
Interventions to Improve Knowledge, Attitudes, and Uptake of Recommended Vaccines during Pregnancy and Postpartum: A Scoping Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
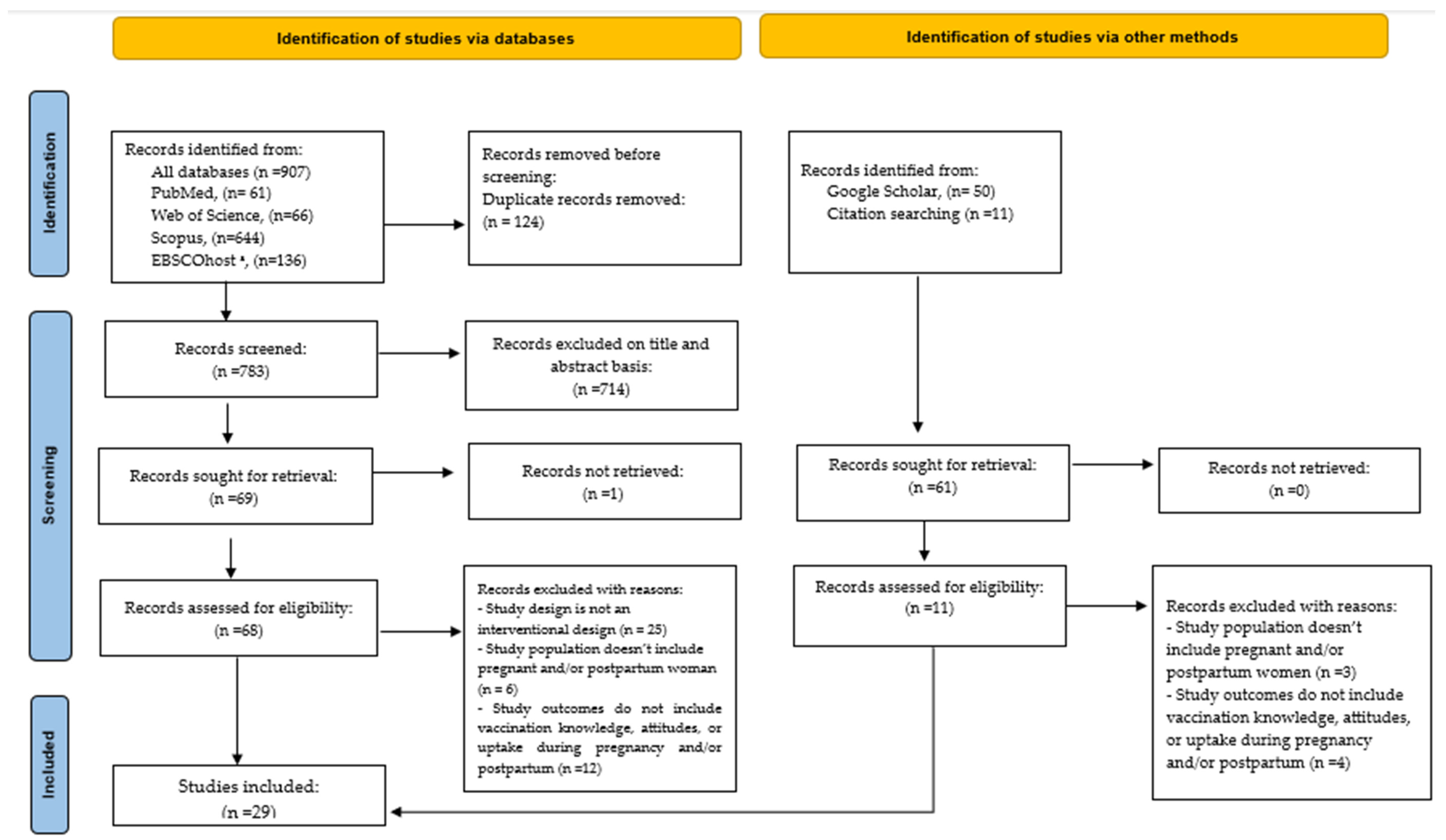
2.1. Search Strategy
2.2. Eligibility Criteria and Study Selection
2.3. Data Extraction and Analysis
3. Results
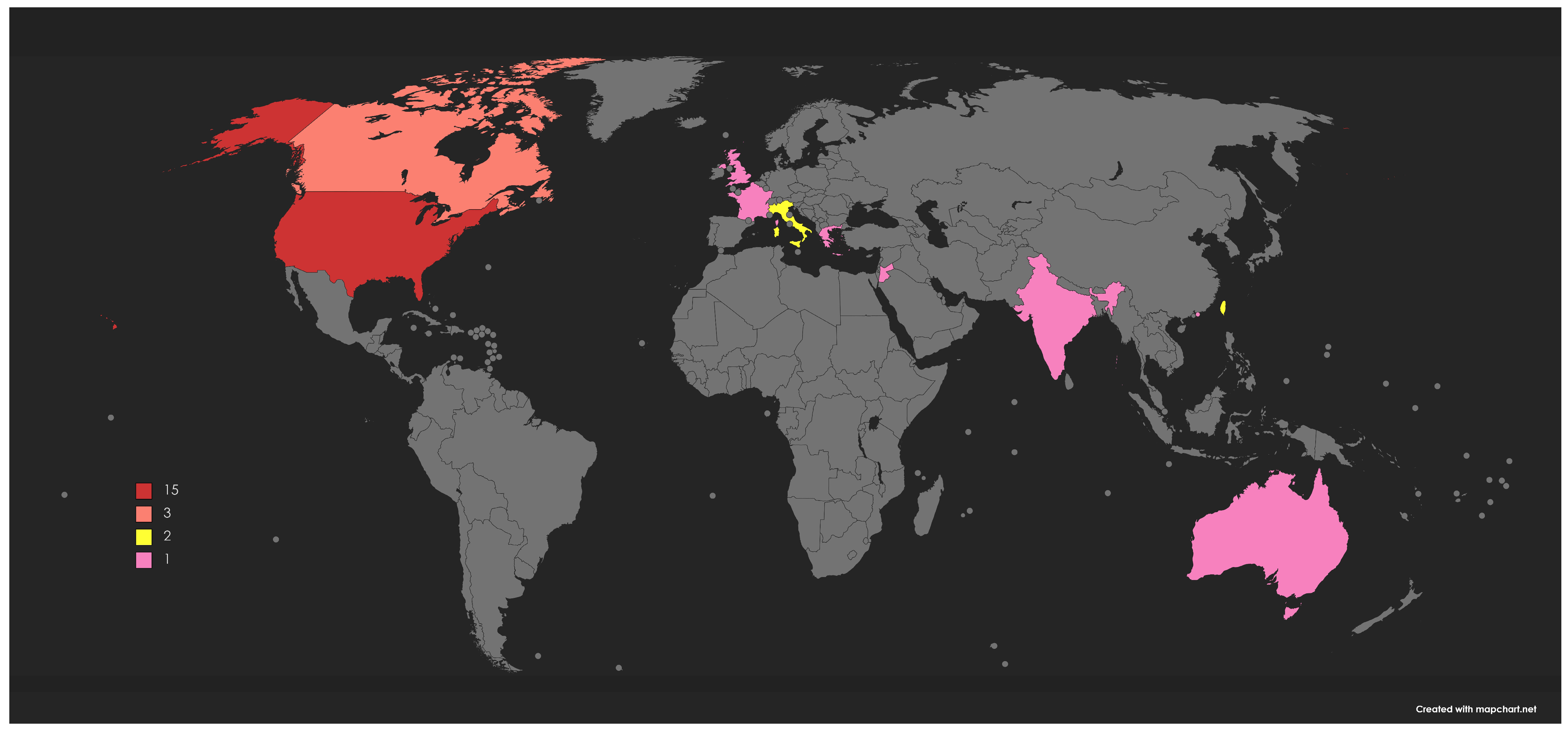
3.1. Characteristics of the Included Studies
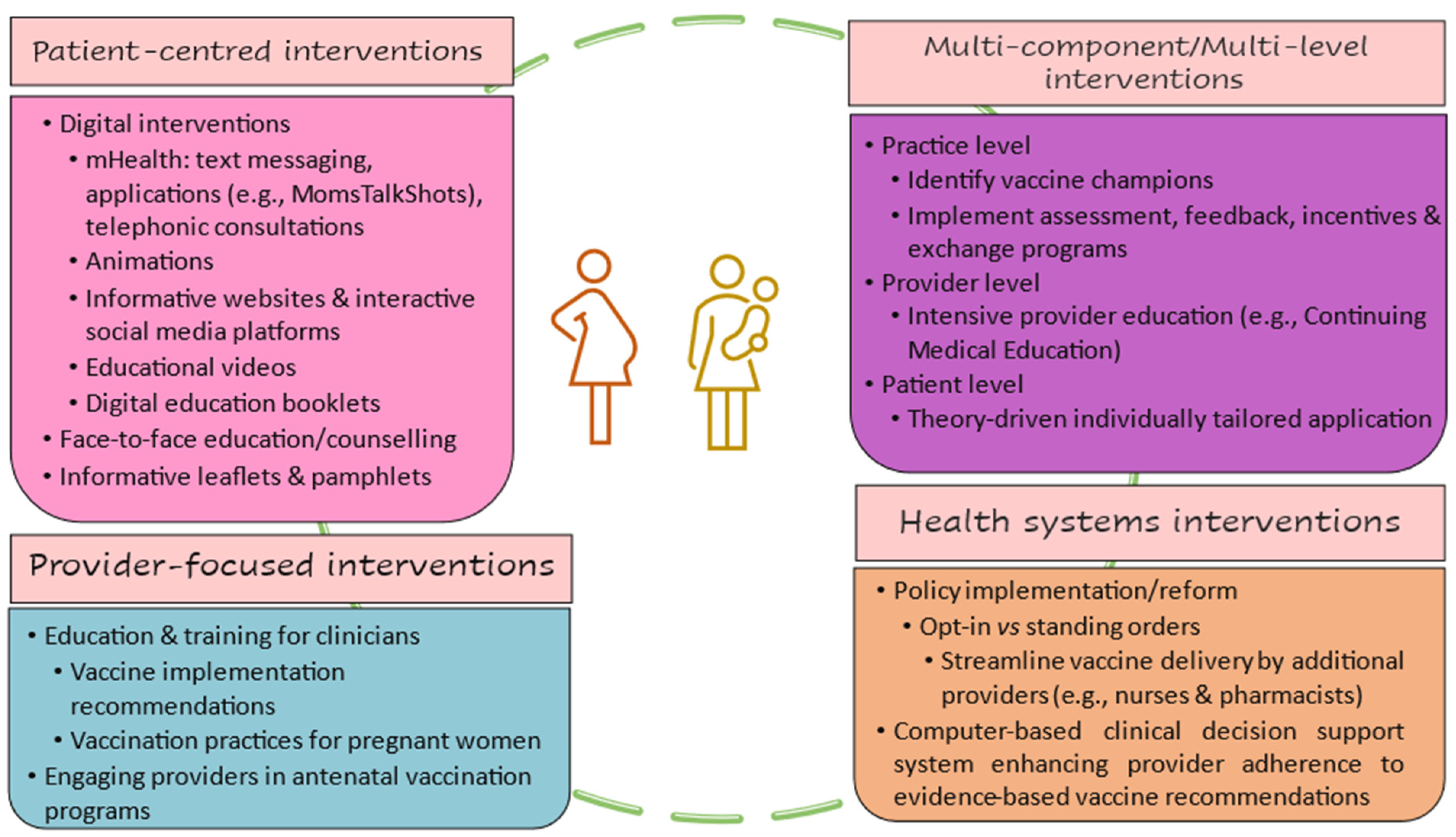
3.2. Main Findings from the Included Interventions Studies Aimed at Improving Knowledge, Acceptance, and Uptake of Maternal Vaccines
3.2.1. Patient-Centered Interventions
3.2.2. Provider-Focused Interventions
3.2.3. Health System Interventions
3.2.4. Multicomponent and Multilevel Interventions
4. Discussion
Limitations and Further Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vojtek, I.; Dieussaert, I.; Doherty, T.M.; Franck, V.; Hanssens, L.; Miller, J.; Bekkat-Berkani, R.; Kandeil, W.; Prado-Cohrs, D.; Vyse, A. Maternal immunization: Where are we now and how to move forward? Ann. Med. 2018, 50, 193–208. [Google Scholar] [CrossRef]
- Sakala, I.G.; Honda-Okubo, Y.; Fung, J.; Petrovsky, N. Influenza immunization during pregnancy: Benefits for mother and infant. Hum. Vaccines Immunother. 2016, 12, 3065–3071. [Google Scholar] [CrossRef]
- Kourtis, A.P.; Read, J.S.; Jamieson, D.J. Pregnancy and Infection. N. Engl. J. Med. 2014, 370, 2211–2218. [Google Scholar] [CrossRef]
- Moraga, P.; GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar]
- Vaccinate Pregnant Patients to Protect Against Pertussis 2022. Available online: https://www.cdc.gov/pertussis/pregnant/hcp/pregnant-patients.html (accessed on 10 April 2023).
