
Physiological Basis of Extracorporeal Membrane Oxygenation and Extracorporeal Carbon Dioxide Removal in Respiratory Failure

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Definitions
- (1)
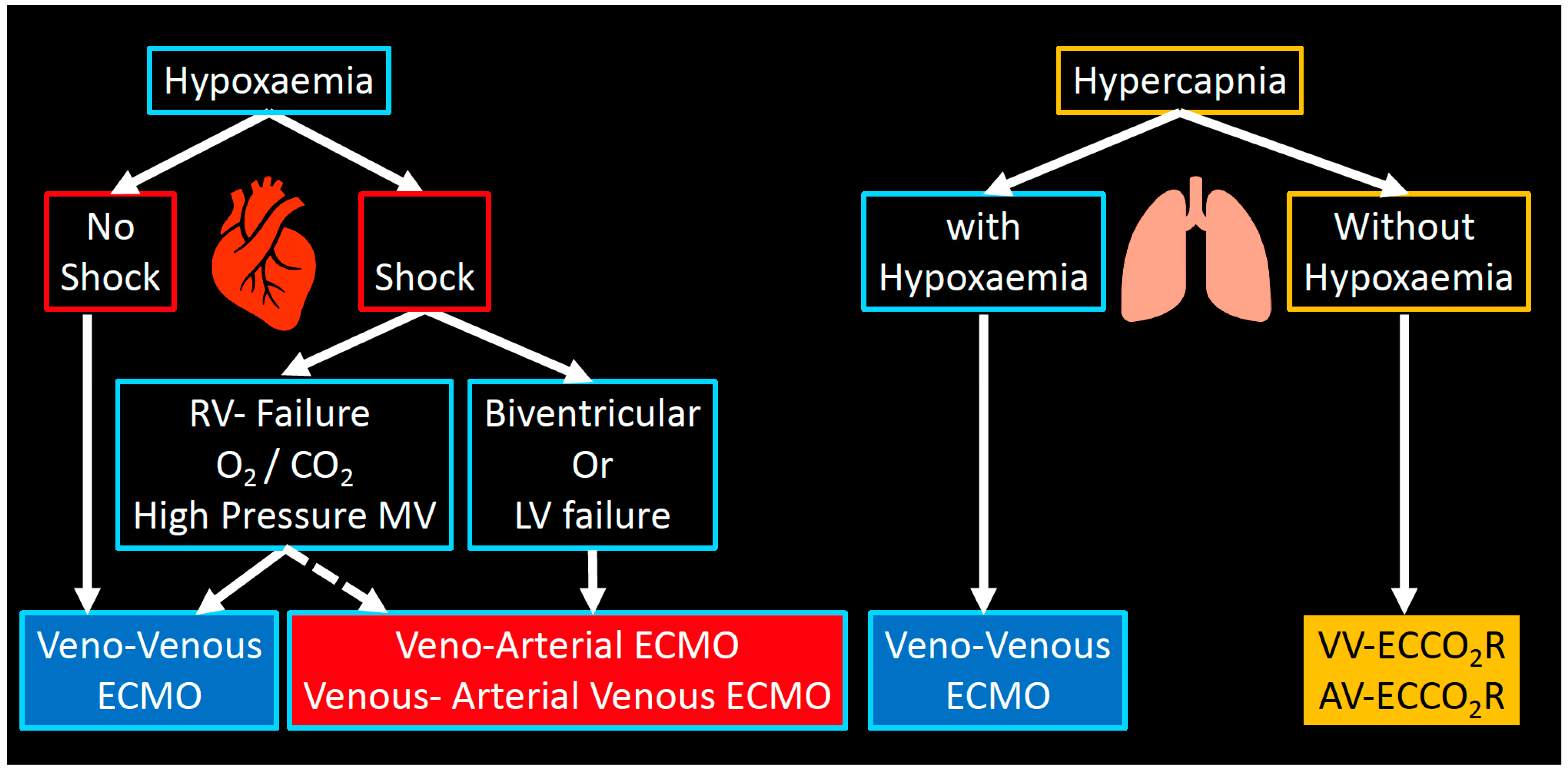
- In veno-venous extracorporeal membrane oxygenation (VV-ECMO), deoxygenated blood is drained from a central vein (e.g., inferior or superior vena cava), pumped through a “membrane lung” or oxygenator, and then reinfused—fully oxygenated and decarboxylated—into a central vein. The gas exchange is driven by the diffusion gradient across the membrane. Fresh gas (sweep gas flow, SGF) flows, countercurrent to the blood, in the lumen of the membrane’s hollow fibers, therefore maintaining a favourable gradient for oxygenation and decarboxylation. To achieve this, the blood flows used in ECMO range between 3 and 7 L/min.
- (2)
- Extracorporeal carbon dioxide removal (ECCO2R) operates in a similar way to VV-ECMO but at much lower blood flow (usually < 1–1.5 L/min). The main difference between VV-ECMO and ECCO2R consists in the fact that CO2 removal has a linear kinetic and is more efficient than oxygenation: for this reason, ECCO2R can be delivered at much lower flows and with smaller cannulae. Although ECCO2R does not provide significant oxygenation, it is able to remove 25–50% of the metabolically produced carbon dioxide.
- (3)
- Veno-arterial extracorporeal membrane oxygenation (VA-ECMO): VA-ECMO provides support for the heart (e.g., biventricular failure). Hybrid configurations for peripheral ECMO (V-VA-ECMO), where there is drainage of the venous system and return into a central artery and a central vein to assist both heart and lung (e.g., severe ARDS and septic cardiomyopathy with cardiogenic shock).
