
Determining What Changed Japanese Suicide Mortality in 2020 Using Governmental Database


Abstract
:1. Introduction
2. Materials and Methods
2.1. Dependent and Independent Variables
2.2. Statistical Analysis
3. Results
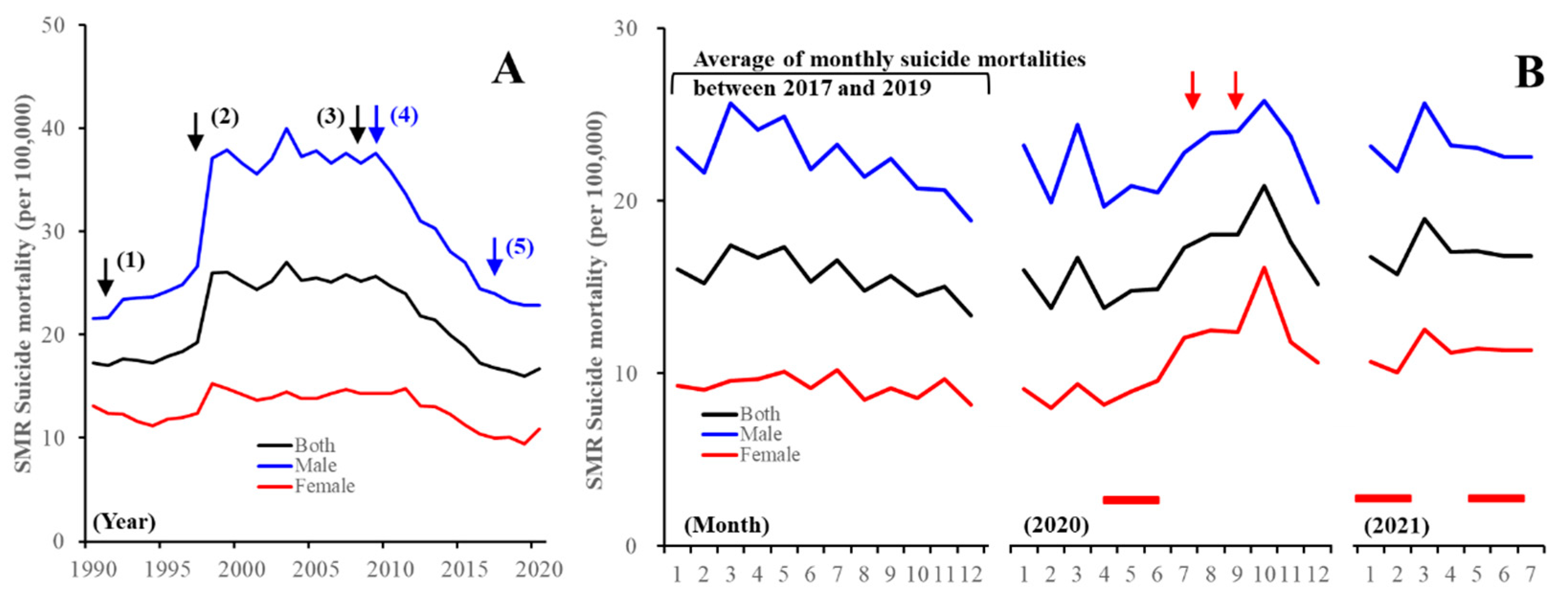
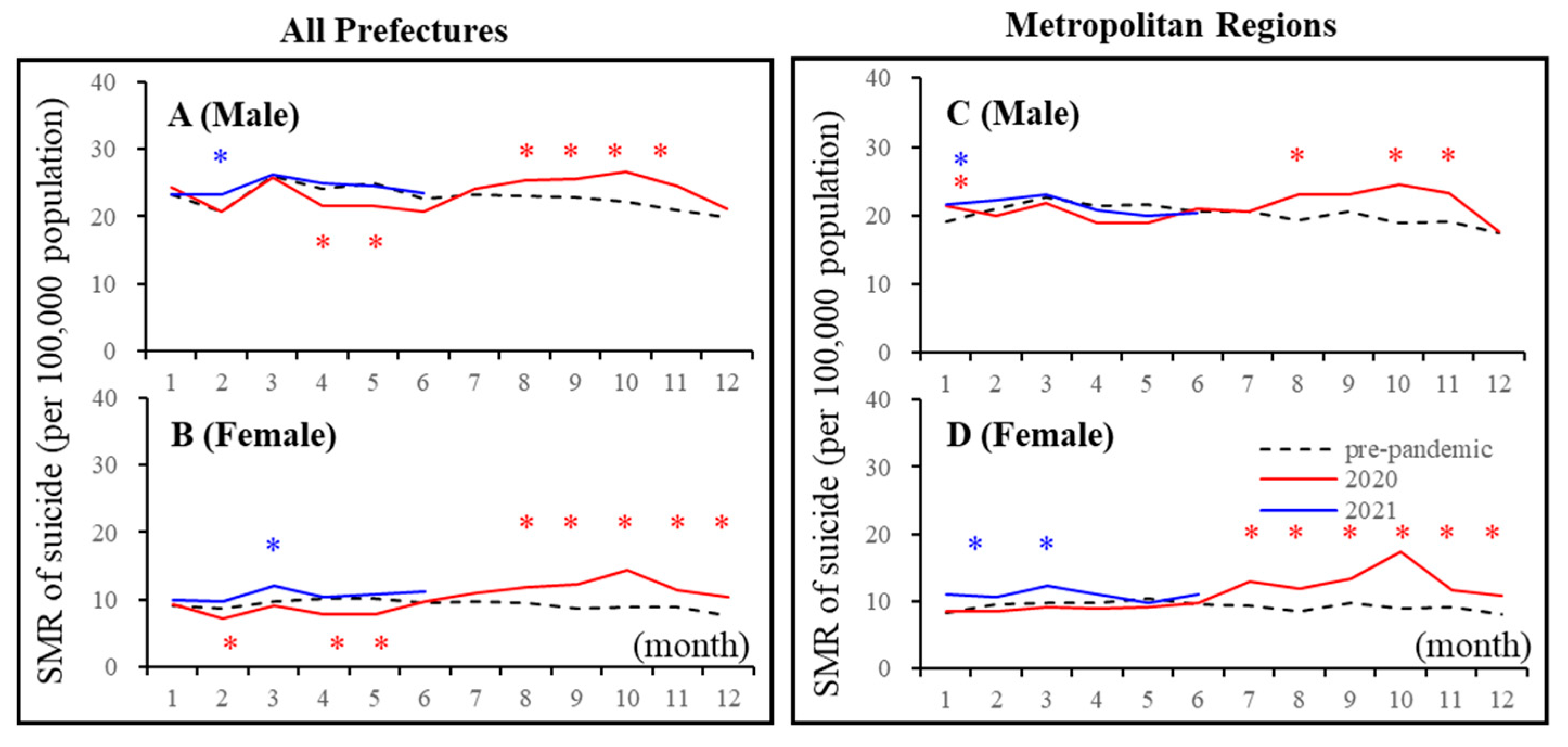
