
Consensus Defined Diastolic Dysfunction and Cardiac Postoperative Morbidity Score: A Prospective Observational Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
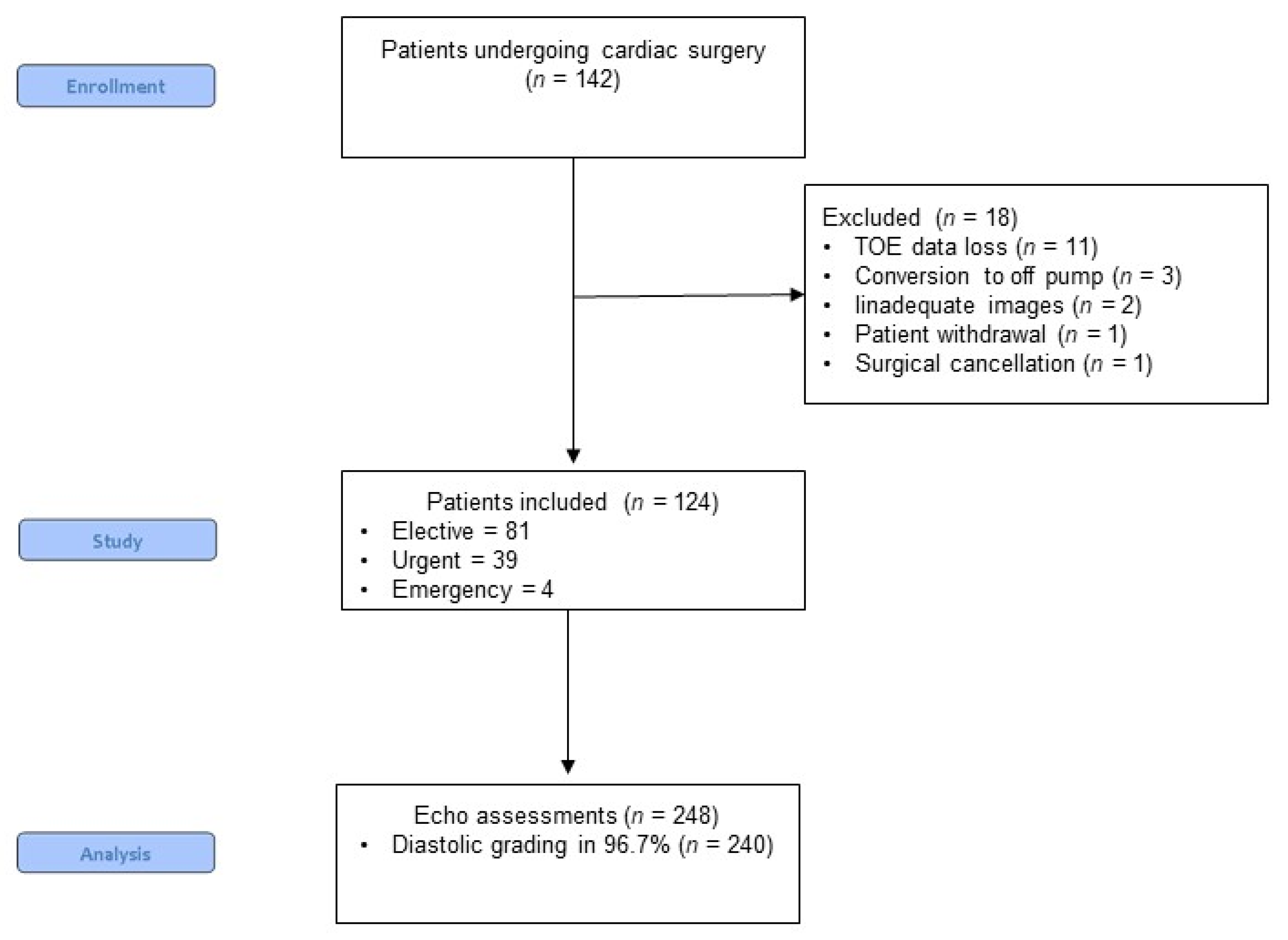
2.1. Patients
2.2. Intraoperative Management
2.3. Echocardiography
2.4. Assessment of Diastolic Dysfunction
2.5. Data Collection
2.6. Statistical Analysis
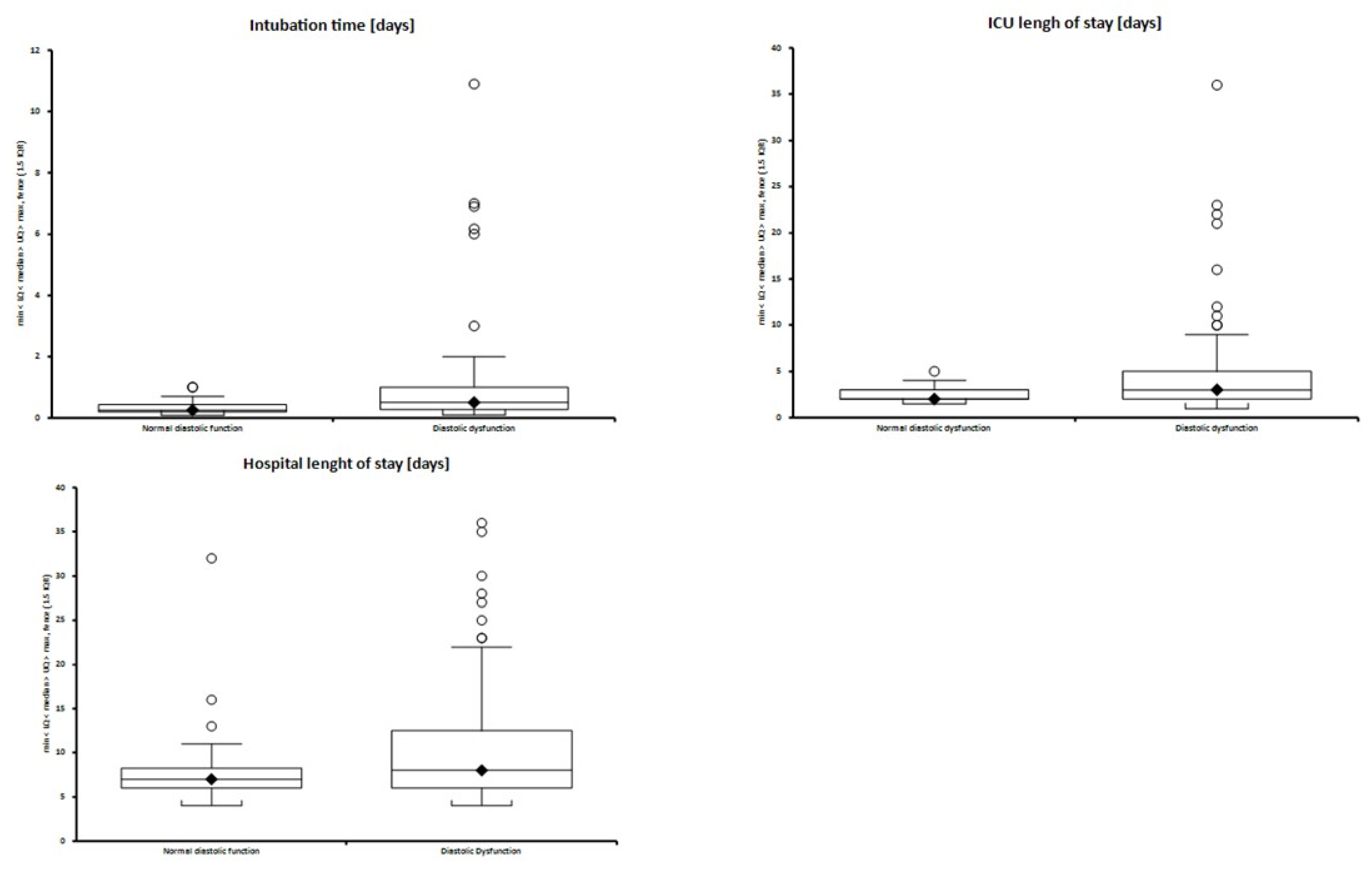
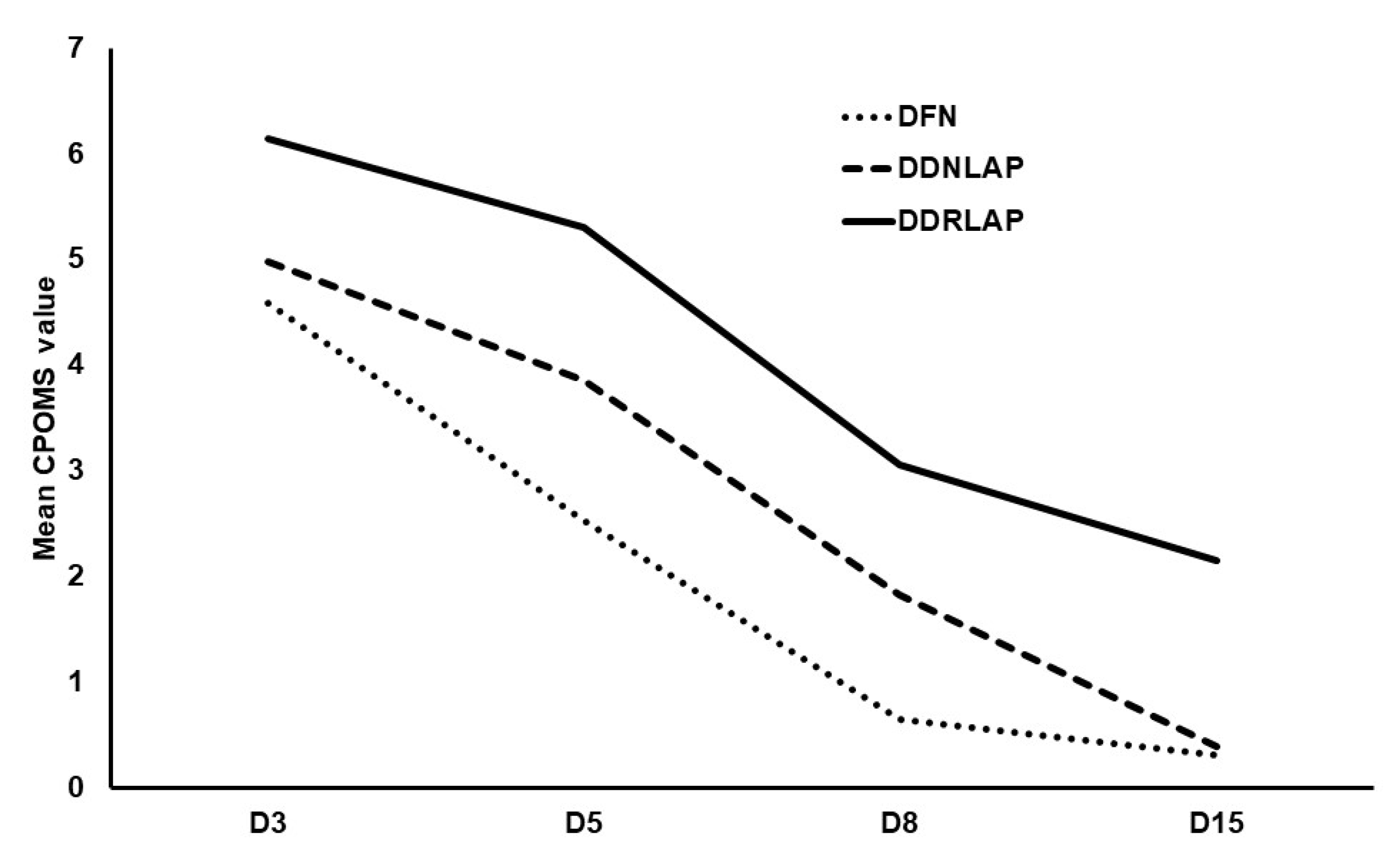
3. Results
4. Discussion
4.1. Hospital Length of Stay
4.2. Approaches to the Measurement of Diastolic Function
4.3. Feasibility of Measuring Diastolic Function in a Cardiac Surgical Population
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Cardiac Postoperative Morbidity Score | (13 Domains: Maximum 1 Point for Each Domain) | ||||
|---|---|---|---|---|---|
| Morbidity Type | CPOMS Criteria | ||||
| Pulmonary | Presence of one or more of the following: | ||||
| New requirement for oxygen or respiratory support (inc. nebulizers/chest physiotherapy on or after D5) | |||||
| Pleural effusion requiring drainage | |||||
| Infectious | Presence of one or more of the following: | ||||
| Currently on antibiotics | |||||
| Has had temperature > 38 °C in last 24 h | |||||
| Has had a white count or CRP requiring in-hospital review or treatment | |||||
| Renal | Presence of one or more of the following: | ||||
| Decreased urine output requiring intervention (inc. IV furosemide) | |||||
| Increased serum creatinine (>30% from preoperative level) | |||||
| Urinary catheter in situ | |||||
| New urinary incontinence | |||||
| Serum potassium abnormalities requiring treatment | |||||
| Gastrointestinal | Presence of one or more of the following: | ||||
| Unable to tolerate an enteral diet for any reason inc nausea, vomiting, abdominal distension | |||||
| Presence of nasogastric tube | |||||
| Diagnosis of gastrointestinal bleeding | |||||
| Cardiovascular | Presence of one or more of the following: | ||||
| Use of inotropic therapy for any cardiovascular cause | |||||
| Presence of pacing wires on or after D5 +/− requiring temporary/new permanent pacing | |||||
| Diagnostic tests/Rx in last 24 h for: | (1) New MI/ischemia | ||||
