
A Lesson from a Measles Outbreak among Healthcare Workers in a Single Hospital in South Korea: The Importance of Knowing the Prevalence of Susceptibility

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Case Definition
2.2. Laboratory Testing
2.3. Real-Time RT-PCR for Measles Virus (MeV) Detection
2.4. RNA Extraction, RT-PCR, and Sequencing
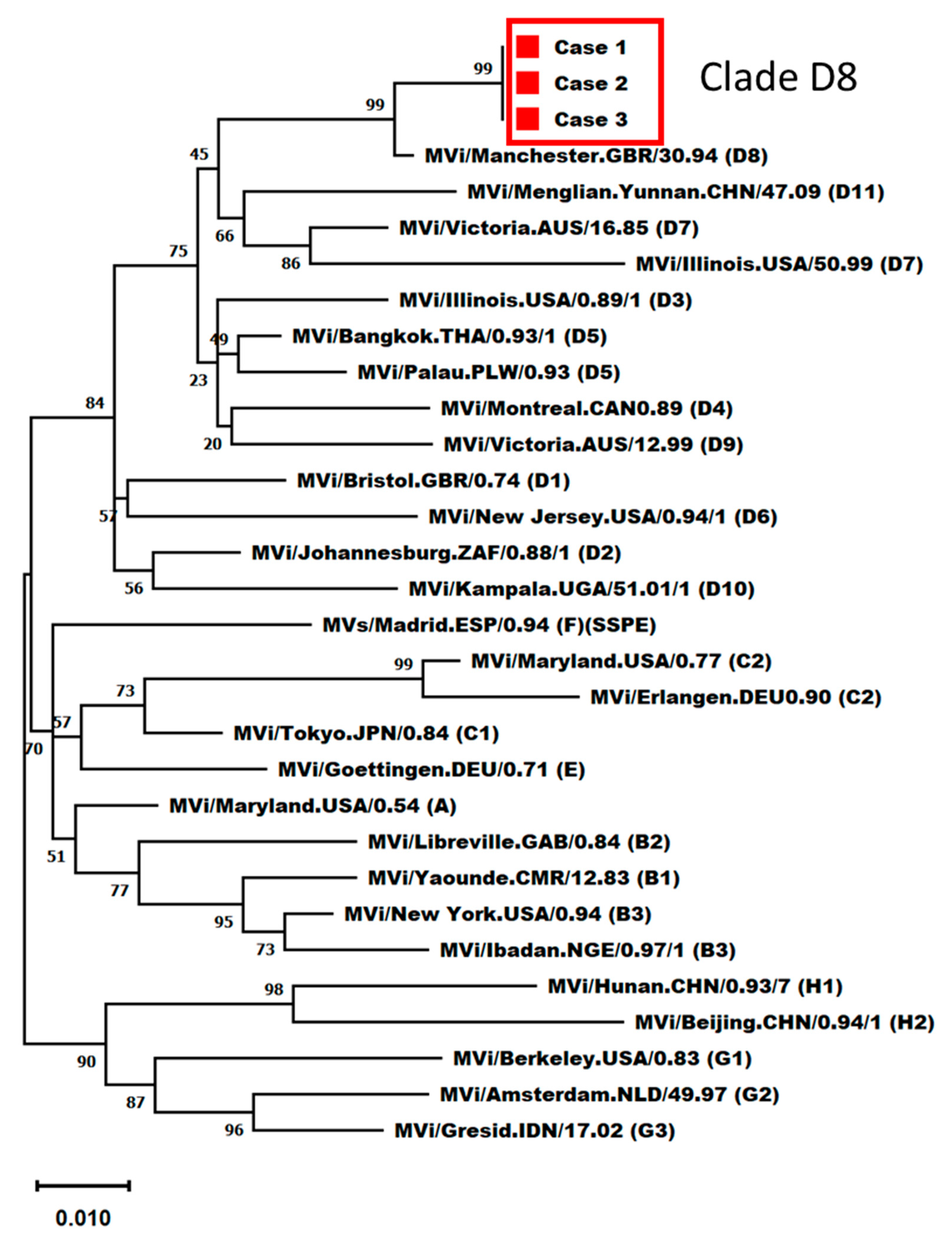
2.5. Phylogenetic Analysis
3. Results
3.1. Outbreak Presentation
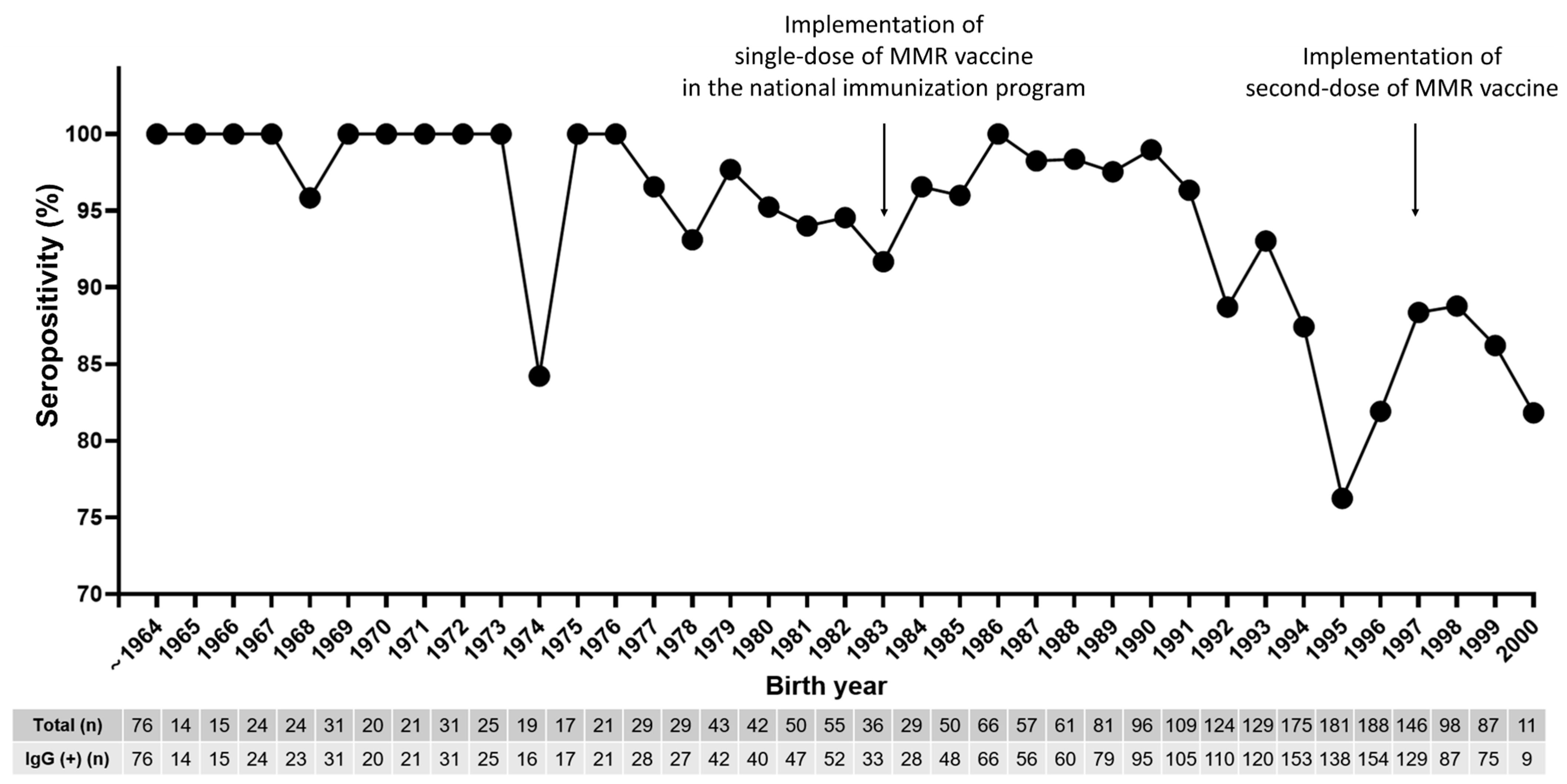
3.2. Seroprevalence of Measles in All HCWs
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gay, N.J. The theory of measles elimination: Implications for the design of elimination strategies. J. Infect. Dis. 2004, 189, S27–S35. [Google Scholar] [CrossRef] [PubMed]
- Choe, Y.J.; Bae, G.R. Current status of measles in the Republic of Korea: An overview of case-based and seroepidemiological surveillance scheme. Korean J. Pediatr. 2012, 55, 455–461. [Google Scholar] [CrossRef]
- Han, S.B.; Park, S.H.; Yi, Y.; Ji, S.K.; Jang, S.H.; Park, M.H.; Lee, J.E.; Jeong, H.S.; Shin, S. Measles seroprevalence among healthcare workers in South Korea during the post-elimination period. Hum. Vaccines Immunother. 2021, 17, 2517–2521. [Google Scholar] [CrossRef] [PubMed]
