
Localized Atrial Tachycardia and Dispersion Regions in Atrial Fibrillation: Evidence of Spatial Concordance

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.1.1. Peri-Procedural Aspects
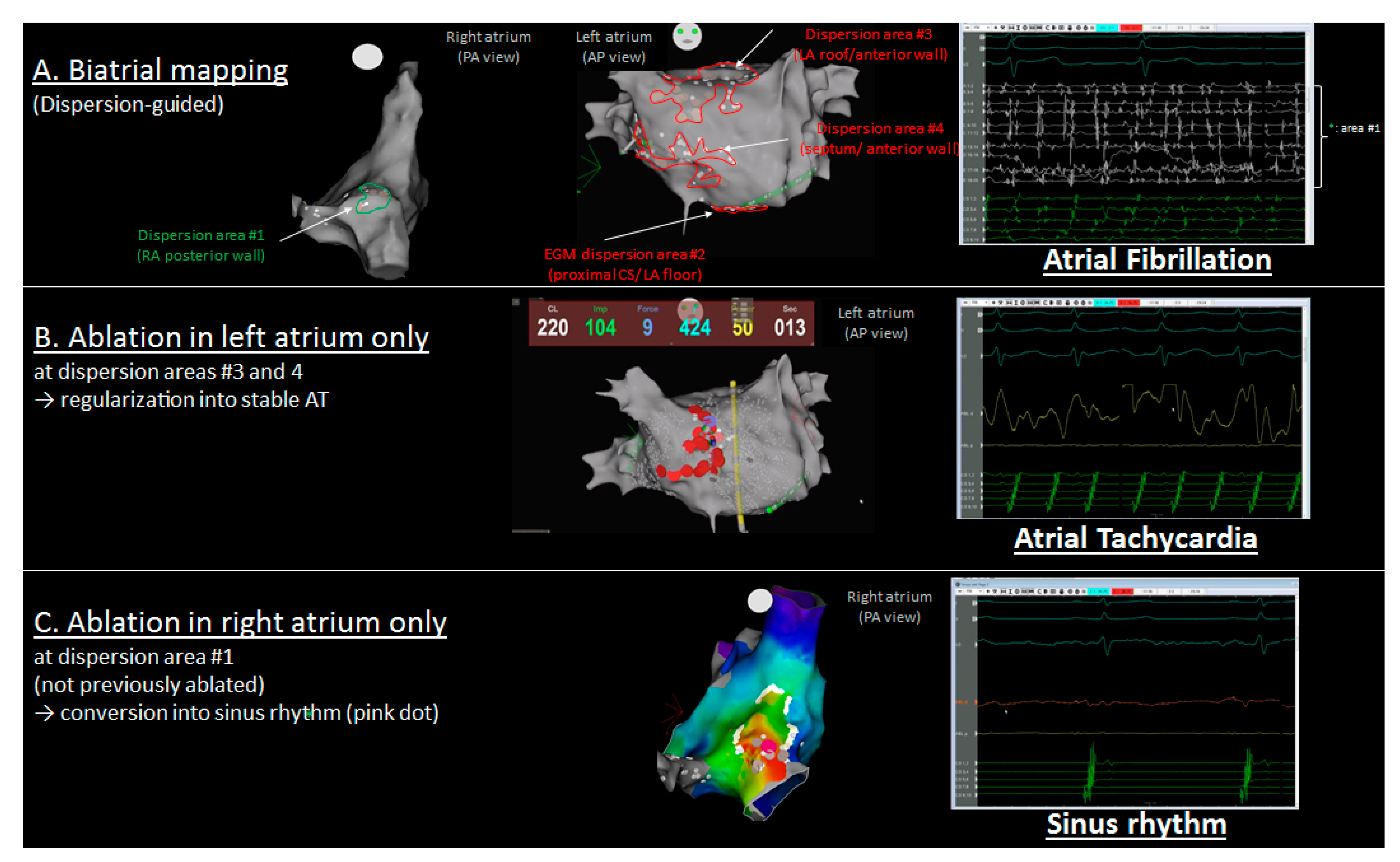
2.1.2. Mapping Protocol
2.1.3. Ablation Protocol
2.1.4. AT Mapping and Classification
3. Statistical Analysis
4. Results
4.1. Population
4.2. Procedure, Mapping, and Analysis
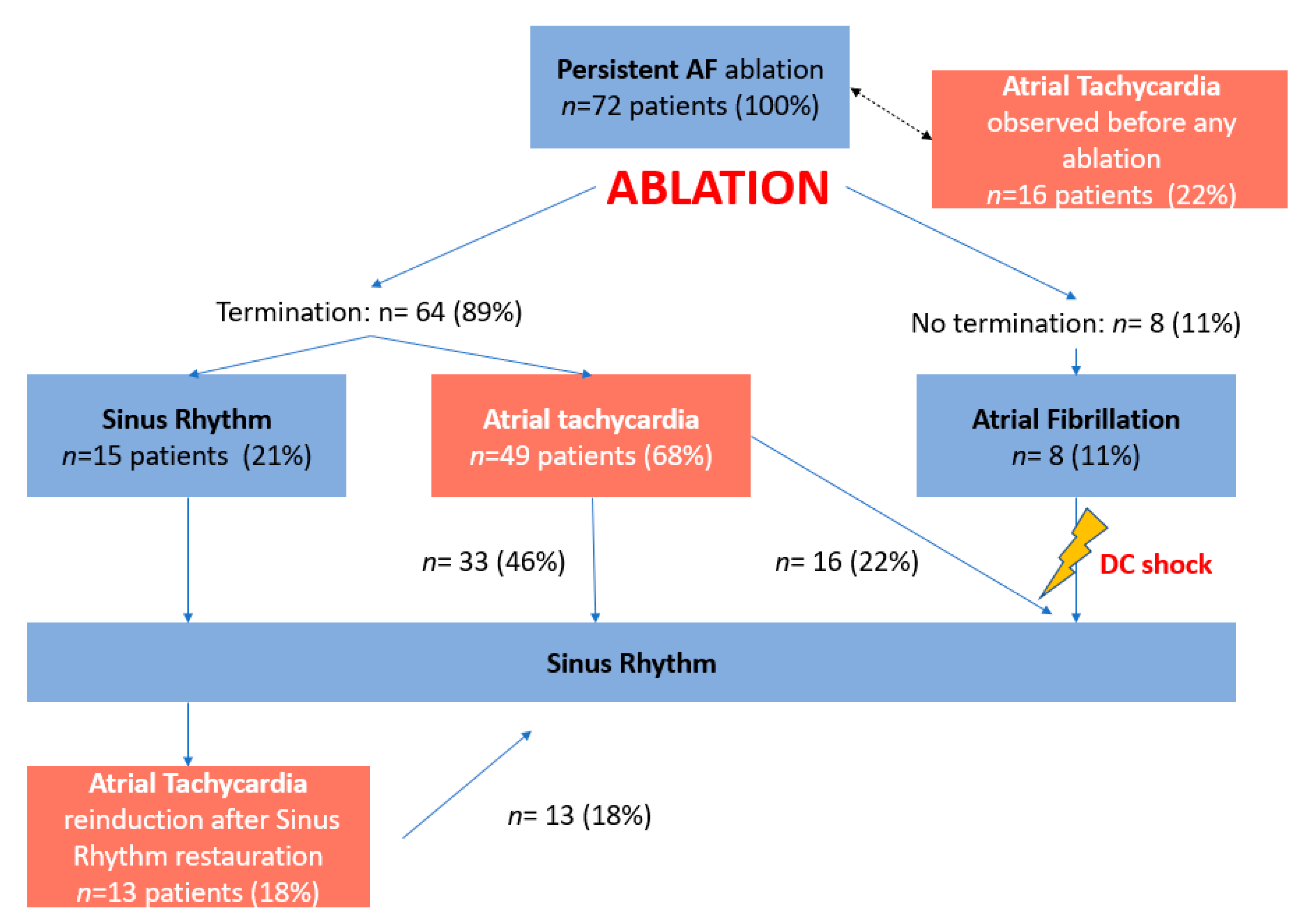
4.3. Atrial Tachycardias
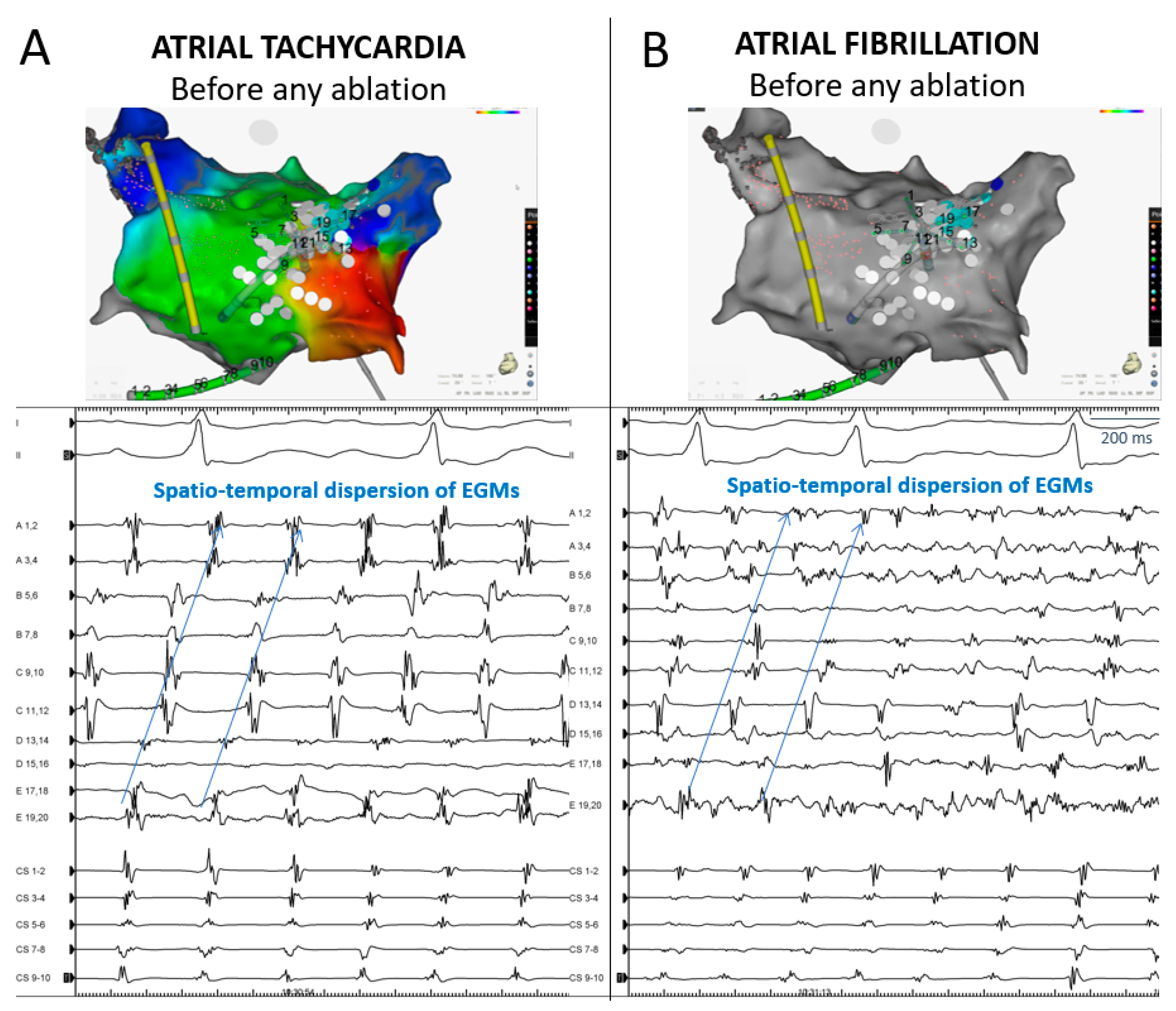
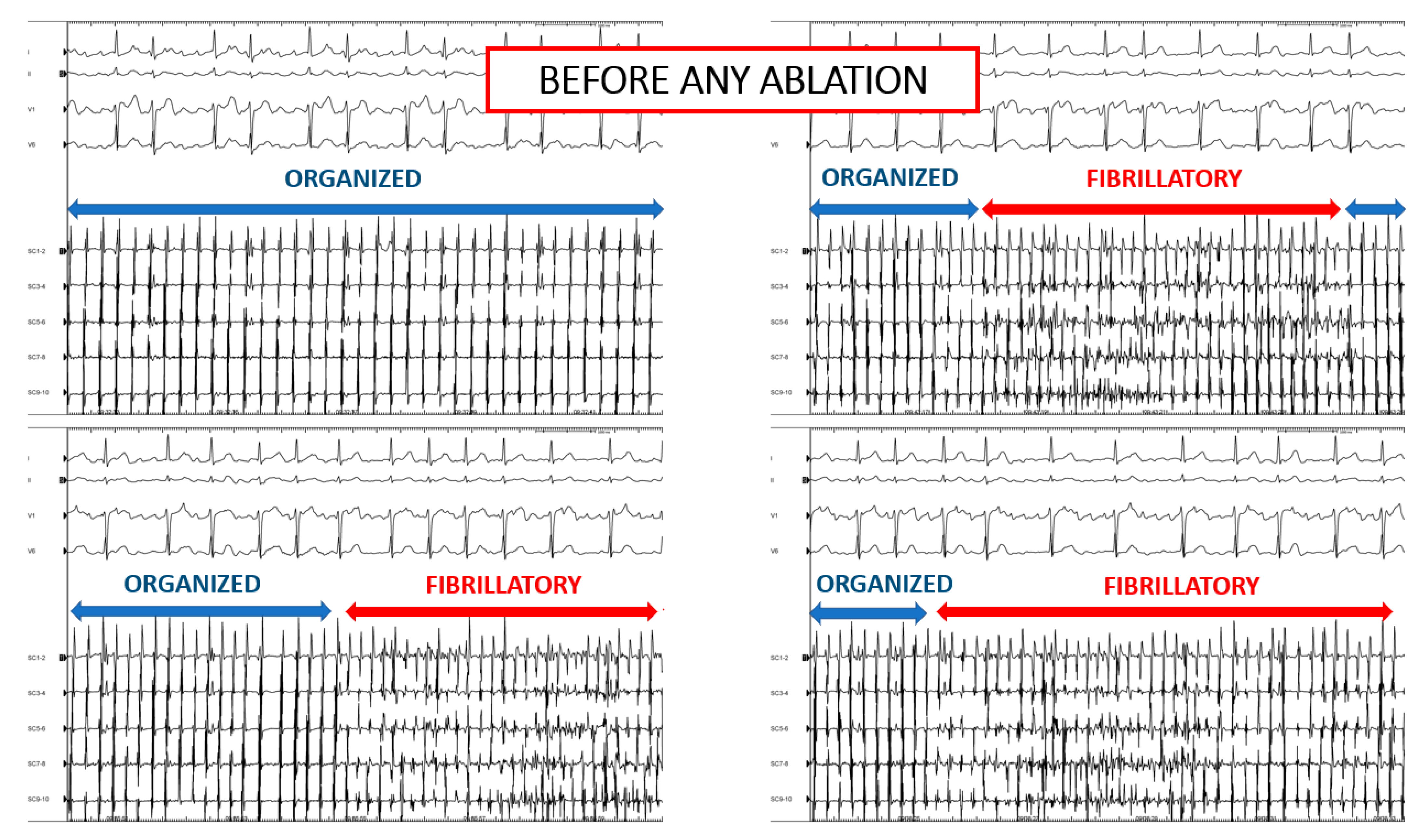
4.4. AT before Any Ablation
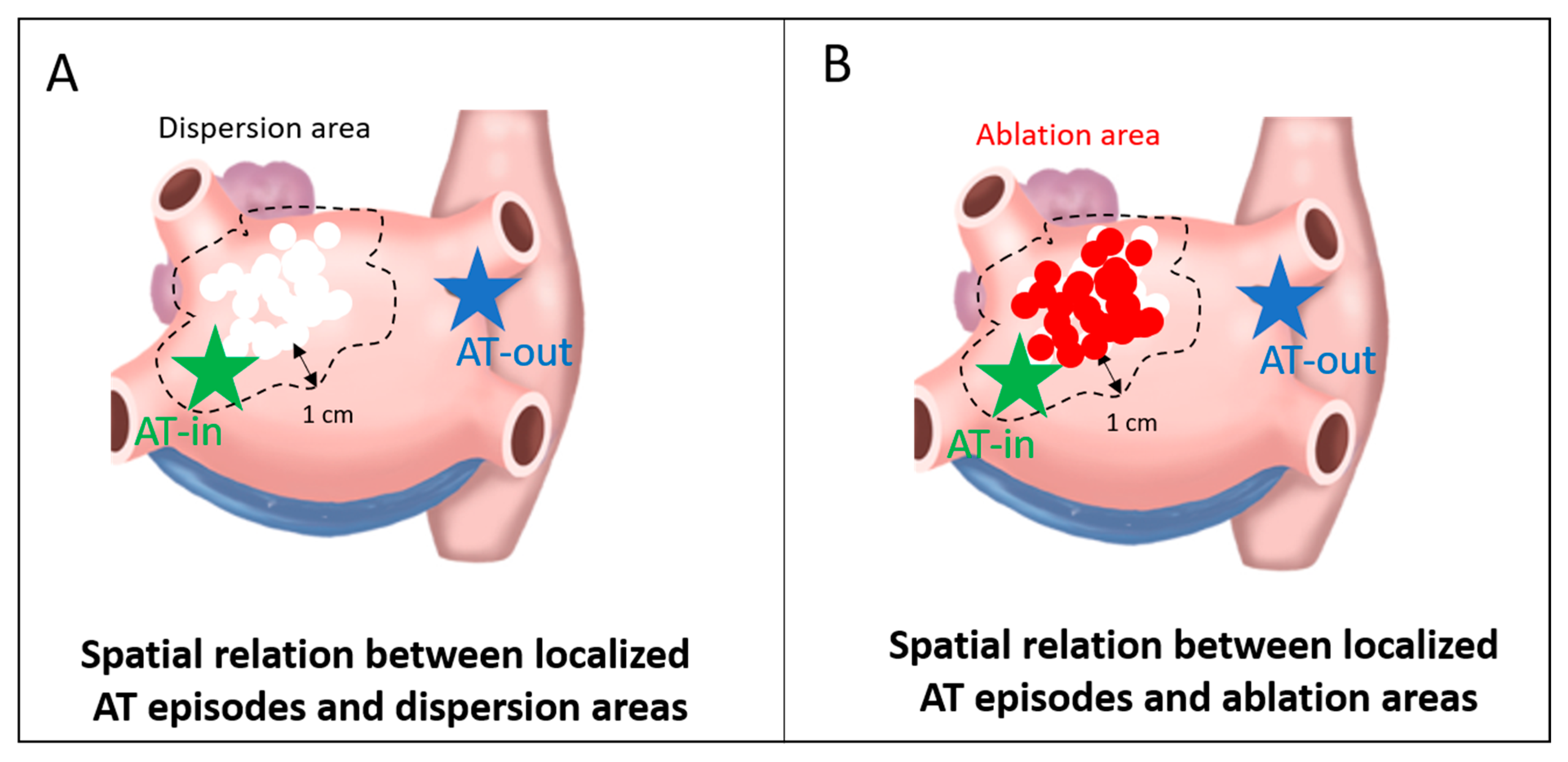
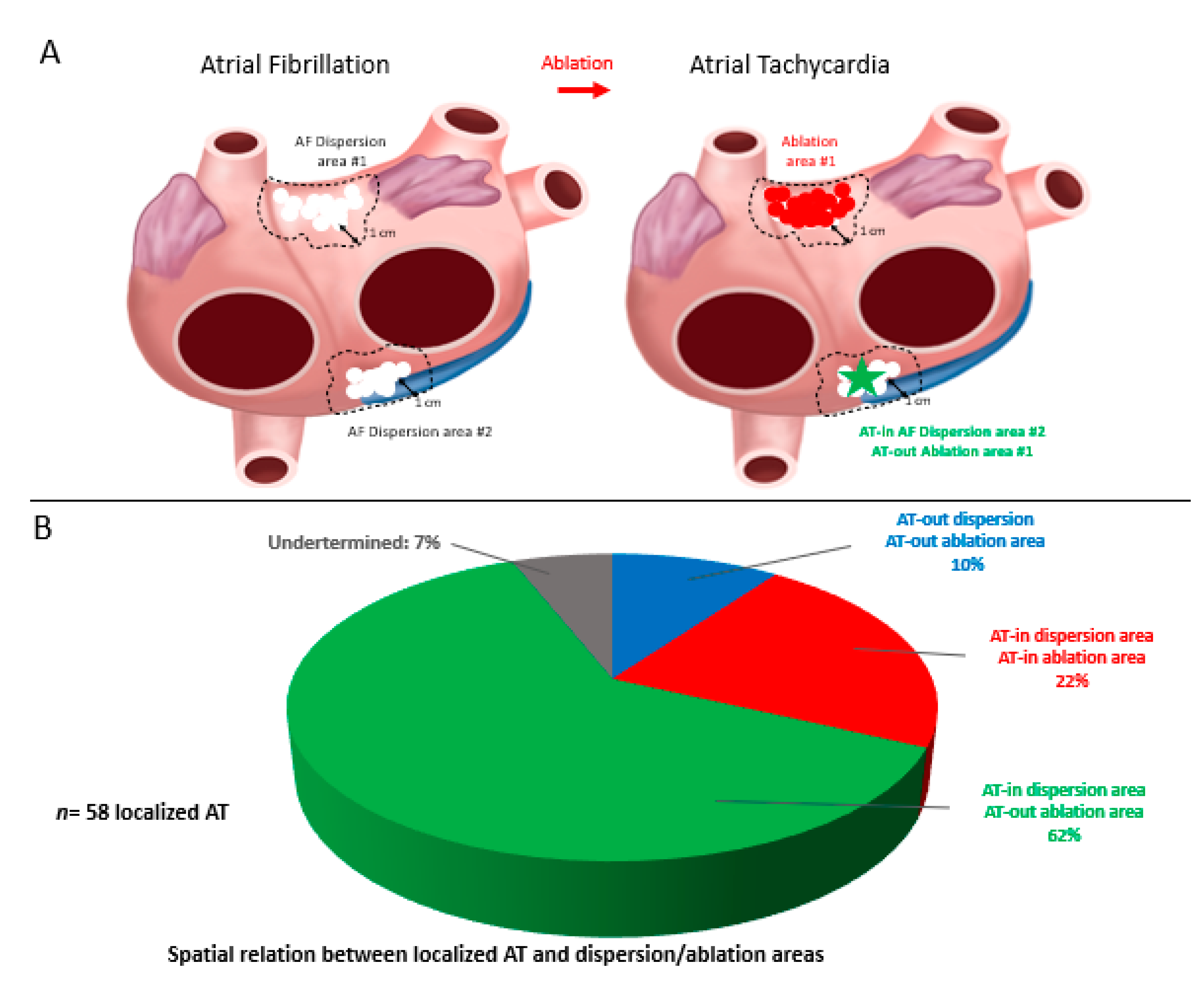
4.5. Spatial Relationship between Localized ATs and Dispersion Regions
4.6. Redo Ablation Procedures
5. Discussion
5.1. Spatial Concordance between Localized AT and AF Drivers
5.2. Mechanistic Significance of Organized AT in Patients with AF
5.3. Clinical Relevance in the Clinical Cardiac Electrophysiological Laboratory
5.4. Ablation-Related ATs
6. Study Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAD | antiarrhythmic drug |
| AF | atrial fibrillation |
| AFCL | atrial fibrillation cycle length |
| AT | atrial tachycardia |
| CFAE | complex fractionated atrial electrogram |
| CL | cycle length |
| CS | coronary sinus |
| DCCV | direct current electrical cardioversion |
| LA | left atrial/atrium |
| PV | pulmonary vein |