| (2) Hypotension | |||||
| (3) Arrhythmia (req fluids, pharmacotherapy/omission of pharmacotherapy) | |||||
| (4) Cardiogenic pulmonary oedema | |||||
| (5) Hypertension (requiring pharmacotherapy or omission of pharmacotherapy) | |||||
| (6) Thrombotic event (requiring anticoagulation) | |||||
| Neurological | Presence of one or more of the following: | ||||
| New neurological deficit | |||||
| (Confusion, delirium, coma, incoordination, drowsy, poor swallow, diplopia, sedation, fluctuating consciousness) | |||||
| Haematological | Presence of one or more of the following: | ||||
| Untherapeutic INR requiring pharmacological Rx or omission of pharmacological Rx | |||||
| Requirment in last 24 h for packed red cells, platelets, fresh frozen plasma, cryoprecipitate | |||||
| Wound | Presence of one or more of the following: | ||||
| Wound dehiscence requiring surgical exploration/drainage of pus +/− isolation of organisms | |||||
| Presence of chest drains | |||||
| Wound pain significant enough to require continuing or escalating analgesic intervention | |||||
| Pain | Postoperative pain significant enough to require parenteral opioids or escalating analgesia | ||||
| Endocrine | New or additional requirements for blood sugar management | ||||
| Electrolyte | Electrolyte imbalance requiring oral or IV intervention (Na/Urea/Phosphate) * | ||||
| Review | Remaining in hospital for further review, investigation, or additional procedure | ||||
| Assisted ambulation | New or escalated post op requirement for mobility assistance (wheelchair, zimmer, crutches, walking stick) | ||||
Appendix B
| Type of Surgery | |
|---|---|
| Isolated CABG | 78 (62.9%) |
| CABG plus valve (AVR/MVR) | 17 (13.7%) |
| Isolated valve | 24 (19.3%) |
| >1 valve | 5 (4%) |
Appendix C
| Where to Start? | Action | Outcomes |
|---|---|---|
| First consider the following questions: | Myocardial disease * | Go to Algorithm B |
| Depressed LVEF (<50%) | Go to Algorithm B | |
| Special circumstances (AF, mitral stenosis or regurgitation, depressed EF) | Go to Special Circumstances | |
| None of the above | Go to Algorithm A | |