- Creanga, A.A.; Johnson, T.F.; Graitcer, S.B.; Hartman, L.K.; Al-Samarrai, T.; Schwarz, A.G.; Chu, S.Y.; Sackoff, J.E.; Jamieson, D.J.; Fine, A.D.; et al. The severity of 2009 pandemic influenza A (H1N1) virus infection in pregnant women. Obstet. Gynecol. 2010, 115, 717–726. [Google Scholar] [CrossRef]
- Siston, A.M.; Rasmussen, S.A.; Honein, M.A.; Fry, A.M.; Seib, K.; Callaghan, W.M.; Louie, J.; Doyle, T.J.; Crockett, M.; Lynfield, R.; et al. Pandemic 2009 influenza A(H1N1) virus illness among pregnant women in the United States. JAMA 2010, 303, 1517–1525. [Google Scholar] [CrossRef]
- Wang, X.; Li, Y.; O’Brien, K.L.; Madhi, S.A.; Widdowson, M.A.; Byass, P.; Omer, S.B.; Abbas, Q.; Ali, A.; Amu, A.; et al. Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: A systematic review and modelling study. Lancet Glob. Health 2020, 8, e497–e510. [Google Scholar] [CrossRef]
- Löwensteyn, Y.N.; Nair, H.; Nunes, M.C.; van Roessel, I.; Vernooij, F.S.; Willemsen, J.; Bont, L.J.; Mazur, N.I.; Thorburn, K.; Chawana, R.; et al. Estimated impact of maternal vaccination on global paediatric influenza-related in-hospital mortality: A retrospective case series. EClinicalMedicine 2021, 37, 100945. [Google Scholar] [CrossRef]
- De Larissa, B.; Greet, H.; Karolien, P.; Walter, D.; Pierre Van, D.; Kirsten, M. Influence of the COVID-19 pandemic and social media on the behaviour of pregnant and lactating women towards vaccination: A scoping review. BMJ Open 2023, 13, e066367. [Google Scholar]
- Vaccines during and after Pregnancy 2021. Available online: https://www.cdc.gov/vaccines/pregnancy/vacc-during-after.html (accessed on 11 April 2023).
- Hui, Z.; Nayagam, S.; Chan, P.; Fuzhen, W.; Thursz, M.; Zundong, Y.; Ning, M.; Xiaojin, S.; Cui, F.; Guomin, Z.; et al. Progress towards elimination of mother-to-child transmission of hepatitis b virus infection in China: A modelling analysis. Bull. World Health Organ. 2021, 99, 10–18. [Google Scholar] [CrossRef]
- World Health Organization. Pertussis vaccines: WHO position paper—August 2015. Note De Synthèse: Position De L’oms Concern. Les Vaccins Anticoquelucheux—Août 2015. Wkly. Epidemiol. Rec. 2015, 90, 433–458. [Google Scholar]
- World Health Organization. Vaccines against influenza WHO position paper–November 2012. Wkly. Epidemiol. Rec. 2012, 87, 461–476. [Google Scholar]
- Questions and Answers: COVID-19 Vaccines and Pregnancy 2022. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-FAQ-Pregnancy-Vaccines-2022.1 (accessed on 11 April 2023).
- Hubka, T.A.; Wisner, K.P. Vaccinations recommended during pregnancy and breastfeeding. J. Am. Osteopath Assoc. 2011, 111 Suppl. 6), S23–S30. [Google Scholar]
- World Health Organization. Protecting All against Tetanus. Available online: https://www.who.int/publications/i/item/protecting-all-against-tetanus (accessed on 8 August 2023).
