
Clinicoprognostic and Histopathological Features of Guttate and Plaque Psoriasis Based on PD-1 Expression

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Demographic and Clinical Characteristics
2.3. IHC Analysis
2.4. Quantitative Real-Time Polymerase Chain Reaction (qRT-PCR)
2.5. Statistical Analysis
3. Results
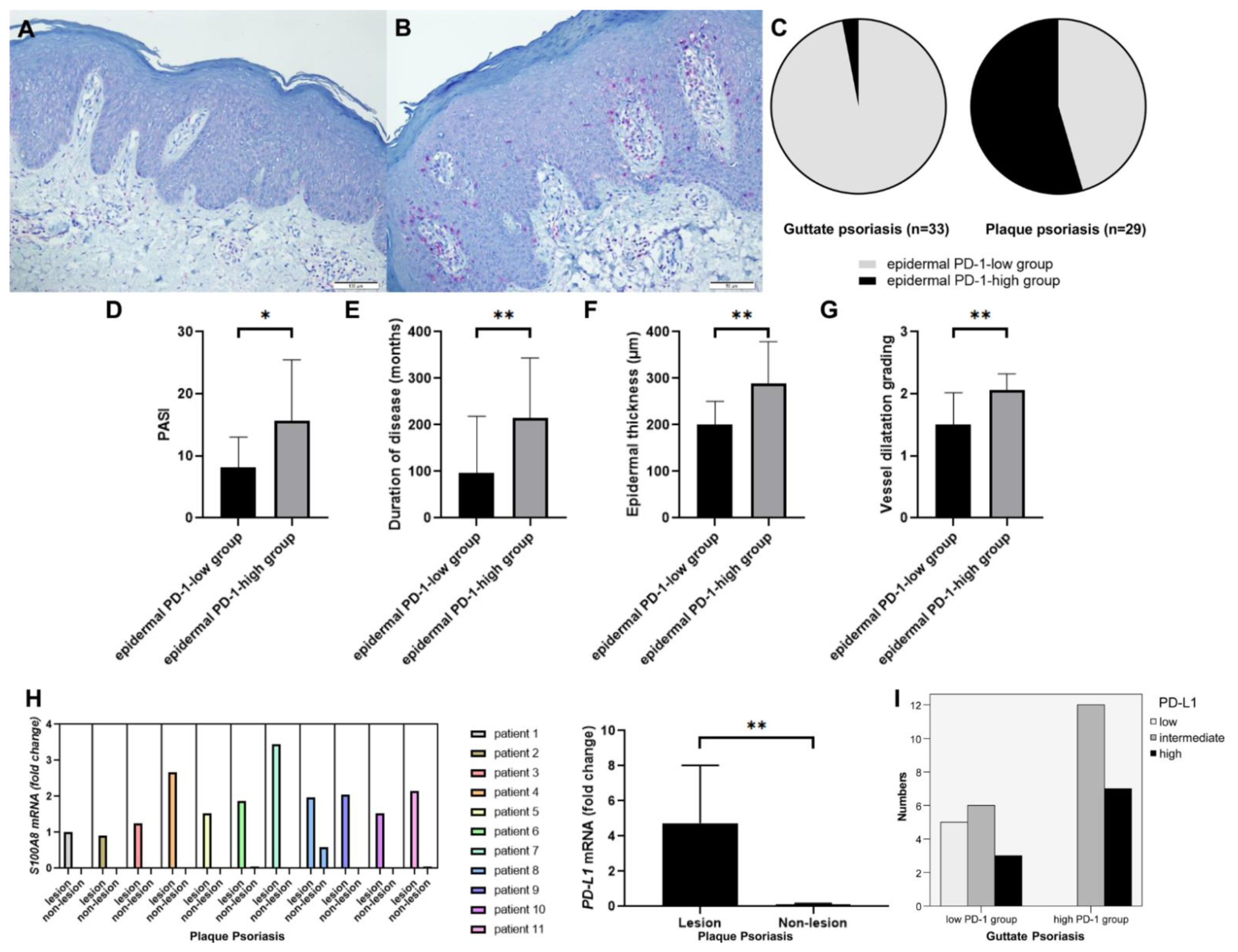
3.1. Clinical and Histopathological Characteristics of CPP according to the Levels of PD-1 Expression
3.2. mRNA Expression Levels of S100A8 and PD-L1 of CPP Lesions Compared to Non-Lesions and PD-L1 Immunohistochemisry in GP
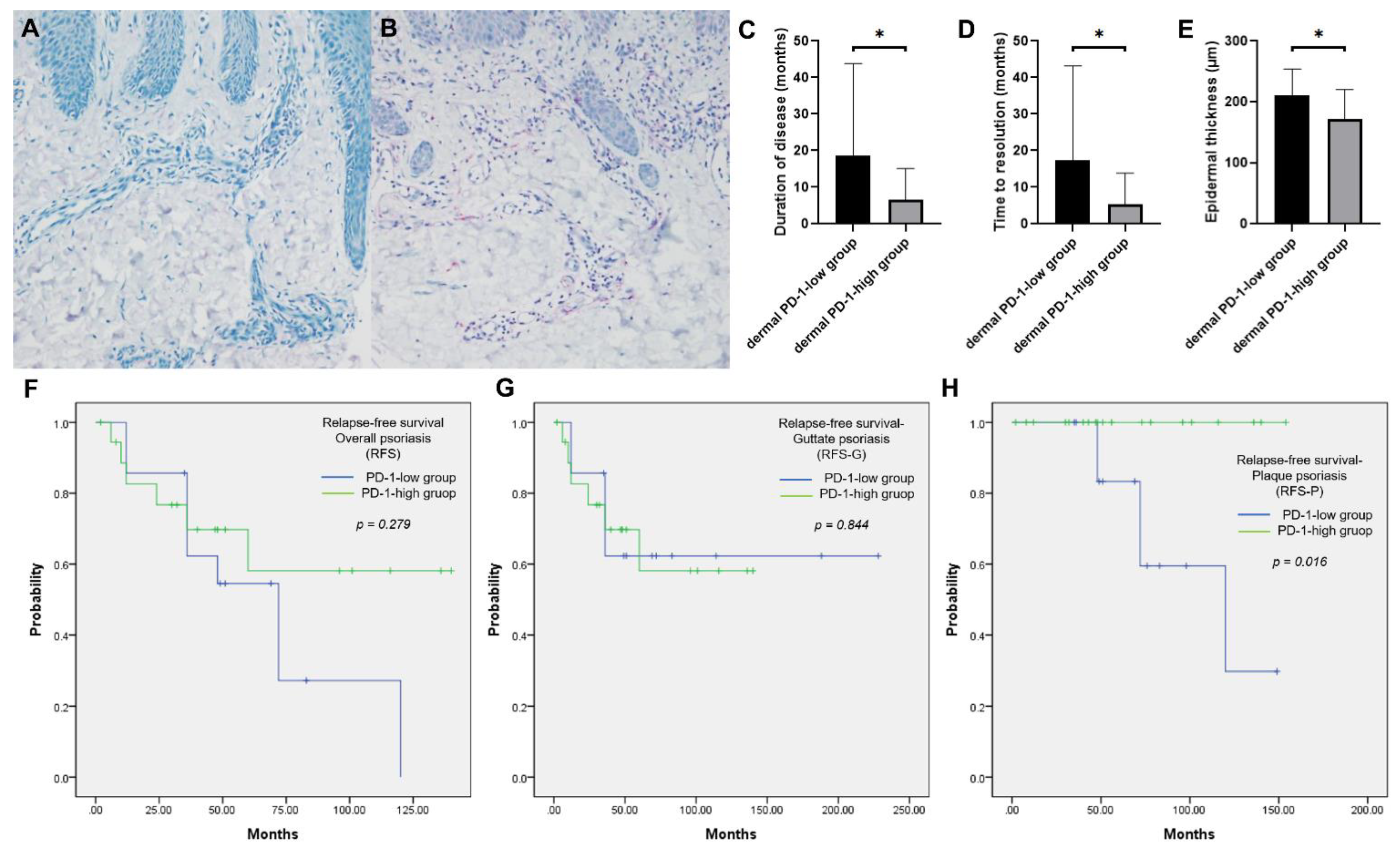
3.3. Clinicoprognostic and Histopathological Characteristics of GP according to the PD-1 Expression Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zaba, L.C.; Fuentes-Duculan, J.; Eungdamrong, N.J.; Abello, M.V.; Novitskaya, I.; Pierson, K.C.; Gonzalez, J.; Krueger, J.G.; Lowes, M.A. Psoriasis is characterized by accumulation of immunostimulatory and Th1/Th17 cell-polarizing myeloid dendritic cells. J. Investig. Dermatol. 2009, 129, 79–88. [Google Scholar] [CrossRef] [Green Version]
- Owczarczyk-Saczonek, A.; Czerwinska, J.; Orylska, M.; Placek, W. Evaluation of selected mechanisms of immune tolerance in psoriasis. Adv. Dermatol. Allergol. 2019, 36, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Bartosinska, J.; Purkot, J.; Kowal, M.; Michalak-Stoma, A.; Krasowska, D.; Chodorowska, G.; Giannopoulos, K. The expression of selected molecular markers of immune tolerance in psoriatic patients. Adv. Clin. Exp. Med. 2018, 27, 721–725. [Google Scholar] [CrossRef]
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef] [Green Version]
- Carter, L.L.; Leach, M.W.; Azoitei, M.L.; Cui, J.; Pelker, J.W.; Jussif, J.; Benoit, S.; Ireland, G.; Luxenberg, D.; Askew, G.R.; et al. PD-1/PD-L1, but not PD-1/PD-L2, interactions regulate the severity of experimental autoimmune encephalomyelitis. J. Neuroimmunol. 2007, 182, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, R.; Ichimura, Y.; Kubota, N.; Saito, A.; Nakamura, Y.; Ishitsuka, Y.; Watanabe, R.; Fujisawa, Y.; Kanzaki, M.; Mizuno, S.; et al. Activation of CD8 T cells accelerates anti-PD-1 antibody-induced psoriasis-like dermatitis through IL-6. Commun. Biol. 2020, 3, 571. [Google Scholar] [CrossRef]
