


Worldwide Child Routine Vaccination Hesitancy Rate among Parents of Children Aged 0–6 Years: A Systematic Review and Meta-Analysis of Cross-Sectional Studies

Abstract
:1. Introduction
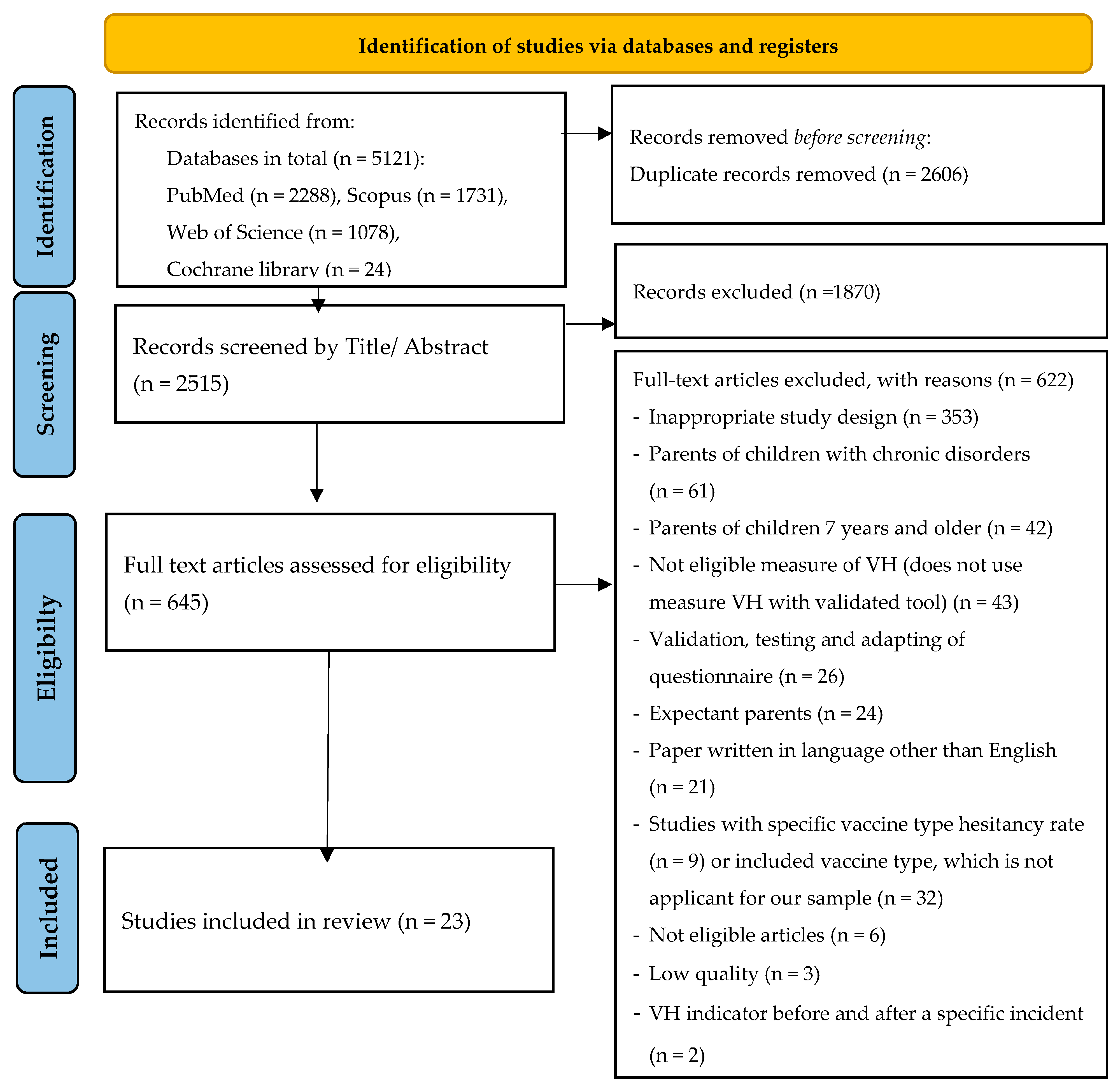
2. Materials and Methods
2.1. Search Strategies
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analyses
3. Results
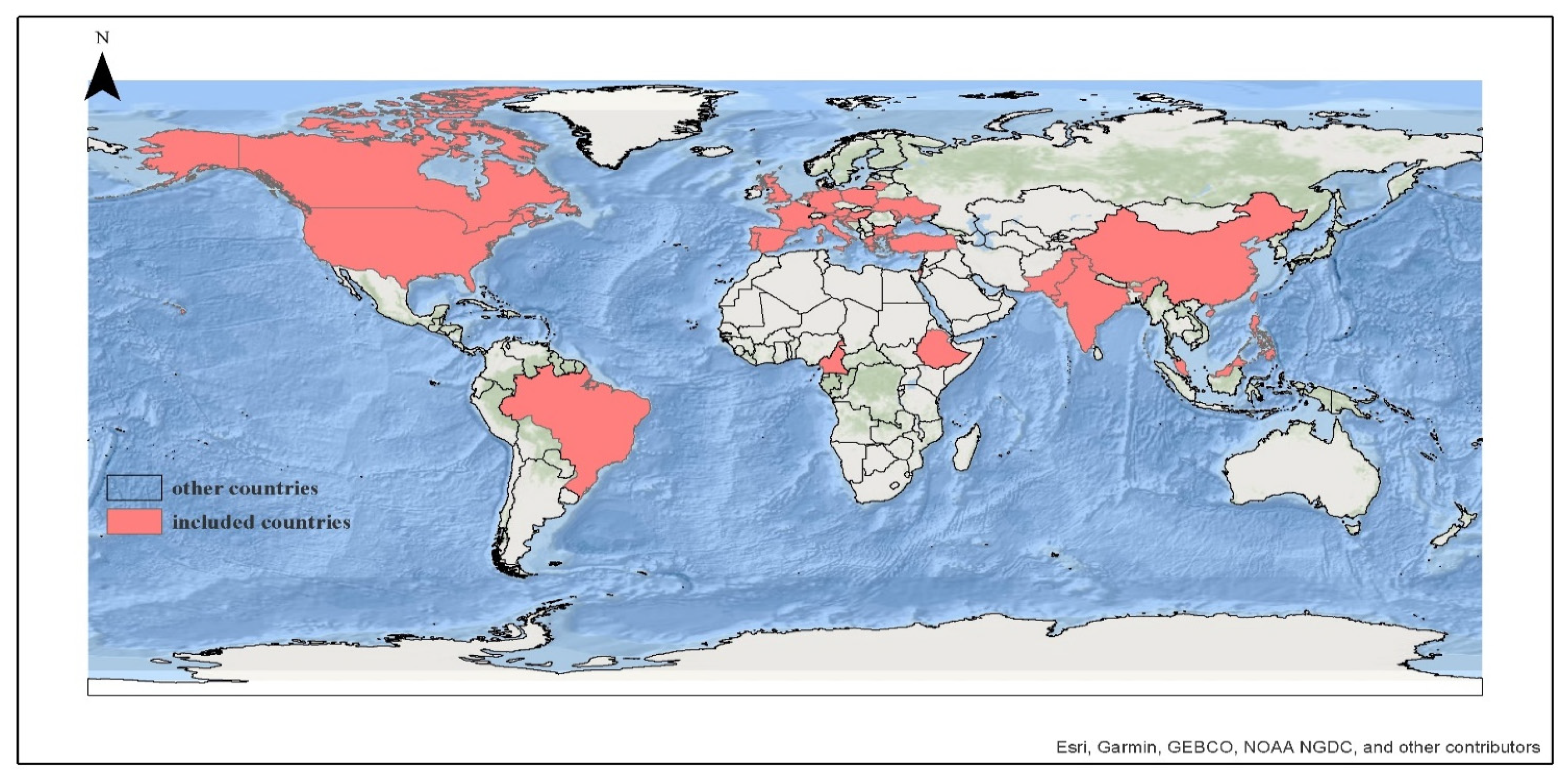
3.1. Overview of Included Studies
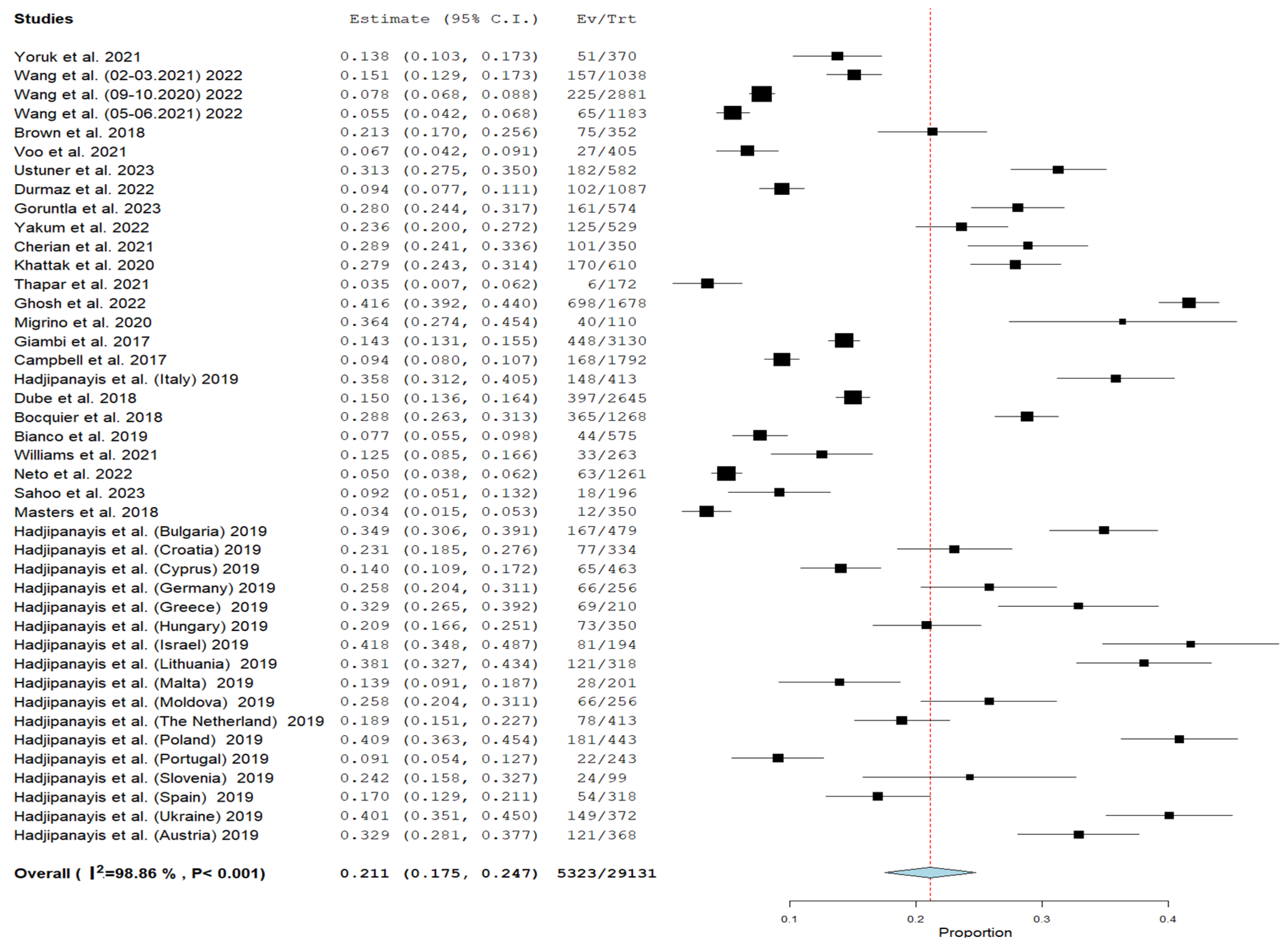
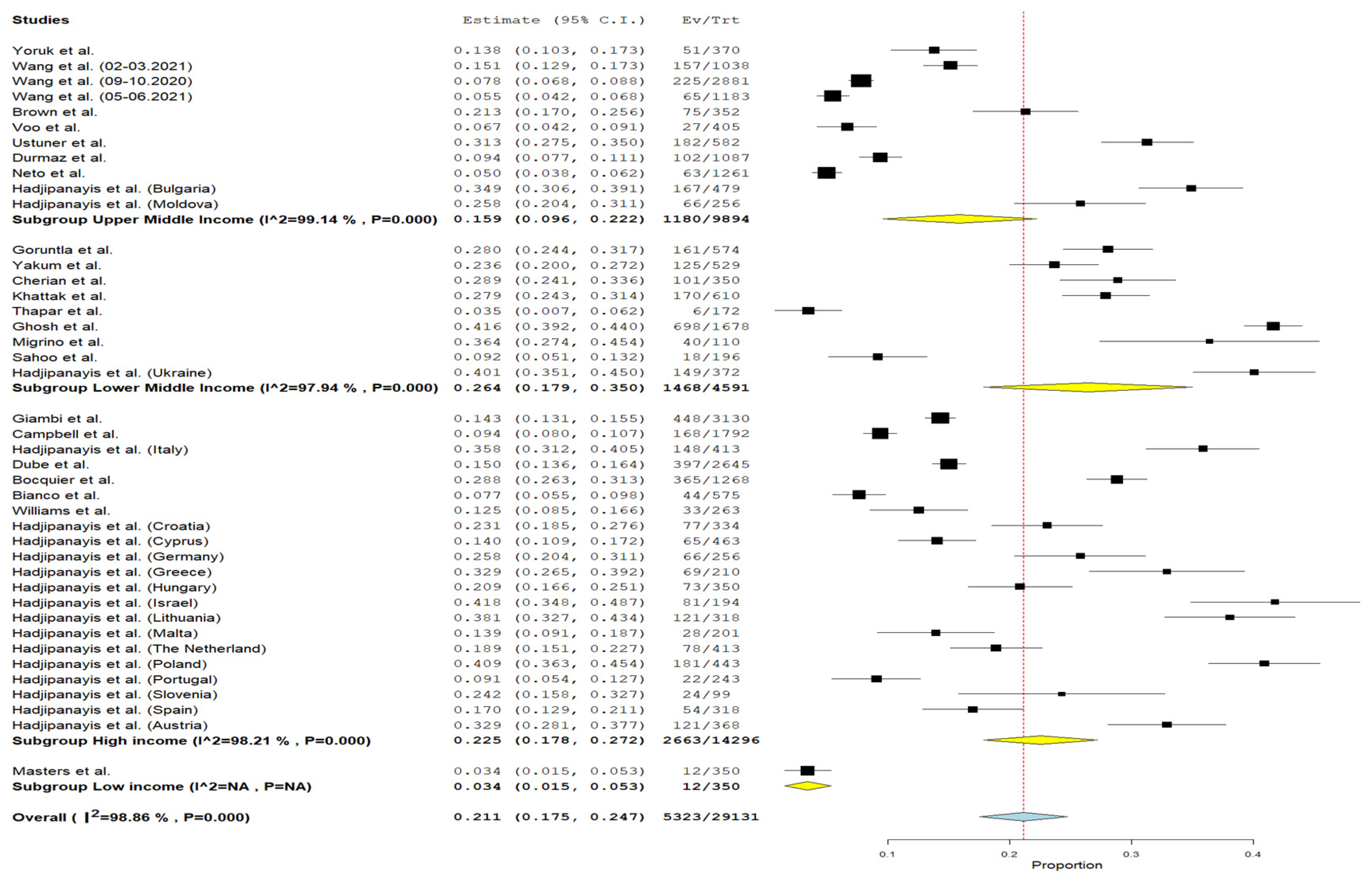
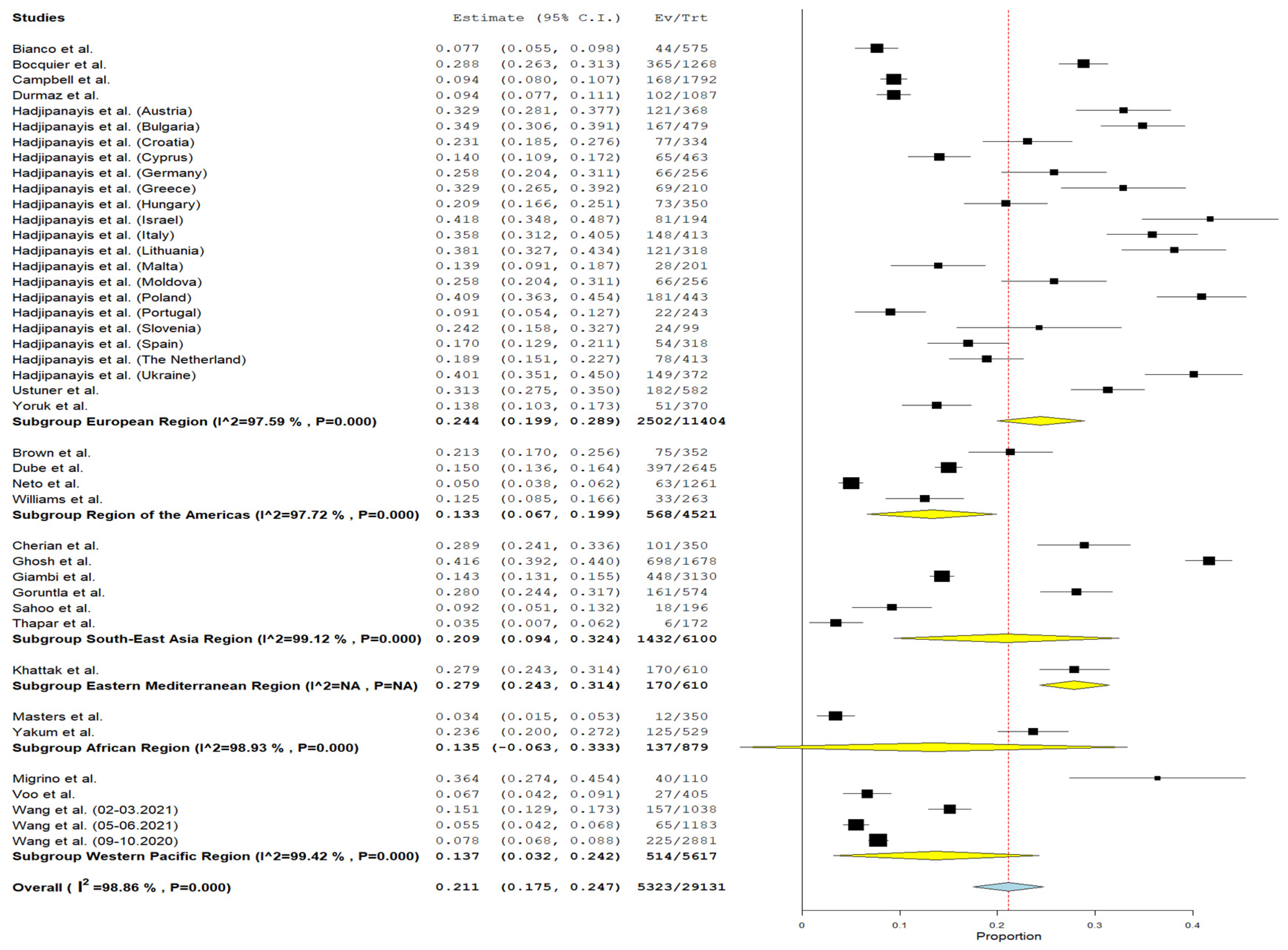
3.2. Cumulative Prevalence
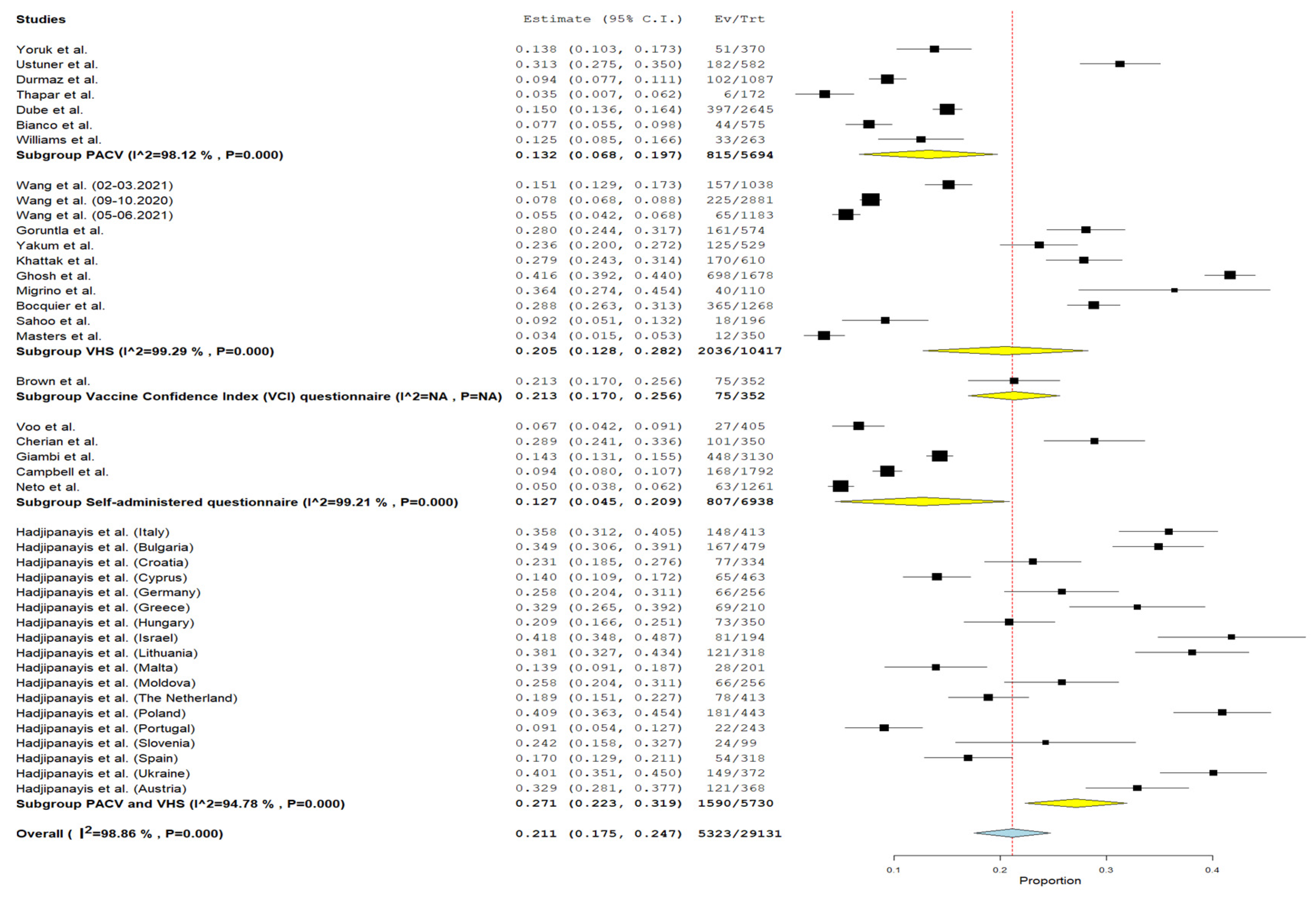