| Algorithm | Indices to Evaluate | Possible Outcomes |
| A (is DD present?) | Septal E’ < 7, Lateral E’ < 10, E/E’ > 14, TR velocity > 2.8, LAVI > 34 | Majority positive = diastolic dysfunction (DD), go to Algorithm B |
| Majority negative = normal diastolic function (DFN) | ||
| 50% positive = indeterminate if diastolic dysfunction (IDDD) | ||
| B (DD is present, what is the grade?) | E/A, Septal E < 7 or Lateral E < 10, E/E > 14′, TR Velocity > 2.8, LAVI > 34 | E/A <0.8 and E <50cm/s = Grade 1 (DD1) |
| E/A > 2.0 = Grade 3 (DD3) | ||
| IF E/A < 0.8 and E > 50 OR E/A 0.8 to 2 | Assess E/E’ > 14, TR Velocity > 2.8, LAVI > 34 | Majority positive = DD Grade 2 (DD2) |
| Majority negative = DD Grade 1 (DD1) | ||
| 50% positive = DD of indeterminate grade (DDIDG) | ||
| Special Circumstances | Indices to Evaluate | Possible Outcomes |
| Atrial Fibrillation | Go to A or B. If B algorithm used include E/E’ > 11 cutoff, E/Vp ratio > 1.4. IVRT (<65 msec) | As per Algorithm A, but if B used, as per AF modification: |
| Majority positive = DDRLAP | ||
| Majority negative = DD1 | ||
| 50% positive = DDIDG | ||
| Mitral Stenosis | In Algorithm B, add IVRT < 60 | As per A or B outcomes if sinus rhythm, or as per AF modification if in AF |
| Mitral Regurgitation | Only use E/E’ if depressed EF, add Ardur-Adur (>30 msec) and IVRT (<60 msec) in Algorithm B | As per A or B outcomes if sinus rhythm, or as per AF modification if in AF |
| Depressed EF | Go to B. Any missing parameters S/D < 0.8 can be used | As per Algorithm B outcomes |
Appendix D
| Presternotomy | n = 124 | Poststernal Closure | n = 124 |
|---|---|---|---|
| DFN | 32 | DFN | 27 |
| DD1 | 58 | DD1 | 51 |
| DD2 | 8 | DD2 | 14 |
| DD3 | 10 | DD3 | 6 |
| DDRLAP | 1 | DDRLAP | 3 |
| DDIDG | 11 | DDIDG | 19 |
| IDDD | 4 | IDDD | 4 |
References
- Zile, M.R.; Gottdiener, J.S.; Hetzel, S.J.; McMurray, J.J.; Komajda, M.; McKelvie, R.; Baicu, C.F.; Massie, B.M.; Carson, P.E. Prevalence and significance of alterations in cardiac structure and function in patients with heart failure and a preserved ejection fraction. Circulation 2011, 124, 2491–2501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillip, B.; Pastor, D.; Bellows, W.; Leung, J.M. The Prevalence of Preoperative Diastolic Filling Abnormalities in Geriatric Surgical Patients. Anesth. Analg. 2003, 97, 1214–1221. [Google Scholar] [CrossRef] [Green Version]