- Choe, Y.J.; Jee, Y.; Oh, M.D.; Lee, J.K. Measles Elimination Activities in the Western Pacific Region: Experience from the Republic of Korea. J. Korean Med. Sci. 2015, 30, S115–S121. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.U.; Kim, J.W.; Eom, H.E.; Oh, H.-K.; Kim, E.S.; Kang, H.J.; Nam, J.-G.; Kim, K.S.; Kim, S.S.; Lee, C.K.; et al. Resurgence of measles in a country of elimination: Interim assessment and current control measures in the Republic of Korea in early 2014. Int. J. Infect. Dis. 2015, 33, 12–14. [Google Scholar] [CrossRef]
- Choi, W.S.; Sniadack, D.H.; Jee, Y.; Go, U.-Y.; So, J.S.; Cho, H.; Bae, G.-R.; Lee, D.H.; Kim, K.; Yoon, H.S.; et al. Outbreak of measles in the Republic of Korea, 2007: Importance of nosocomial transmission. J. Infect. Dis. 2011, 204, S483–S490. [Google Scholar] [CrossRef]
- Eom, H.; Park, Y.; Kim, J.; Yang, J.-S.; Kang, H.; Kim, K.; Chun, B.C.; Park, O.; Hong, J.I. Occurrence of measles in a country with elimination status: Amplifying measles infection in hospitalized children due to imported virus. PLoS ONE 2018, 13, e0188957. [Google Scholar] [CrossRef]
- Choe, Y.J.; Park, Y.J.; Kim, J.W.; Eom, H.E.; Park, O.; Oh, M.-D.; Lee, J.-K. An Outbreak of Measles in a University in Korea, 2014. J. Korean Med. Sci. 2017, 32, 1876–1878. [Google Scholar] [CrossRef]
- Hummel, K.B.; Erdman, D.D.; Heath, J.; Bellini, W.J. Baculovirus expression of the nucleoprotein gene of measles virus and utility of the recombinant protein in diagnostic enzyme immunoassays. J. Clin. Microbiol. 1992, 30, 2874–2880. [Google Scholar] [CrossRef]