- Peng, S.; Cao, M.; Sun, X.; Zhou, Y.; Chen, C.Y.; Ma, T.; Li, H.; Li, B.; Zhu, B.; Li, X. Recombinant programmed cell death 1 inhibits psoriatic inflammation in imiquimod-treated mice. Int. J. Mol. Med. 2020, 46, 869–879. [Google Scholar] [CrossRef] [PubMed]
- Ko, H.C.; Jwa, S.W.; Song, M.; Kim, M.B.; Kwon, K.S. Clinical course of guttate psoriasis: Long-term follow-up study. J. Dermatol. 2010, 37, 894–899. [Google Scholar] [CrossRef] [PubMed]
- Mallon, E.; Bunce, M.; Savoie, H.; Rowe, A.; Newson, R.; Gotch, F.; Bunker, C.B. HLA-C and guttate psoriasis. Br. J. Dermatol. 2000, 143, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Pfingstler, L.F.; Maroon, M.; Mowad, C. Guttate psoriasis outcomes. Cutis 2016, 97, 140–144. [Google Scholar] [PubMed]
- Kim, S.A.; Choi, J.W.; Kim, B.R.; Youn, S.W. Correlation between histopathologic findings of psoriasis determined using quantitative computer-aided analysis and elements of the Psoriasis Area and Severity Index. J. Am. Acad. Dermatol. 2015, 73, 325–326. [Google Scholar] [CrossRef] [PubMed]
- Yun, W.J.; Lee, D.W.; Chang, S.E.; Yoon, G.S.; Huh, J.R.; Won, C.H.; Lee, M.W.; Kim, S.E.; Kim, B.J.; Moon, K.C.; et al. Role of CD4+CD25high+FOXP3+Regulatory T Cells in Psoriasis. Ann. Dermatol. 2010, 22, 397–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, P.; He, Y.; Wang, H.; Kuang, Y.; Chen, W.; Li, J.; Chen, M.; Zhang, J.; Su, J.; Zhao, S.; et al. The expression of mCTLA-4 in skin lesion inversely correlates with the severity of psoriasis. J. Dermatol. Sci. 2018, 89, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Xu, W.; Yuan, Y.; Ayithan, N.; Imai, Y.; Wu, X.; Miller, H.; Olson, M.; Feng, Y.; Huang, Y.H.; et al. Immune-checkpoint protein VISTA critically regulates the IL-23/IL-17 inflammatory axis. Sci. Rep. 2017, 7, 1485. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.J.; Lee, Y.J.; Choi, M.E.; Yun, K.A.; Won, C.H.; Lee, M.W.; Choi, J.H.; Chang, S.E. Expression of lymphocyte-activating gene 3 and T-cell immunoreceptor with immunoglobulin and ITIM domains in cutaneous melanoma and their correlation with programmed cell death 1 expression in tumor-infiltrating lymphocytes. J. Am. Acad. Dermatol. 