| PVI | pulmonary vein isolation |
| RA | right atrial/atrium |
| RF | radiofrequency |
| SR | sinus rhythm |
References
- Nademanee, K.; McKenzie, J.; Kosar, E.; Schwab, M.; Sunsaneewitayakul, B.; Vasavakul, T.; Khunnawat, C.; Ngarmukos, T. A new approach for catheter ablation of atrial fibrillation: Mapping of the electrophysiologic substrate. J. Am. Coll. Cardiol. 2004, 43, 2044–2053. [Google Scholar] [CrossRef] [Green Version]
- Jadidi, A.S.; Lehrmann, H.; Keyl, C.; Sorrel, J.; Markstein, V.; Minners, J.; Park, C.-I.; Denis, A.; Jaïs, P.; Hocini, M.; et al. Ablation of Persistent Atrial Fibrillation Targeting Low-Voltage Areas With Selective Activation Characteristics. Circ. Arrhythmia Electrophysiol. 2016, 9, e002962. [Google Scholar] [CrossRef] [PubMed]
- Seitz, J.; Bars, C.; Théodore, G.; Beurtheret, S.; Lellouche, N.; Bremondy, M.; Ferracci, A.; Faure, J.; Penaranda, G.; Yamazaki, M.; et al. AF Ablation Guided by Spatiotemporal Electrogram Dispersion Without Pulmonary Vein Isolation. J. Am. Coll. Cardiol. 2017, 69, 303–321. [Google Scholar] [CrossRef]
- Lin, R.; Zeng, C.; Xu, K.; Wu, S.; Qin, M.; Liu, X. Dispersion-guided ablation in conjunction with circumferential pulmonary vein isolation is superior to stepwise ablation approach for persistent atrial fibrillation. Int. J. Cardiol. 