- Kamath, G.D.; Kukreja, S.; Mukherjee, P.; Kolhapure, S.; Sathyanarayanan, S. Maternal immunization: Trends in South and Southeast Asian countries. J. Matern. Fetal Neonatal Med. 2022, 35, 8372–8381. [Google Scholar] [CrossRef] [PubMed]
- Baïssas, T.; Boisnard, F.; Cuesta Esteve, I.; Garcia Sanchez, M.; Jones, C.E.; Rigoine de Fougerolles, T.; Tan, L.; Vitoux, O.; Klein, C. Vaccination in pregnancy against pertussis and seasonal influenza: Key learnings and components from high-performing vaccine programmes in three countries: The United Kingdom, the United States and Spain. BMC Public Health 2021, 21, 2182. [Google Scholar] [CrossRef]
- Corbeau, M.; Mulliez, A.; Chenaf, C.; Eschalier, B.; Lesens, O.; Vorilhon, P. Trends of influenza vaccination coverage in pregnant women: A ten-year analysis from a French healthcare database. Sci. Rep. 2022, 12, 7153. [Google Scholar] [CrossRef]
- Davies, B.; Olivier, J.; Amponsah-Dacosta, E. Health Systems Determinants of Delivery and Uptake of Maternal Vaccines in Low- and Middle-Income Countries: A Qualitative Systematic Review. Vaccines 2023, 11, 869. [Google Scholar] [CrossRef]
- Hoque, M.; Buckus, S.; Hoque, M.; Hoque, M.; Van Hal, G. COVID-19 Vaccine Acceptability Among Pregnant Women at a Primary Health Care Facility in Durban, South Africa. Eur. J. Med. Health Sci. 2020, 2, 493. [Google Scholar] [CrossRef]
- Oduwole, E.O.; Pienaar, E.D.; Mahomed, H.; Wiysonge, C.S. Overview of Tools and Measures Investigating Vaccine Hesitancy in a Ten Year Period: A Scoping Review. Vaccines 2022, 10, 1198. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Frew, P.M.; Kriss, J.L.; Chamberlain, A.T.; Malik, F.; Chung, Y.; Cortés, M.; Omer, S.B. A randomized trial of maternal influenza immunization decision-making: A test of persuasive messaging models. Hum. Vaccines Immunother. 2016, 12, 1989–1996. [Google Scholar] [CrossRef]
- Wong, V.W.Y.; Fong, D.Y.T.; Lok, K.Y.W.; Wong, J.Y.H.; Sing, C.; Choi, A.Y.-Y.; Yuen, C.Y.S.; Tarrant, M. Brief education to promote maternal influenza vaccine uptake: A randomized controlled trial. Vaccine 2016, 34, 5243–5250. [Google Scholar] [CrossRef]
- O’Leary, S.T.; Narwaney, K.J.; Wagner, N.M.; Kraus, C.R.; Omer, S.B.; Glanz, J.M. Efficacy of a Web-Based Intervention to Increase Uptake of Maternal Vaccines: An RCT. Am. J. Prev. Med. 2019, 57, e125–e133. [Google Scholar] [CrossRef]
- Goodman, K.; Mossad, S.B.; Taksler, G.B.; Emery, J.; Schramm, S.; Rothberg, M.B. Impact of Video Education on Influenza Vaccination in Pregnancy. J. Reprod. Med. 2015, 60, 471–479. [Google Scholar] [PubMed]
- Moniz, M.H.; Hasley, S.; Meyn, L.A.; Beigi, R.H. Improving influenza vaccination rates in pregnancy through text messaging: A randomized controlled trial. Obstet. Gynecol. 2013, 121, 734–740. [Google Scholar] [CrossRef]
- Stockwell, M.S.; Westhoff, C.; Kharbanda, E.O.; Vargas, C.Y.; Camargo, S.; Vawdrey, D.K.; Castaño, P.M. Influenza Vaccine Text Message Reminders for Urban, Low-Income Pregnant Women: A Randomized Controlled Trial. Am. J. Public Health 2014, 104, e7–e12. [Google Scholar] [CrossRef] [PubMed]
- Meharry, P.M.; Cusson, R.M.; Stiller, R.; Vázquez, M. Maternal influenza vaccination: Evaluation of a patient-centered pamphlet designed to increase uptake in pregnancy. Matern. Child Health J. 2014, 18, 1205–1214. [Google Scholar] [CrossRef]
- Salmon, D.A.; Limaye, R.J.; Dudley, M.Z.; Oloko, O.K.; Church-Balin, C.; Ellingson, M.K.; Spina, C.I.; Brewer, S.E.; Orenstein, W.A.; Halsey, N.A.; et al. MomsTalkShots: An individually tailored educational application for maternal and infant vaccines. Vaccine 2019, 37, 6478–6485. [Google Scholar] [CrossRef]
- Frew, P.M.; Saint-Victor, D.S.; Owens, L.E.; Omer, S.B. Socioecological and message framing factors influencing maternal influenza immunization among minority women. Vaccine 2014, 32, 1736–1744. [Google Scholar] [CrossRef] [PubMed]
- Yudin, M.H.; Mistry, N.; De Souza, L.R.; Besel, K.; Patel, V.; Mejia, S.B.; Bernick, R.; Ryan, V.; Urquia, M.; Beigi, R.H.; et al. Text messages for influenza vaccination among pregnant women: A randomized controlled trial. Vaccine 2017, 35, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.W.; Tsai, S.M.; Lin, P.C.; Chou, F.H. Efficacy of a Smartphone Application to Promote Maternal Influenza Vaccination: A Randomized Controlled Trial. Vaccines 2022, 10, 369. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Mazzucco, W.; Bonaccorso, N.; Cimino, L.; Conforto, A.; Sciortino, M.; Catalano, G.; D’anna, M.R.; Maiorana, A.; Venezia, R.; et al. Educational interventions on pregnancy vaccinations during childbirth classes improves vaccine coverages among pregnant women in Palermo’s province. Vaccines 2021, 9, 1455. [Google Scholar] [CrossRef] [PubMed]
- Parsons, J.; Grimley, C.; Newby, K. Effectiveness of a Digital Intervention in Increasing Flu Vaccination–Related Risk Appraisal, Intention to Vaccinate and Vaccination Behaviour among Pregnant Women. Health Educ. Behav. 2022, 49, 1033–1041. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Pelopidas Koutroumanis, P.; Kritikopoulou, C.; Theodoridou, K.; Katerelos, P.; Tsiaousi, I.; Rodolakis, A.; Loutradis, D. Knowledge about influenza and adherence to the recommendations for influenza vaccination of pregnant women after an educational intervention in Greece. Hum. Vaccines Immunother. 2019, 15, 1070–1074. [Google Scholar] [CrossRef]
- Bruno, S.; Carducci, B.; Quaranta, G.; Beccia, V.; Di Pilla, A.; La Milia, D.I.; Di Pumpo, M.; Carini, E.; Masini, L.; Tamburrini, E.; et al. Enhancement of vaccination attitude and flu vaccination coverage among pregnant women attending birthing preparation course. Vaccines 2021, 9, 183. [Google Scholar] [CrossRef]
- Hebballi, N.B.; Parker, T.; Garcia, E.I.; Ferguson, D.M.; Lesser, S.; Tsao, K.; Broussard, M.; Wootton, S.H. Pertussis and influenza immunization: Perceived attitude and decision of postpartum patients. BMC Pregnancy Childbirth 2022, 22, 975. [Google Scholar] [CrossRef]
