36.1–44.0 UAE: 41.2–46.0 | Change in UFS score 12 months: MD or RR (95% CI), UAE vs. HIFU:19.54 (15.21–23.87), p < 0.001, I2: 0% Changes in QoL score at 12 months: MD or RR (95% CI), UAE vs. HIFU: 15.72 (8.30–23.13), p < 0.001, I2: 73% |
| Adverse events: MD or RR (95% CI), UAE vs. HIFU: 3.42 (0.07–158.04), p = 0.53, I2 = 86% Pregnancy rate: MD or RR (95% CI), UAE vs. HIFU: 0.06 (0.01–0.45), p = 0.006, I2: 0% reintervention rates: MD or RR (95% CI), UAE vs. HIFU: 0.25 (0.15–0.42), p < 0.001, I2: 52% | |||||
| Torkzaban M et al., 2020 [30] | Systematic review (17) | Clinical application and safety of contrasted enhanced ultrasound (CEUS) | CEUS provide detailed data about fibroid volume, vascularization during and post UAE. Intraprocedural CEUS during HIFU faster volume shrinkage with less needed energy and early detection of residual tissue. | ||
| Sandberg EM et al., 2018 [31] | Meta-analysis (85) | To compare uterine sparing treatment options for fibroids in terms of reintervention risk and quality of life | Myomectomy: 17,789 UAE: 5114 Artery ligation: 8244 Laparoscopic 50 RFA: 652 MRg/USg)–HIFU: 1548 Laparo-ablation: 20 Hysteroscopy: 1741 RFA: 120 | 29.3–47.9 | Quality of life at 12 months: HIFU: 24.5 (95% CI: 90.8 to 18.1), I2: 96.9%. Reintervention risks: 60 months LM 12.2%, UAE 14.4%, HIFU 59.3% |
| Verpalena IM et al., 2019 [32] | Meta-analysis (16) | Reevaluation of effectiveness of MRgHIFU for uterine fibroids by excluding studies with restrictive protocols that no longer used | 1323 | NA | NPV: Overall (I2 = 99.38%, p = 0.000), 95% CI: 68.1% (59.9–76.0%) tSSS: Overall (I2 = 94.46%, p < 0.001), 95% CI: 43.001 (34.300, 51.701), Overall (I2 = 97.87%, p < 0.001) 95% CI: 49.265(39.989, 58.541), Overall (I2 = 75.35%, p = 0.0001) 95% CI: 59.875 (53.673, 66.078) QoL: Overall (I2 = 98.33%, p < 0.001) 31.444 (−16.275, 79,162), Overall (I2 = 99.76%, p < 0.001) 31.458 (−5.585, 