

Mapping the Cognitive Biases Related to Vaccination: A Scoping Review of the Literature

Abstract
:1. Introduction
2. Methodology
2.1. Study Process
2.2. Search Strategy
2.3. Databases
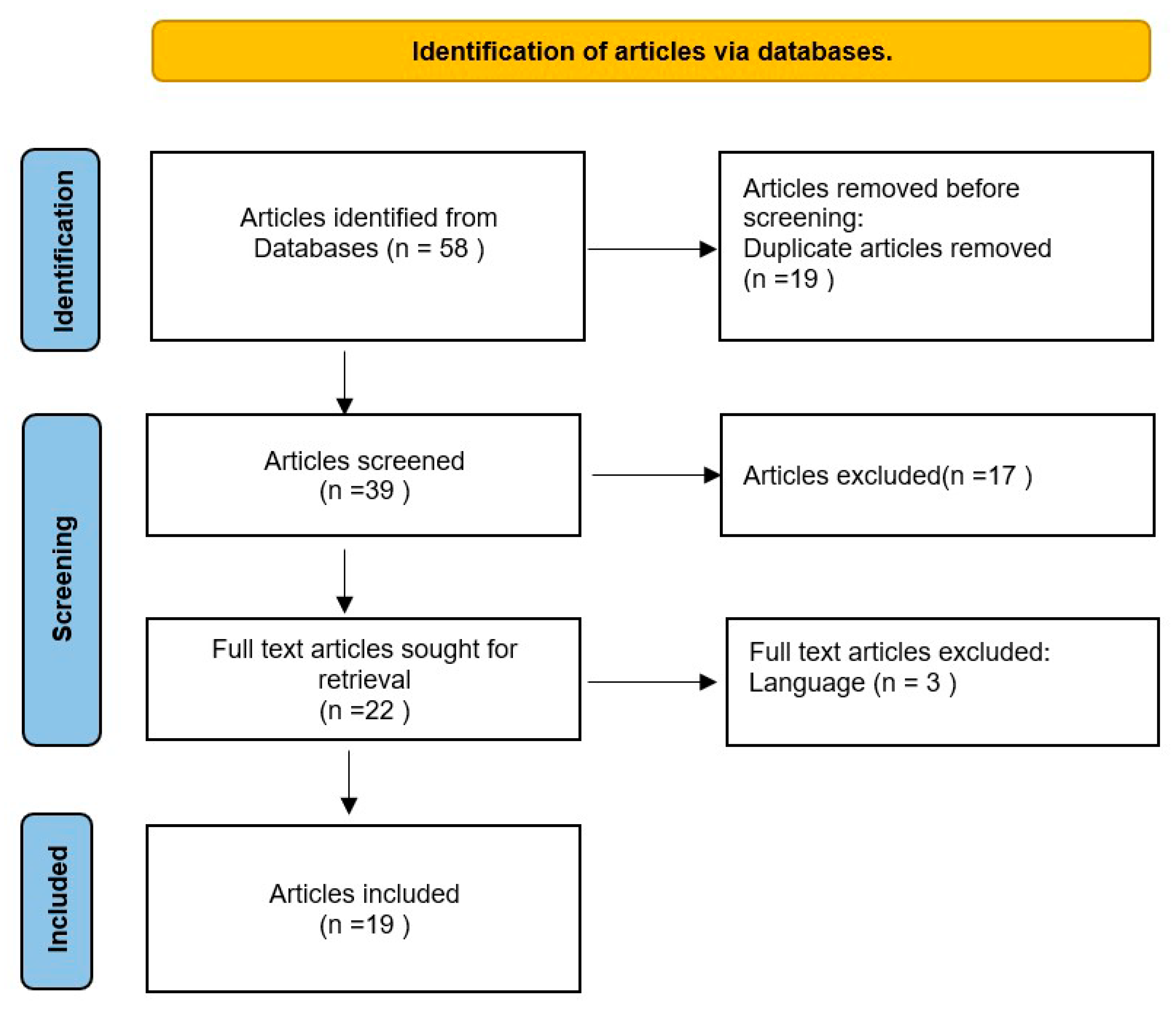
2.4. Study Selection
2.5. Data Extraction
2.6. Analysis and Data Items
2.7. Identification of Knowledge Gaps
3. Results
3.1. Group #1: Cognitive Biases Seen during Processing of Vaccine-Related Information
3.2. Group #2: Cognitive Biases Seen during Vaccination Decision-Making
3.3. Group #3: Cognitive Biases Due to Prior Beliefs Regarding Vaccination
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Orgranization. National Regulatory Authority of India Meets WHO International Standards for Vaccine Regulations; WHO South-East Asia Region: New Delhi, India, 2017; Available online: https://www.who.int/india/news/detail/12-07-2017-national-regulatory-authority-of-india-meets-who-international-standards-for-vaccine-regulations (accessed on 10 October 2023).