3. Physiology of ECMO
3.1. Oxygenation
3.1.1. Oxygen Delivery and Demand
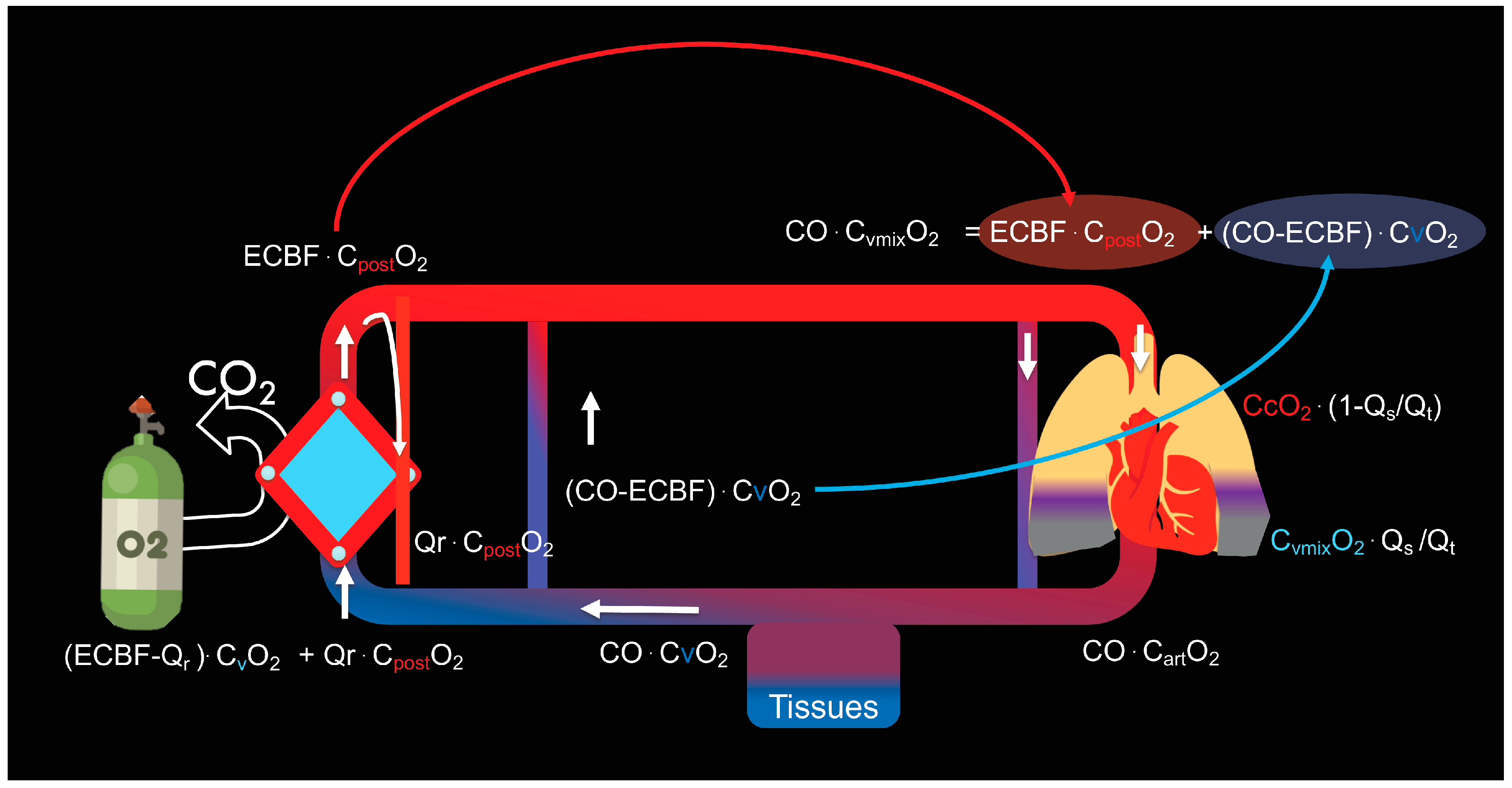
3.1.2. Shunt of the Membrane Lung
3.1.3. Recirculation
- Low SaO2 and poor increase in SaO2 at higher ECBF
- Increase in Spre-oxyO2 and reduction in SaO2 over time
- Ppre-oxyO2 > 10% of Ppost-oxyO2
- Spre-oxyO2 > 75% with SaO2 < 85%
3.1.4. Gas Exchange in Partially Dependent Patients
3.2. Carbon Dioxide Removal
3.2.1. Determinants of CO2 Removal
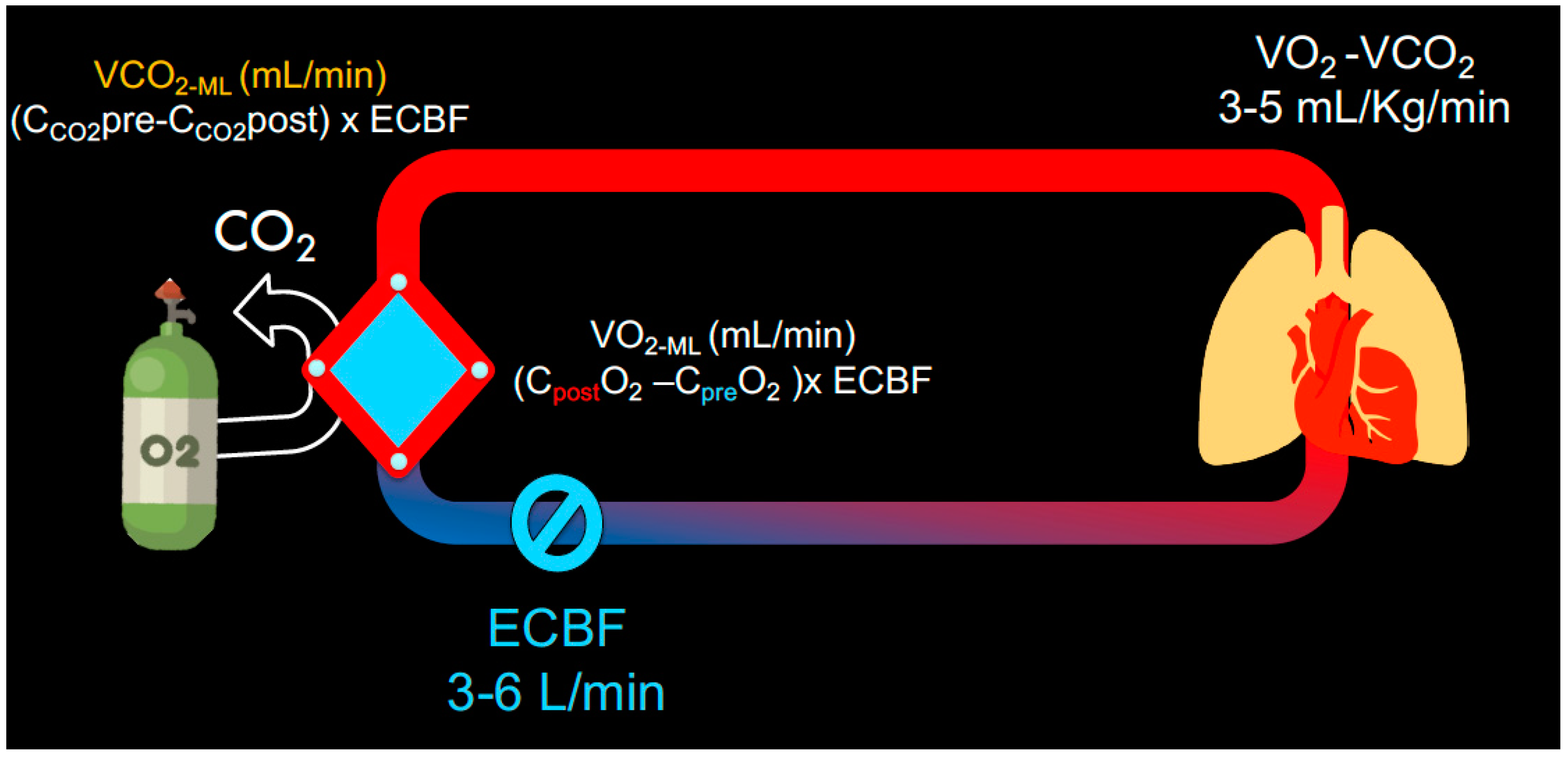
3.2.2. Carbon Dioxide Transfer across the Membrane
- (1)
- The first method is based on the difference in CO2 content of the blood at each side of the membrane:
- (2)
- Alternatively, we can measure the concentration of CO2 from the sweep gas outlet of the membrane:
3.2.3. Membrane Dead Space
3.3. Monitoring of Gas Exchange
- A pre-oxygenator blood gas
- A post-oxygenator blood gas
- An arterial blood gas
- A mixed venous blood gas (if a pulmonary artery catheter is in place)
- Expired PCO2 from the sweep gas port (if possible)
- Native lung minute ventilation
- VCO2 native lung (via volumetric capnography)
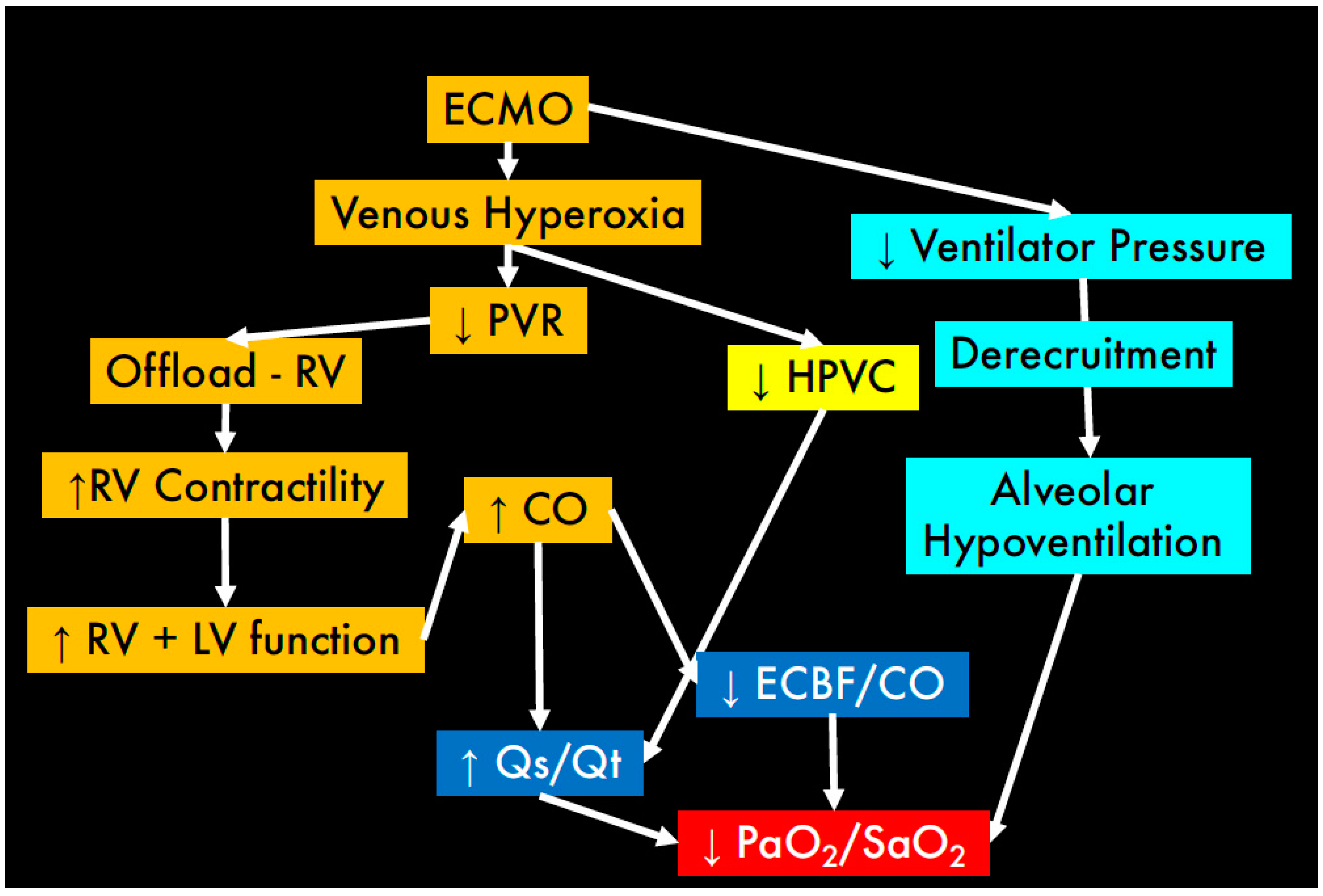