- Momani, A.; Hamaideh, S.H.; Masadeh, A.B.; Alhalaiqa, F.; Bani Mostafa, F.N.; Weld Ali, H.I.; Masa’Deh, R. The effect of COVID-19 vaccine tele-educational program on vaccine hesitancy and receiving the vaccine among women planning for pregnancy, pregnant or breastfeeding mothers. PLoS ONE 2023, 18, e0282627. [Google Scholar] [CrossRef]
- Hallas, D.; Altman, S.; Mandel, E.; Fletcher, J. Vaccine hesitancy in prenatal women and mothers of newborns: Results of an interventional study. Nurse Pract. 2023, 48, 36–47. [Google Scholar] [CrossRef]
- Hayles, E.H.; Cooper, S.C.; Wood, N.; Sinn, J.; Skinner, S.R. What predicts postpartum pertussis booster vaccination? A controlled intervention trial. Vaccine 2015, 33, 228–236. [Google Scholar] [CrossRef]
- Giduthuri, J.G.; Purohit, V.; Maire, N.; Kudale, A.; Utzinger, J.; Schindler, C.; Weiss, M.G. Influenza vaccination of pregnant women: Engaging clinicians to reduce missed opportunities for vaccination. Vaccine 2019, 37, 1910–1917. [Google Scholar] [CrossRef] [PubMed]
- Bonneau, C.; Seror, J.; Seror, E.; Hervé, F.L.; Rouzier, R. Efficacy of systematic information and prescription of vaccine to implement the recommendations to prevent post-partum pertussis: A limited impact. Gynecol. Obstet. Fertil. 2010, 38, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.; Mink, C.; Kim, M.; Naylor, S.; Zangwill, K.M.; Allred, N.J. Effectiveness of hospital-based postpartum procedures on pertussis vaccination among postpartum women. Am. J. Obstet. Gynecol. 2014, 210, 237.e1–237.e6. [Google Scholar] [CrossRef] [PubMed]
- Trick, W.E.; Linn, E.S.; Jones, Z.; Caquelin, C.; Kee, R.; Morita, J.Y. Using computer decision support to increase maternal postpartum tetanus, diphtheria, and acellular pertussis vaccination. Obstet. Gynecol. 2010, 116, 51–57. [Google Scholar] [CrossRef]
- Mazzoni, S.E.; Brewer, S.E.; Pyrzanowski, J.L.; Durfee, M.J.; Dickinson, L.M.; Barnard, J.G.; Dempsey, A.F.; O’Leary, S.T. Effect of a multi-modal intervention on immunization rates in obstetrics and gynecology clinics. Am. J. Obstet. Gynecol. 2016, 214, 617.e1–617.e7. [Google Scholar] [CrossRef]
- Li, Y.; Brousseau, N.; Guay, M.; Dubé, È.; Laghdir, Z.; Boucoiran, I.; Tapiéro, B.; Quach, C. Coverage for pertussis vaccination during pregnancy with 4 models of vaccine delivery: A quasiexperimental, multicentre observational study. CMAJ Open 2022, 10, E56–E63. [Google Scholar] [CrossRef]
- Cheng, P.J.; Huang, S.Y.; Su, S.Y.; Peng, H.H.; Chang, C.L. Increasing postpartum rate of vaccination with tetanus, diphtheria, and acellular pertussis vaccine by incorporating pertussis cocooning information into prenatal education for group B streptococcus prevention. Vaccine 2015, 33, 7225–7231. [Google Scholar] [CrossRef]
- O’Leary, S.T.; Pyrzanowski, J.; Brewer, S.E.; Sevick, C.; Miriam Dickinson, L.; Dempsey, A.F. Effectiveness of a multimodal intervention to increase vaccination in obstetrics/gynecology settings. Vaccine 2019, 37, 3409–3418. [Google Scholar] [CrossRef]
- Chamberlain, A.T.; Seib, K.; Ault, K.A.; Rosenberg, E.S.; Frew, P.M.; Cortés, M.; Whitney, E.A.S.; Berkelman, R.L.; Orenstein, W.A.; Omer, S.B. Improving influenza and Tdap vaccination during pregnancy: A cluster-randomized trial of a multi-component antenatal vaccine promotion package in late influenza season. Vaccine 2015, 33, 3571–3579. [Google Scholar] [CrossRef]
- Omer, S.B.; O’leary, S.T.; Bednarczyk, R.A.; Ellingson, M.K.; Spina, C.I.; Dudley, M.Z.; Chamberlain, A.T.; Limaye, R.J.; Brewer, S.E.; Frew, P.M.; et al. Multi-tiered intervention to increase maternal immunization coverage: A randomized, controlled trial. Vaccine 2022, 40, 4955–4963. [Google Scholar] [CrossRef] [PubMed]
- LeBaron, C.W.; Mercer, J.T.; Massoudi, M.S.; Dini, E.; Stevenson, J.; Fischer, W.M.; Loy, H.; Quick, L.S.; Warming, J.C.; Tormey, P.; et al. Changes in clinic vaccination coverage after institution of measurement and feedback in 4 states and 2 cities. Arch. Pediatr. Adolesc. Med. 1999, 153, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Lok, K.Y.; Tarrant, M. Interventions to increase the uptake of seasonal influenza vaccination among pregnant women: A systematic review. Vaccine 2016, 34, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Brillo, E.; Tosto, V.; Buonomo, E. Interventions to increase uptake of influenza vaccination in pregnancy: A systematic review and meta-analysis. Int. J. Gynaecol. Obstet. 2023, 162, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Parsons, J.; Griffiths, S.E.; Thomas, N.; Atherton, H. How effective are digital interventions in increasing flu vaccination among pregnant women? A systematic review and meta-analysis. J. Public Health 2022, 44, 863–876. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, H.; McMillan, M.; Roberts, C.T.; Marshall, H.S. A systematic review of interventions to improve uptake of pertussis vaccination in pregnancy. PLoS ONE 2019, 14, e0214538. [Google Scholar] [CrossRef]
- Heyman, K.P.; Worley, M.J.; Frey, M.K.; Kessler, R.T.; Bodurka, D.C.; Slomovitz, B.M. Willingness of pregnant women to vaccinate themselves and their newborns with the HPV vaccine. Vaccine 2011, 29, 4618–4622. [Google Scholar] [CrossRef]
- Etti, M.; Calvert, A.; Galiza, E.; Lim, S.; Khalil, A.; Le Doare, K.; Heath, P.T. Maternal vaccination: A review of current evidence and recommendations. Am. J. Obstet. Gynecol. 2022, 226, 459–474. [Google Scholar] [CrossRef]
- Giles, M.L.; Khai, K.; Krishnaswamy, S.; Bellamy, K.; Angliss, M.; Smith, C.; Fay, O.; Paddle, P.; Vollenhoven, B. An evaluation of strategies to achieve greater than 90% coverage of maternal influenza and pertussis vaccines including an economic evaluation. BMC Pregnancy Childbirth 2021, 21, 771. [Google Scholar] [CrossRef]
- Larson Williams, A.; Mitrovich, R.; Mwananyanda, L.; Gill, C. Maternal vaccine knowledge in low- and middle-income countries-and why it matters. Hum. Vaccines Immunother. 2019, 15, 283–286. [Google Scholar] [CrossRef]