- Sanders, D.; Dudley, M.; Groban, L. Diastolic dysfunction, cardiovascular aging, and the anesthesiologist. Anesthesiol. Clin. 2009, 27, 497–517. [Google Scholar] [CrossRef] [Green Version]
- Kaw, R.; Hernandez, A.V.; Pasupuleti, V.; Deshpande, A.; Nagarajan, V.; Bueno, H.; Coleman, C.I.; Ioannidis, J.P.A.; Bhatt, D.L.; Blackstone, E.H. Effect of diastolic dysfunction on postoperative outcomes after cardiovascular surgery: A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2016, 152, 1142–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swaminathan, M.; Nicoara, A.; Phillips-Bute, B.G.; Aeschlimann, N.; Milano, C.A.; MacKensen, G.B.; Podgoreanu, M.V.; Velazquez, E.J.; Stafford-Smith, M.; Mathew, J.P.; et al. Utility of a simple algorithm to grade diastolic dysfunction and predict outcome after coronary artery bypass graft surgery. Ann. Thorac. Surg. 2011, 91, 1844–1850. [Google Scholar] [CrossRef]
- Youn, Y.N.; Shim, C.Y.; Yang, H.; Hong, S.; Chung, N.; Yoo, K.J. Effect of diastolic dysfunction on early outcomes during elective off-pump coronary artery bypass grafting: A prospective observational study. Ann. Thorac. Surg. 2011, 92, 587–593. [Google Scholar] [CrossRef]
- Beaubien-Souligny, W.; Brand, F.Z.A.; Lenoir, M.; Amsallem, M.; Haddad, F.; Denault, A.Y. Assessment of Left Ventricular Diastolic Function by Transesophageal Echocardiography Before Cardiopulmonary Bypass: Clinical Implications of a Restrictive Profile. J. Cardiothorac. Vasc. Anesth. 2019, 33, 2394–2401. [Google Scholar] [CrossRef] [PubMed]
- Matyal, R.; Hess, P.E.; Subramaniam, B.; Mitchell, J.; Panzica, P.J.; Pomposelli, F.; Mahmood, F. Perioperative diastolic dysfunction during vascular surgery and its association with postoperative outcome. J. Vasc. Surg. 2009, 50, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Fayad, A.; Ansari, M.T.; Yang, H.; Ruddy, T.; Wells, G.A. Perioperative Diastolic Dysfunction in Patients Undergoing Noncardiac Surgery Is an Independent Risk Factor for Cardiovascular Events. Anesthesiology 2016, 125, 72–91. [Google Scholar] [CrossRef]