- Erdman, D.D.; Heath, J.L.; Watson, J.C.; Markowitz, L.E.; Bellini, W.J. Immunoglobulin M antibody response to measles virus following primary and secondary vaccination and natural virus infection. J. Med. Virol. 1993, 41, 44–48. [Google Scholar] [CrossRef]
- Ma, C.; Rodewald, L.; Hao, L.; Su, Q.; Zhang, Y.; Wen, N.; Fan, C.; Yang, H.; Luo, H.; Wang, H.; et al. Progress Toward Measles Elimination—China, January 2013–June 2019. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1112–1116. [Google Scholar] [CrossRef] [PubMed]
- Baxi, R.; Mytton, O.T.; Abid, M.; Maduma-Butshe, A.; Iyer, S.; Ephraim, A.; Brown, K.E.; O’Moore, P. Outbreak report: Nosocomial transmission of measles through an unvaccinated healthcare worker-implications for public health. J. Public Health 2014, 36, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Chen, C.; Tang, A.; Wu, B.; Liu, L.; Wu, M.; Wang, H. Epidemiological Investigation and Virus Tracing of a Measles Outbreak in Zhoushan Islands, China, 2019. Front. Public Health 2020, 8, 600196. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Office for the Western Pacific. Measles-Rubella Bulletin. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/331240/Measles-Rubella-Bulletin-2020-Vol-14-No-02.pdf?sequence=2&isAllowed=y (accessed on 19 August 2023).