2019, 278, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Kottkamp, H.; Berg, J.; Bender, R.; Rieger, A.; Schreiber, D. Box Isolation of Fibrotic Areas (BIFA): A Patient-Tailored Substrate Modification Approach for Ablation of Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2016, 27, 22–30. [Google Scholar] [CrossRef]
- Narayan, S.M.; Krummen, D.E.; Shivkumar, K.; Clopton, P.; Rappel, W.-J.; Miller, J.M. Treatment of Atrial Fibrillation by the Ablation of Localized Sources: CONFIRM (Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation) Trial. J. Am. Coll. Cardiol. 2012, 60, 628–636. [Google Scholar] [CrossRef] [Green Version]
- Haissaguerre, M.; Hocini, M.; Denis, A.; Shah, A.J.; Komatsu, Y.; Yamashita, S.; Daly, M.; Amraoui, S.; Zellerhoff, S.; Picat, M.-Q.; et al. Driver Domains in Persistent Atrial Fibrillation. Circulation 2014, 130, 530–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherr, D.; Khairy, P.; Miyazaki, S.; Aurillac-Lavignolle, V.; Pascale, P.; Wilton, S.B.; Ramoul, K.; Komatsu, Y.; Roten, L.; Jadidi, A.; et al. Five-Year Outcome of Catheter Ablation of Persistent Atrial Fibrillation Using Termination of Atrial Fibrillation as a Procedural Endpoint. Circ. Arrhythmia Electrophysiol. 2015, 8, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Tutuianu, C.; Szilagyi, J. Atrial Tachycardias Following Atrial Fibrillation Ablation. Curr. Cardiol. Rev. 2014, 11, 149–156. [Google Scholar] [CrossRef] [Green Version]
