
Trends in Vaccine Completeness in Children Aged 0–23 Months in Cape Town, South Africa

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
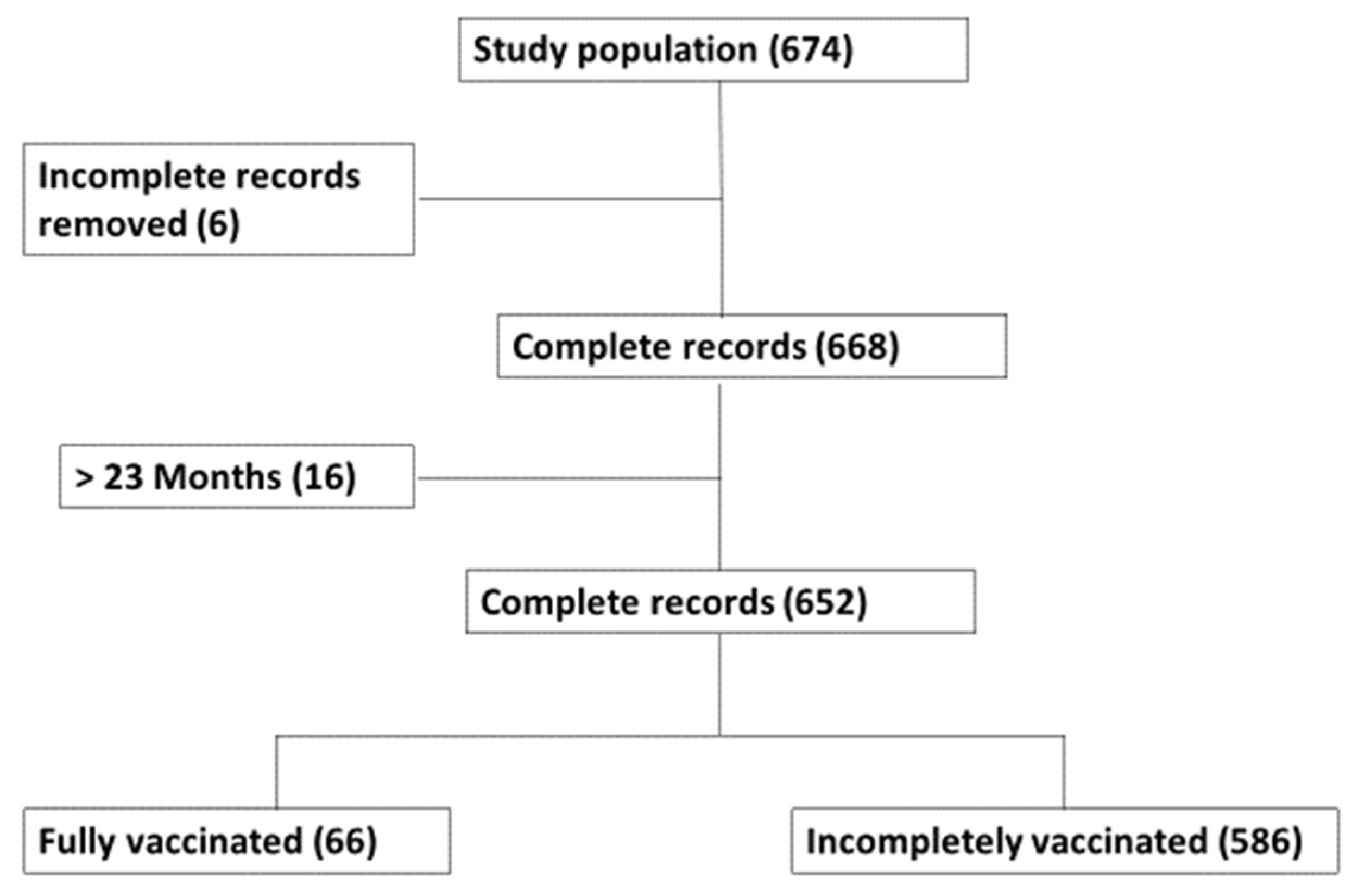
2.2. Study Population and Sample Size
2.3. Data Collection
2.4. Data Analysis
2.5. Study Variables
3. Results
3.1. Dose-Specific Vaccination Prevalence
3.2. Socio-Demographic Characteristics of the Mother/Caregiver and the Child
3.2.1. Influence of Basic Demographic Characteristics on the Vaccination Status
3.2.2. Influence of Vaccination Visit on the Vaccination Status
3.2.3. Influence of Caregiver Position, Education Level, and Employment Standing on the Vaccination Status
3.2.4. Influence of Transport during Vaccination Visit and Facility Characteristics on the Vaccination Status
3.3. Mother/Caregiver Related Factors
3.4. Measurement of Factors Associated with Missed Opportunity Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ghattas, M.; Dwivedi, G.; Lavertu, M.; Alameh, M.G. Vaccine Technologies and Platforms for Infectious Diseases: Current Progress, Challenges, and Opportunities. Vaccines 2021, 9, 1490. [Google Scholar] [CrossRef] [PubMed]
- Orenstein, W.A.; Ahmed, R. Simply put: Vaccination saves lives. Proc. Natl. Acad. Sci. USA 2017, 114, 4031–4033. [Google Scholar] [CrossRef] [PubMed]
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Achoki, T.; Sartorius, B.; Watkins, D.; Glenn, S.D.; Kengne, A.P.; Oni, T.; Wiysonge, C.S.; Walker, A.; Adetokunboh, O.O.; Babalola, T.K.; et al. Health trends, inequalities and opportunities in South Africa’s provinces, 1990–2019: Findings from the Global Burden of Disease 2019 Study. J. Epidemiol. Community Health 2022, 76, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Attwell, K.; Ward, P.R.; Meyer, S.B.; Rokkas, P.J.; Leask, J. “Do-it-yourself”: Vaccine rejection and complementary and alternative medicine (CAM). Soc. Sci. Med. 2018, 196, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Montalbán, A.; Corder, R.M.; Gomes, M.G.M. Herd immunity under individual variation and reinfection. J. Math. Biol. 2022, 85, 2. [Google Scholar] [CrossRef] [PubMed]
- Kartoglu, U.; Ames, H. Ensuring quality and integrity of vaccines throughout the cold chain: The role of temperature monitoring. Expert. Rev. Vaccines 2022, 21, 799–810. [Google Scholar] [CrossRef]
- Brisse, M.; Vrba, S.M.; Kirk, N.; Liang, Y.; Ly, H. Emerging Concepts and Technologies in Vaccine Development. Front. Immunol. 2020, 11, 583077. [Google Scholar] [CrossRef]
- Fine, P.; Eames, K.; Heymann, D.L. “Herd immunity”: A rough guide. Clin. Infect. Dis. 2011, 52, 911–916. [Google Scholar] [CrossRef]