3.1. Suicide Mortality Disaggregated by Gender
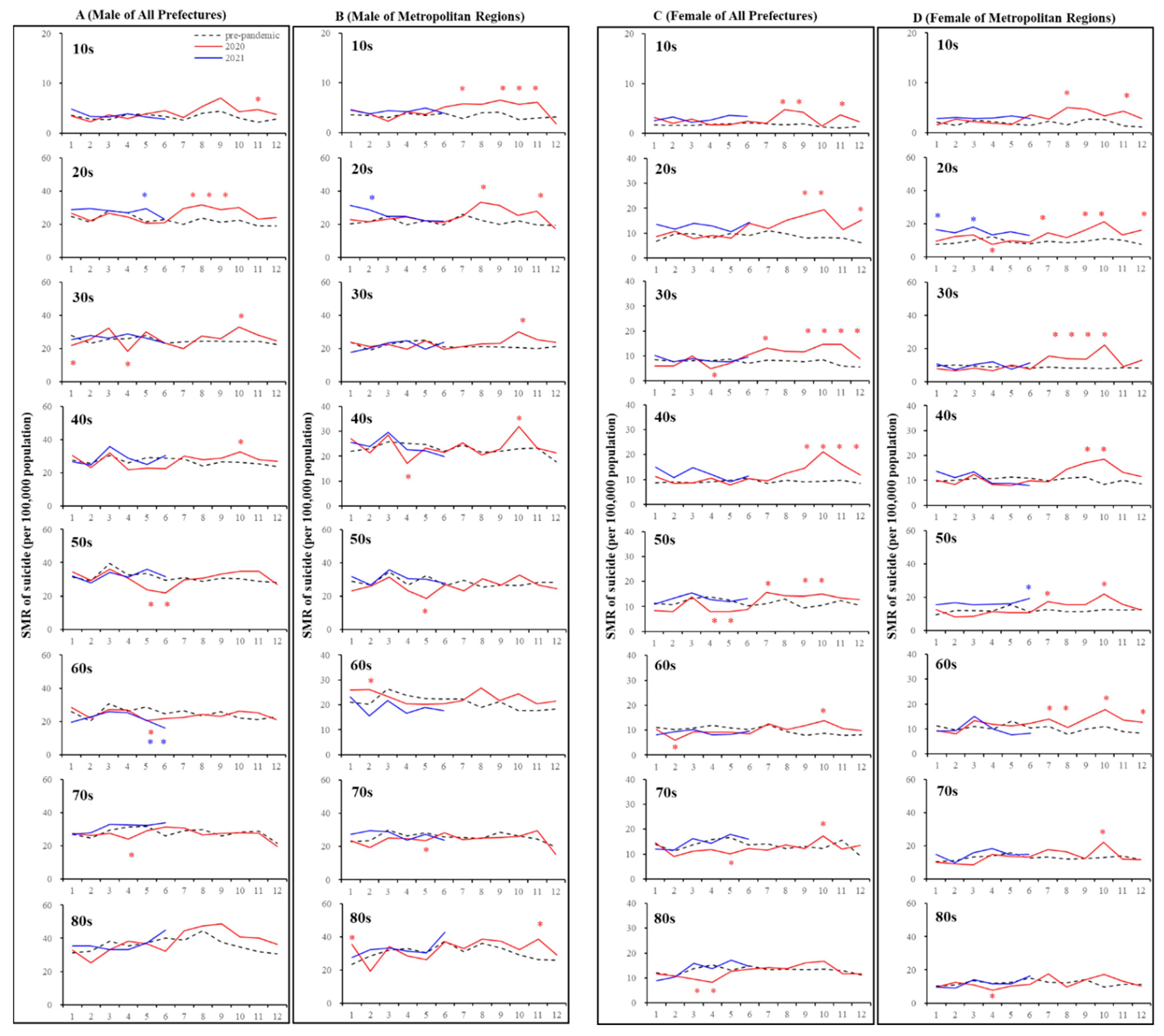
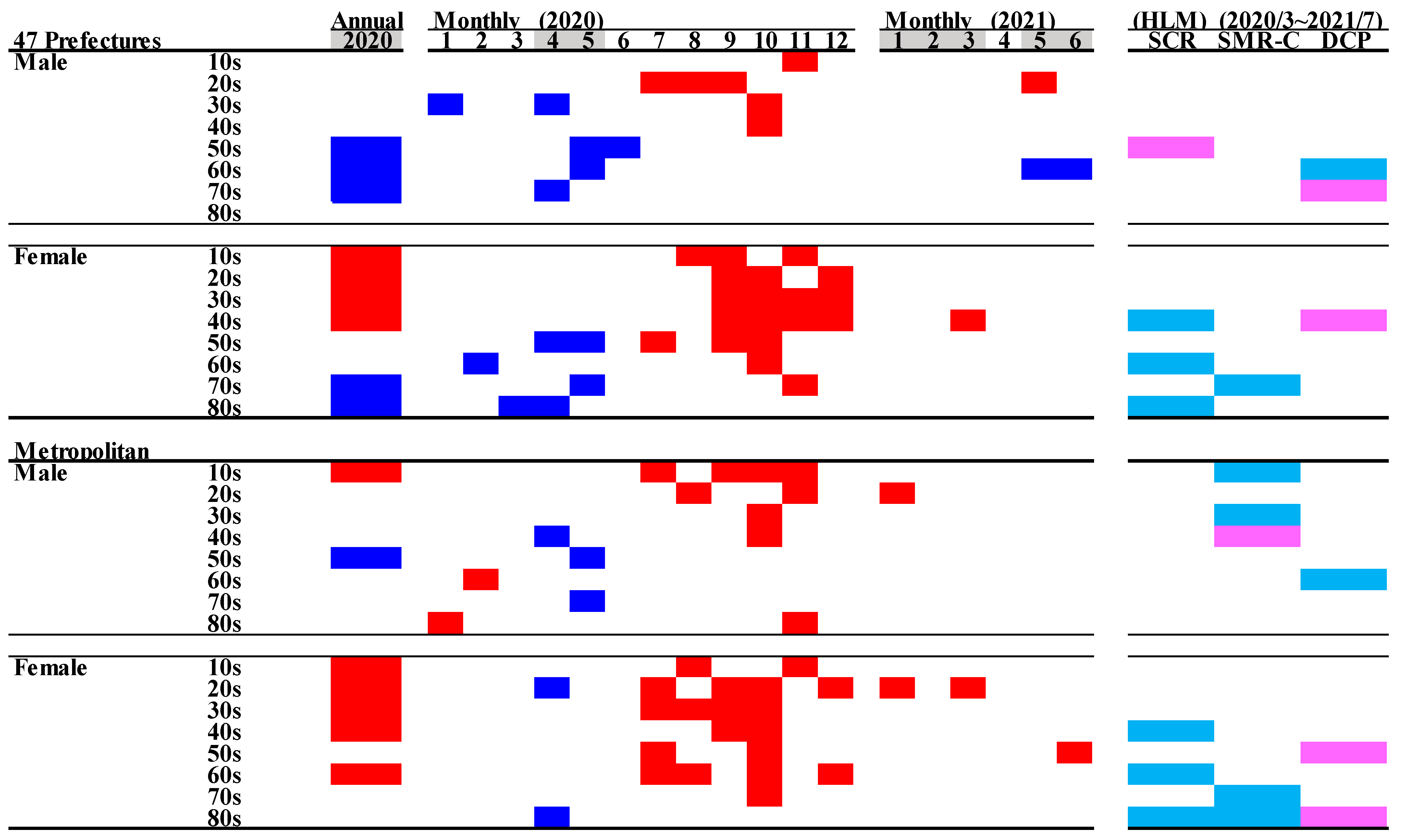
3.2. Suicide Mortality Disaggregated by Age
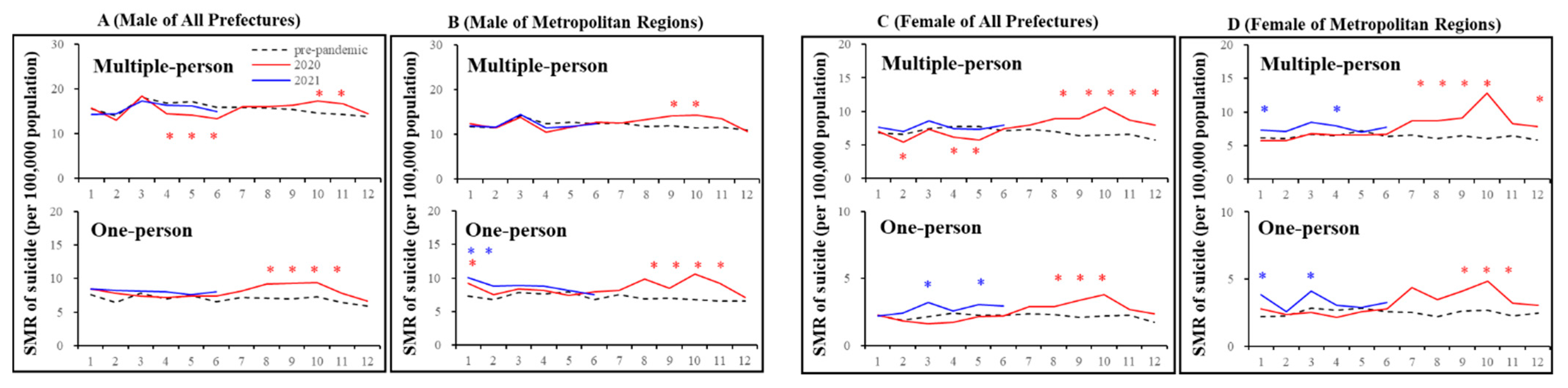
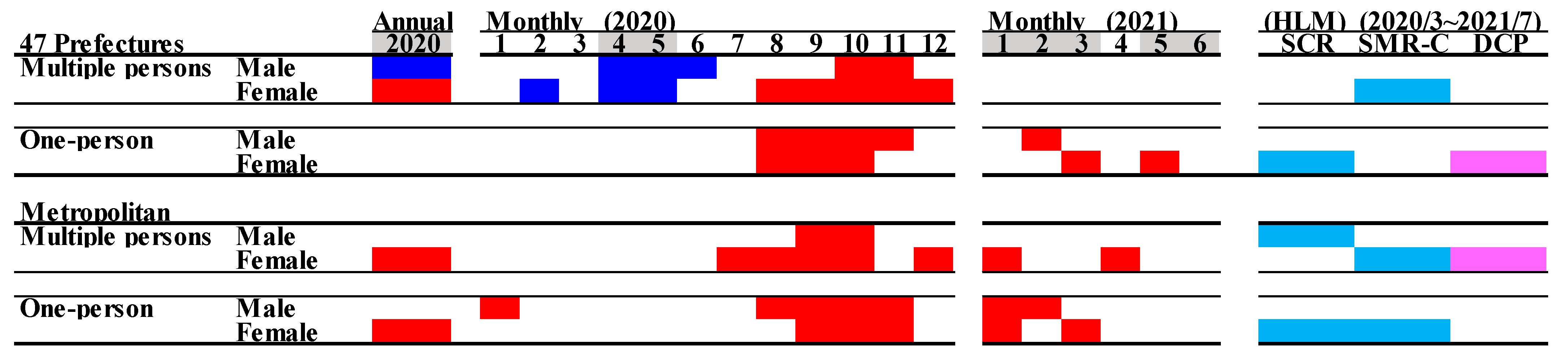
3.3. Suicide Mortality Disaggregated by Household Condition