- Jung, J.; Kim, S.K.; Kwak, S.H.; Hong, M.J.; Kim, S.H. Seroprevalence of Measles in Healthcare Workers in South Korea. Infect. Chemother. 2019, 51, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, K.; Kobayashi, T.; Chowell, G. Transmission potential of modified measles during an outbreak, Japan, March–May 2018. Euro Surveill. 2018, 23, 1800239. [Google Scholar] [CrossRef] [PubMed]
- Davidson, N.; Andrews, R.M.; Riddell, M.; Leydon, J.; Lynch, P.; Team, O.I. A measles outbreak among young adults in Victoria, February 2001. Commun. Dis. Intell. 2002, 26, 273–278. [Google Scholar]
- Maltezou, H.C.; Wicker, S. Measles in health-care settings. Am. J. Infect. Control 2013, 41, 661–663. [Google Scholar] [CrossRef]
- Kang, H.J.; Han, Y.W.; Kim, S.J.; Kim, Y.-J.; Kim, A.-R.; Kim, J.A.; Jung, H.-D.; Eom, H.E.; Park, O.; Kim, S.S. An increasing, potentially measles-susceptible population over time after vaccination in Korea. Vaccine 2017, 35, 4126–4132. [Google Scholar] [CrossRef]
- Kim, S.-K.; Park, H.-Y.; Kim, S.-H. A third dose of measles vaccine is needed in young Korean health care workers. Vaccine 2018, 36, 3888–3889. [Google Scholar] [CrossRef]
- Atrasheuskaya, A.V.; Kulak, M.V.; Neverov, A.A.; Rubin, S.; Ignatyev, G.M. Measles cases in highly vaccinated population of Novosibirsk, Russia, 2000–2005. Vaccine 2008, 26, 2111–2118. [Google Scholar] [CrossRef]
- Seward, J.F.; Orenstein, W.A. Editorial commentary: A rare event: A measles outbreak in a population with high 2-dose measles vaccine coverage. Clin. Infect. Dis. 2012, 55, 403–405. [Google Scholar] [CrossRef] [PubMed]
- Avramovich, E.; Indenbaum, V.; Haber, M.; Amitai, Z.; Tsifanski, E.; Farjun, S.; Sarig, A.; Bracha, A.; Castillo, K.; Markovich, M.P.; et al. Measles Outbreak in a Highly Vaccinated Population—Israel, July–August 2017. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1186–1188. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.Y.; Shao, H.H.; Tsou, M.T. Measles immunity in medical center staff after changes in national and local hospital vaccination policies. BMC Infect. Dis. 2022, 22, 427. [Google Scholar] [CrossRef] [PubMed]
- Gans, H.A.; Arvin, A.M.; Galinus, J.; Logan, L.; DeHovitz, R.; Maldonado, Y. Deficiency of the humoral immune response to measles vaccine in infants immunized at age 6 months. JAMA 1998, 280, 527–532. [Google Scholar] [CrossRef]
- Moss, W.J.; Griffin, D.E. Global measles elimination. Nat. Rev. Microbiol. 2006, 4, 900–908. [Google Scholar] [CrossRef]
- Rosen, J.B.; Rota, J.S.; Hickman, C.J.; Sowers, S.B.; Mercader, S.; Rota, P.A.; Bellini, W.J.; Huang, A.J.; Doll, M.K.; Zucker, J.R.; et al. Outbreak of measles among persons with prior evidence of immunity, New York City, 2011. Clin. Infect. Dis. 2014, 58, 1205–1210. [Google Scholar] [CrossRef]
- Hahné, S.J.; Nic Lochlainn, L.M.; van Burgel, N.D.; Kerkhof, J.; Sane, J.; Yap, K.B.; van Binnendijk, R.S. Measles outbreak among previously immunized healthcare workers, The Netherlands, 2014. J. Infect. Dis. 2016, 214, 1980–1986. [Google Scholar] [CrossRef]
- Shefer, A.; Atkinson, W.; Friedman, C.; Griffin, D.E. Immunization of health-care personnel: Recommendations of the Advisory Committee on Immunization Practices (ACIP). Morb. Mortal. Wkly. Rep. Recomm. Rep. 2011, 60, 1–45. [Google Scholar]
- Kim, S.S.; Han, H.W.; Go, U.; Chung, H.W. Sero-epidemiology of measles and mumps in Korea: Impact of the catch-up campaign on measles immunity. Vaccine 2004, 23, 290–297. [Google Scholar] [CrossRef]
- Chun, J.Y.; Park, W.B.; Kim, N.J.; Choi, E.H.; Funk, S.; Oh, M.D. Estimating contact-adjusted immunity levels against measles in South Korea and prospects for maintaining elimination status. Vaccine 2020, 38, 107–111. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control and Prevention. Guidelines for Adult Immunization, 2nd ed.; Korea Centers for Disease Control and Prevention: Cheongju, Republic of Korea, 2012.