3.4. ECMO Initiation: Physiological Considerations
- (1)
- Abolition of hypoxic vasoconstriction due to the increased oxygen in the mixed venous blood as a consequence of ECMO;
- (2)
- Changes in the respiratory quotient of the natural lung (that is consequent to the decarboxylated blood that arrives to the pulmonary artery);
3.5. Weaning, “Trial off” and Decannulation
- Step 1: Decrease FdO2
- Step 2: Reduction in Sweep Gas Flow
3.6. Physiology of ECCO2R
3.7. Principles of CO2 Diffusion and Transport
3.8. Determinants of CO2 Transfer
- Extracorporeal blood flow (ECBF)
- Sweep gas flow (SGF)
- Membrane size and characteristics
- CO2 gradient
3.8.1. Extracorporeal Blood Flow (ECBF)
3.8.2. Sweep Gas Flow (SGF)
3.8.3. Membrane Characteristics
3.8.4. Transmembrane pCO2 Gradient
3.9. CO2 Removal Rate
3.9.1. Gaseous CO2 Removal
3.9.2. Liquid CO2 Removal
3.10. Potential Clinical Applications
- (1)
- Gattinoni and Kolobow first described the use of ECCO2R in ARDS in the late 1970s [23,24,26], following the affirmation of the “baby lung” concept and the development of lung protective ventilation strategies [46,47]. ECCO2R was suggested as an adjunctive tool that enabled ventilation with low tidal volumes (VT 6–8 mL/Kg PBW) to prevent further lung injury, whilst addressing the hypercapnia resulting from a reduced minute ventilation. However, protective lung ventilation remains feasible in many situations without the use of ECCO2R, particularly when tolerating a moderate degree of hypercapnia (“permissive hypercapnia”). More recently, the role of ECCO2R in ARDS has gained renewed interest [48,49,50], often in parallel with the predicament of ultra-protective lung ventilation (VT 3–4 mL/Kg PBW) [51,52,53]. Such approach does not provide adequate CO2 clearance and an alternative strategy for CO2 removal, e.g., extracorporeal support, becomes necessary.
- (2)
- Another potential application is in acute type 2 respiratory failure, such as acute exacerbations of obstructive airway disease (COPD and severe acute asthma). The postulated role for ECCO2R is to correct the acute element of respiratory acidosis, allowing the avoidance of intubation in patients with COPD exacerbation, or facilitating extubation in those patients already on invasive ventilation [54,55,56,57]. A theoretical benefit has also been suggested in severe acute asthma [58].