- Kuck, K.-H.; Brugada, J.; Fürnkranz, A.; Metzner, A.; Ouyang, F.; Chun, K.J.; Elvan, A.; Arentz, T.; Bestehorn, K.; Pocock, S.J.; et al. Cryoballoon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2016, 374, 2235–2245. [Google Scholar] [CrossRef]
- Yamashita, S.; Hooks, D.A.; Shah, A.; Relan, J.; Cheniti, G.; Kitamura, T.; Berte, B.; Mahida, S.; Sellal, J.-M.; Al Jefairi, N.; et al. Atrial tachycardias: Cause or effect with ablation of persistent atrial fibrillation? J. Cardiovasc. Electrophysiol. 2017, 29, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Ban, J.-E.; Chen, Y.-L.; Park, H.-C.; Lee, H.-S.; Lee, D.-I.; Choi, J.-I.; Lim, H.-E.; Park, S.-W.; Kim, Y.-H. Relationship Between Complex Fractionated Atrial Electrograms During Atrial Fibrillation and the Critical Site of Atrial Tachycardia That Develops After Catheter Ablation for Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2014, 25, 146–153. [Google Scholar] [CrossRef]
- Mandapati, R.; Skanes, A.; Chen, J.; Berenfeld, O.; Jalife, J. Stable Microreentrant Sources as a Mechanism of Atrial Fibrillation in the Isolated Sheep Heart. Circulation 2000, 101, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Berenfeld, O.; Zaitsev, A.V.; Mironov, S.F.; Pertsov, A.M.; Jalife, J. Frequency-Dependent Breakdown of Wave Propagation Into Fibrillatory Conduction Across the Pectinate Muscle Network in the Isolated Sheep Right Atrium. Circ. Res. 2002, 90, 1173–1180. [Google Scholar] [CrossRef] [Green Version]