- Maertens, K.; Orije, M.R.P.; Van Damme, P.; Leuridan, E. Vaccination during pregnancy: Current and possible future recommendations. Eur. J. Pediatr. 2020, 179, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Baral, R.; Higgins, D.; Regan, K.; Pecenka, C. Impact and cost-effectiveness of potential interventions against infant respiratory syncytial virus (RSV) in 131 low-income and middle-income countries using a static cohort model. BMJ Open 2021, 11, e046563. [Google Scholar] [CrossRef] [PubMed]
- Munoz, F.M.; Ferrieri, P. Group B Streptococcus vaccination in pregnancy: Moving toward a global maternal immunization program. Vaccine 2013, 31 (Suppl. 4), D46–D51. [Google Scholar] [CrossRef] [PubMed]
- Russell, L.B.; Kim, S.Y.; Cosgriff, B.; Pentakota, S.R.; Schrag, S.J.; Sobanjo-ter Meulen, A.; Verani, J.R.; Sinha, A. Cost-effectiveness of maternal GBS immunization in low-income sub-Saharan Africa. Vaccine 2017, 35, 6905–6914. [Google Scholar] [CrossRef]
- Ben Natan, M.; El Kravchenko, B.; Sakashidlo, K.; Mor, S. What drives pregnant women’s decisions to accept the pertussis vaccine? Appl. Nurs. Res. 2017, 38, 60–63. [Google Scholar] [CrossRef]
- Arriola, C.S.; Suntarattiwong, P.; Dawood, F.S.; Soto, G.; Das, P.; Hunt, D.R.; Sinthuwattanawibool, C.; Kurhe, K.; Thompson, M.G.; Wesley, M.G.; et al. What do pregnant women think about influenza disease and vaccination practices in selected countries. Hum. Vaccines Immunother. 2021, 17, 2176–2184. [Google Scholar] [CrossRef]
- Fernandez, M.E.; Ruiter, R.A.C.; Markham, C.M.; Kok, G. Intervention Mapping: Theory- and Evidence-Based Health Promotion Program Planning: Perspective and Examples. Front. Public Health 2019, 7, 209. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author (Publication Year) | Country | Vaccine(s) | Population Group | Study Design | Category of the Intervention | Description of the Intervention | Main Results |
|---|---|---|---|---|---|---|---|
| Paula M. Frewa et al. (2016) [27] | United States | Influenza | Pregnant women | Randomized controlled trial (RCT) | Patient-centered intervention | Two forms of targeted persuasive messaging models: (i) affective messaging intervention (“Pregnant Pause” video) and (ii) cognitive messaging intervention (“Vaccines for a Healthy Pregnancy” video) in comparison to generic influenza vaccine information statements (VIS) | No effect after a single exposure to either affective messaging or cognitive messaging interventions on the vaccine uptake |
| Valerie Wing Yu Wong et al. (2016) [28] | Hong Kong | Influenza | Pregnant women | RCT | Patient-centered intervention | Brief, one-to-one education session on influenza vaccination uptake during pregnancy and the proportion of participants seeking out influenza vaccination | Uptake was higher among participants who received brief education compared to the standard care group. More participants in the education group-initiated discussion about influenza vaccination with their healthcare provider, but the difference was not statistically significant. |
| Sean T. O’Leary, (2019) [29] | United States | Tetanus–diphtheria–acellular pertussis (Tdap) and influenza | Pregnant women | RCT | Patient-centered intervention | Women were randomly assigned to one of three arms: “website with vaccine information and interactive social media components”, “website with vaccine information only”, or usual care. | Participants in both the first and second arms had higher vaccine uptake than the usual care group. There were no significant differences in vaccine uptake between study groups for the Tdap vaccine. |
| Kenneth Goodman et al. (2015) [30] | United States | Influenza | Pregnant women | RCT | Patient-centered intervention | Pre- and post-educational video on health beliefs was assessed, and unvaccinated women were subsequently interviewed by phone. Those in the control group viewed another video addressing handwashing hygiene. | The educational video positively influenced vaccination health beliefs without impacting vaccination uptake rates. The physician’s recommendation was strongly associated with the participant’s decision to vaccinate. |
| Michelle H. Moniz et al. (2013) [31] | Canada | Influenza | Pregnant women | RCT | Patient-centered intervention | Participants received 12 weekly text messages regarding general preventive health information in pregnancy and the importance of influenza vaccination during pregnancy. | Text messaging intervention was not effective at increasing influenza vaccination uptake rates among a low-income, urban, ambulatory pregnant population. |
| Melissa S. Stockwell et al. (2014) [32] | United States | Influenza | Pregnant women | RCT | Patient-centered intervention | Participants in the intervention group received five weekly text messages regarding influenza vaccination and two text message appointment reminders. | Text messaging was associated with increased influenza uptake, in a low-income obstetric population, mainly those who received the intervention early in their third trimester. |
| Pamela M. Meharry et al. (2013) [33] | United States | Influenza | Pregnant women | RCT | Patient-centered intervention | A pamphlet was tailored to pregnant women entitled “Influenza in Pregnancy”. | The pamphlet significantly increased the pregnant women’s perceptions of the safety and benefits of vaccination against influenza during pregnancy and the overall uptake. |
| Matthew Z. Dudley et al. (2022) [34] | United States | Influenza | Pregnant women | RCT | Patient-centered intervention | Educational videos through MomsTalkShots, algorithmically tailored application to pregnant women’s vaccine attitudes, including intentions | MomsTalkShots increased the perceived risk of maternal influenza infection and confidence in influenza vaccine efficacy. |
| Paula M. Frewa et al. (2014) [35] | United States | Influenza | Pregnant women | RCT | Patient-centered intervention | Two types of messages: positively oriented (“gain-frame”) messages communicate information by emphasizing the benefits of receiving the vaccine, and negatively oriented (“loss-frame”) messages emphasize the risks of not receiving the vaccine | Neither gain- nor loss-framed messages were significantly associated with an increased likelihood of influenza vaccination among pregnant women. |
