
Left Atrial Remodeling and Brain Natriuretic Peptide Levels Variation after Left Atrial Appendage Occlusion

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
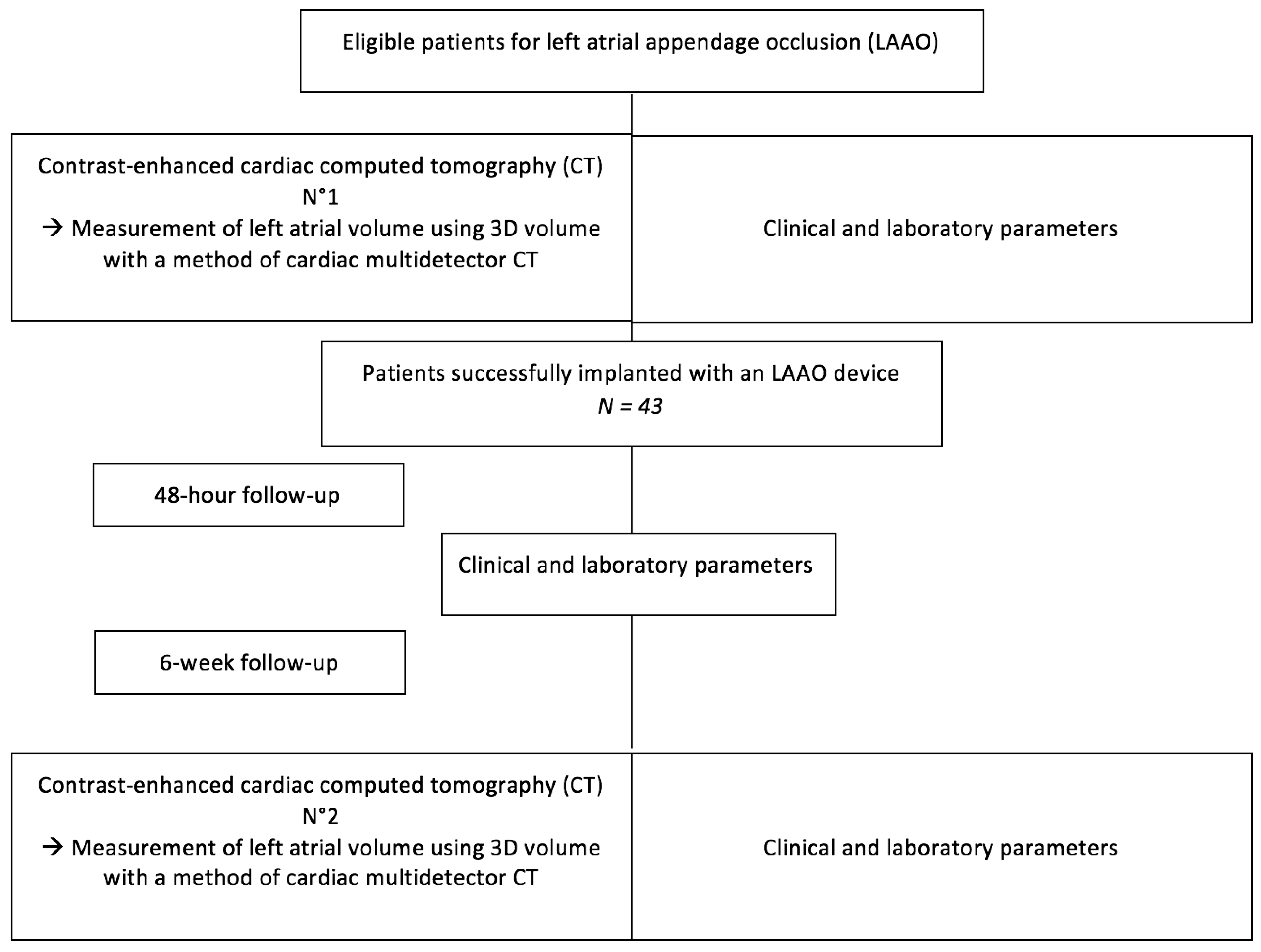
2.1. Study Flow Chart
2.2. Cardiac CT Analysis
2.3. Statistical Analysis
3. Results
3.1. Patients Baseline Characteristics
3.2. CT Results and Left Atrial Remodeling
3.3. Procedural and Post-Procedural Characteristics
3.4. Atrial Remodeling and Natriuretic Peptides
4. Discussion
4.1. Left Atrial Remodeling after LAAO
4.2. Natriuretic Peptide Variation after LAAC
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AF | atrial fibrillation |
| BNP | brain natriuretic peptide |
| LAA | left atrial appendage |
| LAAO | left atrial appendage occlusion |
| OAC | oral anticoagulant |
References
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.H.; McAnulty, J.H., Jr.; Zheng, Z.J.; et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk Factors in Atrial Fi-brillation (ATRIA) Study. JAMA 2001, 285, 2370–2375. [Google Scholar] [CrossRef] [PubMed]
- Regazzoli, D.; Ancona, F.; Trevisi, N.; Guarracini, F.; Radinovic, A.; Oppizzi, M.; Agricola, E.; Marzi, A.; Sora, N.C.; Della Bella, P.; et al. Left Atrial Appendage: Physiology, Pathology, and Role as a Therapeutic Target. BioMed Res. Int. 2015, 2015, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bungard, T.J.; Ghali, W.A.; Teo, K.K.; McAlister, F.A.; Tsuyuki, R.T. Why do patients with atrial fibrillation not receive warfarin? Arch. Intern. Med. 2000, 160, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Saving the Brain: Proper Anticoagulation Therapy for Patients with Atrial Fibrillation. Medical Update. 2016. Available online: https://medicalupdate.pennstatehealth.org/cardiology/saving-the-brain-proper-anticoagulation-therapy-for-patients-with-atrial-fibrillation/ (accessed on 1 May 2020).
- Meier, B.; Blaauw, Y.; Khattab, A.A.; Lewalter, T.; Sievert, H.; Tondo, C.; Glikson, M. EHRA/EAPCI expert consensus statement on catheter-based left atrial appendage occlusion. Europace 2014, 16, 1397–1416. [Google Scholar] [CrossRef] [PubMed]
- Naksuk, N.; Padmanabhan, D.; Yogeswaran, V.; Asirvatham, S.J. Left Atrial Appendage: Embryology, Anatomy, Physiology, Arrhythmia and Therapeutic Intervention. JACC Clin. Electrophysiol. 2016, 2, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Block, P.C.; Burstein, S.; Casale, P.N.; Kramer, P.H.; Teirstein, P.; Williams, D.O.; Reisman, M. Percutaneous left atrial appendage transcatheter occlusion to prevent stroke in high-risk patients with atrial fibrillation: Early clinical experience. Circulation 2002, 105, 1887–1889. [Google Scholar]