- Cho, D.-H.; Park, S.-M.; Kim, M.-N.; Kim, S.-A.; Lim, H.; Shim, W.-J. Presence of Preoperative Diastolic Dysfunction Predicts Postoperative Pulmonary Edema and Cardiovascular Complications in Patients Undergoing Noncardiac Surgery. Echocardiography 2014, 31, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Licker, M.; Cikirikcioglu, M.; Inan, C.; Cartier, V.; Kalangos, A.; Theologou, T.; Cassina, T.; Diaper, J. Preoperative diastolic function predicts the onset of left ventricular dysfunction following aortic valve replacement in high-risk patients with aortic stenosis. Crit. Care 2010, 14, R101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernard, F.; Denault, A.A.; Babin, D.; Goyer, C.; Couture, P.; Couturier, A.A.; Buithieu, J. Diastolic dysfunction is predictive of difficult weaning from cardiopulmonary bypass. Anesth. Analg. 2001, 92, 291–298. [Google Scholar] [CrossRef]
- D’Agostino, R.S.; Jacobs, J.P.; Badhwar, V.; Paone, G.; Rankin, J.S.; Han, J.M.; McDonald, D.; Edwards, F.H.; Shahian, D.M. The Society of Thoracic Surgeons Adult Cardiac Surgery Database: 2017 Update on Outcomes and Quality. Ann. Thorac. Surg. 2017, 103, 18–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salem, R.; Denault, A.Y.; Couture, P.; Bélisle, S.; Fortier, A.; Guertin, M.C.; Carrier, M.; Martineau, R. Left ventricular end-diastolic pressure is a predictor of mortality in cardiac surgery independently of left ventricular ejection fraction. Br. J. Anaesth. 2006, 97, 292–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, J.; Keogh, B.E.; Van Der Meulen, J.; Browne, J.P.; Treasure, T.; Mythen, M.G.; Montgomery, H.E. The development of a postoperative morbidity score to assess total morbidity burden after cardiac surgery. J. Clin. Epidemiol. 2012, 65, 423–433. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [Green Version]