- Nnaji, C.A.; Wiysonge, C.S.; Cooper, S.; Mayeye, A.; Luphondo, L.; Mabuya, T.; Kalui, N.; Lesosky, M.; Ndwandwe, D. Contextualising missed opportunities for children’s vaccination: A theory-informed qualitative study in primary care settings in Cape Town, South Africa. Hum. Vaccines Immunother. 2023, 19, 2162771. [Google Scholar] [CrossRef]
- Ndwandwe, D.; Nnaji, C.A.; Mashunye, T.; Uthman, O.A.; Wiysonge, C.S. Incomplete vaccination and associated factors among children aged 12–23 months in South Africa: An analysis of the South African demographic and health survey 2016. Hum. Vaccines Immunother. 2021, 17, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Turok, I.; Visagie, J.; Scheba, A. Social inequality and spatial segregation in Cape Town. In Urban Socio-Economic Segregation and Income Inequality: A Global Perspective; Springer: Berlin/Heidelberg, Germany, 2021; pp. 71–90. [Google Scholar]
- Cooper, S.; van Rooyen, H.; Wiysonge, C.S. COVID-19 vaccine hesitancy in South Africa: How can we maximize uptake of COVID-19 vaccines? Expert. Rev. Vaccines 2021, 20, 921–933. [Google Scholar] [CrossRef] [PubMed]
- Burnett, R.J.; Larson, H.J.; Moloi, M.H.; Tshatsinde, E.A.; Meheus, A.; Paterson, P.; François, G. Addressing public questioning and concerns about vaccination in South Africa: A guide for healthcare workers. Vaccine 2012, 30 (Suppl. S3), C72–C78. [Google Scholar] [CrossRef] [PubMed]
- Coetzee, D.J.; Ferrinho, P.; Reinach, S.G. A vaccination survey using the EPI methodology ot evaluate the impact of a child health outreach programme in an urban area of South Africa. Bull. World Health Organ. 1993, 71, 33–39. [Google Scholar] [PubMed]
- Ijsselmuiden, C.B.; Küstner, H.G.; Barron, P.M.; Steinberg, W.J. Notification of five of the EPI target diseases in South Africa. An assessment of disease and vaccination reporting. S. Afr. Med. J. 1987, 72, 311–316. [Google Scholar] [PubMed]
- Cooper, C.A. Vaccine hesitancy and respect for public health measures: Citizens’ trust in politicians and public servants across national, subnational and municipal levels of government. SSM Popul. Health 2023, 22, 101386. [Google Scholar] [CrossRef] [PubMed]
- Sewpaul, R.; Sifunda, S.; Gaida, R.; Mokhele, T.; Naidoo, I.; Reddy, S.P. Vaccine hesitancy and related factors among South African adults in 2021: Unpacking uncertainty versus unwillingness. Front. Public Health 2023, 11, 1233031. [Google Scholar] [CrossRef]
- Ackah, B.B.B.; Woo, M.; Stallwood, L.; Fazal, Z.A.; Okpani, A.; Ukah, U.V.; Adu, P.A. COVID-19 vaccine hesitancy in Africa: A scoping review. Glob. Health Res. Policy 2022, 7, 21. [Google Scholar] [CrossRef]
- Burger, R.; Köhler, T.; Golos, A.M.; Buttenheim, A.M.; English, R.; Tameris, M.; Maughan-Brown, B. Longitudinal changes in COVID-19 vaccination intent among South African adults: Evidence from the NIDS-CRAM panel survey, February to May 2021. BMC Public Health 2022, 22, 422. [Google Scholar] [CrossRef]