3.11. Effects of ECCO2R on Intensity of Mechanical Ventilation
4. Conclusions
Funding
Conflicts of Interest
Abbreviations
| O2 | Oxygen |
| CO2 | Carbon dioxide |
| CaO2 | Arterial O2 content |
| CcO2 | Pulmonary end-capillary O2 content |
| CvmixO2 | Mixed venous O2 content |
| CvO2 | Venous O2 content |
| Cpre-oxyO2 | Pre-oxygenator O2 content |
| Cpost-oxyO2 | Post-oxygenator O2 content |
| Ccapillary-oxyO2 | O2 content of ‘capillary’ blood in the oxygenator |
| Ppre-oxyO2 | Pre-oxygenator O2 partial pressure |
| Ppost-oxyO2 | Post-oxygenator O2 partial pressure |
| PAO2 | Alveolar O2 partial pressure |
| PaCO2 | Arterial CO2 partial pressure |
| Cpre-oxyCO2 | Pre-oxygenator CO2 content |
| Cpost-oxyCO2 | Post-oxygenator CO2 content |
| Ppost-oxyCO2 | Post-oxygenator CO2 partial pressure |
| PCO2ML (exp) | CO2 partial pressure in the membrane effluent gas |
| PCO2ML (pre) | Pre-oxygenator (or pre-membrane) CO2 partial pressure |
| PexpCO2 | CO2 partial pressure in the membrane effluent gas |
| FiO2 | Fraction of inspired O2 |
| FdO2 | Fraction of delivered O2 |
| DO2 | Oxygen delivery |
| CO | Cardiac output |
| Qt | Total cardiac output |
| Qs | Shunt flow |
| Qs/Qt | Shunt fraction |
| Qr | Recirculating blood flow |
| ECBF | Extra corporeal blood flow |
| SGF | Sweep gas flow |
| VO2 | O2 consumption |
| VO2ML | O2 transfer of the membrane lung |
| VCO2 | CO2 production |
| VCO2 TOT | Total CO2 clearance |
| VCO2ML | Amount of CO2 removed by membrane lung |
| VCO2 NL | Amount of CO2 removed by native lung |
| VCO2 (D) | CO2 transfer across the membrane, calculated as per Douglas |
| VCO2 (CORR) | VCO2 corrected for a standard inlet PCO2 of 6 kPa |
| V DSML | Membrane lung dead space |
| ΔP | Predicted difference in driving pressure |
| κ | Correction factor |
| CRS | Static compliance of the respiratory system |
| V Dalv/VT | Alveolar dead space fraction |
| RR | respiratory rate |
| H2O | Water |
| H2CO3 | Carbonic acid |
| H+ | Hydrogen ion |
| HCO3− | Bicarbonate ion |
| Hb | Haemoglobin |
| HbO2 | Oxygenated haemoglobin |
| HbH+ | Reduced haemoglobin |
| P H2O | Partial pressure of water |
| Patm | Atmospheric pressure |
References
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, T.; Vasques, F.; Rapetti, F.; Maiolo, G.; Collino, F.; Romitti, F.; Camporota, L.; Cressoni, M.; Cadringher, P.; Quintel, M.; et al. Driving pressure and mechanical power: New targets for VILI prevention. Ann. Transl. Med. 2017, 5, 286. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5537108/ (accessed on 30 January 2021). [CrossRef] [PubMed] [Green Version]
- Gattinoni, L.; Tonetti, T.; Cressoni, M.; Cadringher, P.; Herrmann, P.; Moerer, O.; Protti, A.; Gotti, M.; Chiurazzi, C.; Carlesso, E.; et al. Ventilator-related causes of lung injury: The mechanical power. Intensiv. Care Med. 2016, 42, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Extracorporeal Life Support Organization—ECMO and ECLS > Registry > Statistics. Available online: https://www.elso.org/Registry/Statistics.aspx (accessed on 6 February 2021).
- Noah, M.A.; Peek, G.J.; Finney, S.J.; Griffiths, M.J.; Harrison, D.A.; Grieve, R.; Sadique, M.Z.; Sekhon, J.S.; McAuley, D.F.; Firmin, R.K.; et al. Referral to an Extracorporeal Membrane Oxygenation Center and Mortality Among Patients with Severe 2009 Influenza A(H1N1). JAMA 2011, 306, 1659–1668. [Google Scholar] [CrossRef] [Green Version]
- Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza Investigators. Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA 2009, 302, 1888–1895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef]
- Patroniti, N.; Zangrillo, A.; Pappalardo, F.; Peris, A.; Cianchi, G.; Braschi, A.; Iotti, G.A.; Arcadipane, A.; Panarello, G.; Ranieri, V.M.; et al. The Italian ECMO network experience during the 2009 influenza A(H1N1) pandemic: Preparation for severe respiratory emergency outbreaks. Intensiv. Care Med. 2011, 37, 1447–1457. [Google Scholar] [CrossRef]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. New Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Tomlinson, G.; Hajage, D.; Wijeysundera, D.N.; Fan, E.; Jüni, P.; Brodie, D.; Slutsky, A.S.; Combes, A. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome and Posterior Probability of Mortality Benefit in a Post Hoc Bayesian Analysis of a Randomized Clinical Trial. JAMA 2018, 320, 2251–2259. [Google Scholar] [CrossRef] [PubMed]