- Blackshear, J.L.; Odell, J.A. Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. Ann. Thorac. Surg. 1996, 61, 755–759. [Google Scholar] [CrossRef]
- Reddy, V.Y.; Sievert, H.; Halperin, J.; Doshi, S.K.; Buchbinder, M.; Neuzil, P.; Huber, K.; Whisenant, B.; Kar, S.; Swarup, V.; et al. Percutaneous left atrial appendage closure vs. warfarin for atrial fibrillation: A randomized clinical trial. JAMA 2014, 312, 1988–1998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, D.R.; Kar, S.; Price, M.J.; Whisenant, B.; Sievert, H.; Doshi, S.K.; Huber, K.; Reddy, V.Y. Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: The PREVAIL trial. J. Am. Coll. Cardiol. 2014, 64, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, C.A.; Rembert, J.C.; Greenfield, J.C. Compliance of left atrium with and without left atrium appendage. Am. J. Physiol. Circ. Physiol. 1990, 259, H1006–H1008. [Google Scholar] [CrossRef] [PubMed]
- Mühlenbruch, G.; Das, M.; Hohl, C.; Wildberger, J.E.; Rinck, D.; Flohr, T.G.; Koos, R.; Knackstedt, C.; Günther, R.W.; Mahnken, A.H. Global left ventricular function in cardiac CT. Evaluation of an automated 3D region-growing segmentation algorithm. Eur. Radiol. 2005, 16, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.Y.; Doshi, S.K.; Kar, S.; Gibson, D.N.; Price, M.J.; Huber, K.; Horton, R.P.; Buchbinder, M.; Neuzil, P.; Gordon, N.T.; et al. 5-Year Outcomes after Left Atrial Appendage Closure: From the PREVAIL and PROTECT AF Trials. J. Am. Coll. Cardiol. 2017, 70, 2964–2975. [Google Scholar] [CrossRef] [PubMed]
- Jalal, Z.; Iriart, X.; Dinet, M.; Corneloup, O.; Pillois, X.; Cochet, H.; Thambo, J. Evaluation of left atrial remodelling following percuta-neous left atrial appendage closure. J. Geriatr. Cardiol. 2017, 14, 496–500. [Google Scholar] [PubMed]
- Phan, Q.T.; Shin, S.Y.; Cho, I.-S.; Lee, W.-S.; Won, H.; Sharmin, S.; Lee, D.-Y.; Kim, T.-H.; Kim, C.-J.; Kim, S.-W. Impact of left atrial appendage closure on cardiac functional and structural remodeling: A difference-in-difference analysis of propensity score matched samples. Cardiol. J. 2019, 26, 519–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luani, B.; Groscheck, T.; Genz, C.; Tanev, I.; Rauwolf, T.; Herold, J.; Medunjanin, S.; Schmeisser, A.; Braun-Dullaeus, R.C. Left atrial enlargement and clinical considerations in pa-tients with or without a residual interatrial shunt after closure of the left atrial appendage with the WATCH-MANTM-device. BMC Cardiovasc. Disord. 