- Piltch-Loeb, R.; Mazibuko, L.; Stanton, E.; Mngomezulu, T.; Gareta, D.; Nxumalo, S.; Kraemer, J.D.; Herbst, K.; Siedner, M.J.; Harling, G. COVID-19 vaccine uptake, confidence and hesitancy in rural KwaZulu-Natal, South Africa between April 2021 and April 2022: A continuous cross-sectional surveillance study. PLoS Glob. Public Health 2023, 3, e0002033. [Google Scholar] [CrossRef]
- Wollburg, P.; Markhof, Y.; Kanyanda, S.; Zezza, A. Assessing COVID-19 vaccine hesitancy and barriers to uptake in Sub-Saharan Africa. Commun. Med. (Lond) 2023, 3, 121. [Google Scholar] [CrossRef] [PubMed]
- Engelbrecht, M.; Heunis, C.; Kigozi, G. COVID-19 Vaccine Hesitancy in South Africa: Lessons for Future Pandemics. Int. J. Environ. Res. Public Health 2022, 19, 6694. [Google Scholar] [CrossRef] [PubMed]
- Steenberg, B.; Myburgh, N.; Sokani, A.; Ngwenya, N.; Mutevedzi, P.; Madhi, S.A. COVID-19 Vaccination Rollout: Aspects of Acceptability in South Africa. Vaccines 2022, 10, 1379. [Google Scholar] [CrossRef] [PubMed]
- Nnaji, C.A.; Wiysonge, C.S.; Adamu, A.A.; Lesosky, M.; Mahomed, H.; Ndwandwe, D. Missed Opportunities for Vaccination and Associated Factors among Children Attending Primary Health Care Facilities in Cape Town, South Africa: A Pre-Intervention Multilevel Analysis. Vaccines 2022, 10, 785. [Google Scholar] [CrossRef] [PubMed]
- Phillips, D.E.; Dieleman, J.L.; Lim, S.S.; Shearer, J. Determinants of effective vaccine coverage in low and middle-income countries: A systematic review and interpretive synthesis. BMC Health Serv. Res. 2017, 17, 681. [Google Scholar] [CrossRef]
- Corrigall, J.; Coetzee, D.; Cameron, N. Is the Western Cape at risk of an outbreak of preventable childhood diseases? Lessons from an evaluation of routine immunisation coverage. S. Afr. Med. J. 2008, 98, 41–45. [Google Scholar]
- Kazungu, J.S.; Adetifa, I.M.O. Crude childhood vaccination coverage in West Africa: Trends and predictors of completeness. Wellcome Open Res 2017, 2, 12. [Google Scholar] [CrossRef]
- Iwu, C.J.; Ngcobo, N.; Jaca, A.; Wiyeh, A.; Pienaar, E.; Chikte, U.; Wiysonge, C.S. A systematic review of vaccine availability at the national, district, and health facility level in the WHO African Region. Expert. Rev. Vaccines 2020, 19, 639–651. [Google Scholar] [CrossRef]
- Iwu-Jaja, C.J.; Jordan, P.; Ngcobo, N.; Jaca, A.; Iwu, C.D.; Mulenga, M.; Wiysonge, C. Improving the availability of vaccines in primary healthcare facilities in South Africa: Is the time right for a system redesign process? Hum. Vaccines Immunother. 2022, 18, 1926184. [Google Scholar] [CrossRef]
- National Department of Health (NDoH); South African Medical Research Council. South Africa Demographic and Health Survey 2016: Key Indicators. 2019. Available online: https://dhsprogram.com/pubs/pdf/FR337/FR337.pdf (accessed on 3 August 2023).