- Papachristofi, O.; Klein, A.A.; Mackay, J.; Nashef, S.; Fletcher, N.; Sharples, L.D. Effect of individual patient risk, centre, surgeon and anaesthetist on length of stay in hospital after cardiac surgery: Association of Cardiothoracic Anaesthesia and Critical Care (ACTACC) consecutive cases series study of 10 UK specialist centres. BMJ Open 2017, 7, e016947. [Google Scholar] [CrossRef]
- Almashrafi, A.; Alsabti, H.; Mukaddirov, M.; Balan, B.; Aylin, P. Factors associated with prolonged length of stay following cardiac surgery in a major referral hospital in Oman: A retrospective observational study. BMJ Open 2016, 6. [Google Scholar] [CrossRef]
- Drighil, A.; Madias, J.E.; Mathewson, J.W.; El Mosalami, H.; El Badaoui, N.; Ramdani, B.; Bennis, A. Haemodialysis: Effects of acute decrease in preload on tissue Doppler imaging indices of systolic and diastolic function of the left and right ventricles. Eur. J. Echocardiogr. 2008, 9, 530–535. [Google Scholar] [CrossRef]
- Vignon, P.; Allot, V.; Lesage, J.; Martaillé, J.-F.; Aldigier, J.-C.; François, B.; Gastinne, H. Diagnosis of left ventricular diastolic dysfunction in the setting of acute changes in loading conditions. Crit. Care 2007, 11, R43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appleton, C.P. Influence of incremental changes in heart rate on mitral flow velocity: Assessment in lightly sedated, conscious dogs. J. Am. Coll. Cardiol. 1991, 17, 227–236. [Google Scholar] [CrossRef] [Green Version]
- Filipovic, M.; Wang, J.; Michaux, I.; Hunziker, P.; Skarvan, K.; Seeberger, M.D. Effects of halothane, sevoflurane and propofol on left ventricular diastolic function in humans during spontaneous and mechanical ventilation. Br. J. Anaesth. 2005, 94, 186–192. [Google Scholar] [CrossRef] [Green Version]
- Filipovic, M.; Michaux, I.; Wang, J.; Hunziker, P.; Skarvan, K.; Seeberger, M. Effects of sevoflurane and propofol on left ventricular diastolic function in patients with pre-existing diastolic dysfunction. Br. J. Anaesth. 2007, 98, 12–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couture, P.; Denault, A.Y.; Shi, Y.; Deschamps, A.; Cossette, M.; Pellerin, M.; Tardif, J.