3.3. Subgroup Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olusanya, O.A.; Bednarczyk, R.A.; Davis, R.L.; Shaban-Nejad, A. Addressing Parental Vaccine Hesitancy and Other Barriers to Childhood/Adolescent Vaccination Uptake During the Coronavirus (COVID-19) Pandemic. Front. Immunol. 2021, 12, 663074. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Wang, L.; Burgner, D.P.; Miller, J.E.; Song, Y.; Ren, X.; Li, Z.; Xing, Y.; Ma, J.; Sawyer, S.M.; et al. Infectious Diseases in Children and Adolescents in China: Analysis of National Surveillance Data from 2008 to 2017. BMJ 2020, 369, m1043. [Google Scholar] [CrossRef] [PubMed]
- Porter, A.; Goldfarb, J. Measles: A Dangerous Vaccine-Preventable Disease Returns. Cleve. Clin. J. Med. 2019, 86, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Siani, A. Measles Outbreaks in Italy: A Paradigm of the Re-Emergence of Vaccine-Preventable Diseases in Developed Countries. Prev. Med. 2019, 121, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Measles. Available online: https://www.who.int/news-room/fact-sheets/detail/measles (accessed on 16 October 2023).
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Охват Иммунизацией [Immunization Coverage]. Available online: https://www.who.int/ru/news-room/fact-sheets/detail/immunization-coverage (accessed on 16 June 2022).
- Vaccines and Immunization: What Is Vaccination? Available online: https://www.who.int/news-room/questions-and-answers/item/vaccines-and-immunization-what-is-vaccination (accessed on 11 October 2023).
- Sadaf, A.; Richards, J.L.; Glanz, J.; Salmon, D.A.; Omer, S.B. A Systematic Review of Interventions for Reducing Parental Vaccine Refusal and Vaccine Hesitancy. Vaccine 2013, 31, 4293–4304. [Google Scholar] [CrossRef]
- Immunization, Vaccines and Biologicals. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/policies/who-recommendations-for-routine-immunization---summary-tables (accessed on 11 October 2023).