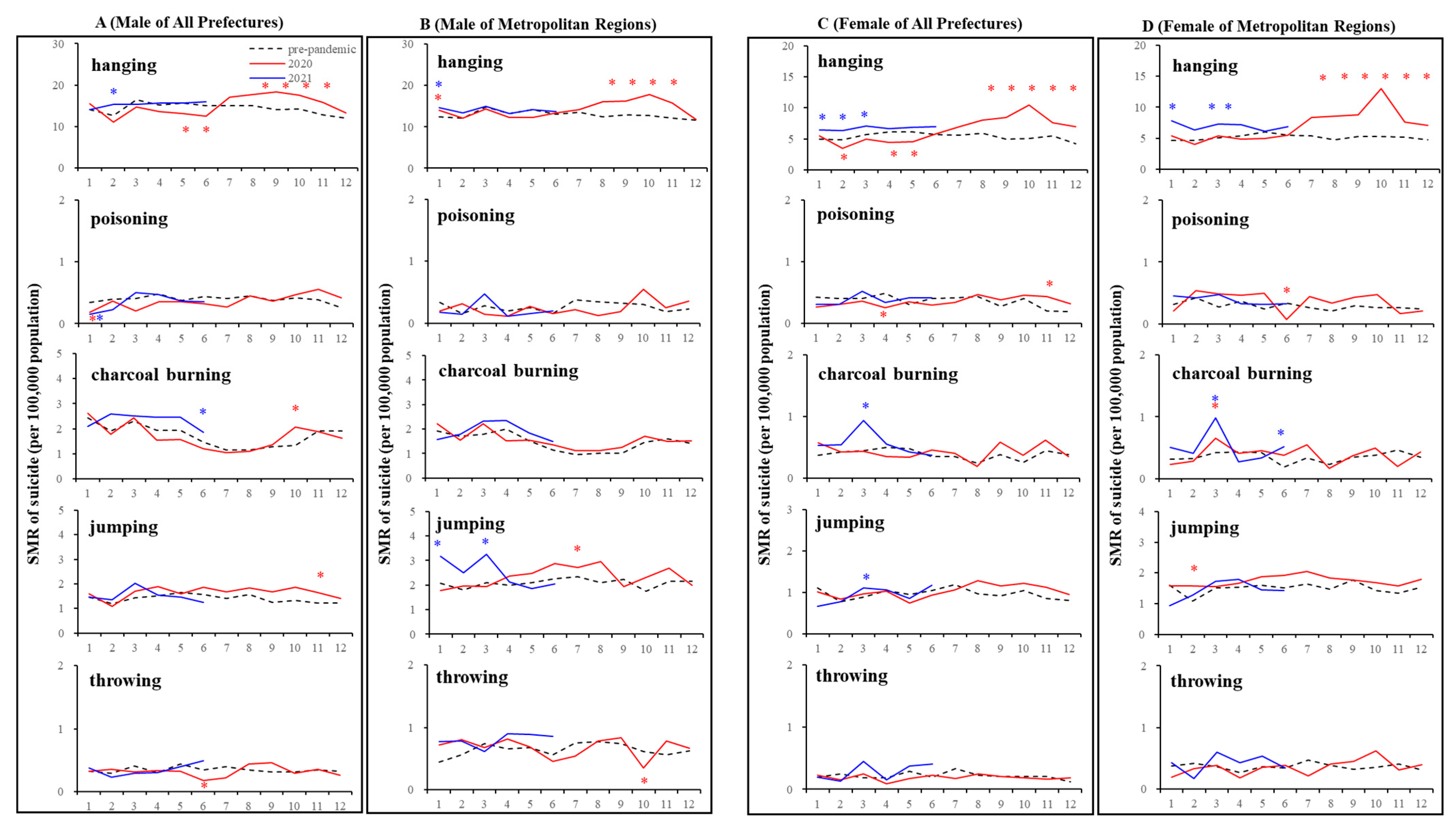
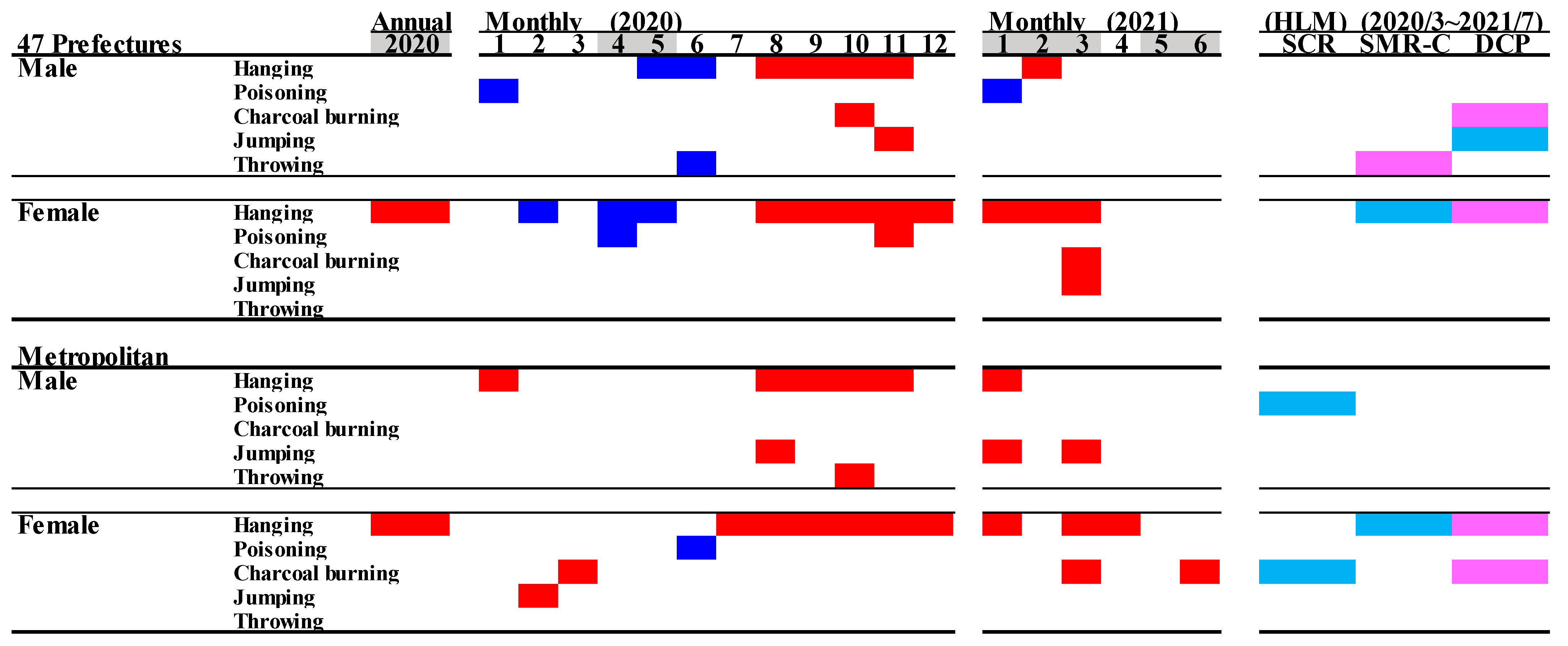
3.4. Suicide Mortality Disaggregated by Suicide Means
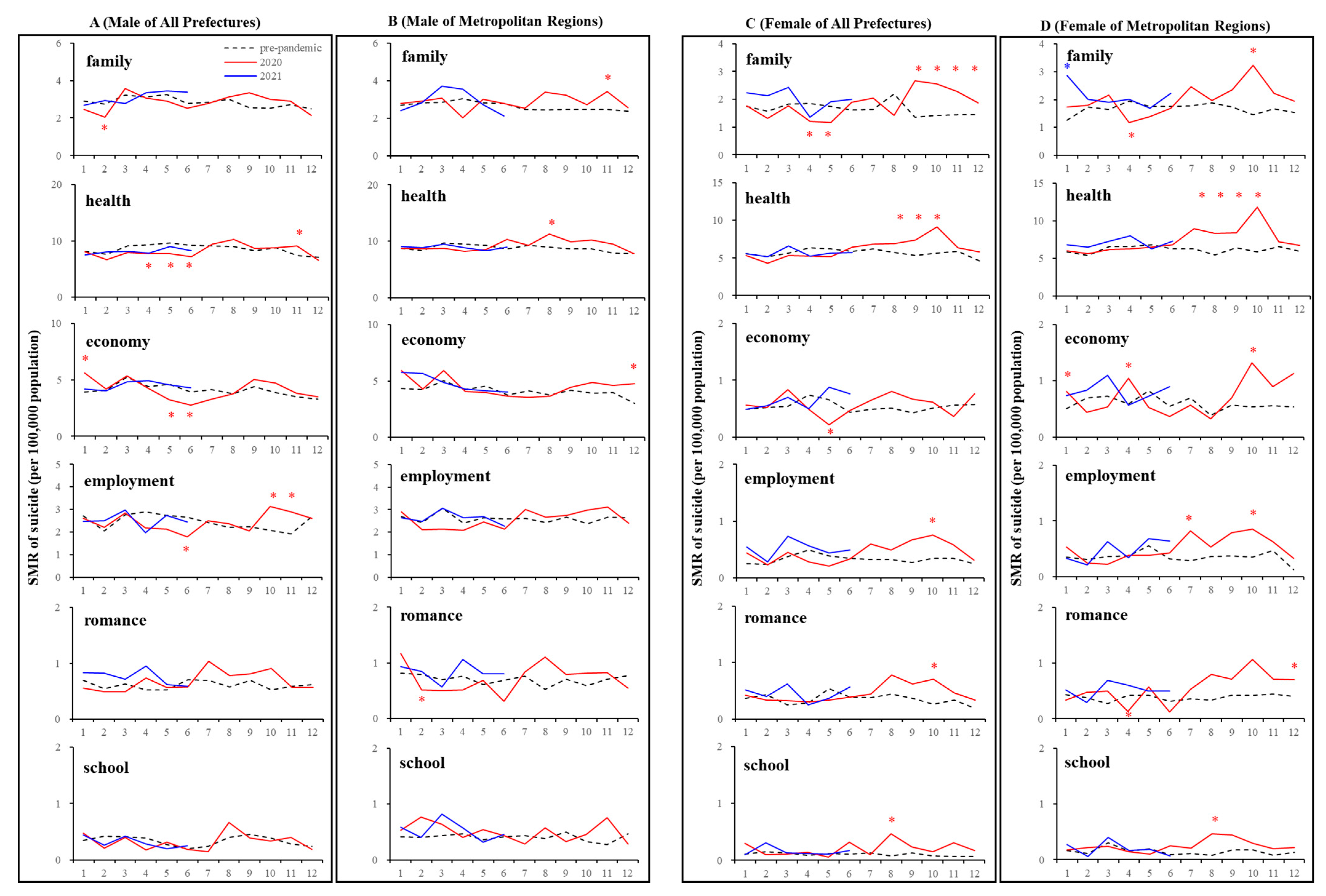
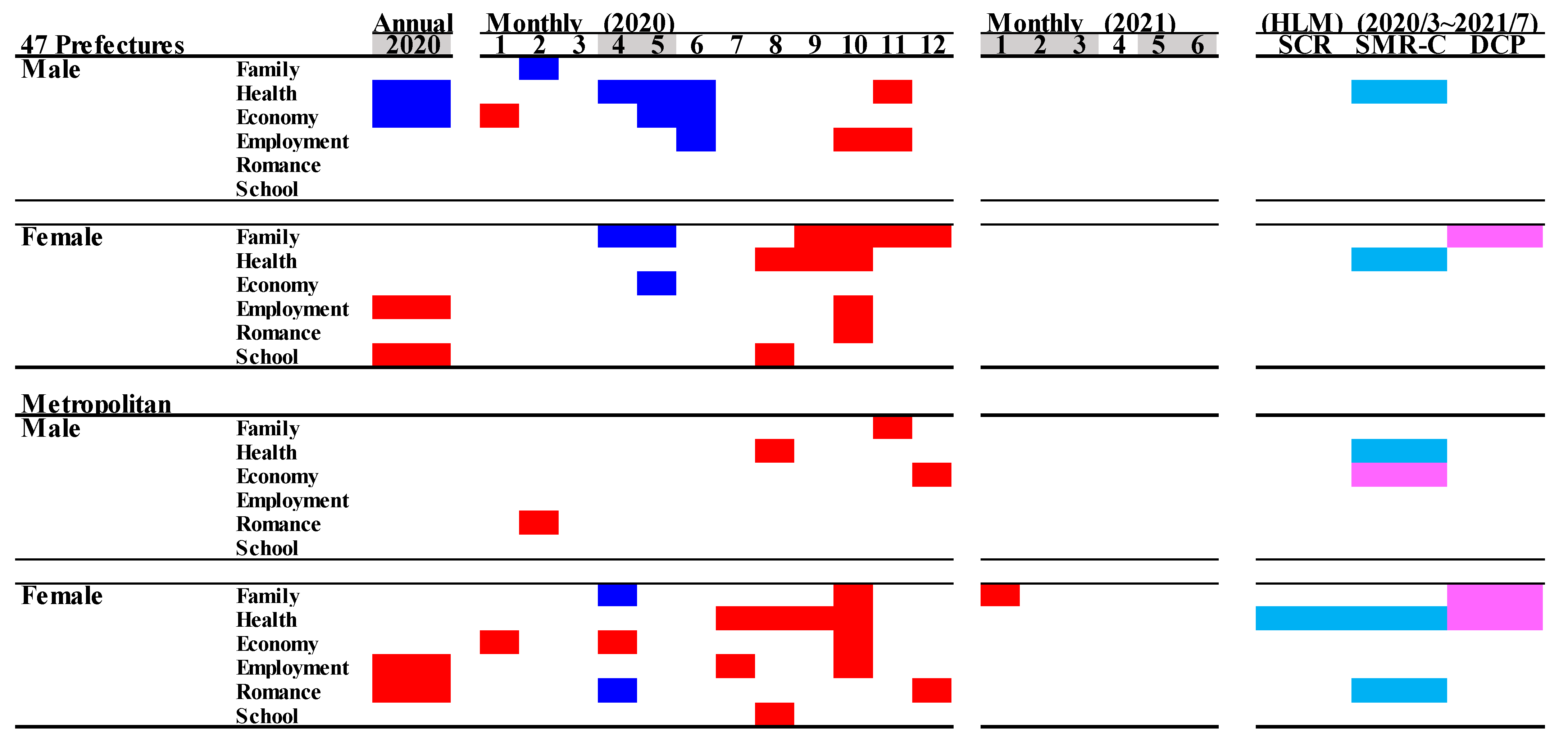
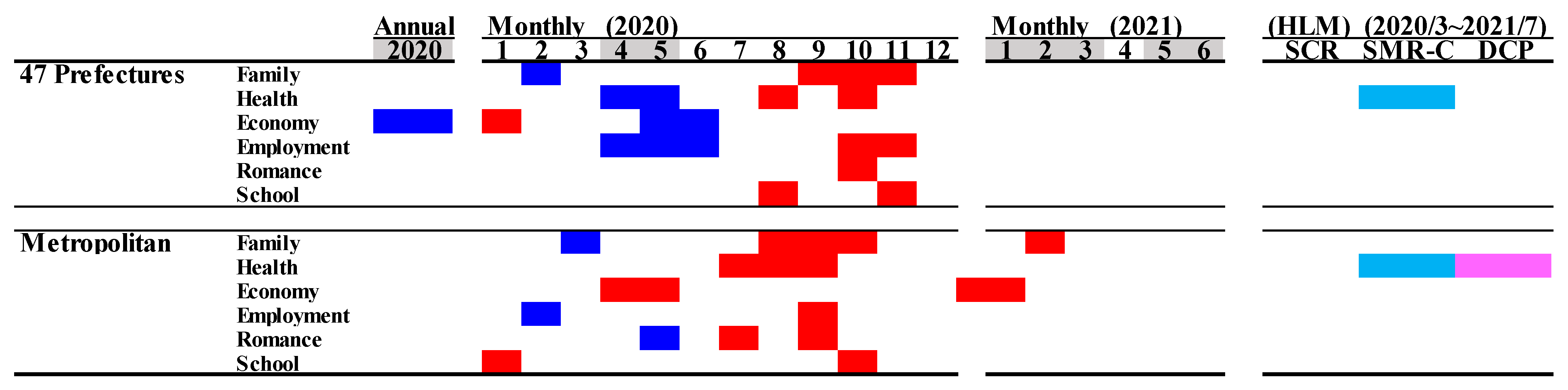
3.5. Suicide Mortality by Motive
4. Discussion
4.1. Overall Fluctuations of Suicide Mortality during COVID-19 Pandemic in Japan
4.2. When and Who Died by Suicide
4.3. When and Who Died by Suicide, and How
4.4. Who Died by Suicide, When, and Why
4.5. Candidate Mechanisms of Specific Fluctuations of Suicide Mortality of Younger Populations
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Who Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 25 October 2021).
- National Institute of Infectious Diseases. Report Week Correspondence Table. Available online: https://www.niid.go.jp/niid/ja/calendar.html (accessed on 1 September 2021).