- Western Cape Province Department of Health. Cape Metro District Health Plan. 2018–2020. Available online: https://resource.capetown.gov.za/documentcentre/Documents/City%20strategies,%20plans%20and%20frameworks/Metro%20District%20Health%20Plan_2019-20.pdf (accessed on 5 August 2023).
- Hu, Y.; Chen, Y.; Guo, J.; Tang, X.; Shen, L. Completeness and timeliness of vaccination and determinants for low and late uptake among young children in eastern China. Hum. Vaccines Immunother. 2014, 10, 1408–1415. [Google Scholar] [CrossRef]
- Dummer, T.J.; Cui, Y.; Strang, R.; Parker, L. Immunization completeness of children under two years of age in Nova Scotia, Canada. Can. J. Public Health 2012, 103, e363–e367. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, S.; Maleq, N.; Guillermet, E.; Colombini, A.; Gessner, B.D. A systematic literature review of missed opportunities for immunization in low- and middle-income countries. Vaccine 2014, 32, 6870–6879. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.L. Recommended solutions to the barriers to immunization in children and adults. Mo. Med. 2014, 111, 344–348. [Google Scholar] [PubMed]
- Forshaw, J.; Gerver, S.M.; Gill, M.; Cooper, E.; Manikam, L.; Ward, H. The global effect of maternal education on complete childhood vaccination: A systematic review and meta-analysis. BMC Infect. Dis. 2017, 17, 801. [Google Scholar] [CrossRef] [PubMed]
- Guyer, B.; Atangana, S. A programme of multiple-antigen childhood immunization in Yaoundé, Cameroon: First-year evaluation, 1975–1976. Bull. World Health Organ. 1977, 55, 633–642. [Google Scholar] [PubMed]
- Bangura, J.B.; Xiao, S.; Qiu, D.; Ouyang, F.; Chen, L. Barriers to childhood immunization in sub-Saharan Africa: A systematic review. BMC Public Health 2020, 20, 1108. [Google Scholar] [CrossRef] [PubMed]
- Anatea, M.D.; Mekonnen, T.H.; Dachew, B.A. Determinants and perceptions of the utilization of tetanus toxoid immunization among reproductive-age women in Dukem Town, Eastern Ethiopia: A community-based cross-sectional study. BMC Int. Health Hum. Rights 2018, 18, 27. [Google Scholar] [CrossRef]
- Bary-Weisberg, D.; Stein-Zamir, C. Vaccination timeliness and completeness among preterm and low birthweight infants: A national cohort study. Hum. Vaccines Immunother. 2021, 17, 1666–1674. [Google Scholar] [CrossRef]
- Peck, M.; Gacic-Dobo, M.; Diallo, M.S.; Nedelec, Y.; Sodha, S.V.; Wallace, A.S. Global Routine Vaccination Coverage, 2018. Morb. Mortal. Wkly. Rep. 2019, 68, 937–942. [Google Scholar] [CrossRef]
- Kayser, V.; Ramzan, I. Vaccines and vaccination: History and emerging issues. Hum. Vaccines Immunother. 2021, 17, 5255–5268. [Google Scholar] [CrossRef]