- Chan, P.S.-F.; Fang, Y.; Kawuki, J.; Chen, S.; Liang, X.; Mo, P.K.-H.; Wang, Z. Parental Acceptance, Parental Hesitancy, and Uptake of Seasonal Influenza Vaccination among Children Aged 6-59 Months: A Systematic Review and Meta-Analysis. Vaccines 2023, 11, 1360. [Google Scholar] [CrossRef]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine Hesitancy around the Globe: Analysis of Three Years of WHO/UNICEF Joint Reporting Form Data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef]
- de Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping Global Trends in Vaccine Confidence and Investigating Barriers to Vaccine Uptake: A Large-Scale Retrospective Temporal Modelling Study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Opel, D.J.; Mangione-Smith, R.; Taylor, J.A.; Korfiatis, C.; Wiese, C.; Catz, S.; Martin, D.P. Development of a Survey to Identify Vaccine-Hesitant Parents: The Parent Attitudes about Childhood Vaccines Survey. Hum. Vaccin. 2011, 7, 419–425. [Google Scholar] [CrossRef]
- Wagner, A.L.; Masters, N.B.; Domek, G.J.; Mathew, J.L.; Sun, X.; Asturias, E.J.; Ren, J.; Huang, Z.; Contreras-Roldan, I.L.; Gebremeskel, B.; et al. Comparisons of Vaccine Hesitancy across Five Low- and Middle-Income Countries. Vaccines 2019, 7, 155. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, T.S.; Reddy, N.S.; Apte, A.; Sinha, B.; Roy, S.; Nair, N.P.; Sindhu, K.N.; Patil, R.; Upadhyay, R.P.; Chowdhury, R. Delayed Vaccination and Its Predictors among Children under 2 Years in India: Insights from the National Family Health Survey-4. Vaccine 2019, 37, 2331–2339. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Wagner, A.L.; Zheng, A.; Sun, X.; Boulton, M.L.; Huang, Z.; Zikmund-Fisher, B.J. The Demographics of Vaccine Hesitancy in Shanghai, China. PLoS ONE 2018, 13, e0209117. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Gagnon, D.; Nickels, E.; Jeram, S.; Schuster, M. Mapping Vaccine Hesitancy—Country-Specific Characteristics of a Global Phenomenon. Vaccine 2014, 32, 6649. [Google Scholar] [CrossRef] [PubMed]
- Jafflin, K.; Deml, M.J.; Schwendener, C.L.; Kiener, L.; Delfino, A.; Gafner, R.; Schudel, S.; Mäusezahl, M.; Berger, C.; Huber, B.M.; et al. Parental and Provider Vaccine Hesitancy and Non-Timely Childhood Vaccination in Switzerland. Vaccine 2022, 40, 3193–3202. [Google Scholar] [CrossRef] [PubMed]
- Phadke, V.K.; Bednarczyk, R.A.; Salmon, D.A.; Omer, S.B. Association Between Vaccine Refusal and Vaccine-Preventable Diseases in the United States: A Review of Measles and Pertussis. JAMA 2016, 315, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Vivion, M.; MacDonald, N.E. Vaccine Hesitancy, Vaccine Refusal and the Anti-Vaccine Movement: Influence, Impact and Implications. Expert Rev. Vaccines 2015, 14, 99–117. [Google Scholar] [CrossRef]
- PRISMA. Available online: http://www.prisma-statement.org/?AspxAutoDetectCookieSupport=1 (accessed on 11 October 2023).
- Rayyan—AI Powered Tool for Systematic Literature Reviews. Available online: https://www.rayyan.ai/ (accessed on 1 December 2023).
- JBI Critical Appraisal Tools. JBI. Available online: https://jbi.global/critical-appraisal-tools (accessed on 11 October 2023).
- OpenMeta [Analyst]—CEBM @ Brown. Available online: http://www.cebm.brown.edu/openmeta/ (accessed on 11 October 2023).
- ArcMap Resources for ArcGIS Desktop. Documentation, Tutorials & More. Available online: https://www.esri.com/en-us/arcgis/products/arcgis-desktop/resources (accessed on 11 October 2023).
- New World Bank Country Classifications by Income Level: 2022–2023. Available online: https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2022-2023 (accessed on 11 October 2023).
- Countries. World Health Organization. Available online: https://www.who.int/countries (accessed on 11 October 2023).
- Bianco, A.; Mascaro, V.; Zucco, R.; Pavia, M. Parent Perspectives on Childhood Vaccination: How to Deal with Vaccine Hesitancy and Refusal? Vaccine 2019, 37, 984–990. [Google Scholar] [CrossRef]
- Sahoo, S.S.; Parida, S.P.; Singh, A.K.; Palepu, S.; Sahoo, D.P.; Bhatia, V. Decision-Making in Childhood Vaccination: Vaccine Hesitancy among Caregivers of under-5 Children from a Tertiary Care Institution in Eastern India. Ther. Adv. Vaccines Immunother. 2023, 11, 25151355231152650. [Google Scholar] [CrossRef]
- Kumar, N.; Thapar, R.; Surendran, P.; Shahdiya, A.; Mahendran, V.; Ramesh, R.; Shetty, D.J.; Unnikrishnan, B.; Mithra, P.; Holla, R.; et al. Vaccine Hesitancy among Mothers of Under-Five Children in Coastal South India: A Facility-Based Cross-Sectional Study. F1000Research 2021, 10, 186. [Google Scholar] [CrossRef]
- Williams, J.T.B.; Rice, J.D.; Lou, Y.; Bayliss, E.A.; Federico, S.G.; Hambidge, S.J.; O’Leary, S.T. Parental Vaccine Hesitancy and Vaccination Disparities in a Safety-Net System. Pediatrics 2021, 147, 2020010710. [Google Scholar] [CrossRef]
- Dubé, È.; Farrands, A.; Lemaitre, T.; Boulianne, N.; Sauvageau, C.; Boucher, F.D.; Tapiero, B.; Quach, C.; Ouakki, M.; Gosselin, V.; et al. Overview of Knowledge, Attitudes, Beliefs, Vaccine Hesitancy and Vaccine Acceptance among Mothers of Infants in Quebec, Canada. Hum. Vaccin. Immunother. 2019, 15, 113. [Google Scholar] [CrossRef] [PubMed]
- Ustuner Top, F.; Çevik, C.; Bora Güneş, N. The Relation between Digital Literacy, Cyberchondria, and Parents’ Attitudes to Childhood Vaccines. J. Pediatr. Nurs. Nurs. Care Child. Fam. 2023, 70, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Yörük, S.; Güler, D. Factors Associated with Pediatric Vaccine Hesitancy of Parents: A Cross-Sectional Study in Turkey. Hum. Vaccin. Immunother. 2021, 17, 4505. [Google Scholar] [CrossRef] [PubMed]
- Durmaz, N.; Suman, M.; Ersoy, M.; Örün, E. Parents’ Attitudes toward Childhood Vaccines and COVID-19 Vaccines in a Turkish Pediatric Outpatient Population. Vaccines 2022, 10, 1958. [Google Scholar] [CrossRef] [PubMed]