- Banerjee, D.; Kosagisharaf, J.R.; Sathyanarayana Rao, T.S. ‘The dual pandemic’ of suicide and COVID-19: A biopsychosocial narrative of risks and prevention. Psychiatry Res. 2021, 295, 113577. [Google Scholar] [CrossRef] [PubMed]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; Pirkis, J.; Caine, E.D.J.T.L.P. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. [Google Scholar] [CrossRef]
- Kawohl, W.; Nordt, C.J.T.L.P. COVID-19, unemployment, and suicide. Lancet Psychiatry 2020, 7, 389–390. [Google Scholar] [CrossRef]
- Reger, M.A.; Stanley, I.H.; Joiner, T.E. Suicide mortality and coronavirus disease 2019—a perfect storm? JAMA Psychiatry 2020, 77, 1093–1094. [Google Scholar] [CrossRef] [Green Version]
- Wasserman, D.; Iosue, M.; Wuestefeld, A.; Carli, V. Adaptation of evidence-based suicide prevention strategies during and after the COVID-19 pandemic. World Psychiatry 2020, 19, 294–306. [Google Scholar] [CrossRef]
- Chang, S.S.; Gunnell, D.; Sterne, J.A.; Lu, T.H.; Cheng, A.T. Was the economic crisis 1997–1998 responsible for rising suicide rates in East/Southeast Asia? A time-trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Soc. Sci. Med. 2009, 68, 1322–1331. [Google Scholar] [CrossRef]
- Anagnostopoulos, D.C.; Giannakopoulos, G.; Christodoulou, N.G. The synergy of the refugee crisis and the financial crisis in Greece: Impact on mental health. Int. J. Soc. Psychiatry 2017, 63, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Pirkis, J.; John, A.; Shin, S.; DelPozo-Banos, M.; Arya, V.; Analuisa-Aguilar, P.; Appleby, L.; Arensman, E.; Bantjes, J.; Baran, A.; et al. Suicide trends in the early months of the COVID-19 pandemic: An interrupted time-series analysis of preliminary data from 21 countries. Lancet Psychiatry 2021, 8, 579–588. [Google Scholar] [CrossRef]
- John, A.; Eyles, E.; Webb, R.T.; Okolie, C.; Schmidt, L.; Arensman, E.; Hawton, K.; O’Connor, R.C.; Kapur, N.; Moran, P.; et al. The impact of the COVID-19 pandemic on self-harm and suicidal behaviour: Update of living systematic review. F1000Research 2020, 9, 1097. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Begum, N.; Saini, A.; Wang, S.; McGuire, P.; Fusar-Poli, P.; Lewis, G.; David, A.S. Suicide, self-harm and thoughts of suicide or self-harm in infectious disease epidemics: A systematic review and meta-analysis. Epidemiol. Psychiatr. Sci. 2021, 30, e32. [Google Scholar] [CrossRef]
- Ministry of Health, Law. Basic Data on Suicide in the Region. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000140901.html (accessed on 1 September 2021).
- Fushimi, M. The importance of studying the increase in suicides and gender differences during the COVID-19 pandemic. QJM Int. J. Med. 2021. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ishikane, M.; Ghaznavi, C.; Ueda, P. Assessment of Suicide in Japan during the COVID-19 Pandemic vs Previous Years. JAMA Netw. Open 2021, 4, e2037378. [Google Scholar] [CrossRef]
- Nomura, S.; Kawashima, T.; Harada, N.; Yoneoka, D.; Tanoue, Y.; Eguchi, A.; Gilmour, S.; Kawamura, Y.; Hashizume, M. Trends in suicide in Japan by gender during the COVID-19 pandemic, through December 2020. Psychiatry Res. 2021, 300, 113913. [Google Scholar] [CrossRef] [PubMed]
- Seposo, X.T. COVID-19 threatens decade-long suicide initiatives in Japan. Asian J. Psychiatr. 2021, 60, 102660. [Google Scholar] [CrossRef]
- Eguchi, A.; Nomura, S.; Gilmour, S.; Harada, N.; Sakamoto, H.; Ueda, P.; Yoneoka, D.; Tanoue, Y.; Kawashima, T.; Hayashi, T.I.; et al. Suicide by gender and 10-year age groups during the COVID-19 pandemic vs previous five years in Japan: An analysis of national vital statistics. Psychiatry Res. 2021, 305, 114173. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Okamoto, S. Increase in suicide following an initial decline during the COVID-19 pandemic in Japan. Nat. Hum. Behav. 2021, 5, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Kino, S.; Jang, S.N.; Gero, K.; Kato, S.; Kawachi, I. Age, period, cohort trends of suicide in Japan and Korea (1986–2015): A tale of two countries. Soc. Sci. Med. 2019, 235, 112385. [Google Scholar] [CrossRef]
- Kato, R.; Okada, M. Can Financial Support Reduce Suicide Mortality Rates? Int. J. Environ. Res. Public Health 2019, 16, 4797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, M.; Hasegawa, T.; Kato, R.; Shiroyama, T. Analysing regional unemployment rates, GDP per capita and financial support for regional suicide prevention programme on suicide mortality in Japan using governmental statistical data. BMJ Open 2020, 10, e037537. [Google Scholar] [CrossRef]
- Nakamoto, M.; Nakagawa, T.; Murata, M.; Okada, M. Impacts of Dual-Income Household Rate on Suicide Mortalities in Japan. Int. J. Environ. Res. Public Health 2021, 18, 5670. [Google Scholar] [CrossRef]
- Shiroyama, T.; Fukuyama, K.; Okada, M. Effects of Financial Expenditure of Prefectures/Municipalities on Regional Suicide Mortality in Japan. Int. J. Environ. Res. Public Health 2021, 18, 8639. [Google Scholar] [CrossRef]
- Hasegawa, T.; Matsumoto, R.; Yamamoto, Y.; Okada, M. Analysing effects of financial support for regional suicide prevention programmes on methods of suicide completion in Japan between 2009 and 2018 using governmental statistical data. BMJ Open 2021, 11, e049538. [Google Scholar] [PubMed]
- Ministry of Health, Labor and Welfare. Preventing Suicide: A Resource for Media Professionals-Update 2017. Available online: https://www.who.int/mental_health/suicide-prevention/resource_booklet_2017/en/ (accessed on 1 December 2019).
- Ministry of Health, Labor and Welfare. Survey Study on the Actual Conditions of Young Carers. Available online: https://elaws.e-gov.go.jp/search/elawsSearch/elaws_search/lsg0500/detail?lawId=501AC1000000032_20190912_000000000000000&openerCode=1 (accessed on 1 May 2021).
- Ministry of Health, Labor and Welfare. Calling Attention When Reporting on Celebrity Suicide. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/who_tebiki.html (accessed on 25 October 2021).