- Streefland, P.; Chowdhury, A.M.R.; Ramos-jimenez, P. Patterns of Vaccination Acceptance. Soc. Sci. Med. 1999, 49, 1705–1716. [Google Scholar] [CrossRef]
- Manfredi, P.; d’Onofrio, A. Modeling the Interplay between Human Behaviour and the Spread of Infectious Diseases; Springer Science and Business Media: New York, NY, USA, 2013. [Google Scholar]
- Jansen, V.A.A.; Funk, S.; Salathe, M. Modelling the Influence of Human Behaviour on the Spread of Infectious Diseases: A Review. J. R. Soc. Interface 2010, 7, 1247–1256. [Google Scholar]
- Voinson, M.; Billiard, S.; Alvergne, A. Beyond Rational Decision-Making: Modelling the Influence of Cognitive Biases on the Dynamics of Vaccination Coverage. PLoS ONE 2015, 10, e0167842. [Google Scholar] [CrossRef] [PubMed]
- Novilla, M.L.B.; Goates, M.C.; Redelfs, A.H.; Quenzer, M.; Novilla, L.K.B.; Leffler, T.; Holt, C.A.; Doria, R.B.; Dang, M.T.; Hewitt, M.; et al. Why Parents Say No to Having Their Children Vaccinated against Measles: A Systematic Review of the Social Determinants of Parental Perceptions on MMR Vaccine Hesitancy. Vaccines 2023, 11, 926. [Google Scholar] [CrossRef] [PubMed]
- Ashkenazi, S.; Livni, G.; Klein, A.; Kremer, N.; Havlin, A.; Berkowitz, O. The Relationship between Parental Source of Information and Knowledge about Measles/Measles Vaccine and Vaccine Hesitancy. Vaccine 2020, 38, 7292–7298. [Google Scholar] [CrossRef] [PubMed]
- Buss, D.M. The Handbook of Evolutionary Psychology; John Wiley & Sons: New York, NY, USA, 2015. [Google Scholar]
- Delgado-Rodríguez, M.; Llorca, J. Bias. J. Epidemiol. Community Health 2004, 58, 629. [Google Scholar] [CrossRef] [PubMed]
- Cambridge Dictionary. Bias. Cambridge Dictionary. Available online: https://dictionary.cambridge.org/dictionary/english/bias (accessed on 10 October 2023).
- Arksey, H.; Malley, L.O. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2007, 5579. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; Brien, K.K.O. Scoping Studies: Advancing the Methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Hansen, C.E.; North, A.; Niccolai, L.M. Cognitive Bias in Clinicians’ Communication about Human Papillomavirus Vaccination. Health Commun. 2020, 35, 430–437. [Google Scholar] [CrossRef]
- Azarpanah, H.; Farhadloo, M.; Vahidov, R.; Pilote, L. Vaccine Hesitancy: Evidence from an Adverse Events Following Immunization Database, and the Role of Cognitive Biases. BMC Public Health 2021, 21, 1686. [Google Scholar] [CrossRef]
- Tversky, A.; Kahneman, D. The Framing of Decisions and the Psychology of Choice. Science 1981, 211, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, K.T.; Buboltz, W.; Levin, I.P.; Doverspike, D.; Svyantek, D.J. Individual Differences in a Within-Subjects Risky-Choice Framing Study. Pers. Individ. Dif. 2011, 51, 248–257. [Google Scholar] [CrossRef]
- Stengård, E.; Juslin, P.; Hahn, U.; Van Den Berg, R. On the Generality and Cognitive Basis of Base-Rate Neglect. Cognition 2022, 226, 105160. [Google Scholar] [CrossRef] [PubMed]
- Cherry, K. How Anchoring Bias Affects Decision-Making. Verywellmind, 8 October 2023. Available online: https://www.verywellmind.com/what-is-the-anchoring-bias-2795029 (accessed on 23 October 2023).