- Khattak, F.A.; Rehman, K.; Shahzad, M.; Arif, N.; Ullah, N.; Kibria, Z.; Arshad, M.; Afaq, S.; Ibrahimzai, A.K.; Haq, Z.U. Prevalence of Parental Refusal Rate and Its Associated Factors in Routine Immunization by Using WHO Vaccine Hesitancy Tool: A Cross Sectional Study at District Bannu, KP, Pakistan. Int. J. Infect. Dis. 2021, 104, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Goruntla, N.; Akanksha, K.; Lalithaasudhaa, K.; Pinnu, V.; Jinka, D.; Bhupalam, P.; Doniparthi, J. Prevalence and Predictors of Vaccine Hesitancy among Mothers of Under-Five Children: A Hospital-Based Cross-Sectional Study. J. Educ. Health Promot. 2023, 12, 34. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.; Annigeri, S.; Kumar Hemram, S.; Kumar Dey, P.; Mazumder, S.; Ghosh, P. Demography and Determinants of Incomplete Immunization in Children Aged 1–5 Years and Vaccine-Hesitancy among Caregivers: An Eastern Indian Perspective. Clin. Epidemiol. Glob. Health 2022, 17, 101155. [Google Scholar] [CrossRef]
- Yakum, M.N.; Funwie, A.D.; Ajong, A.B.; Tsafack, M.; Ze, L.E.E.; Shah, Z. The Burden of Vaccine Hesitancy for Routine Immunization in Yaounde-Cameroon: A Cross-Sectional Study. PLoS Glob. Public Health 2022, 2, e0001012. [Google Scholar] [CrossRef]
- Masters, N.B.; Tefera, Y.A.; Wagner, A.L.; Boulton, M.L. Vaccine Hesitancy among Caregivers and Association with Childhood Vaccination Timeliness in Addis Ababa, Ethiopia. Hum. Vaccines Immunother. 2018, 14, 2340–2347. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, S.; Fang, Y. Parental Willingness and Associated Factors of Pediatric Vaccination in the Era of COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1453. [Google Scholar] [CrossRef] [PubMed]
- Bocquier, A.; Fressard, L.; Cortaredona, S.; Zaytseva, A.; Ward, J.; Gautier, A.; Peretti-Watel, P.; Verger, P. Social Differentiation of Vaccine Hesitancy among French Parents and the Mediating Role of Trust and Commitment to Health: A Nationwide Cross-Sectional Study. Vaccine 2018, 36, 7666–7673. [Google Scholar] [CrossRef] [PubMed]
- Migriño, J.; Gayados, B.; Birol, K.R.J.; De Jesus, L.; Lopez, C.W.; Mercado, W.C.; Tolosa, J.M.C.; Torreda, J.; Tulagan, G. Factors Affecting Vaccine Hesitancy among Families with Children 2 Years Old and Younger in Two Urban Communities in Manila, Philippines. West. Pacific Surveill. Response J. WPSAR 2020, 11, 20. [Google Scholar] [CrossRef] [PubMed]
- Hadjipanayis, A.; van Esso, D.; del Torso, S.; Dornbusch, H.J.; Michailidou, K.; Minicuci, N.; Pancheva, R.; Mujkic, A.; Geitmann, K.; Syridou, G.; et al. Vaccine Confidence among Parents: Large Scale Study in Eighteen European Countries. Vaccine 2020, 38, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Neto, J.O.; Olbrich, S.R.L.R. Attitudes, Hesitancy, Concerns, and Inconsistencies Regarding Vaccines Reported by Parents of Preschool Children. Rev. Paul. Pediatr. 2023, 41, e2022009. [Google Scholar] [CrossRef] [PubMed]
- Campbell, H.; Edwards, A.; Letley, L.; Bedford, H.; Ramsay, M.; Yarwood, J. Changing Attitudes to Childhood Immunisation in English Parents. Vaccine 2017, 35, 2979–2985. [Google Scholar] [CrossRef] [PubMed]
- Cherian, V.; Saini, N.K.; Sharma, A.K.; Philip, J. Prevalence and Predictors of Vaccine Hesitancy in an Urbanized Agglomeration of New Delhi, India. J. Public Health 2022, 44, 70–76. [Google Scholar] [CrossRef]
- Giambi, C.; Fabiani, M.; D’Ancona, F.; Ferrara, L.; Fiacchini, D.; Gallo, T.; Martinelli, D.; Pascucci, M.G.; Prato, R.; Filia, A.; et al. Parental Vaccine Hesitancy in Italy—Results from a National Survey. Vaccine 2018, 36, 779–787. [Google Scholar] [CrossRef]
- Voo, J.Y.H.; Lean, Q.Y.; Ming, L.C.; Hanafiah, N.H.M.; Al-Worafi, Y.M.; Ibrahim, B. Vaccine Knowledge, Awareness and Hesitancy: A Cross Sectional Survey among Parents Residing at Sandakan District, Sabah. Vaccines 2021, 9, 1348. [Google Scholar] [CrossRef]
- Brown, A.L.; Sperandio, M.; Turssi, C.P.; Leite, R.M.A.; Berton, V.F.; Succi, R.M.; Larson, H.; Napimoga, M.H. Vaccine Confidence and Hesitancy in Brazil. Cad. Saude Publica 2018, 34, e00011618. [Google Scholar] [CrossRef]
- Wang, Q.; Xiu, S.; Yang, L.; Han, Y.; Cui, T.; Shi, N.; Liu, M.; Yi, Y.; Liu, C.; Wang, X.; et al. Changes in Parental Attitudes Toward COVID-19 Vaccination and Routine Childhood Vaccination During the COVID-19 Pandemic: Repeated Cross-Sectional Survey Study. JMIR Public Health Surveill. 2022, 8, e33235. [Google Scholar] [CrossRef] [PubMed]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 Vaccine Acceptance and Hesitancy in Low- and Middle-Income Countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Moradpour, J.; Shajarizadeh, A.; Carter, J.; Chit, A.; Grootendorst, P. The Impact of National Income and Vaccine Hesitancy on Country-Level COVID-19 Vaccine Uptake. PLoS ONE 2023, 18, e0293184. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, P.; Bhattacherjee, S.; Mukherjee, A.; Dasgupta, S. Vaccine Hesitancy for Childhood Vaccinations in Slum Areas of Siliguri, India. Indian J. Public Health 2018, 62, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Obohwemu, K.; Christie-De Jong, F.; Ling, J. Parental Childhood Vaccine Hesitancy and Predicting Uptake of Vaccinations: A Systematic Review. Prim. Health Care Res. Dev. 2022, 23, e68. [Google Scholar] [CrossRef]
- Dyda, A.; King, C.; Dey, A.; Leask, J.; Dunn, A.G. A Systematic Review of Studies That Measure Parental Vaccine Attitudes and Beliefs in Childhood Vaccination. BMC Public Health 2020, 20, 1253. [Google Scholar] [CrossRef]
- Kaufman, J.; Ryan, R.; Walsh, L.; Horey, D.; Leask, J.; Robinson, P.; Hill, S. Face-to-Face Interventions for Informing or Educating Parents about Early Childhood Vaccination. Cochrane Database Syst. Rev. 2018, 5. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; et al. Strategies for Addressing Vaccine Hesitancy—A Systematic Review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1. Validation, testing, or adaptation of questionnaires |