- Munshi, L.; Walkey, A.; Goligher, E.; Pham, T.; Uleryk, E.M.; Fan, E. Venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: A systematic review and meta-analysis. Lancet Respir. Med. 2019, 7, 163–172. [Google Scholar] [CrossRef]
- Conrad, S.A.; Broman, L.M.; Taccone, F.S.; Lorusso, R.; Malfertheiner, M.V.; Pappalardo, F.; Di Nardo, M.; Belliato, M.; Grazioli, L.; Barbaro, R.P.; et al. The Extracorporeal Life Support Organization Maastricht Treaty for Nomenclature in Extracorporeal Life Support. A Position Paper of the Extracorporeal Life Support Organization. Am. J. Respir. Crit. Care Med. 2018, 198, 447–451. [Google Scholar] [CrossRef]
- Riley, R.L.; Cournand, A. ‘Ideal’ Alveolar Air and the Analysis of Ventilation-Perfusion Relationships in the Lungs. J. Appl. Physiol. 1949, 1, 825–847. [Google Scholar] [CrossRef]
- Quintel, M.; Bartlett, R.H.; Grocott, M.P.W.; Combes, A.; Ranieri, M.V.; Baiocchi, M.; Nava, S.; Brodie, D.; Camporota, L.; Vasques, F.; et al. Extracorporeal Membrane Oxygenation for Respiratory Failure. Anesthesiology 2020, 132, 1257–1276. [Google Scholar] [CrossRef] [PubMed]
- West, J.B. Understanding pulmonary gas exchange: Ventilation-perfusion relationships. J. Appl. Physiol. 2004, 97, 1603–1604. [Google Scholar] [CrossRef] [PubMed]
- Cove, E.M.; Federspiel, W.J. Veno-venous extracorporeal CO2 removal for the treatment of severe respiratory acidosis. Crit. Care 2015, 19, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, M.; Costa, E.L.V.; Maciel, A.T.; E Silva, D.P.; Friedrich, N.; Barbosa, E.V.S.; Hirota, A.S.; Schettino, G.; Azevedo, L.C.P. Determinants of Oxygen and Carbon Dioxide Transfer during Extracorporeal Membrane Oxygenation in an Experimental Model of Multiple Organ Dysfunction Syndrome. PLoS ONE 2013, 8, e54954. [Google Scholar] [CrossRef] [PubMed]
- MacLaren, G.; Combes, A.; Bartlett, R.H. Contemporary extracorporeal membrane oxygenation for adult respiratory failure: Life support in the new era. Intensiv. Care Med. 2012, 38, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Pesenti, A.; Patroniti, N.; Fumagalli, R. Carbon dioxide dialysis will save the lung. Crit. Care Med. 2010, 38, S549–S554. [Google Scholar] [CrossRef]
- Terragni, P.P.; Birocco, A.; Faggiano, C.; Ranieri, V.M. Extracorporeal CO2 Removal. Contrib. Nephrol. 2010, 165, 185–196. [Google Scholar] [PubMed]
- Terragni, P.; Maiolo, G.; Ranieri, V.M. Role and potentials of low-flow CO2 removal system in mechanical ventilation. Curr. Opin. Crit. Care 2012, 18, 93–98. [Google Scholar] [CrossRef]
- Gattinoni, L.; Pesenti, A.; Kolobow, T.; Damia, G. A new look at therapy of the adult respiratory distress syndrome: Motionless lungs. Int. Anesthesiol. Clin. 1983, 21, 97–117. [Google Scholar] [CrossRef]
- Gattinoni, L.; Kolobow, T.; Agostoni, A.; Damia, G.; Pelizzola, A.; Rossi, G.P.; Langer, M.; Solca, M.; Citterio, R.; Pesenti, A.; et al. Clinical application of low frequency positive pressure ventilation with extracorporeal CO2 removal (LFPPV-ECCO2R) in treatment of adult respiratory distress syndrome (ARDS). Int. J. Artif. Organs 1979, 2, 282–283. [Google Scholar] [PubMed]
- Gattinoni, L.; Kolobow, T.; Tomlinson, T.; White, D.; Pierce, J. Control of intermittent positive pressure breathing (ippb) by extracorporeal removal of carbon dioxide. Br. J. Anaesth. 1978, 50, 753–758. [Google Scholar] [CrossRef] [Green Version]
- Gattinoni, L.; Kolobow, T.; Damia, G.; Agostoni, A.; Pesenti, A. Extracorporeal carbon dioxide removal (ECCO2R): A new form of respiratory assistance. Int. J. Artif. Organs 1979, 2, 183–185. [Google Scholar] [PubMed]
- Gattinoni, L.; Kolobow, T.; Tomlinson, T.; Iapichino, G.; Samaja, M.; White, D.; Pierce, J. Low-frequency positive pressure ventilation with extracorporeal carbon dioxide removal (LFPPV-ECCO2R): An experimental study. Anesth Analg. 1978, 57, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, R.H. Physiology of Gas Exchange During ECMO for Respiratory Failure. J. Intensiv. Care Med. 2016, 32, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Vasques, F.; Romitti, F.; Gattinoni, L.; Camporota, L. How I wean patients from veno-venous extra-corporeal membrane oxygenation. Crit. Care 2019, 23, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Boyle, A.J.; Sklar, M.C.; McNamee, J.J.; Brodie, D.; Slutsky, A.S.; Brochard, L.; McAuley, D.F.; Abrams, D.; Combes, A.; Fan, E.; et al. Extracorporeal carbon dioxide removal for lowering the risk of mechanical ventilation: Research questions and clinical potential for the future. Lancet Respir. Med. 2018, 6, 874–884. [Google Scholar] [CrossRef] [Green Version]