-C.C. Effects of anesthetic induction in patients with diastolic dysfunction. Can. J. Anesth. Can. D’anesthésie 2009, 56, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Lanspa, M.J.; Gutsche, A.R.; Wilson, E.L.; Olsen, T.D.; Hirshberg, E.L.; Knox, D.B.; Brown, S.M.; Grissom, C.K. Application of a simplified definition of diastolic function in severe sepsis and septic shock. Crit. Care 2016, 20, 243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanfilippo, F.; Corredor, C.; Arcadipane, A.; Landesberg, G.; Vieillard-Baron, A.; Cecconi, M.; Fletcher, N. Tissue Doppler assessment of diastolic function and relationship with mortality in critically ill septic patients: A systematic review and meta-analysis. Br. J. Anaesth. 2017, 119, 583–594. [Google Scholar] [CrossRef] [Green Version]
- Poelaert, J. Diastolic dysfunction and sepsis: The devil is in the detail. Br. J. Anaesth. 2017, 119, 555–557. [Google Scholar] [CrossRef] [Green Version]
- Ashes, C.M.; Yu, M.; Meineri, M.; Katznelson, R.; Carroll, J.; Rao, V.; Djaiani, G. Diastolic dysfunction, cardiopulmonary bypass, and atrial fibrillation after coronary artery bypass graft surgery. Br. J. Anaesth. 2014, 113, 815–821. [Google Scholar] [CrossRef] [Green Version]



| Normal Diastolic Function (n = 25) | Diastolic Dysfunction (n = 96) | p Value | |
|---|---|---|---|
| Patient characteristics | |||
| Male | 92% (23) | 78.1% (75) | p = 0.16 |
| BMI | 27.8 (23.1–31.2) | 28.7 (26–32.4) | p = 0.12 |
| Age | 61.8 (54.0–70.6) | 68.8 (61.3–76.9) | p = 0.021 |
| Diabetes | 28.0% (7) | 33.3% (32) | p = 0.81 |
| Hyperlipidemia | 52.0% (13) | 78.1% (75) | p = 0.01 |
| Hypertension | 32.0% (8) | 80.2% (77) | p < 0.001 |
| NYHA | 36.4% (8) | 77.2% (71) | p < 0.001 |
| RWMAs | 6.3% (1) | 55.4% (41) | p < 0.001 |
| EF < 50% | 0 (0) | 30.2% (29) | p = 0.001 |
| Medication | |||
| Beta blockers | 58.3% (14) | 63.5% (61) | p = 0.65 |
| Ca channel blockers | 20.0% (5) | 30.5% (29) | p = 0.45 |
| Nitrates | 24.0% (6) | 32.3% (31) | p = 0.48 |
| Statins | 72.0% (18) | 78.1% (75) | p = 0.60 |
| ACE inhibitors | 52.0% (13) | 70.8% (68) | p = 0.10 |
| Diuretics | 8.0% (2) | 25.0% (24) | p = 0.10 |
| Surgery | |||
| CPB time | 90 (80–104) | 88.5 (74–108) | p = 0.77 |
| X-clamp time | 65 (39–80) | 65 (50–83) | p = 0.66 |
| Electives | 64.0% (16) | 65.6% (63) | p = 1.00 |