| 2. Studies involving expectant parents’ vaccine hesitancy |
| 3. Research designs other than cross-sectional, including retrospective, qualitative, pretest–posttest, systematic reviews, meta-analyses, randomized controlled trials, cohort studies, and case–control studies |
| 4. Studies assessing the VH indicator before and after a specific incident |
| 5. Studies lacking a general vaccine hesitancy (VH) indicator |
| 6. Studies that assessed VH for only one type of vaccine |
| 7. Studies in which it was impossible to calculate the absolute value of the indicator for the sample |
| 8. Studies that examined hesitancy in the entire population regarding vaccination in general (except when focused on parents) | |
| 9. Studies involving parents of children with chronic disorders | |
| 10. Studies that examined hesitancy regarding immunization programs with specific characteristics (mumps, seasonal influenza, and varicella) | |
| 11. Studies involving parents of children aged 7 years and older | |
| 12. Studies that examined vaccine hesitancy for high-risk populations (typhoid, hepatitis A, dengue, etc.) | |
| 13. Studies for populations of specific regions (Japanese encephalitis, yellow fever, tick-borne encephalitis), as well as for HPV and COVID-19 vaccines. |
| Number | Reference | Country | WHO Region | Income Level | Study Period | Type of Study | Sample Size | Population | Data Collection Tool | Hesitancy, n (%) | Refusal/Delay, n (%) | Quality (JBI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Bianco et al. (2019) [29] | Italy | European Region | High income | From April to June 2017 | Cross-sectional study | 575 parents | Parents having at least one child aged 1–5 years | Parent Attitudes about Childhood Vaccines (PACV) scale | 44 (7.7%) | 141 (24.6%) | High (7) |
| 2 | Sahoo et al. (2023) [30] | India | South-East Asia Region | Lower middle income | From March to May 2019 | Cross-sectional study | 196 caregivers | Сaregivers of children aged 6 months to below 5 years | WHO SAGE 10-item Vaccine Hesitancy Scale for assessing parental attitude towards childhood vaccines (PACV); a scale for measuring “belief toward vaccines” | 18 (9.18%); 6 months to 1 year—10 (16.9%); 1–2 years—5 (6.2%); 2–5 years—3 (5.4%) | N/A | High (9) |
| 3 | Williams et al. (2021) [32] | USA | Region of the Americas | High income | August 2019 through February 2020 | Cross-sectional study | 263 parents | English- and Spanish-speaking parents of children aged 2 years | Parent Attitudes about Childhood Vaccines (PACV) scale | 33 (13%); 4 (4%) Spanish-speaking parents were hesitant versus 29 (19%) English-speaking parents | N/A | High (7) |
| 4 | E. Dubé et al. (2019) [33] | Canada | Region of the Americas | High income | During the period of March 2014 to February 2015 | Cross-sectional study | 2645 mothers of newborns | Mothers of newborns (2 months of age) | Parent Attitudes about Childhood Vaccines (PACV) scale | 1492 (56.4%) ((397 (15.0%) mothers had a score of 50 and higher (high level of VH)) | N/A | High (7) |
| 5 | F. Ustuner Top et al. (2023) [34] | Turkey | European Region | Upper middle income | Implemented online between July 2021 and October 2021 | Cross-sectional study | 582 parents | Parents with children aged 3–5 years old | Parent Attitudes about Childhood Vaccines (PACV) scale | 182 (31.3%) (3 years—79 (31.9%); 4 years—51 (29.8%); 5 years—52 (31.9%)) | N/A | High (8) |
| 6 | Thapar et al. (2021) [31] | India | South-East Asia Region | Lower middle income | During the months of March and April 2017 | Cross-sectional study | 172 mothers | Mothers of under-five children | Parent Attitudes about Childhood Vaccines (PACV) scale | 6 (3.4%) | 13 (7.6%) | High (9) |
| 7 | S. Yoruk et al. (2021) [35] | Turkey | European Region | Upper middle income | September–December 2020 | Cross-sectional study | 370 parents | Parents of children between 12 months and 6 years old | Parent Attitudes about Childhood Vaccines (PACV) scale | 51 (13.8%); 0–24 months—27 (12.4%); 25–59 months—24 (15.7%) | 18 (4.8%) | High (9) |
| 8 | Durmaz et al. (2022) [36] | Turkey | European Region | Upper middle income | Between September and December 2021 | Cross-sectional study | 1087 parents | Parents of children aged 0–60 months | Parent Attitudes about Childhood Vaccines (PACV) scale | 102 (9.38%) | N/A | High (8) |
| 9 | Hadjipanayis et al. (2020) [45] | 18 European countries: Austria, Bulgaria, Croatia, Cyprus, Germany, Greece, Hungary, Israel, Italy, Lithuania, Malta, Moldova, the Netherlands, Poland, Portugal, Slovenia, Spain, Ukraine | European Region | High income: Austria, Croatia, Cyprus, Germany, Greece, Hungary, Israel, Italy, Lithuania, Malta, the Netherlands, Poland, Portugal, Slovenia, Spain; upper middle income: Bulgaria, Moldova; lower middle income: Ukraine | N/A | Mixed study | 5736 parents; European countries: Austria (n = 368), Bulgaria (n = 479), Croatia (n = 334), Cyprus (n = 463), Germany (n = 256), Greece (n = 210), Hungary (n = 350), Israel (n = 194), Italy (n = 413), Lithuania (n = 318), Malta (n = 201), Moldova (n = 256), the Netherlands (n = 413), Poland (n = 443), Portugal (n = 243), Slovenia (n = 99), Spain (n = 318), Ukraine (n = 372) | Parents having at least one child 1 to 4 years of age, living in one of the participating eighteen European countries | Questionnaire was developed by the European Academy of Paediatrics Research in Ambulatory Setting Network (EAPRASnet) steering committee, based on two sources: PACV and WHO SAGE VHS. Most of the items were taken from PACV, and a minority from the WHO SAGE recommendations | 24% of 5736 respondents defined themselves as “somewhat hesitant” and 4% as “very hesitant”. European countries: Austria 121 (33%), Bulgaria 167 (35%), Croatia 77 (23%), Cyprus 65 (14%), Germany 66 (26%), Greece 69 (33%), Hungary 73 (21%), Israel 81 (42%), Italy 148 (36%), Lithuania 121 (38%), Malta 28 (14%), Moldova 66 (26%), the Netherlands 78 (19%), Poland 181 (41%), Portugal 22 (9%), Slovenia 24 (24%), Spain 54 (17%), Ukraine 149 (40%) | N/A | High (9) |