2019, 81, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Wang, J.; Deng, X.; Xiong, F.; Ge, J.; Xiang, B.; Wu, X.; Ma, J.; Zhou, M.; Li, X.; et al. Role of the tumor microenvironment in PD-L1/PD-1-mediated tumor immune escape. Mol. Cancer 2019, 18, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bock, M.; Hulstaert, E.; Kruse, V.; Brochez, L. Psoriasis Vulgaris Exacerbation during Treatment with a PD-1 Checkpoint Inhibitor: Case Report and Literature Review. Case Rep. Dermatol. 2018, 10, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Bartosinska, J.; Zakrzewska, E.; Raczkiewicz, D.; Purkot, J.; Michalak-Stoma, A.; Kowal, M.; Krasowska, D.; Chodorowska, G.; Giannopoulos, K. Suppressed Programmed Death 1 Expression on CD4+ and CD8+ T Cells in Psoriatic Patients. Mediat. Inflamm. 2017, 2017, 5385102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okazaki, T.; Honjo, T. PD-1 and PD-1 ligands: From discovery to clinical application. Int. Immunol. 2007, 19, 813–824. [Google Scholar] [CrossRef] [Green Version]
- Pedoeem, A.; Azoulay-Alfaguter, I.; Strazza, M.; Silverman, G.J.; Mor, A. Programmed death-1 pathway in cancer and autoimmunity. Clin. Immunol. 2014, 153, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Tsushima, F.; Iwai, H.; Otsuki, N.; Abe, M.; Hirose, S.; Yamazaki, T.; Akiba, H.; Yagita, H.; Takahashi, Y.; Omura, K.; et al. Preferential contribution of B7-H1 to programmed death-1-mediated regulation of hapten-specific allergic inflammatory responses. Eur. J. Immunol. 2003, 33, 2773–2782. [Google Scholar] [CrossRef] [PubMed]
- Okiyama, N.; Katz, S.I. Programmed cell death 1 (PD-1) regulates the effector function of CD8 T cells via PD-L1 expressed on target keratinocytes. J. Autoimmun. 2014, 53, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugita, S.; Kawazoe, Y.; Imai, A.; Usui, Y.; Takahashi, M.; Mochizuki, M. Suppression of IL-22-producing T helper 22 cells by RPE cells via PD-L1/PD-1 interactions. Investig. Opthalmology Vis. Sci. 2013, 54, 6926–6933. [Google Scholar] [CrossRef] [Green Version]