| Mark H. Yudin et al. (2017) [36] | Canada | Influenza | Pregnant women | RCT | Patient-centered intervention | Two messages weekly for four consecutive weeks, reinforcing that vaccination against influenza is recommended for all pregnant women and is safe during pregnancy and breastfeeding | Weekly text messages did not increase the likelihood of getting vaccinated during pregnancy. |
| Ya-Wen Chang et al. (2022) [37] | Taiwan | Influenza | Pregnant women | Multicenter randomized controlled trial | Patient-centered intervention | An “Influenza Vaccination Reminder Application” was evaluated for improving vaccination intention among pregnant women. | The intervention statistically significantly increased pregnant women’s knowledge about influenza and vaccines, strengthened their positive attitudes towards maternal influenza vaccination, and promoted positive behavioral intention toward influenza vaccination. |
| Claudio Costantino et al. (2021) [38] | Italy | Influenza and Tdap | Pregnant women | Multicenter, pre- and post-educational intervention | Patient-centered intervention | Educational intervention on vaccination during pregnancy, immunization during life course, and vaccination recommended in Italy conducted by healthcare workers during childbirth classes | The educational intervention improved considerably the vaccination uptake during pregnancy. |
| Joanne Parsons et al. (2022) [39] | United Kingdom | Influenza | Pregnant women | Before and after interventional study | Patient-centered intervention | 4 min long animation addressing beliefs about the risk of influenza and the efficacy of the vaccination. | An increased appraisal of the likelihood of getting flu during pregnancy and severity of influenza infection during pregnancy, and increased intentions to accept influenza vaccination during pregnancy |
| Helena C. Maltezou et al. (2019) [40] | Greece | Influenza | Pregnant women | Before and after interventional study | Patient-centered intervention | A leaflet that was given if the participant asked for it. It included information about the complications due to influenza infection among pregnant women and neonates and the efficacy and safety of influenza vaccine administered during pregnancy. | Educational intervention was associated with an increased uptake rate of 19.5% among pregnant women compared to <2% in the past years. |
| Stefania Bruno et al. (2021) [41] | Italy | Influenza | Pregnant women | Pre–post intervention study | Patient-centered intervention | Training sessions carried out during a birthing preparation course, aimed at increasing the attitude toward vaccination among pregnant women | Vaccination knowledge and attitude significantly increased after a training session. |
| Nutan B. Hebballi et al. (2022) [42] | United States | Tdap | Postpartum women | Before and after intervention study | Patient-centered intervention | A brief educational intervention session about maternal pertussis and the Tdap vaccine was given to interested hospitalized postpartum women, after which the Tdap vaccine was offered to eligible patients who did not receive it while they were pregnant. Medical records were reviewed to determine if surveyed participants received the vaccine before discharge. | A total of 25% were vaccinated before the study as part of routine hospital-based screening, and 38.2% were vaccinated after the intervention. Uptake increased with no significant difference before and after intervention. |
| Aaliyah Momani et al. (2023) [43] | Jordan | COVID-19 | Pregnant and postpartum women | Quasi-experimental pre–post intervention study | Patient-centered intervention | Individual-centered tele-education (interactive education phone sessions, phone calls consultancy, text messages, and digital education booklet) was given to women in the intervention group for 2 weeks. | Education of pregnant women decreased hesitancy and improved willingness to be vaccinated against COVID-19. |
| Hallas Donna et al. (2023) [44] | United States | Influenza and Tdap | Pregnant women | Quasi-experimental intervention study | Patient-centered intervention | Study materials are provided online. The intervention was created to motivate participants to seek further information from scientific sources that were available to all study participants on the researchers’ website. | A total of 82% of vaccine-hesitant pregnant women had full prenatal vaccination coverage after receiving the intervention. The implemented intervention for vaccine-hesitant pregnant women was effective in shifting their status from hesitant to acceptor. |
| Elizabeth Helen Hayles et al. (2014) [45] | Australia | Tdap | Postpartum women | Quasi-experimental intervention study | Patient-centered intervention | Evaluate the role of message-framing vs. standard health information in the promotion of Tdap vaccination | Among susceptible mothers, 70% were vaccinated postintervention. No difference in vaccination rates, which were similar between groups. Overall pertussis vaccine coverage increased from 23% to 77%, and the ‘trusted’ environment with minimal access barriers had increased baseline pertussis vaccine coverage from 23% to 77%. |
| Joseph G. Giduthurim et al. (2019) [46] | India | Influenza | Pregnant women | RCT | Provider-focused intervention | Clinicians were interviewed and provided with antenatal influenza vaccination (AIV) implementation recommendations (global, academic, and local). | Engaging clinicians effectively reduced missed opportunities for AIV in urban middle-class settings. The absence of any similar impact in slum-based clinics might be the result of critical limitations of vaccine access. |
| C. Bonneau et al. (2010) [47] | France | Tdap | Postpartum women | Pre–post intervention study | Provider-focused intervention | Doctors and midwives received educational training on the benefits of pertussis vaccination during postpartum. Then, they provided oral (twice: midwife and doctor) and written information about pertussis and prescription for the Tdap vaccine for postpartum women. | Limited effect of the intervention At follow-up, vaccine uptake increased by 8%. |