- May, A.G.; Omecinski, K.S.; Frankowski, B.J.; Federspiel, W.J. Effect of Hematocrit on the CO2 Removal Rate of Artificial Lungs. ASAIO J. 2020, 66, 1161–1165. [Google Scholar] [CrossRef]
- Kolobow, T.; Gattinoni, L.; Tomlinson, T.; Pierce, J.E. An alternative to breathing. J. Thorac. Cardiovasc. Surg. 1978, 75, 261–266. [Google Scholar] [CrossRef]
- Duscio, E.; Cipulli, F.; Vasques, F.; Collino, F.; Rapetti, F.; Romitti, F.; Quintel, M.; Vassalli, F.; Gattinoni, L.; Tonetti, T.; et al. Extracorporeal CO2 Removal: The Minimally Invasive Approach, Theory, and Practice. Crit. Care Med. 2019, 47, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Strassmann, S.; Brodie, D.; Ritter, P.; Larsson, A.; Borchardt, R.; Windisch, W. Impact of membrane lung surface area and blood flow on extracorporeal CO2 removal during severe respiratory acidosis. Intensiv. Care Med. Exp. 2017, 5, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrett, A.N.; Hart, N.; Camporota, L. In vivo carbon dioxide clearance of a low-flow extracorporeal carbon dioxide removal circuit in patients with acute exacerbations of chronic obstructive pulmonary disease. Perfusion 2020, 35, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Godet, T.; Combes, A.; Zogheib, E.; Jabaudon, M.; Futier, E.; Slutsky, A.S.; Constantin, J.-M. Novel CO2 removal device driven by a renal-replacement system without hemofilter. A first step experimental validation. Anaesth. Crit. Care Pain Med. 2015, 34, 135–140. [Google Scholar] [CrossRef]
- Turani, F.; Martini, S.; Marinelli, A.; Falco, M.; Barchetta, R.; Candidi, F.; Gargano, F. ECCO2 removal with a phosphorylcholine-coated membrane oxygenator in difficult respiratory weaning patients. Crit. Care 2013, 17, 129. [Google Scholar] [CrossRef] [Green Version]
- Zanella, A.; Mangili, P.; Giani, M.; Redaelli, S.; Scaravilli, V.; Castagna, L.; Sosio, S.; Pirrone, F.; Albertini, M.; Patroniti, N.; et al. Extracorporeal carbon dioxide removal through ventilation of acidified dialysate: An experimental study. J. Heart Lung Transplant. 2014, 33, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Arazawa, D.T.; Oh, H.-I.; Ye, S.-H.; Johnson, C.A.; Woolley, J.R.; Wagner, W.R.; Federspiel, W.J. Immobilized carbonic anhydrase on hollow fiber membranes accelerates CO2 removal from blood. J. Membr. Sci. 2012, 403–404, 25–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimmel, J.D.; Arazawa, D.T.; Ye, S.-H.; Shankarraman, V.; Wagner, W.R.; Federspiel, W.J. Carbonic anhydrase immobilized on hollow fiber membranes using glutaraldehyde activated chitosan for artificial lung applications. J. Mater. Sci. Mater. Med. 2013, 24, 2611–2621. [Google Scholar] [CrossRef]
- Arthurs, G.; Sudhakar, M. Carbon dioxide transport. Contin. Educ. Anaesth. Crit. Care Pain 2005, 5, 207–210. [Google Scholar] [CrossRef] [Green Version]
- Jeffries, R.G.; Lund, L.; Frankowski, B.; Federspiel, W.J. An extracorporeal carbon dioxide removal (ECCO2R) device operating at hemodialysis blood flow rates. Intensiv. Care Med. Exp. 2017, 5, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arazawa, D.T.; Kimmel, J.D.; Finn, M.; Federspiel, W.J. Acidic sweep gas with carbonic anhydrase coated hollow fiber membranes synergistically accelerates CO2 removal from blood. Acta Biomater. 2015, 25, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanella, A.; Castagna, L.; Salerno, D.; Scaravilli, V.; Abd El Aziz El Sayed Deab, S.; Magni, F.; Gianni, M.; Mazzola, S.; Mantegazza, F.; Albertini, M.; et al. Respiratory Electrodialysis. A Novel, Highly Efficient Extracorporeal CO2 Removal Technique. Am. J. Respir. Crit. Care Med. 2015, 192, 719–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- May, A.G.; Sen, A.; Cove, M.E.; Kellum, J.A.; Federspiel, W.J. Extracorporeal CO2 removal by hemodialysis: In vitro model and feasibility. Intensiv. Care Med. Exp. 2017, 5, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recommendations|Extracorporeal Carbon Dioxide Removal for Acute Respiratory Failure|Guidance|NICE. NICE. Available online: https://www.nice.org.uk/guidance/ipg564/chapter/1-recommendations (accessed on 11 February 2021).