- Frew, P.M.; Lutz, C.S. Interventions to increase pediatric vaccine uptake: An overview of recent findings. Hum. Vaccines Immunother. 2017, 13, 2503–2511. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.; Ryan, R.; Walsh, L.; Horey, D.; Leask, J.; Robinson, P.; Hill, S. Face-to-face interventions for informing or educating parents about early childhood vaccination. Cochrane Database Syst. Rev. 2018, 5, Cd010038. [Google Scholar] [CrossRef] [PubMed]
- Bobo, F.T.; Asante, A.; Woldie, M.; Dawson, A.; Hayen, A. Child vaccination in sub-Saharan Africa: Increasing coverage addresses inequalities. Vaccine 2022, 40, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, A.A.; Alghamdi, H.A. Knowledge, Attitude, and Practice of Vaccination Among Parents in Jeddah City, Saudi Arabia. Cureus 2023, 15, e41721. [Google Scholar] [CrossRef]
- Ames, H.M.; Glenton, C.; Lewin, S. Parents’ and informal caregivers’ views and experiences of communication about routine childhood vaccination: A synthesis of qualitative evidence. Cochrane Database Syst. Rev. 2017, 2, Cd011787. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Eligible Age | Vaccine Offered (Dose) | Eligible | Vaccinated (%) | Not Vaccinated (%) |
|---|---|---|---|---|
| Birth | BCG | 652 | 637 (97.70) | 15 (2.30) |
| OPV (0) | 652 | 630 (96.63) | 22 (3.37) | |
| 6 Weeks | OPV (1) | 544 | 505 (92.83) | 39 (7.17) |
| RV (1) | 544 | 537 (98.71) | 7 (1.29) | |
| DTaP-IPV-Hib-HepB (1) | 544 | 537 (98.71) | 7 (1.29) | |
| PCV (1) | 544 | 536 (98.53) | 8 (1.47) | |
| 10 Weeks | DTaP-IPV-HIB-HepB (2) | 475 | 468 (98.53) | 7 (1.47) |
| 14 Weeks | RV (2) | 401 | 385 (96.00) | 16 (3.99) |
| DTaP-IPV-Hib-HepB (3) | 401 | 392 (97.76) | 9 (2.24) | |
| PCV (2) | 401 | 389 (97.01) | 12 (2.99) | |
| 6 Months | Measles (1) | 341 | 325 (95.31) | 16 (4.69) |
| 9 Months | PCV (3) | 246 | 238 (96.75) | 9 (3.66) |
| 12 Months | Measles (2) | 169 | 153 (90.53) | 16 (9.47) |
| 18 Months | DTaP-IPV-HepB (4) | 73 | 65 (89.04) | 8 (10.69) |
| Variables | All (n = 652), n (%) | Fully (n = 66), n (%) | Incompletely (n = 586), n (%) |
|---|---|---|---|
| CHILDREN CHARACTERISTICS | |||
| Sex of child | |||
| Male | 321, (49.23) | 36, (11.21) | 285, (88.79) |
| Female | 331, (50.77) | 30, (9.06) | 301, (90.94) |
| Age of child (months) | |||
| ≤10 | 473, (75.55) | 2, (0.42) | 471, (99.58) |
| 11–15 | 93, (14.26) | 4, (4.30) | 89, (95.70) |
| 16–20 | 66, (10.12) | 44, (66.67) | 22, (33.33) |
| 21–23 | 19, (2.91) | 16, (84.21) | 3, (15.79) |
| Birth order | |||
| First | 233, (35.74) | 21, (9.01) | 212, (89.83) |
| Second | 228, (34.97) | 18, (7.89) | 210, (92.11) |
| Third | 127, (19.48) | 17, (13.39) | 110, (86.61) |
| ≥Fourth | 64, (9.82) | 10, (15.63) | 54, (84.38) |
| Birth weight | |||
| Average | 413, (63.34) | 44, (10.65) | 369, (89.35) |
| Large | 155, (23.77) | 11, (7.10) | 144, (92.90) |
| Small | 80, (12.27) | 10, (12.5) | 70, (87.5) |
| Reason for visit | |||
| Vaccination | 449, (68.86) | 41, (9.13) | 408, (90.87) |
| Child treatment (sick) | 113, (17.33) | 16, (14.16) | 97, (85.84) |