- Tversky, A.; Kahneman, D. Evidential Impact of Base Rates. In Judgment Under Uncertainty: Heuristics and Biases; American Association for the Advancement of Science: Washington, DC, USA, 1981; p. 153. [Google Scholar]
- Brown, K.F.; Kroll, J.S.; Hudson, M.J.; Ramsay, M.; Green, J.; Vincent, C.A.; Fraser, G.; Sevdalis, N. Omission Bias and Vaccine Rejection by Parents of Healthy Children: Implications for the Influenza A/H1N1 Vaccination Programme. Vaccine 2010, 28, 4181–4185. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.C.; Sweetman, G. A Healthcare Quality Management System Underpinning the 3-E Model and Its Application in a New Tertiary Hospital in Australia. Int. J. Nurs. Sci. 2017, 4, 112–116. [Google Scholar] [CrossRef]
- Dubov, A.; Phung, C. Nudges or Mandates? The Ethics of Mandatory Flu Vaccination. Vaccine 2015, 33, 2530–2535. [Google Scholar] [CrossRef]
- Tversky, A.; Kahneman, D. Judgment under Uncertainty: Heuristics and Biases: Biases in Judgments Reveal Some Heuristics of Thinking under Uncertainty. Science 1974, 185, 1124–1131. [Google Scholar] [CrossRef]
- Smith, J.C.; Appleton, M.; MacDonald, N.E. Building Confidence in Vaccines. In Advances in Experimental Medicine and Biology; Curtis, N., Finn, A., Pollard, A.J., Eds.; Springer: New York, NY, USA, 2013; pp. 81–98. [Google Scholar]
- Van Woensel, L. A Bias Radar for Responsible Policy-Making; Healey, D., Payne, L., Eds.; St. Antony’s Series; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Mansour, S.B.; Jouini, E.; Napp, C. Is There a “Pessimistic” Bias in Individual Beliefs? Evidence from a Simple Survey. Theory Decis. 2006, 61, 345–362. [Google Scholar] [CrossRef]
- Betsch, C.; Sachse, K. Debunking Vaccination Myths: Strong Risk Negations Can Increase Perceived Vaccination Risks. Health Psychol. 2013, 32, 146–155. [Google Scholar] [CrossRef]
- Baron, J.; Ritov, I. Omission Bias, Individual Differences, and Normality. Organ. Behav. Hum. Decis. Process. 2004, 94, 74–85. [Google Scholar] [CrossRef]
- Asch, D.A.; Baron, J.; Hershey, J.C.; Kunreuther, H.; Meszaros, J.; Ritov, I. Omission Bias and Pertussis Vaccination. Med. Decis. Mak. 1994, 14, 118–123. [Google Scholar] [CrossRef]
- Ritov, I.; Baron, J. Protected Values and Omission Bias. Organ. Behav. Hum. Decis. Process. 1999, 79, 79–94. [Google Scholar] [CrossRef] [PubMed]
- Lumen. Barriers to Individual Decision Making and Styles of Decision Making. Available online: https://courses.lumenlearning.com/wmopen-principlesofmanagement/chapter/introduction-the-decision-making-process/ (accessed on 23 October 2023).
- Cherry, K. Understanding the Optimism Bias: AKA the Illusion of Invulnerability. Verywellmind, 17 February 2022. Available online: https://www.verywellmind.com/what-is-the-optimism-bias-2795031 (accessed on 23 October 2023).