68.501) Fibroid shrinkage: Overall (I2 = 82.1%, p < 0.001), 95% CI: 33.162 (27.865, 38.460), Overall (I2 = 96.8%, p < 0.001) 95% CI: 36.620 (28.942, 44.298), Overall (I2 = 0%, p = 0.0986) 95% CI: 37.742 (32.696, 42.789) AE: Overall (I2 = 79.04%, p = 0.000), 95% CI: 0.087 (0.057, 0.132) |
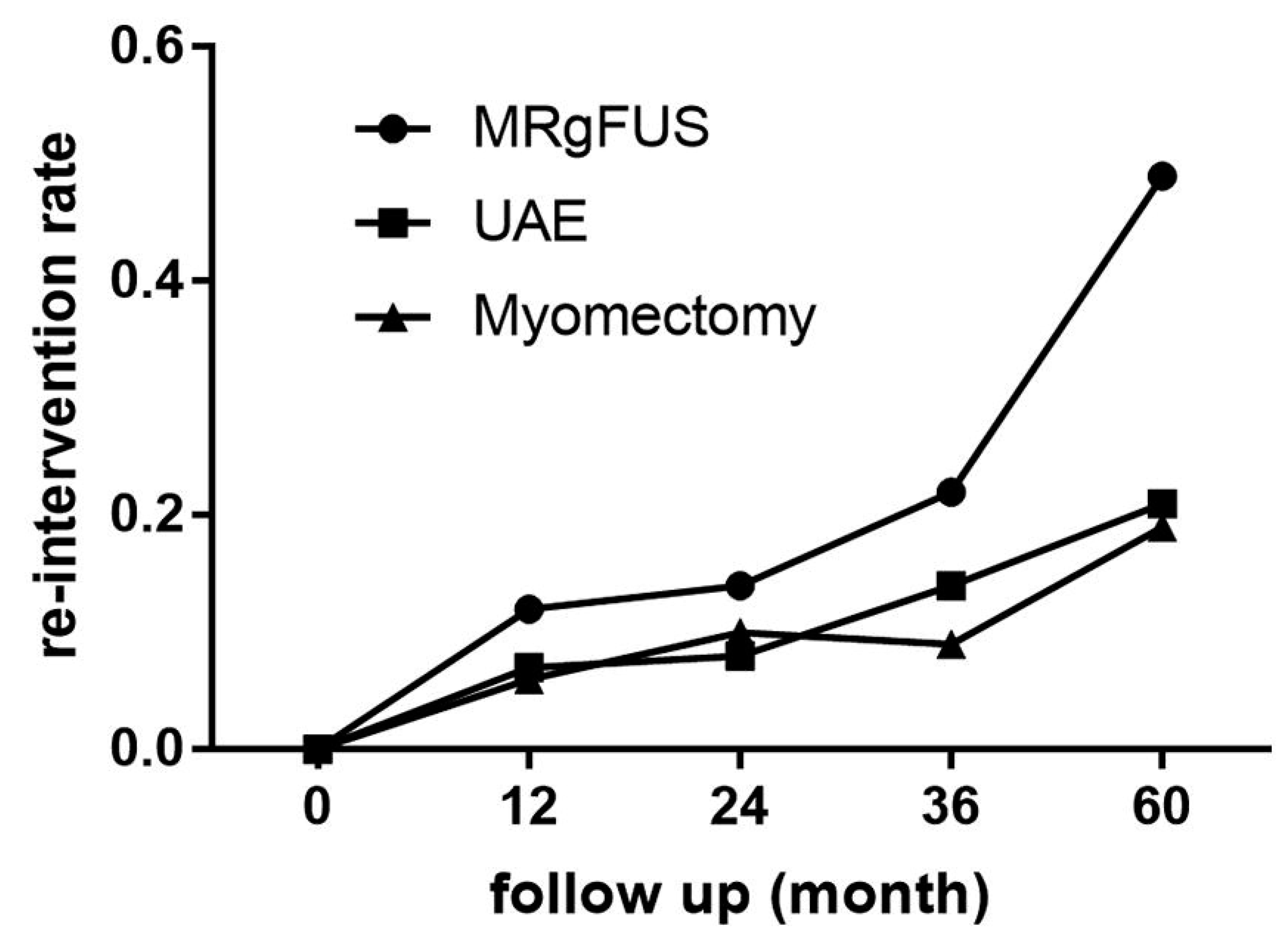
| Xu F et al., 2021 [33] | Meta-analysis (31) | Comparison of reintervention rates of myomectomy, UAE and MRgHIFU in different follow up times | 42103 | NA | Re-intervention rates: 12 months re-intervention Myomectomy: 0.06 (95% CI, 0.01–0.11; I2 = 95.1%; p = 0.000). UAE: 0.07 (95% CI, 0.06–0.09; I2 = 14.2%; p = 0.324) MRgFUS 0.12 (95% CI, 0.04–0.20; I2 = 89.1%; p = 0.000) 36-month re-intervention: MRgFUS: 0.22 (95% CI, 0.11–0.32; I2 = 86.3%; p = 0.002) UAE 0.22 (95% CI, 0.11–0.32; I2 = 86.3%; p = 0.002) myomectomy 0.09 (95% CI, 0.05–0.13; I2 = 0.0%; p = 0.508) 60-month reintervention: MRgFUS 0.49 (95% CI, 0.21–0.77; I2 = 96.5%; p = 0.000) UAE: 0.21 (95% CI, 0.17–0.25; I2 = 84.1%; p = 0.000) myomectomy: 0.19 (95% CI, 0.15–0.24; I2 = 53.7%; p = 0.071) |
| Taheri M et al., 2019 [34] | Systematic review (81) | Examines the changes in uterine and fibroid volume in UAE, HIFU and RFA | NA | 32.4–52 | Pooled mean fibroid volume reduction ± SD: UAE: 3 mo: 44% ± 9%; 6 mo: 54% ± 10%; 9 mo: 61%; 12 mo: 66% ± 10%; 24 mo: 70% ± 11% RFA: 3 mo: 55% ± 9%; 6 mo: 70% ± 5%; 9 mo: 78%; 12 mo: 75% ± 15%; 24 mo: 83% ± 8%; 36 mo: 84%10%, HIFU: 3 mo: 21% ± 6%; 6 mo: 32% ± 11%; 12 mo: 28% ± 16%; 24 mo: 34% ± 8%; 36 mo: 32% |
| Anneveldt KJ et al., 2021 [35] | Systematic review (21) | Reproductive outcomes in Mg HIFU and USgHIFU | 276 | NA | 47% pregnancy rate after 76 month f-up 90% live birth rate median time to conceive 16 months (1–66 months) 72–80% delivered by caesarian section |
| Author [Ref] | Major Adverse Events | Frequency (%) |
|---|---|---|