- Gattinoni, L.; Pesenti, A.; Rossi, G.; Vesconi, S.; Fox, U.; Kolobow, T.; Agostoni, A.; Pelizzola, A.; Langer, M.; Uziel, L.; et al. Treatment of acute respiratory failure with low frequency positive-pressure ventilation and extracorporeal removal of CO2. Lancet 1980, 316, 292–294. [Google Scholar] [CrossRef]
- Gattinoni, L.; Pesenti, A. The concept of “baby lung”. Intensive Care Med. 2005, 31, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Taccone, F.S.; Malfertheiner, M.V.; Ferrari, F.; Di Nardo, M.; Swol, J.; Broman, L.M.; Vercaemst, L.; Barrett, N.; Pappalardo, F.; Belohlavek, J.; et al. Extracorporeal CO2 removal (ECCO2R) in critically ill patients: A systematic review. Minerva Anestesiol 2017, 83, 762–772. [Google Scholar] [PubMed]
- Romay, E.; Ferrer, R. Extracorporeal CO2 removal: Technical and physiological fundaments and principal indications. Med. Intensiv. 2016, 40, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Camporota, L.; Barrett, N. Current Applications for the Use of Extracorporeal Carbon Dioxide Removal in Critically Ill Patients. BioMed Res. Int. 2016, 2016, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terragni, P.P.; Terragni, P.P.; Del Sorbo, L.; Mascia, L.; Urbino, R.; Martin, E.L.; Birocco, A.; Faggiano, C.; Quintel, M.; Gattinoni, L.; et al. Tidal volume lower than 6 ml/kg enhances lung protection: Role of extracorporeal carbon dioxide removal. Anesthesiology 2009, 111, 826–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bein, T.; Weber-Carstens, S.; Goldmann, A.; Müller, T.; Staudinger, T.; Brederlau, J.; Muellenbach, R.; Dembinski, R.; Graf, B.M.; Wewalka, M.; et al. Lower tidal volume strategy (≈3 mL/kg) combined with extracorporeal CO2 removal versus ‘conventional’ protective ventilation (6 mL/kg) in severe ARDS. Intensiv. Care Med. 2013, 39, 847–856. [Google Scholar] [CrossRef] [Green Version]
- Fanelli, V.; Ranieri, M.V.; Mancebo, J.; Moerer, O.; Quintel, M.; Morley, S.; Moran, I.; Parrilla, F.; Costamagna, A.; Gaudiosi, M.; et al. Feasibility and safety of low-flow extracorporeal carbon dioxide removal to facilitate ultra-protective ventilation in patients with moderate acute respiratory distress syndrome. Crit. Care 2016, 20, 36. [Google Scholar] [CrossRef] [Green Version]
- Del Sorbo, L.; Pisani, L.; Filippini, C.; Fanelli, V.; Fasano, L.; Terragni, P.; Dell’Amore, A.; Urbino, R.; Mascia, L.; Evangelista, A.; et al. Extracorporeal Co2 Removal in Hypercapnic Patients at Risk of Noninvasive Ventilation Failure: A Matched Cohort Study with Historical Control*. Crit. Care Med. 2015, 43, 120–127. [Google Scholar] [CrossRef]
- Kluge, S.; Braune, S.A.; Engel, M.; Nierhaus, A.; Frings, D.; Ebelt, H.; Uhrig, A.; Metschke, M.; Wegscheider, K.; Suttorp, N.; et al. Avoiding invasive mechanical ventilation by extracorporeal carbon dioxide removal in patients failing noninvasive ventilation. Intensiv. Care Med. 2012, 38, 1632–1639. [Google Scholar] [CrossRef] [PubMed]
- Pettenuzzo, T.; Fan, Y.; Del Sorbo, L. Extracorporeal carbon dioxide removal in acute exacerbations of chronic obstructive pulmonary disease. Ann. Transl. Med. 2018, 6, 31. [Google Scholar] [CrossRef] [PubMed]
- Morales-Quinteros, L.; Del Sorbo, L.; Artigas, A. Extracorporeal carbon dioxide removal for acute hypercapnic respiratory failure. Ann. Intensiv. Care 2019, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Schneider, T.-M.; Bence, T.; Brettner, F. “Awake” ECCO2R superseded intubation in a near-fatal asthma attack. J. Intensive Care 2017, 5, 53. [Google Scholar] [CrossRef] [Green Version]
- Goligher, E.C.; For the SUPERNOVA investigators (European Society of Intensive Care Medicine trials group) and for the International ECMO Network (ECMONet); Combes, A.; Brodie, D.; Ferguson, N.D.; Pesenti, A.M.; Ranieri, V.M.; Slutsky, A.S. Determinants of the effect of extracorporeal carbon dioxide removal in the SUPERNOVA trial: Implications for trial design. Intensiv. Care Med. 2019, 45, 1219–1230. [Google Scholar] [CrossRef] [PubMed]
- Combes, A.; Fanelli, V.; Pham, T.; Ranieri, V.M.; European Society of Intensive Care Medicine Trials Group and the “Strategy of Ultra-Protective lung ventilation with Extracorporeal CO2 Removal for New-Onset moderate to severe ARDS” (SUPERNOVA) investigators. Feasibility and safety of extracorporeal CO2 removal to enhance protective ventilation in acute respiratory distress syndrome: The SUPERNOVA study. Intensive Care Med. 2019, 45, 592–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ficial, B.; Vasques, F.; Zhang, J.; Whebell, S.; Slattery, M.; Lamas, T.; Daly, K.; Agnew, N.; Camporota, L. Physiological Basis of Extracorporeal Membrane Oxygenation and Extracorporeal Carbon Dioxide Removal in Respiratory Failure. Membranes 2021, 11, 225. https://doi.org/10.3390/membranes11030225
Ficial B, Vasques F, Zhang J, Whebell S, Slattery M, Lamas T, Daly K, Agnew N, Camporota L. Physiological Basis of Extracorporeal Membrane Oxygenation and Extracorporeal Carbon Dioxide Removal in Respiratory Failure. Membranes. 2021; 11(3):225. https://doi.org/10.3390/membranes11030225
Chicago/Turabian StyleFicial, Barbara, Francesco Vasques, Joe Zhang, Stephen Whebell, Michael Slattery, Tomas Lamas, Kathleen Daly, Nicola Agnew, and Luigi Camporota. 2021. "Physiological Basis of Extracorporeal Membrane Oxygenation and Extracorporeal Carbon Dioxide Removal in Respiratory Failure" Membranes 11, no. 3: 225. https://doi.org/10.3390/membranes11030225