- Wasserman, I.M. The impact of epidemic, war, prohibition and media on suicide: United States, 1910–1920. Suicide Life Threat. Behav. 1992, 22, 240–254. [Google Scholar]
- Liang, S.T.; Liang, L.T.; Rosen, J.M. COVID-19: A comparison to the 1918 influenza and how we can defeat it. Postgrad. Med. J. 2021, 97, 273–274. [Google Scholar] [CrossRef]
- Chan, S.M.; Chiu, F.K.; Lam, C.W.; Leung, P.Y.; Conwell, Y. Elderly suicide and the 2003 SARS epidemic in Hong Kong. Int. J. Geriatr. Psychiatry 2006, 21, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Cheung, Y.T.; Chau, P.H.; Yip, P.S. A revisit on older adults suicides and Severe Acute Respiratory Syndrome (SARS) epidemic in Hong Kong. Int. J. Geriatr. Psychiatry 2008, 23, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- Yip, P.S.; Cheung, Y.T.; Chau, P.H.; Law, Y.W. The impact of epidemic outbreak: The case of severe acute respiratory syndrome (SARS) and suicide among older adults in Hong Kong. Crisis 2010, 31, 86–92. [Google Scholar] [CrossRef]
- Zortea, T.C.; Brenna, C.T.A.; Joyce, M.; McClelland, H.; Tippett, M.; Tran, M.M.; Arensman, E.; Corcoran, P.; Hatcher, S.; Heisel, M.J.; et al. The Impact of Infectious Disease-Related Public Health Emergencies on Suicide, Suicidal Behavior, and Suicidal Thoughts. Crisis 2020, 1–14. [Google Scholar] [CrossRef]
- Fire and Disaster Management Agency. 2014 Firefighting White Paper. Available online: https://www.fdma.go.jp/publication/#whitepaper (accessed on 1 June 2021).
- Matsubayashi, T.; Sawada, Y.; Ueda, M. Natural disasters and suicide: Evidence from Japan. Soc. Sci. Med. 2013, 82, 126–133. [Google Scholar] [CrossRef]
- Madianos, M.G.; Evi, K. Trauma and natural disaster: The case of earthquakes in Greece. J. Loss Trauma 2010, 15, 138–150. [Google Scholar] [CrossRef]
- Gordon, K.H.; Bresin, K.; Dombeck, J.; Routledge, C.; Wonderlich, J.A.J.C. The impact of the 2009 Red River Flood on interpersonal risk factors for suicide. Crisis 2011, 32, 52–55. [Google Scholar] [CrossRef]
- Farooq, S.; Tunmore, J.; Ali, W.; Ayub, M. Suicide, self-harm and suicidal ideation during COVID-19: A systematic review. Psychiatry Res. 2021, 306, 114228. [Google Scholar] [CrossRef]
- John, A.; Pirkis, J.; Gunnell, D.; Appleby, L.; Morrissey, J. Trends in suicide during the COVID-19 pandemic. BMJ 2020, 371, m4352. [Google Scholar] [CrossRef]
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Surveys of Population, Population Change and the Number of Households Based on the Basic Resident Registration. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&toukei=00200241&tstat=000001039591 (accessed on 1 September 2021).
- Nakano, T.; Hasegawa, T.; Okada, M. Analysing the Impacts of Financial Support for Regional Suicide Prevention Programmes on Suicide Mortality Caused by Major Suicide Motives in Japan Using Statistical Government Data. Int. J. Environ. Res. Public Health 2021, 18, 3414. [Google Scholar] [CrossRef]
- Shiratori, Y.; Tachikawa, H.; Nemoto, K.; Endo, G.; Aiba, M.; Matsui, Y.; Asada, T. Network analysis for motives in suicide cases: A cross-sectional study. Psychiatry Clin. Neurosci. 2014, 68, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Idogawa, M.; Tange, S.; Nakase, H.; Tokino, T. Interactive Web-based Graphs of Coronavirus Disease 2019 Cases and Deaths per Population by Country. Clin. Infect. Dis. 2020, 71, 902–903. [Google Scholar] [CrossRef]
- Fukuyama, K.; Kato, R.; Murata, M.; Shiroyama, T.; Okada, M. Clozapine Normalizes a Glutamatergic Transmission Abnormality Induced by an Impaired NMDA Receptor in the Thalamocortical Pathway via the Activation of a Group III Metabotropic Glutamate Receptor. Biomolecules 2019, 9, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakano, T.; Hasegawa, T.; Suzuki, D.; Motomura, E.; Okada, M. Amantadine Combines Astroglial System Xc(-) Activation with Glutamate/NMDA Receptor Inhibition. Biomolecules 2019, 9, 191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, M.; Fukuyama, K.; Kawano, Y.; Shiroyama, T.; Ueda, Y. Memantine protects thalamocortical hyper-glutamatergic transmission induced by NMDA receptor antagonism via activation of system xc. Pharmacol. Res. Perspect. 2019, 7, e00457. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labor and Welfare. 2020 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsuhakusyo2020.html (accessed on 1 June 2021).
- Gunnell, D.; Bennewith, O.; Hawton, K.; Simkin, S.; Kapur, N. The epidemiology and prevention of suicide by hanging: A systematic review. Int. J. Epidemiol. 2005, 34, 433–442. [Google Scholar] [CrossRef]
- IOC. Joint Statement from the International Olympic Committee and the Tokyo 2020 Organising Committee. Available online: https://olympics.com/ioc/news/joint-statement-from-the-international-olympic-committee-and-the-tokyo-2020-organising-committee (accessed on 1 September 2021).
- Nagata, M.; Ojima, M.; Kurachi, T.; Miura, H.; Kawamoto, T. Economic effects of the 2020 Tokyo Olympics (Japanese). Bank Jpn. Rep. Res. Pap. 2015, 12, 1–11. [Google Scholar]
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Labor Force Survey. Available online: https://www.stat.go.jp/data/roudou/pref/index.html (accessed on 26 October 2021).
- Agency, N.P. Criminal Statistics: Stoker and Domestic Violence. Available online: https://www.npa.go.jp/publications/statistics/safetylife/dv.html (accessed on 26 October 2021).
- Odgers, C.L.; Schueller, S.M.; Ito, M. Screen time, social media use, and adolescent development. Annu. Rev. Dev. Psychol. 2020, 2, 485–502. [Google Scholar] [CrossRef]
- Ellis, W.E.; Dumas, T.M.; Forbes, L.M. Physically isolated but socially connected: Psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Can. J. Behav. Sci. /Rev. Can. Des. Sci. Du Comport. 2020, 52, 177. [Google Scholar] [CrossRef]
- Kapetanovic, S.; Gurdal, S.; Ander, B.; Sorbring, E. Reported changes in adolescent psychosocial functioning during the COVID-19 outbreak. Adolescents 2021, 1, 10–20. [Google Scholar] [CrossRef]
- Magson, N.R.; Freeman, J.Y.A.; Rapee, R.M.; Richardson, C.E.; Oar, E.L.; Fardouly, J. Risk and Protective Factors for Prospective Changes in Adolescent Mental Health during the COVID-19 Pandemic. J. Youth Adolesc. 2021, 50, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Fegert, J.M.; Vitiello, B.; Plener, P.L.; Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child. Adolesc. Psychiatry Ment. Health 2020, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, P.J. Suicidality in children and adolescents: Lessons to be learned from the COVID-19 crisis. Eur. Child. Adolesc. Psychiatry 2020, 29, 737–738. [Google Scholar] [CrossRef]
- Japan Suicide Countermeasures Promotion Center. Enlightenment/Recommendation. Available online: https://jscp.or.jp/action/jisatsu_benkyokai_report0810.html (accessed on 26 October 2021).