- Berenfeld, O. Quantifying activation frequency in atrial fibrillation to establish underlying mechanisms and ablation guidance. Heart Rhythm. 2007, 4, 1225–1234. [Google Scholar] [CrossRef] [PubMed]
- Atienza, F.; Almendral, J.; Jalife, J.; Zlochiver, S.; Ploutz-Snyder, R.; Torrecilla, E.G.; Arenal, Á.; Kalifa, J.; Fernández-Avilés, F.; Berenfeld, O. Real-time dominant frequency mapping and ablation of dominant frequency sites in atrial fibrillation with left-to-right frequency gradients predicts long-term maintenance of sinus rhythm. Heart Rhythm. 2009, 6, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Haïssaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Todd, D.M.; Fynn, S.P.; Hobbs, W.J.; Fitzpatrick, A.P.; Garratt, C.J. Prevalence and significance of focal sources of atrial arrhythmia in patients undergoing cardioversion of persistent atrial fibrillation. J. Cardiovasc. Electrophysiol. 2000, 11, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Israel, C.W.; Ehrlich, J.R.; Grönefeld, G.; Klesius, A.; Lawo, T.; Lemke, B.; Hohnloser, S.H. Prevalence, characteristics and clinical implications of regular atrial tachyarrhythmias in patients with atrial fibrillation: Insights from a study using a new implantable device. J. Am. Coll. Cardiol. 2001, 38, 355–363. [Google Scholar] [CrossRef] [Green Version]