2017, 17, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapeau, C.; Gutkowska, J.; Schiller, P.W.; Milne, R.W.; Thibault, G.; Garcia, R.; Genest, J.; Cantin, M. Localization of immunoreactive synthetic atrial natriuretic factor (ANF) in the heart of various animal species. J. Histochem. Cytochem. 1985, 33, 541–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakkireddy, D.; Turagam, M.; Afzal, M.R.; Rajasingh, J.; Atkins, D.; Dawn, B.; Di Biase, L.; Bartus, K.; Kar, S.; Natale, A.; et al. Left Atrial Appendage Closure and Systemic Homeostasis: The LAA HOMEOSTASIS Study. J. Am. Coll. Cardiol. 2018, 71, 135–144. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| RAR Group N = 6 | No RAR Group N = 37 | p | |
|---|---|---|---|
| Age, years | 80 ± 5.7 | 75 ± 8.2 | 0.120 |
| Sex (male) | 5 (84) | 23 (62) | 0.304 |
| Hypertension | 5 (84) | 36 (98) | 0.262 |
| Diabetes | 3 (50) | 8 (22) | 0.164 |
| CHA2DS2-VASc score | 4.3 ± 1.21 | 4.2 ± 1.4 | 0.873 |
| HAS BLED score | 4 ± 0.9 | 4.3 ± 1.26 | 0.498 |
| Paroxysmal AF | 1 (16) | 12 (33) | 0.401 |
| Permanent AF | 5 (84) | 25 (67) | 0.401 |
| Prior stroke | 5 (84) | 25 (67) | 0.401 |
| Congestive heart failure | 1 (16) | 6 (16) | 0.681 |
| History of CAD | 1 (16) | 10 (27) | 0.512 |
| History of CABG | 0 (0) | 4 (11) | 0.535 |
| Prior bleeding | 5 (84) | 31 (84) | 0.681 |
| Prior TAVR | 0 (0) | 1 (3) | 0.857 |
| LVEF, % | 60 ± 4 | 56 ± 9 | 0.110 |
| Creatinine clearance, mL/min | 66 ± 14 | 66 ± 26 | 0.919 |
| Pre-procedural NT-proBNP, pg/mL | 486 ± 392 | 2987 ± 6766 | 0.054 |
| Post-procedural NT-proBNP, pg/mL | 1274 ± 1316 | 2156 ± 3248 | 0.402 |
| FU NT-proBNP, pg/mL | 1255 ± 1603 | 2574 ± 3309 | 0.308 |
| Post-procedural troponin, pg/mL | 0.26 ± 0.17 | 0.34 ± 0.39 | 0.370 |
| Indication for LAAO | |||
| Previous bleeding under OAC | 5 (84) | 31 (84) | 0.681 |
| Cerebral amyloid angiopathy | 1 (16) | 4 (11) | |
| High risk of bleeding | 0 (0) | 1 (3) | |
| Stroke despite OAC | 0 (0) | 1 (3) |
| RAR Group N = 6 | No RAR Group N = 37 | p | |
|---|---|---|---|
| Procedure | |||
| Device success | 6 (100) | 37 (100) | 1.00 |
| Technical success | 6 (100) | 36 (97) | 0.875 |