- Omer, S.B.; Salmon, D.A.; Orenstein, W.A.; de Hart, M.P.; Halsey, N. Vaccine Refusal, Mandatory Immunization, and the Risks of Vaccine-Preventable Diseases. N. Engl. J. Med. 2009, 360, 1981–1988. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.R.; Tversky, A. Ambiguity Aversion and Comparative Ignorance. Q. J. Econ. 1995, 110, 585–603. [Google Scholar] [CrossRef]
- Ball, L.K.; Evans, G.; Bostrom, A. Risky Business: Challenges in Vaccine Risk Communication. Pediatrics 1998, 101, 453–458. [Google Scholar] [CrossRef]
- Krantz, D.; Rabin, M. Loss Aversion in Riskless Choice: A Reference-Dependent Model. Q. J. Econ. 1991, 106, 1039–1061. [Google Scholar]
- Seethaler, S.L. Shades of Grey in Vaccination Decision Making: Tradeoffs, Heuristics, and Implications. Sci. Commun. 2016, 38, 2. [Google Scholar] [CrossRef]
- Bond, L.; Nolan, T. Making Sense of Perceptions of Risk of Diseases and Vaccinations: A Qualitative Study Combining Models of Health Beliefs, Decision-Making and Risk Perception. BMC Public Health 2011, 11, 943. [Google Scholar] [CrossRef]
- Duginan, B. Dunning-Kruger Effect. Available online: https://www.britannica.com/science/Dunning-Kruger-effect (accessed on 10 October 2023).
- Motta, M.; Callaghan, T.; Sylvester, S. Knowing Less but Presuming More: Dunning-Kruger Effects and the Endorsement of Anti-Vaccine Policy Attitudes. Soc. Sci. Med. 2018, 211, 274–281. [Google Scholar] [CrossRef]
- Samelson, W.; Zeckhauser, R. Status Quo Bias in Decision Making. J. Risk Uncertain. 1988, 59, 7–59. [Google Scholar] [CrossRef]
- Kata, A. A Postmodern Pandora’s Box: Anti-Vaccination Misinformation on the Internet. Vaccine 2010, 28, 1709–1716. [Google Scholar] [CrossRef] [PubMed]
- Pope, J.W. False Consensus Effect. In Encyclopedia of Cross-Cultural Psychology; Wiley-Blackwell: Hoboken, NJ, USA, 2013; pp. 2009–2011. [Google Scholar]
- Kreps, S.; Dasgupta, N.; Brownstein, J.S.; Hswen, Y.; Kriner, D.L. Public Attitudes toward COVID-19 Vaccination: The Role of Vaccine Attributes, Incentives, and Misinformation. npj Vaccines 2021, 6, 73. [Google Scholar] [CrossRef] [PubMed]
- Clear Thinking Team. Default Effect: Definition, Examples and Effects. Clear Thinking, 31 Decemeber 2020. Available online: https://www.clearerthinking.org/post/default-effect-definition-examples-and-effects/ (accessed on 23 October 2023).
- Nickerson, R.S. Confirmation Bias: A Ubiquitous Phenomenon in Many Guises. Rev. J. Psychol. 1998, 2, 175–220. [Google Scholar] [CrossRef]
- Meszaros, J.R.; David, A.A.; Baron, J.; Hershey, J.C.; Kunreuther, H.; Schwartz-buzagloj, J. Cognitive Processes and the Decisions of Some Parents to Forego Pertussis Vaccination for Their Children. J. Clin. Epidemiol. 1996, 49, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.S.B.T. In Two Minds: Dual-Process Accounts of Reasoning. Trends Cogn. Sci. 2003, 7, 454–459. [Google Scholar] [CrossRef]
- Van Swol, L.M. Perceived Importance of Information: The Effects of Mentioning Information, Shared Information Bias, Ownership Bias, Reiteration, and Confirmation Bias. Gr. Process. Intergr. Relat. 2007, 10, 239–256. [Google Scholar] [CrossRef]
- Krueger, J.; Clement, R.W. The Truly False Consensus Effect: An Ineradicable and Egocentric Bias in Social Perception. J. Pers. Soc. Psychol. 1994, 67, 596–610. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.M.; Mckeever, B.W.; Mckeever, R.; Kim, J.K.; Jang, S.M.; Mckeever, B.W.; Mckeever, R.; Kim, J.K.; Jang, S.M. From Social Media to Mainstream News: The Information Flow of the Vaccine-Autism Controversy in the US, Canada, and the UK From Social Media to Mainstream News: The Information Flow of the Vaccine-Autism Controversy in the US, Canada, and the UK. Health Commun. 2019, 34, 110–117. [Google Scholar] [CrossRef]
- Mcleod, S. What Is Cognitive Dissonance Theory? Simply Psychology. 24 October 2023. Available online: https://www.simplypsychology.org/cognitive-dissonance.html (accessed on 24 October 2023).