- Nabar, A. Class IC antiarrhythmic drug induced atrial flutter: Electrocardiographic and electrophysiological findings and their importance for long term outcome after right atrial isthmus ablation. Heart Br. Card. Soc. 2001, 85, 424–429. [Google Scholar] [CrossRef] [Green Version]
- Bianconi, L.; Mennuni, M.; Lukic, V.; Castro, A.; Chieffi, M.; Santini, M. Effects of oral propafenone administration before electrical cardioversion of chronic atrial fibrillation: A placebo-controlled study. J. Am. Coll. Cardiol. 1996, 28, 700–706. [Google Scholar] [CrossRef]
- Baykaner, T.; Zaman, J.A.; Rogers, A.J.; Navara, R.; Alhusseini, M.; Borne, R.T.; Park, S.; Wang, P.J.; Krummen, D.E.; Sauer, W.H.; et al. Spatial relationship of sites for atrial fibrillation drivers and atrial tachycardia in patients with both arrhythmias. Int. J. Cardiol. 2017, 248, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Chugh, A.; Ulfarsson, M.; Good, E.; Kühne, M.; Crawford, T.; Sarrazin, J.F.; Chalfoun, N.; Wells, D.; Boonyapisit, W.; et al. Relationship between the spectral characteristics of atrial fibrillation and atrial tachycardias that occur after catheter ablation of atrial fibrillation. Heart Rhythm. 2009, 6, 11–17. [Google Scholar] [CrossRef]