- Sharpe, A.H.; Pauken, K.E. The diverse functions of the PD1 inhibitory pathway. Nat. Rev. Immunol. 2018, 18, 153–167. [Google Scholar] [CrossRef]
- Yan, K.; Han, L.; Deng, H.; Fang, X.; Zhang, Z.; Huang, G.; Zheng, Z.Z.; Huang, Q.; Xu, J. The distinct role and regulatory mechanism of IL-17 and IFN-gamma in the initiation and development of plaque vs guttate psoriasis. J. Dermatol. Sci. 2018, 92, 106–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, G.; Feng, X.; Na, A.; Jiang, Y.; Cai, Q.; Kong, J.; Ma, H. Acute guttate psoriasis patients have positive streptococcus hemolyticus throat cultures and elevated antistreptococcal M6 protein titers. J. Dermatol. 2005, 32, 91–96. [Google Scholar] [CrossRef]
- Yan, K.X.; Fang, X.; Han, L.; Zhang, Z.H.; Kang, K.F.; Zheng, Z.Z.; Huang, Q. Foxp3+ regulatory T cells and related cytokines differentially expressed in plaque vs. guttate psoriasis vulgaris. Br. J. Dermatol. 2010, 163, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Phadungsaksawasdi, P.; Fujiyama, T.; Kurihara, K.; Ito, T.; Honda, T.; Tokura, Y. PD-1 Expression Defines Epidermal CD8+CD103+ T Cells Preferentially Producing IL-17A and Using Skewed TCR Repertoire in Psoriasis. J. Investig. Dermatol. 2021, 141, 2426–2435.e5. [Google Scholar] [CrossRef] [PubMed]
- Youngnak-Piboonratanakit, P.; Tsushima, F.; Otsuki, N.; Igarashi, H.; Machida, U.; Iwai, H.; Takahashi, Y.; Omura, K.; Yokozeki, H.; Azuma, M. The expression of B7-H1 on keratinocytes in chronic inflammatory mucocutaneous disease and its regulatory role. Immunol. Lett. 2004, 94, 215–222. [Google Scholar] [CrossRef]
- Kim, D.S.; Je, J.H.; Kim, S.H.; Shin, D.; Kim, T.G.; Kim, D.Y.; Kim, S.M.; Lee, M.G. Programmed death-ligand 1, 2 expressions are decreased in the psoriatic epidermis. Arch. Dermatol. Res. 2015, 307, 531–538. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Epidermal PD-1-Low Group (n = 14) | Epidermal PD-1-High Group (n = 15) | p-Value |
|---|---|---|---|
| Sex (n (%)) | 0.298 | ||
| Male | 9 (64.3) | 12 (80.0) | |
| Female | 5 (42.9) | 3 (20.0) | |
| Age (years) | 0.949 | ||
| Range | 12–81 | 17–66 | |
| Mean ± SD | 45.64 ± 19.17 | 46.33 ± 15.15 | |
| Family history of psoriasis | 0.483 | ||