| 10 | Khattak et al. (2021) [37] | Pakistan | Eastern Mediterranean Region | Lower middle income | From March to July 2019 | Cross-sectional study | 610 parents | Parents with children aged 0–59 months | WHO SAGE Vaccine Hesitancy tool | N/A | 170 (27.9%) refusers | High (9) |
| 11 | Goruntla et al. (2023) [38] | India | South-East Asia Region | Lower middle income | From July to December 2021 | Cross-sectional study | 574 respondents | Mothers of children under 5 years old | WHO SAGE Vaccine Hesitancy tool | 161 (28.05%) | 161 mothers (refusal = 7; delay = 154) | High (9) |
| 12 | Ghosh et al. (2022) [39] | India | South-East Asia Region | Lower middle income | From June 2018 to November 2019 | Cross-sectional study | 1678 caregivers | Caregivers of children aged 1–5 years | WHO SAGE Vaccine Hesitancy tool | 698 parents (41.6%) (˂24 months—225 (41.4%); 24–47 months—196 (47.5%); ˃47 months—277 (38.4%)) | N/A | High (8) |
| 13 | Yakum et al. (2022) [40] | Cameroon | African Region | Lower middle income | November 2021 | Cross-sectional study | 529 parents/guardians | Parents/guardians of children aged 0–59 months | WHO SAGE Vaccine Hesitancy tool | 137 (25%) (without yellow fever vaccine 125 (23.6%)) | N/A | High (8) |
| 14 | Masters et al. (2018) [41] | Ethiopia | African Region | Low income | 1–21 June 2017 | Cross-sectional study | 350 caregivers | Caregivers of children aged 3 to 12 months | WHO SAGE Vaccine Hesitancy tool | 12 (3.44%) | 13 (3.74%) | High (8) |
| 15 | Wang et al. (2022) [52] | China | Western Pacific Region | Upper middle income | From September to October 2020, February to March 2021, May to June 2021 | Three waves of cross-sectional studies | 2881/1038/1183 parents | Parents of children aged ≤ 6 years | Self-administered questionnaire with WHO SAGE Vaccine Hesitancy tool | 225/2881 (7.8%), 157/1038 (15.1%), 65/1183 (5.5%) | N/A | High (7) |
| 16 | Bocquier et al. (2018) [43] | France | European Region | High income | Between January and July 2016 | Cross-sectional telephone survey | 3927 parents (1268 (32%) parents of children aged 3 or younger) | Parents of children aged 1–15 years | Three questions adapted from the SAGE group’s definition of VH | N/A | Refusers = 1090 (26%); Delayers = 272 (7%) (among parents of children aged 3 or younger: Refusers = 270 (21.3%); Delayers = 95 (7.4%)) * | High (8) |
| 17 | Migriño et al. (2020) [44] | Philippines | Western Pacific Region | Lower middle income | N/A | Cross-sectional study | 110 respondents | Parents and caregivers of at least one child 2 years old or younger | A modified questionnaire adapted from the SAGE Working Group on Vaccine Hesitancy | 40 (36.4%) | N/A | High (8) |
| 18 | Neto et al. (2023) [46] | Brazil | Region of the Americas | Upper middle income | From January 2018 to December 2019 | Cross-sectional study | 1261 parents | Parents of children aged up to 72 months | Self-administered questionnaire | 63 (5%) | N/A | High (8) |
| 19 | Campbell et al. (2017) [47] | England | European Region | High income | Between January and April 2015 | Cross-sectional study | 1792 parents (0–2 years = 1130; 3–4 = 999; both ages = 337) | Primary caregivers of children aged from 2 months to ˂5 years | Self-administered questionnaire using computer-assisted personal interviewing | N/A | Refusers = 43 (2%); Delayers = 125 (7%) * | High (8) |
| 20 | Cherian et al. (2022) [48] | India | South-East Asia Region | Lower middle income | From November 2015 to April 2017 | Cross-sectional study | 350 caregivers | Caregivers of children aged 13–24 months | Self-structured questionnaire | 101 (28.9%) | N/A | High (8) |
| 21 | Giambi et al. (2017) [49] | Italy | European Region | High income | In the period December 2015–June 2016 | Cross-sectional study | 3130 parents | Parents of children aged 16–36 months | Self-structured questionnaire | 448 (15.6%) | N/A | High (9) |
| 22 | Voo et al. (2021) [50] | Malaysia | Western Pacific Region | Upper middle income | From February to March 2018 | Cross-sectional study | 405 parents | Parents of children aged 0–4 years | Self-administered questionnaire | 27 (6.8%) | N/A | High (9) |
| 23 | Brown et al. (2018) [51] | Brazil | Region of the Americas | Upper middle income | Between February and July 2016 | Cross-sectional study (online and face-to-face interviews) | 952 parents (352 parents of children aged ≤ 5 years) | Parents of children aged ≤ 5 years | Vaccine Confidence Index (VCI) questionnaire | Overall VH = 16.5% (n = 157). Of the 352 parents of children aged ≤ 5 years, 75 (21.3%) reported VH | Overall refusal rate = 4.5% (n = 43). Of the 352 parents of children aged ≤ 5 years, 6 (1.7%) refused vaccine | High (8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abenova, M.; Shaltynov, A.; Jamedinova, U.; Semenova, Y. Worldwide Child Routine Vaccination Hesitancy Rate among Parents of Children Aged 0–6 Years: A Systematic Review and Meta-Analysis of Cross-Sectional Studies. Vaccines 2024, 12, 31. https://doi.org/10.3390/vaccines12010031
Abenova M, Shaltynov A, Jamedinova U, Semenova Y. Worldwide Child Routine Vaccination Hesitancy Rate among Parents of Children Aged 0–6 Years: A Systematic Review and Meta-Analysis of Cross-Sectional Studies. Vaccines. 2024; 12(1):31. https://doi.org/10.3390/vaccines12010031
Chicago/Turabian StyleAbenova, Madina, Askhat Shaltynov, Ulzhan Jamedinova, and Yuliya Semenova. 2024. "Worldwide Child Routine Vaccination Hesitancy Rate among Parents of Children Aged 0–6 Years: A Systematic Review and Meta-Analysis of Cross-Sectional Studies" Vaccines 12, no. 1: 31. https://doi.org/10.3390/vaccines12010031