- Rostock, T.; Salukhe, T.V.; Hoffmann, B.A.; Steven, D.; Berner, I.; Müllerleile, K.; Theis, C.; Bock, K.; Servatius, H.; Sultan, A.; et al. Prognostic Role of Subsequent Atrial Tachycardias Occurring During Ablation of Persistent Atrial Fibrillation. Circ. Arrhythmia Electrophysiol. 2013, 6, 1059–1065. [Google Scholar] [CrossRef] [Green Version]
- Gerstenfeld, E.P.; Dixit, S.; Bala, R.; Callans, D.J.; Lin, D.; Sauer, W.; Garcia, F.; Cooper, J.; Russo, A.M.; Marchlinski, F. Surface electrocardiogram characteristics of atrial tachycardias occurring after pulmonary vein isolation. Heart Rhythm. 2007, 4, 1136–1143. [Google Scholar] [CrossRef]
- Karch, M.R.; Zrenner, B.; Deisenhofer, I.; Schreieck, J.; Ndrepepa, G.; Dong, J.; Lamprecht, K.; Barthel, P.; Luciani, E.; Schömig, A.; et al. Freedom From Atrial Tachyarrhythmias After Catheter Ablation of Atrial Fibrillation. Circulation 2005, 111, 2875–2880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwai, S.; Takahashi, Y.; Masumura, M.; Yamashita, S.; Doi, J.; Yamamoto, T.; Sakakibara, A.; Nomoto, H.; Yoshida, Y.; Sugiyama, T.; et al. Occurrence of Focal Atrial Tachycardia During the Ablation Procedure Is Associated with Arrhythmia Recurrence After Termination of Persistent Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2017, 28, 489–497. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Population | n = 72 |
|---|---|
| Age, years | 67.2 ± 9 |
| Female | 19 (26%) |
| AF type | |
| Short-standing persistent * | 38 (53%) |
| Long-standing persistent ** | 14 (19%) |