- Choih, J.; Shimy, S.; Jeongs, Y. Susceptibility of health care workers to measles, rubella, and varicella at a university hospital. Infect. Chemother. 2003, 1, 401–406. [Google Scholar]
- Kang, J.-H.; Park, Y.S.; Park, S.Y.; Kim, S.B.; Ko, K.-P.; Seo, Y.-H. Varicella seroprevalence among health care workers in Korea: Validity of self-reported history and cost-effectiveness of prevaccination screening. Am. J. Infect. Control. 2014, 42, 885–887. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Liu, J.; Xing, F.; Ye, H.; Dai, G.; Liu, M.; Lo, S.K.-F.; Lau, R.W.-T.; Chiu, K.H.-Y.; Chan, J.F.-W.; et al. Nosocomial transmission of chickenpox and varicella zoster virus seroprevalence rate amongst healthcare workers in a teaching hospital in China. BMC Infect. Dis. 2019, 19, 582. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 2018 * | 2019 * | 2020 * | 2021 * | 2022 * | |
|---|---|---|---|---|---|
| No. of samples (n) | 972 | 518 | 288 | 299 | 233 |
| Seropositive (%) | 926 (95.3) | 450 (86.9) | 257 (89.2) | 271 (90.6) | 211 (90.6) |
| Seronegative (%) | 46 (4.7) | 51 (9.8) | 25 (8.7) | 23 (7.7) | 19 (8.2) |
| Equivocal (%) | 0 (0) | 17 (3.3) | 6 (2.1) | 5 (1.7) | 3 (1.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.; Chung, J.-W.; Chang, Y.J.; Lim, E.J.; Moon, S.H.; Do, H.H.; Lee, J.H.; Cho, S.-M.; Kwon, B.S.; Chung, Y.-S.; et al. A Lesson from a Measles Outbreak among Healthcare Workers in a Single Hospital in South Korea: The Importance of Knowing the Prevalence of Susceptibility. Vaccines 2023, 11, 1505. https://doi.org/10.3390/vaccines11091505
Choi S, Chung J-W, Chang YJ, Lim EJ, Moon SH, Do HH, Lee JH, Cho S-M, Kwon BS, Chung Y-S, et al. A Lesson from a Measles Outbreak among Healthcare Workers in a Single Hospital in South Korea: The Importance of Knowing the Prevalence of Susceptibility. Vaccines. 2023; 11(9):1505. https://doi.org/10.3390/vaccines11091505
Chicago/Turabian StyleChoi, Sungim, Jae-Woo Chung, Yun Jung Chang, Eun Jung Lim, Sun Hee Moon, Han Ho Do, Jeong Hun Lee, Sung-Min Cho, Bum Sun Kwon, Yoon-Seok Chung, and et al. 2023. "A Lesson from a Measles Outbreak among Healthcare Workers in a Single Hospital in South Korea: The Importance of Knowing the Prevalence of Susceptibility" Vaccines 11, no. 9: 1505. https://doi.org/10.3390/vaccines11091505