| GDGCU | 64, (9.82) | 4, (6.25) | 60, (93.75) |
| Other | 26, (3.99) | 5, (19.23) | 21, (80.77) |
| RtHB asked by health worker | |||
| Yes | 637, (97.70) | 66, (10.36) | 571, (89.64) |
| No | 15, (2.30) | 15, (100) | |
| Time of visit | |||
| Morning (8.01 a.m.–12 noon) | 393, (60.28) | 41, (10.43) | 352, (89.57) |
| Afternoon (12.01–5:59 p.m.) | 258, (39.57) | 25, (9.69) | 233, (90.31) |
| MATERNAL OR/CAREGIVER CHARACTERISTICS | |||
| Maternal age | |||
| 16–24 | 181, (27.76) | 14, (7.73) | 167, (92.27) |
| 25–34 | 321, (49.23) | 35, (10.90) | 286, (89.10) |
| 35+ | 150, (23.01) | 17, (11.33) | 133, (88.67) |
| Caregiver sex | |||
| Male | 15, (2.30) | 3, (20) | 12, (80) |
| Female | 630, (96.63) | 63, (10) | 567, (90) |
| Marital Status | |||
| Married | 221, (33.90) | 25, (11.31) | 196, (88.67) |
| Single | 423, (64.88) | 41, (9.69) | 382, (90.31) |
| Divorced | 4, (0.61) | 4, (100) | |
| Widowed | 3, (0.46) | 3, (100) | |
| Other | 1, (0.15) | 1, (100) | |
| Relationship to child | |||
| Mother | 604, (92.64) | 57, (9.44) | 547, (90.56) |
| Father | 14, (2.15) | 3, (21.43) | 11, (78.57) |
| Sibling | 34, (5.21) | 6, (17.65) | 28, (82.35) |
| Maternal Education | |||
| NFE | 2, (0.31) | 1, (50.00) | 1, (50.00) |
| Primary | 31, (4.75) | 2, (6.45) | 29, (93.55) |
| Secondary | 499, (68.87) | 51, (10.22) | 448, (8978) |
| Post-secondary | 120, (18.40) | 12, (10.00) | 108, (90.10) |
| Employment Status | |||
| Yes | 166, (25.46) | 21, (12.65) | 145, (87.35) |
| No | 486, (74.54) | 45, (9.26) | 441, 90.74) |
| Maternal antenatal care | |||
| Yes | 641, (98.31) | 65, (10.02) | 576, (88.75) |
| No | 11, (1.69) | 1, (9.09) | 10, (90.91) |
| Means of transport | |||
| Private | 68, (10.43) | 6, (8.82) | 62, (91.18) |
| Public | 205, (31.44) | 22, (10.73) | 183, (89.27) |
| Walk | 379, (58.13) | 38, (10.03) | 341, (89.97) |
| Immunisation message in last 3 months | |||
| Yes | 402, (61.66) | 48, (11.94) | 354, (88.06) |
| No | 249, (38.19) | 18, (7.23) | 231, (92.77) |
| FACILITY CHARACTERISTICS | |||
| Facility type | |||
| Clinic | 326, (50) | 36, (11.04) | 290, (88.96) |
| CDC | 324, (49.69) | 30, (9.26) | 294, (90.74) |
| Facility Owner | |||
| Province | 250, (38.34) | 19, (7.60) | 231, (92.40) |
| City | 401, (61.50) | 47, (11.72) | 354, (88.28) |
| Number of health workers | |||
| <20 | 148, (22.70) | 19, (12.84) | 129, (87.16) |
| 20 < 50 | 271, (41.56) | 27, (9.96) | 244, (90.04) |
| ≥50 | 230, (35.28) | 20, (8.70) | 210, (91.30) |
| Vaccine stock-out in the past 3 months | |||
| Yes | 141, (21.63) | 14, (9.93) | 127, (90.07) |
| No | 509, (78.07) | 52, (10.22) | 455, (89.39) |
| Vaccine cold-chain challenges in the past 3 months | |||
| Yes | 39, (5.98) | 4, (10.26) | 35, (89.74) |
| No | 612, (93.7) | 62, (10.13) | 550, (89.87) |
| Variables | All (n = 652), n (%) | Measurement of Association | |||