| n | Intubation | New AF | HLOS | ICU LOS | MACCE | D3 | D5 | D8 | D15 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Normal diastolic function | 25 | 0.25 (0.2–0.42) | 3 (12.0%) | 7 (6–8) | 2 (2–3) | 0 (0%) | 5 (3–6) | 2 (1–5) | 0 (0–0) | 0 (0–0) |
| Diastolic dysfunction (any grade) | 96 | 0.5 (0.27–1) | 36 (38.3%) | 8 (6–12.5) | 3 (2–5) | 5 (5.2%) | 6 (3–8) | 4.5 (2–6) | 0 (0–4) | 0 (0–0) |
| p = 0.001 | p = 0.016 | p = 0.055 | p = 0.019 | p = 0.582 | p = 0.12 | p = 0.009 | p = 0.009 | p = 0.14 | ||
| Indeterminate diastolic dysfunction | 3 | (2.41%) | ||||||||
| Atrial fibrillation OR (95% CI) = 4.50 (1.22–25.17) p = 0.018 | ||||||||||
| % Difference for Length of Stay (95% CI) (Preadjustment) | p Value | Odds Ratio for Prolonged Length of Stay >11 d (95% CI) | p Value | |
|---|---|---|---|---|
| Age (per year) | 1.2% (0.4, 1.9) | 0.003 | 1.04 (1.00–1.09) | 0.03 |
| Bypass time (per min) | −25.2% (−38.8, −8.5) | 0.005 | 0.55 (0.22–1.40) | 0.21 |
| Non-elective vs. Elective | 24.5% (1.7, 52.5) | 0.034 | 1.10 (0.42–2.90) | 0.85 |
| Diastolic dysfunction vs. normal diastolic function | 12.1% (−10.4, 40.2) | 0.32 | 2.02 (0.61–6.66) | 0.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyle, B.; Zawadka, M.; Shanahan, H.; Cooper, J.; Rogers, A.; Hamarneh, A.; Sivaraman, V.; Anwar, S.; Smith, A. Consensus Defined Diastolic Dysfunction and Cardiac Postoperative Morbidity Score: A Prospective Observational Study. J. Clin. Med. 2021, 10, 5198. https://doi.org/10.3390/jcm10215198
Kyle B, Zawadka M, Shanahan H, Cooper J, Rogers A, Hamarneh A, Sivaraman V, Anwar S, Smith A. Consensus Defined Diastolic Dysfunction and Cardiac Postoperative Morbidity Score: A Prospective Observational Study. Journal of Clinical Medicine. 2021; 10(21):5198. https://doi.org/10.3390/jcm10215198
Chicago/Turabian StyleKyle, Bonnie, Mateusz Zawadka, Hilary Shanahan, Jackie Cooper, Andrew Rogers, Ashraf Hamarneh, Vivek Sivaraman, Sibtain Anwar, and Andrew Smith. 2021. "Consensus Defined Diastolic Dysfunction and Cardiac Postoperative Morbidity Score: A Prospective Observational Study" Journal of Clinical Medicine 10, no. 21: 5198. https://doi.org/10.3390/jcm10215198