- Illusory Correlation. Psychology, 8 January 2016. Available online: http://psychology.iresearchnet.com/social-psychology/decision-making/illusory-correlation/ (accessed on 23 October 2023).
- Moore, G.E. Principia Ethica; Cambridge University Press: Cambridge, UK, 1903. [Google Scholar]
- Meier, B.P.; Lappas, C.M. The Influence of Safety, Efficacy, and Medical Condition Severity on Natural versus Synthetic Drug Preference. Med. Decis. Mak. 2016, 36, 1011–1019. [Google Scholar] [CrossRef]
- American Medical Association. AMA Adopts New Policy Aimed at Addressing Public Health Disinformation. American Medical Association. 2022. Available online: https://www.ama-assn.org/press-center/press-releases/ama-adopts-new-policy-aimed-addressing-public-health-disinformation (accessed on 20 October 2023).
- Institute for Government. Policy Making. Institute for Government. Available online: https://www.instituteforgovernment.org.uk/our-work/topics/policy-making (accessed on 11 October 2023).
- Centre for Action Learning. Action Learning. Available online: https://centreforactionlearning.com/action-learning/ (accessed on 11 October 2023).
- Hornsey, M.J.; Trembath, M.; Gunthorpe, S. ‘You Can Criticize Because You Care’: Identity Attachment, Constructiveness, and the Intergroup Sensitivity Effect. Eur. J. Soc. Psychol. 2004, 518, 499–518. [Google Scholar] [CrossRef]
- Weigert, M. How the Internet Amplifies Our Cognitive Biases. HackerNoon, 11 April 2019. Available online: https://hackernoon.com/in-the-digital-age-cognitive-biases-are-running-wild-420b8f4f7cb5 (accessed on 11 October 2023).
- Tricco, A.C.; Lillie, E.; Zarin, W.; Brien, K.K.O.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Ma, Q.; Horsley, T.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No. | Cognitive Bias | Definition | Example |
|---|---|---|---|
| 1 | Framing effect | The agent’s decision is influenced if you compose a message without changing the primary message [15]. | By highlighting the lesser proportion of patients with AEFIs than the majority of patients with no AEFIs, one might cast doubt on the effectiveness of vaccination. |
| 2 | Base-rate neglect | The inclination to prioritize specialized information while ignoring broad information despite the fact that the latter is more crucial [19]. | Rare AEFIs are overestimated, whereas typical, moderate AEFIs are underestimated [20]. |
| 3 | Availability bias | The inclination to give elements that are simpler to remember more weight [21]. | The media coverage of a rare serious or severe AEFI incident provides a dramatic and emotionally stirring message that is likely to be remembered when vaccination decisions are made [22]. |
| 4 | Anchoring effect | The capacity for making decisions that largely depend on values that are originally offered [23]. | One sees a side effect after vaccination and thinks that vaccines with that particular side effect are more prevalent [24]. |
| 5 | Authority bias | The tendency to give the opinions of people of authority greater weight [25]. | When a medical practitioner disseminates anti-vaccination material, it may influence individuals to choose not to be vaccinated since the medical practitioner is an authoritative person. |
| 6 | Pessimism bias | The propensity to overestimate the chance of bad things happening while underestimating the likelihood of good things happening is known as pessimistic bias [26]. | Children will likely not have an AEFI after receiving a vaccine, but anxious/panic/depressed parents may think they will. |
| 7 | Negativity bias | More trust is given to negative information than positive information [27]. | More focus is placed on rare adverse events associated with vaccines than their overwhelming benefits. |
| No. | Cognitive Bias | Definition | Example |
|---|---|---|---|
| 1 | Omission bias | The propensity to undervalue the consequences of taking action (commission) even when the consequences of inaction are worse or on equal to those of action (omission) [29]. | When parents foresee AEFIs, they prefer to omit immunization because they view it as a commission (not vaccinating). |
| 2 | Ambiguity aversion | The propensity, regardless of consequences, to choose a known danger over an unknown risk [34]. | People choose established risks from diseases over more uncertain risks associated with vaccination against the same disease [35]. |
| 3 | Loss aversion | The propensity to place more importance on preventing losses than making equal gains [36]. | Patients may only concentrate on a 1% probability of experiencing AEs while discussing AEFIs rather than the 99% possibility of no AEs [37]. |