| Procedural success | 6 (100) | 35 (95) | 0.758 |
| Total time in the lab, min | 81 ± 25 | 94 ± 33 | 0.346 |
| Fluoroscopy time, min | 30 ± 18 | 23 ± 13 | 0.407 |
| Contrast used (mL) | 57 ± 19 | 59 ± 34 | 0.868 |
| Mean number of devices used | 1.2 ± 0.5 | 1.2 ± 0.4 | 0.522 |
| Size of the device used | 21 ± 4 | 23 ± 4 | 0.507 |
| In-Hospital MACE | |||
| Vascular complication | 0 (0) | 0 (0) | 1.00 |
| Cardiac tamponnade | 0 (0) | 1 (3) | 0.860 |
| Device migration | 0 (0) | 1 (3) | 0.860 |
| Device thrombus | 1 (16) | 3 (8) | 0.465 |
| Stroke/TIA | 0 (0) | 0 (0) | 1.00 |
| Post-procedure CT | |||
| Time delay CT1-LAAO | 27 ± 41 | 40 ± 44 | 0.502 |
| Time delay LAAO-CT2 | 50 ± 16 | 48 ± 38 | 0.839 |
| Left atrial volume CT1 | 127 ± 46 | 141 ± 66 | 0.551 |
| Left atrial volume CT2 | 151 ± 51 | 138 ± 64 | 0.597 |
| Device thrombus | 0 | 0 | 1.00 |
| No peridevice leak | 6 (100) | 33 (89) | 0.349 |
| Small peridevice leak | 0 (0) | 3 (8) | 0.630 |
| Large peridevice leak | 0 (0) | 1 (3) | 0.860 |
| MACE at 1Y-FU | |||
| FU in days | 801 ± 474 | 736 ± 383 | 0.761 |
| Stroke/TIA | 0 (0) | 0 (0) | 1.00 |
| Cardiac death | 0 (0) | 2 (6) | 0.381 |
| Non cardiac death | 0 (0) | 4 (11) | 0.063 |
| Major bleeding | 1 (16) | 3 (8) | 0.465 |
| Device migration | 0 | 1 (3) | 0.860 |
| Heart failure | 0 (0) | 3 (8) | 0.622 |
| Pre-Procedure CT | Post-Procedure CT | |
|---|---|---|
| Time delay CT-LAAO (day) | 39 ± 43 | 48 ± 36 |
| Left atrial volume CT (mL) | 139 ± 64 | 140 ± 63 |
| Reverse remodeling (LA) | - | 6 (14%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pommier, T.; Leclercq, T.; Guenancia, C.; Richard, C.; Porot, G.; Laurent, G.; Lorgis, L. Left Atrial Remodeling and Brain Natriuretic Peptide Levels Variation after Left Atrial Appendage Occlusion. J. Clin. Med. 2021, 10, 3443. https://doi.org/10.3390/jcm10153443
Pommier T, Leclercq T, Guenancia C, Richard C, Porot G, Laurent G, Lorgis L. Left Atrial Remodeling and Brain Natriuretic Peptide Levels Variation after Left Atrial Appendage Occlusion. Journal of Clinical Medicine. 2021; 10(15):3443. https://doi.org/10.3390/jcm10153443
Chicago/Turabian StylePommier, Thibaut, Thibault Leclercq, Charles Guenancia, Carole Richard, Guillaume Porot, Gabriel Laurent, and Luc Lorgis. 2021. "Left Atrial Remodeling and Brain Natriuretic Peptide Levels Variation after Left Atrial Appendage Occlusion" Journal of Clinical Medicine 10, no. 15: 3443. https://doi.org/10.3390/jcm10153443