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All 47 Prefectures | Five Metropolitan Regions | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | ||||||||||||||
| Year | Month | Mean | ± | SD | (p) | Mean | ± | SD | (p) | Mean | ± | SD | (p) | Mean | ± | SD | (p) |
| Pre-pandemic | 1 | 23.2 | ± | 4.8 | 9.1 | ± | 2.2 | 19.2 | ± | 3.3 | 8.4 | ± | 1.4 | ||||
| Average | 2 | 20.6 | ± | 4.3 | 8.6 | ± | 2.3 | 21.0 | ± | 3.3 | 9.6 | ± | 1.4 | ||||
| (2017–2019) | 3 | 26.1 | ± | 4.7 | 9.7 | ± | 2.8 | 22.6 | ± | 2.9 | 9.8 | ± | 1.5 | ||||
| 4 | 24.0 | ± | 4.5 | 10.2 | ± | 2.7 | 21.4 | ± | 2.6 | 9.9 | ± | 1.5 | |||||
| 5 | 24.9 | ± | 5.0 | 10.1 | ± | 2.8 | 21.7 | ± | 4.0 | 10.5 | ± | 1.0 | |||||
| 6 | 22.7 | ± | 4.7 | 9.5 | ± | 2.1 | 20.5 | ± | 2.2 | 9.5 | ± | 1.4 | |||||
| 7 | 23.2 | ± | 5.3 | 9.8 | ± | 2.6 | 20.7 | ± | 3.0 | 9.4 | ± | 1.0 | |||||
| 8 | 23.0 | ± | 4.7 | 9.5 | ± | 2.6 | 19.4 | ± | 2.7 | 8.6 | ± | 1.5 | |||||
| 9 | 22.8 | ± | 5.1 | 8.6 | ± | 2.2 | 20.5 | ± | 3.7 | 9.7 | ± | 1.3 | |||||
| 10 | 22.1 | ± | 4.9 | 8.8 | ± | 2.1 | 19.0 | ± | 2.5 | 9.0 | ± | 1.3 | |||||
| 11 | 21.0 | ± | 4.5 | 9.0 | ± | 2.1 | 19.2 | ± | 3.6 | 9.2 | ± | 1.2 | |||||
| 12 | 19.9 | ± | 3.4 | 7.5 | ± | 2.0 | 17.4 | ± | 2.6 | 8.1 | ± | 1.2 | |||||
| 2020 | 1 | 24.3 | ± | 6.1 | (0.35) | 9.3 | ± | 3.5 | (0.75) | 21.3 | ± | 3.4 | (0.03) * | 8.4 | ± | 1.7 | (0.93) |
| 2 | 20.8 | ± | 6.4 | (0.88) | 7.3 | ± | 3.1 | (0.01) ** | 20.1 | ± | 3.0 | (0.32) | 8.6 | ± | 2.8 | (0.30) | |
| 3 | 25.9 | ± | 7.8 | (0.83) | 9.0 | ± | 3.9 | (0.27) | 21.8 | ± | 2.6 | (0.47) | 9.2 | ± | 1.8 | (0.46) | |
| 4 | 21.6 | ± | 6.1 | (0.01) * | 7.8 | ± | 3.9 | (0.00) ** | 19.0 | ± | 3.5 | (0.08) | 8.9 | ± | 1.7 | (0.22) | |
| 5 | 21.6 | ± | 8.4 | (0.01) ** | 7.9 | ± | 3.9 | (0.00) ** | 18.9 | ± | 3.4 | (0.11) | 9.0 | ± | 2.5 | (0.08) | |
| 6 | 20.7 | ± | 5.9 | (0.08) | 9.7 | ± | 3.8 | (0.76) | 21.1 | ± | 3.4 | (0.51) | 9.7 | ± | 1.8 | (0.81) | |
| 7 | 24.2 | ± | 7.3 | (0.32) | 10.9 | ± | 4.7 | (0.09) | 20.5 | ± | 3.4 | (0.93) | 12.9 | ± | 3.4 | (0.01) ** | |
| 8 | 25.4 | ± | 7.1 | (0.01) * | 11.7 | ± | 4.9 | (0.00) ** | 23.0 | ± | 2.1 | (0.00) ** | 11.9 | ± | 3.2 | (0.01) * | |
| 9 | 25.7 | ± | 6.1 | (0.02) * | 12.3 | ± | 4.3 | (0.00) ** | 23.0 | ± | 3.0 | (0.07) | 13.4 | ± | 1.9 | (0.00) ** | |
| 10 | 26.7 | ± | 6.9 | (0.00) ** | 14.5 | ± | 5.5 | (0.00) ** | 24.4 | ± | 4.4 | (0.00) ** | 17.3 | ± | 1.8 | (0.00) ** | |
| 11 | 24.6 | ± | 5.8 | (0.00) ** | 11.4 | ± | 4.0 | (0.00) ** | 23.2 | ± | 2.8 | (0.01) ** | 11.7 | ± | 2.8 | (0.02) * | |
| 12 | 21.1 | ± | 6.3 | (0.18) | 10.3 | ± | 4.6 | (0.00) ** | 17.6 | ± | 1.4 | (0.82) | 10.8 | ± | 2.3 | (0.03) * | |
| 2021 | 1 | 23.3 | ± | 6.5 | (1.00) | 10.0 | ± | 3.8 | (0.37) | 21.6 | ± | 3.8 | (0.03) * | 11.0 | ± | 1.6 | (0.00) ** |
| 2 | 23.2 | ± | 5.5 | (0.03) * | 9.7 | ± | 4.3 | (0.19) | 22.2 | ± | 4.2 | (0.54) | 10.6 | ± | 1.9 | (0.48) | |
| 3 | 26.3 | ± | 8.3 | (0.99) | 12.0 | ± | 4.6 | (0.00) ** | 23.1 | ± | 3.8 | (0.93) | 12.4 | ± | 2.9 | (0.03) * | |
| 4 | 24.9 | ± | 8.5 | (0.71) | 10.4 | ± | 3.4 | (0.97) | 20.7 | ± | 6.1 | (0.89) | 11.1 | ± | 2.3 | (0.22) | |
| 5 | 24.5 | ± | 8.2 | (0.94) | 10.7 | ± | 3.5 | (0.52) | 19.9 | ± | 6.4 | (0.68) | 9.7 | ± | 2.7 | (0.66) | |
| 6 | 23.5 | ± | 7.7 | (0.80) | 11.2 | ± | 4.8 | (0.06) | 20.3 | ± | 3.6 | (0.99) | 11.1 | ± | 3.1 | (0.25) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, R.; Motomura, E.; Fukuyama, K.; Shiroyama, T.; Okada, M. Determining What Changed Japanese Suicide Mortality in 2020 Using Governmental Database. J. Clin. Med. 2021, 10, 5199. https://doi.org/10.3390/jcm10215199
Matsumoto R, Motomura E, Fukuyama K, Shiroyama T, Okada M. Determining What Changed Japanese Suicide Mortality in 2020 Using Governmental Database. Journal of Clinical Medicine. 2021; 10(21):5199. https://doi.org/10.3390/jcm10215199
Chicago/Turabian StyleMatsumoto, Ryusuke, Eishi Motomura, Kouji Fukuyama, Takashi Shiroyama, and Motohiro Okada. 2021. "Determining What Changed Japanese Suicide Mortality in 2020 Using Governmental Database" Journal of Clinical Medicine 10, no. 21: 5199. https://doi.org/10.3390/jcm10215199