| Yes | 1 (7.1) | 0 (0.0) | |
| No | 13 (92.9) | 15 (100.0) | |
| Preceding upper respiratory infection | 0.483 | ||
| Yes | 1 (7.1) | 0 (0.0) | |
| No | 13 (92.9) | 15 (100.0) | |
| PASI score | 0.014 * | ||
| Range | 1.2–19.8 | 1.6–41.8 | |
| Mean ± SD | 8.20 ± 4.83 | 15.71 ± 9.77 | |
| Pruritus | 0.125 | ||
| Yes | 14 (100.0) | 12 (80.0) | |
| No | 0 (0.0) | 3 (20.0) | |
| Disease duration (months) | 0.009 * | ||
| Range | 1–360 | 36–480 | |
| Mean ± SD | 96.79 ± 122.0 | 215.2 ± 128.2 |
| Characteristics | Epidermal PD-1-Low Group (n = 14) | Epidermal PD-1-High Group (n = 15) | p-Value |
|---|---|---|---|
| Epidermal thickness (µm) | 0.004 * | ||
| Range | 127.92–293.11 | 157.38–475.04 | |
| Mean ± SD | 200.19 ± 20.74 | 289.88 ± 88.88 | |
| Horny layer thickness (µm) | 0.201 | ||
| Range | 11.63–117.40 | 26.83–163.65 | |
| Mean ± SD | 44.23 ± 29.11 | 58.59 ± 36.33 | |
| Rete ridge count (n) | 0.354 | ||
| Range | 8–15 | 8–15 | |
| Mean ± SD | 11.43 ± 2.06 | 12.20 ± 1.70 | |
| Cellular infiltration grading | 0.567 | ||
| Range | 1–3 | 1–3 | |
| Mean ± SD | 1.79 ± 0.80 | 1.93 ± 0.59 | |
| Vessel dilatation grading | 0.002 * | ||
| Range | 1–2 | 2–3 | |
| Mean ± SD | 1.50 ± 0.52 | 2.07 ± 0.26 |
| Characteristics | Dermal PD-1-Low Group (n = 14) | Dermal PD-1-High Group (n = 19) | p-Value |
|---|---|---|---|
| Sex (n (%)) | 0.966 | ||
| Male | 8 (57.1) | 11 (57.9) | |
| Female | 6 (42.9) | 6 (42.9) | |
| Age (years) | 0.086 | ||
| Range | 5–47 | 9–56 | |
| Mean ± SD | 20.86 ± 12.56 | 27.37 ± 11.61 | |
| ≤18 | 8 (57.1) | 5 (26.3) | 0.073 |
| >18 | 6 (42.9) | 14 (73.7) | |
| Family history of psoriasis | 0.424 | ||
| Yes | 1 (7.1) | 0 (0.0) | |
| No | 13 (92.9) | 19 (100.0) | |
| Preceding upper respiratory infection | 0.319 | ||
| Yes | 8 (57.1) | 14 (73.7) | |
| No | 6 (42.9) | 5 (26.3) | |
| PASI score | 0.388 | ||
| Range | 0.90–15.30 | 2.00–14.50 | |
| Mean ± SD | 7.46 ± 4.83 | 6.02 ± 3.88 | |
| BSA (%) | 0.254 | ||
| Range | 1.00–20.00 | 1.00–19.00 | |
| Mean ± SD | 9.96 ± 6.33 | 7.13 ± 6.23 | |
| Pruritus | 0.561 | ||
| Yes | 9 (64.3) | 14 (73.7) | |
| No | 5 (35.7) | 5 (26.3) | |
| Disease duration (months) | 0.002 * | ||
| Range | 3–83 | 1–40 | |