| 4 | Optimism bias | The propensity to view a specific health issue with an overly positive outlook and believe that others face it more seriously than oneself [22]. | People believe they are healthy, immune to the flu, and able to fight it off, so they do not think of themselves as being at danger of contracting it [38]. |
| 5 | Present bias | The tendency to prioritize current expenditures and advantages above those obtained in the future [22]. | People are more aware of the adverse reactions to vaccines (as a cost); thus, they are given greater weight. Future benefits that are not immediately obvious are given less weight, such as immunity to a disease. |
| 6 | Protected values | Protecting absolute ideals that individuals believe should not be sold off should not be a priority [30]. | Respecting parents’ choice about vaccination [13]. |
| 7 | The Dunning–Kruger effect | A cognitive bias in which individuals with relatively poor intellectual or social ability substantially overestimate their own knowledge or competence in that subject in comparison to external standards, the performance of their peers, or that of the general population [39]. | Anti-vaccination policy attitudes [40]. |
| 8 | Status quo bias | When someone prefers to do nothing or adhere to a past choice, it is clear that they are biased [41]. | Unvaccinated children remain unvaccinated due to parents’ status quo thinking. |
| No. | Cognitive Bias | Definition | Example |
|---|---|---|---|
| 1 | Confirmation bias | The propensity to remember and understand data that support our preexisting ideas [46]. | People who are vaccine-hesitant exaggerate AEFIs and downplay the threat of diseases that may be prevented by vaccination [5,47]. People tend to focus on what matters to them and ignore what does not, which often results in the “ostrich effect,” in which a person buries their head in the sand to avoid facts that would contradict their initial assertion. |
| 2 | Belief bias | The propensity to assess the validity of an argument is dependent on the conclusion’s plausibility [48]. | It would be ineffective to discuss vaccine safety in terms of minor AEFIs with those who think vaccination programs are driven by huge businesses’ profits. |
| 3 | Shared information bias | The propensity to focus more time and effort on material that group members are already acquainted with while spending less time and effort on fresh information [49]. | Concentrating on just a few anti-vaccine issues, such as the disproved MMR–autism connection on internet anti-vaccine echo chambers. |
| 4 | False consensus effect | The propensity to exaggerate how much one’s viewpoint is shared by the wider public [50]. | Mothers who are against (for) vaccination are more (less) likely to discuss the topic on social media [51]. This leads to the development of strong false consensuses on vaccine reluctance in online groups. |
| 5 | Cognitive dissonance | Cognitive dissonances are beliefs, attitudes, or behavior that clash with each other [52]. One of these attitudes, beliefs, or behaviors changes as a reaction to the mental discomfort that results from this in an attempt to reduce the discomfort and restore balance. | If a parent learns that vaccinations are effective but is also concerned that they can endanger their kid, they may conclude that vaccines do not function in order to get rid of the cognitive dissonance. |
| 6 | Illusory correlation | The illusory correlation is the assumption of a link between two variables when it is likely not true [53]. | Any instance of autism and vaccination co-occurring is used by parents to justify their decision to not vaccinate because they have a preconceived notion that there is a link between vaccination and autism. |
| 7 | Appeal to nature bias/fallacy | When it is suggested that something is good because it is natural or bad because it is unnatural, there is bias involved [54] | Some individuals place a higher value on innate immunity than artificially induced immunity boosters like vaccinations [55] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raj, A.; Singh, A.K.; Wagner, A.L.; Boulton, M.L. Mapping the Cognitive Biases Related to Vaccination: A Scoping Review of the Literature. Vaccines 2023, 11, 1837. https://doi.org/10.3390/vaccines11121837
Raj A, Singh AK, Wagner AL, Boulton ML. Mapping the Cognitive Biases Related to Vaccination: A Scoping Review of the Literature. Vaccines. 2023; 11(12):1837. https://doi.org/10.3390/vaccines11121837
Chicago/Turabian StyleRaj, Amar, Awnish Kumar Singh, Abram L. Wagner, and Matthew L. Boulton. 2023. "Mapping the Cognitive Biases Related to Vaccination: A Scoping Review of the Literature" Vaccines 11, no. 12: 1837. https://doi.org/10.3390/vaccines11121837