| Jeng CJ et al., 2020 [3] | Urinary retention | 0.001 |
| Acute renal failure | 0.0003 | |
| Bowel perforation | 0.0001 | |
| Abdominal hernia | 0.00009 | |
| Thrombocytopenia | 0.00009 | |
| Leg and buttock pain | 0.00019 | |
| Fever | 0.0004 | |
| Chen J et al., 2018 [37] | Second degree skin burn | 0.0022 |
| Liu Y et al., 2018 [28] | Skin burns | 0.149 |
| Leg pain | 0.057 | |
| Urinary retention | 0.040 | |
| Vaginal bleeding | 0.034 | |
| Hyperpyrexia | 0.028 | |
| Renal failure | 0.023 | |
| Acute cystitis | 0.017 | |
| Bowel injury | 0.017 | |
| Deep vein thrombosis | 0.115 | |
| Hydronephrosis | 0.0057 | |
| Thrombocytopenia | 0.00005 | |
| Intrauterine infection | 0.011 | |
| Liu X et al., 2020 [20] | Pelvic adhesions after HIFU | 0.43 |
| No pelvic adhesions after HIFU | 0.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torres-de la Roche, L.A.; Rafiq, S.; Devassy, R.; Verhoeven, H.C.; Becker, S.; De Wilde, R.L. Should Ultrasound-Guided High Frequency Focused Ultrasound Be Considered as an Alternative Non-Surgical Treatment of Uterine Fibroids in Non-Asiatic Countries? An Opinion Paper. J. Clin. Med. 2022, 11, 839. https://doi.org/10.3390/jcm11030839
Torres-de la Roche LA, Rafiq S, Devassy R, Verhoeven HC, Becker S, De Wilde RL. Should Ultrasound-Guided High Frequency Focused Ultrasound Be Considered as an Alternative Non-Surgical Treatment of Uterine Fibroids in Non-Asiatic Countries? An Opinion Paper. Journal of Clinical Medicine. 2022; 11(3):839. https://doi.org/10.3390/jcm11030839
Chicago/Turabian StyleTorres-de la Roche, Luz Angela, Sarah Rafiq, Rajesh Devassy, Hugo Christian Verhoeven, Sven Becker, and Rudy Leon De Wilde. 2022. "Should Ultrasound-Guided High Frequency Focused Ultrasound Be Considered as an Alternative Non-Surgical Treatment of Uterine Fibroids in Non-Asiatic Countries? An Opinion Paper" Journal of Clinical Medicine 11, no. 3: 839. https://doi.org/10.3390/jcm11030839