| Persistent/unknown duration | 20 (28%) |
| Structural heart disease | 25 (39%) |
| Systemic hypertension | 26 (39%) |
| Diabetes mellitus | 9 (12.5%) |
| Obesity (BMI > 30) | 4 (5.5%) |
| LVEF (%) | 46 ± 19 |
| LA volume, mL | 153 ± 41 |
| RA volume, mL | 135 ± 47 |
| Spontaneous AF at the beginning of procedure | 47 (65%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gitenay, E.; Bars, C.; Bremondy, M.; Ayari, A.; Maillot, N.; Baptiste, F.; Taormina, A.; Fofana, A.; Siame, S.; Kalifa, J.; et al. Localized Atrial Tachycardia and Dispersion Regions in Atrial Fibrillation: Evidence of Spatial Concordance. J. Clin. Med. 2021, 10, 3170. https://doi.org/10.3390/jcm10143170
Gitenay E, Bars C, Bremondy M, Ayari A, Maillot N, Baptiste F, Taormina A, Fofana A, Siame S, Kalifa J, et al. Localized Atrial Tachycardia and Dispersion Regions in Atrial Fibrillation: Evidence of Spatial Concordance. Journal of Clinical Medicine. 2021; 10(14):3170. https://doi.org/10.3390/jcm10143170
Chicago/Turabian StyleGitenay, Edouard, Clément Bars, Michel Bremondy, Anis Ayari, Nicolas Maillot, Florian Baptiste, Antonio Taormina, Aicha Fofana, Sabrina Siame, Jérôme Kalifa, and et al. 2021. "Localized Atrial Tachycardia and Dispersion Regions in Atrial Fibrillation: Evidence of Spatial Concordance" Journal of Clinical Medicine 10, no. 14: 3170. https://doi.org/10.3390/jcm10143170