|---|---|---|---|---|---|
| Bivariate Odds Ratio (95% CI) | p-Value | Adjusted Odds Ratio (95% CI) | p-Value | ||
| CHILDREN CHARACTERISTICS | |||||
| Sex of child | |||||
| Male | 321, (49.23) | Ref | Ref | ||
| Female | 331, (50.77) | 1.27 (0.76–2.11) | 0.363 | 1.17 (0.47–2.91) | 0.731 |
| Age of child (months) | |||||
| ≤10 | 473, (72.55) | Ref | Ref | ||
| 11–15 | 93, (14.26) | 0.06 (0.01–0.31) | 0.001 | 0.05 (0.009–0.31) | 0.001 |
| 16–20 | 66, (10.12) | 0.002 (0.0004–0.008) | 0.000 | 0.001 (0.0003–0.0065) | 0.000 |
| 21–23 | 19, (2.91) | 0.0005 (0.0001–0.004) | 0.000 | 0.0003 (0.00004–0.0029) | 0.000 |
| Birth order | |||||
| First | 233, (335.74) | Ref | Ref | ||
| Second | 228, (34.97) | 1.16 (0.60–2.23) | 0.666 | 0.75 (0.25–2.28) | 0.615 |
| Third | 127, (19.48) | 0.64 (0.32–1.26) | 0.200 | 0.68 (0.21–2.23) | 0.522 |
| ≥Fourth | 64, (9.82) | 0.53 (0.24–1.20) | 0.130 | 0.33 (0.07–1.56) | 0.162 |
| Birth Weight | |||||
| Average | 413, (63.34) | Ref | Ref | ||
| Large | 155, (23.77) | 1.56 (0.78–3.11) | 0.205 | 1.83 (0.60–5.56) | 0.288 |
| Small | 80, (12.27) | 0.82 (0.40–1.71) | 0.602 | 0.75 (0.20–2.82) | 0.671 |
| Not specified | 4, (0.61) | 0.48 (0.52–4.36) | 0.512 | 1.35 (0.014–127.99) | 0.897 |
| Reason for visit | |||||
| Vaccination | 449, (68.87) | Ref | Ref | ||
| Non-vaccination | 203, (31.13) | 0.71 (0.42–1.21) | 0.214 | 1.86 (0.68–5.12) | 0.229 |
| Time of visit | |||||
| Morning (8.01 a.m.–12 noon) | 393, (60.28) | Ref | Ref | ||
| Afternoon | 258, (39.57) | 1.09 (0.64–1.83) | 0.759 | 1.69 (0.66–4.30) | 0.272 |
| MATERNAL OR/CAREGIVER CHARACTERISTICS | |||||
| Maternal age | |||||
| 16–24 | 181, (27.76) | Ref | Ref | ||
| 25–34 | 321, (49.23) | 0.69 (0.39–1.31) | 0.253 | 0.76 (0.39–1.48) | 0.424 |
| 35+ | 150, (23.01) | 0.66 (0.31–1.39) | 0.266 | 0.83 (0.37–1.86) | 0.646 |
| Caregiver sex | |||||
| Male | 15, (2.30) | Ref | Ref | ||
| Female | 630, (96.63) | 2.25 (0.61–8.19) | 0.219 | 0.76 (0.015–37.25) | 0.889 |
| Not specified | 7, (1.07) | empty | |||
| Marital Status | |||||
| Married | 221, (33.90) | Ref | Ref | ||
| Single | 423, (64.88) | 1.19 (0.70–2.01) | 0.520 | 1.07 (0.61–1.89) | 0.803 |
| Divorced | 4, (0.61) | empty | |||
| Widowed | 3, (0.46) | empty | |||
| Other | 1, (0.15) | empty | |||
| Relationship to child | |||||
| Mother | 604, (92.64) | Ref | Ref | ||
| Father | 14, (2.15) | 0.38 (0.10–1.41) | 0.149 | 0.35 (0.01–17.74) | 0.602 |
| Sibling | 34, (5.21) | 0.49 (0.19–1.22) | 0.126 | 0.38 (0.14–1.09) | 0.073 |
| Maternal education | |||||
| No Formal Education | 2, (0.31) | Ref | Ref | ||
| Primary | 31, (4.75) | 8.78 (0.54–142.58) | 0.126 | 6.12 (0.36–105.26) | 0.212 |
| Secondary | 499, (76.53) | 14.5 (0.64–328.46) | 0.093 | 10.28 (0.44–241.42) | 0.148 |
| Post-secondary | 120, (18.40) | 9 (0.53–153.31) | 0.129 | 6.57 (0.36–120.32) | 0.205 |
| Employment status | |||||