| Mean ± SD | 18.57 ± 25.24 | 6.53 ± 8.59 | |
| ≥4 | 2 (14.3) | 11 (57.9) | 0.011* |
| >4 | 12 (85.7) | 8 (42.1) | |
| Time to disease resolution (months) | 0.008 * | ||
| Range | 1–83 | 1–40 | |
| Mean ± SD | 17.36 ± 25.83 | 5.32 ± 8.53 | |
| Relapse of overall psoriasis | 0.062 | ||
| Yes | 9 (64.3) | 6 (31.6) | |
| No | 5 (35.7) | 13 (68.4) | |
| Relapse of guttate psoriasis | 0.803 | ||
| Yes | 5 (35.7) | 6 (31.6) | |
| No | 9 (64.3) | 13 (68.4) | |
| Relapse of plaque psoriasis | 0.005 * | ||
| Yes | 5 (35.7) | 0 (0.0) | |
| No | 9 (64.3) | 19 (100.0) |
| Characteristics | Dermal PD-1-Low Group (n = 14) | Dermal PD-1-High Group (n = 19) | p-Value |
|---|---|---|---|
| Epidermal thickness (µm) | 0.046 * | ||
| Range | 154.28–295.05 | 92.63–261.91 | |
| Mean ± SD | 210.92 ± 43.02 | 171.96 ± 48.13 | |
| Horny layer thickness (µm) | 0.199 | ||
| Range | 23.27–97.70 | 31.50–112.55 | |
| Mean ± SD | 55.76 ± 18.31 | 50.54 ± 19.23 | |
| Rete ridge count (n) | 0.900 | ||
| Range | 6–14 | 8–14 | |
| Mean ± SD | 11.07 ± 2.40 | 11.11 ± 2.00 | |
| Cellular infiltration grading | 651 | ||
| Range | 1–2 | 1–3 | |
| Mean ± SD | 1.50 ± 0.52 | 1.63 ± 0.60 | 0. |
| Vessel dilatation grading | 0.892 | ||
| Range | 1–3 | 1–3 | |
| Mean ± SD | 1.86 ± 0.66 | 1.74 ± 0.65 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, C.-J.; Yang, H.-J.; Bang, S.-H.; Lee, W.-J.; Won, C.-H.; Lee, M.-W.; Song, Y.; Chang, S.-E. Clinicoprognostic and Histopathological Features of Guttate and Plaque Psoriasis Based on PD-1 Expression. J. Clin. Med. 2021, 10, 5200. https://doi.org/10.3390/jcm10215200
Jung C-J, Yang H-J, Bang S-H, Lee W-J, Won C-H, Lee M-W, Song Y, Chang S-E. Clinicoprognostic and Histopathological Features of Guttate and Plaque Psoriasis Based on PD-1 Expression. Journal of Clinical Medicine. 2021; 10(21):5200. https://doi.org/10.3390/jcm10215200
Chicago/Turabian StyleJung, Chang-Jin, Hee-Joo Yang, Seung-Hyun Bang, Woo-Jin Lee, Chong-Hyun Won, Mi-Woo Lee, Youngsup Song, and Sung-Eun Chang. 2021. "Clinicoprognostic and Histopathological Features of Guttate and Plaque Psoriasis Based on PD-1 Expression" Journal of Clinical Medicine 10, no. 21: 5200. https://doi.org/10.3390/jcm10215200