| Yes | 166, (25.46) | Ref | Ref | ||
| No | 486, (74.54) | 1.42 (0.82–2.46) | 0.213 | 1.31 (0.72–2.38) | 0.379 |
| Maternal antenatal care | |||||
| Yes | 649, (99.54) | Ref | Ref | ||
| No | 11, (1.69) | 0.79 (0.096–6.52) | 0.827 | 1.0 (0.11–9.51) | 1.0 |
| Means of transport | |||||
| Private | 68, (10.43) | Ref | Ref | ||
| Public | 205, (31.44) | 0.80 (0.31–2.08) | 0.654 | 0.73 (0.28–1.92) | 0.521 |
| Walk | 379, (58.13) | 0.87 (0.35–2.14) | 0.759 | 0.71 (0.27–1.83) | 0.478 |
| Immunisation message in last 3 months | |||||
| Yes | 402, (61.66) | Ref | Ref | ||
| No | 250, (38.34) | 1.74 (0.99–3.07) | 0.055 | 1.77 (0.98–3.20) | 0.058 |
| FACILITY CHARACTERISTICS | |||||
| Facility type | |||||
| Clinic | 326, (50) | Ref | Ref | ||
| CDC | 324, (49.69) | 1.22 (0.73–2.03) | 0.452 | 0.76 (0.35–1.65) | 0.481 |
| Not specified | 2, (0.31) | Empty | Empty | ||
| Facility Owners | |||||
| Province | 250, (38.34) | Ref | Ref | ||
| City | 401, (61.50) | 0.62 (0.35–1.08) | 0.093 | 0.53 (0.21–1.34) | 0.179 |
| Number of health workers | |||||
| <20 | 148, (22.70) | Ref | Ref | ||
| 20 < 50 | 271, (41.56) | 1.33 (0.71–2.49) | 0.369 | 1.10 (0.54–2.26) | 0.794 |
| ≥50 | 230, (35.28) | 1.55 (0.80–3.00) | 0.199 | 1.27 (0.46–3.79) | 0.669 |
| Not specified | 3, (0.46) | Empty | Empty | ||
| Vaccine stock-out in the past 3 months | |||||
| Yes | 141, (21.63) | Ref | Ref | ||
| No | 509, (78.07) | 0.97 (0.52–1.80) | 0.920 | 1.13 (0.41–3.09) | 0.811 |
| Not specified | 2, (0.31) | empty | Empty | ||
| Vaccine cold-chain challenges in the past 3 months | |||||
| Yes | 39, (5.98) | Ref | Ref | ||
| No | 612, (93.87) | 0.98 (0.34–2.86) | 0.976 | 0.89 (0.27–2.86) | 0.841 |
| Not specified | 1, (0.15) | empty | Empty | ||
| Immunisation waiting time | |||||
| Less than 30 min | 165, (25.31) | Ref | Ref | ||
| >30 | 327, (50.15) | 0.94 (0.51–1.75) | 0.854 | 0.93 (0.49–1.76) | 0.829 |
| Not specified | 115, (17.64) | 0.92 (0.42–2.03) | 0.840 | 0.81 (0.35–1.84) | 0.614 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ndwandwe, D.; Ndlovu, M.; Mayeye, A.; Luphondo, N.; Muvhulawa, N.; Ntamo, Y.; Dludla, P.V.; Wiysonge, C.S. Trends in Vaccine Completeness in Children Aged 0–23 Months in Cape Town, South Africa. Vaccines 2023, 11, 1782. https://doi.org/10.3390/vaccines11121782
Ndwandwe D, Ndlovu M, Mayeye A, Luphondo N, Muvhulawa N, Ntamo Y, Dludla PV, Wiysonge CS. Trends in Vaccine Completeness in Children Aged 0–23 Months in Cape Town, South Africa. Vaccines. 2023; 11(12):1782. https://doi.org/10.3390/vaccines11121782
Chicago/Turabian StyleNdwandwe, Duduzile, Musawenkosi Ndlovu, Asanda Mayeye, Nomahlubi Luphondo, Ndivhuwo Muvhulawa, Yonela Ntamo, Phiwayinkosi V. Dludla, and Charles S. Wiysonge. 2023. "Trends in Vaccine Completeness in Children Aged 0–23 Months in Cape Town, South Africa" Vaccines 11, no. 12: 1782. https://doi.org/10.3390/vaccines11121782