| Sylvia Yeh et al. (2014) [48] | United States | Tdap | Postpartum women | Cluster randomized controlled trial | Health system intervention | A two-stage intervention: an “opt-in” order as part of the preprinted postpartum orders. Then, the intervention simplified the delivery of vaccinations by implementing a policy with standing orders for postpartum vaccination for Tdap and seasonal H1N1 influenza vaccination. | The introduction of the opt-in order achieved an increase in postpartum vaccination from 0% to 18%. The introduction of the standing order approach resulted in a further increase to 69%. No postpartum Tdap vaccinations were documented in the comparison hospital. |
| William E. Trick, et al. (2010) [49] | United States | Tdap | Postpartum women | Before and after intervention study | Health system intervention | Computer-based clinical decision support system incorporated into the hospital’s information system. When an order for iron supplementation was entered, a dialogue box was displayed containing a Tdap recommendation reminder, and an order for Tdap was generated and sent to the pharmacy and nursing staff unless the order was deselected. | The computer-based clinical decision support algorithm dramatically increased the Tdap vaccination uptake rate of postpartum women. |
| Sara E Mazzoni et al. (2016) [50] | United States | Influenza, Tdap and human papillomavirus (HPV) | Pregnant and postpartum women | Multicenter, pre–post multiple interventions | Multilevel intervention | 1—Education sessions for non-provider medical staff on HPV and Tdap in pregnancy; 2—Existing standing orders for vaccines were revised or expanded depending on the vaccine; for instance, before the intervention, a standing order for a vaccine would be processed only if the vaccine was covered by insurance. After the intervention, an order for all indicated vaccines regardless of insurance; 3—Standing orders expanded to include influenza in the outpatient setting. For Tdap, each clinic began stocking and administering Tdap. Additional staff training, including providers, was conducted. Patient handouts were created and routinely given out at each first antenatal session and ultrasound visit. | The uptake rate of influenza vaccination increased from 35.4% in the preintervention period to 46.0% after the intervention. Tdap vaccination increased from 87.6% before the intervention period to 94.5% in the period after intervention. |
| Yinan Li et al. (2022) [51] | Canada | Tdap | Pregnant women | A quasi-experimental multicenter study | Health system intervention | Four province-based implementation models of maternal Tdap vaccine delivery: 1—existing standard of practice model, at local community service centers; 2—family medicine groups; 3—obstetrics clinic; 4— during the oral glucose challenge test (done during pregnancy to screen for gestational diabetes). | Compared with local community service centers, overall vaccine coverage was significantly higher when Tdap was offered in family medicine groups or an obstetrics clinic providing antenatal care. The oral glucose challenge test model did not improve overall vaccine coverage. |
| Po-Jen Cheng et al. (2015) [52] | Taiwan | Tdap | Postpartum women | Pre–post intervention study | Multilevel intervention | Intensive physician and nursing education programs about early-onset neonatal Streptococcus Group B (GBS) infection, neonatal pertussis infection, and perinatal preventive strategies for both GBS and pertussis, followed by an office-based intervention incorporating pertussis education programs into prenatal GBS screening clinics. | Tdap vaccination was more likely during the postintervention period compared with the preintervention period. |
| Sean T. O’Leary et al. (2019) [53] | United States | Influenza, Tdap and HPV | Pregnant women | Cluster randomized controlled trial | Multilevel intervention | Designation of vaccination champions, staff/provider training, assistance with vaccine purchasing/management, identification of eligible patients, standing order implementation, chart review/feedback, and patient education materials. Control practices continued usual care. | No significant differences between intervention and control groups for the uptake of influenza vaccine among pregnant women. Observed study arms increased their uptake. No significant differences in uptake of the Tdap vaccine in the intervention group vs. control groups. |
| A.T. Chamberlain et al. (2015) [54] | United States | Influenza and Tdap | Pregnant women | A cluster-randomized trial | Multilevel intervention | Identification of a vaccine champion, provider-to-patient talking points, educational brochures, posters, lapel buttons, and iPads loaded with a patient-centered tutorial. | Antenatal influenza and Tdap vaccination uptake was higher in the intervention group than in the control group, although not statistically significantly different. |
| Saad B. Omer et al. (2022) [55] | United States | Influenza and Tdap | Pregnant women | Cluster- and individually randomized controlled trial | Multilevel intervention | Obstetric clinics are randomized to receive the practice and provider-level interventions or continue their usual standard of care. The practice-level intervention: identification of a vaccination champion and implementation of the Assessment, Feedback, Incentives and Exchange program [56]. Provider-level interventions included Continuing Medical Education module. Patient-level intervention: theory-driven individually tailored application was developed. | No significant difference in vaccine uptake for either influenza or Tdap between the different study arms. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayouni, I.; Amponsah-Dacosta, E.; Noll, S.; Kagina, B.M.; Muloiwa, R. Interventions to Improve Knowledge, Attitudes, and Uptake of Recommended Vaccines during Pregnancy and Postpartum: A Scoping Review. Vaccines 2023, 11, 1733. https://doi.org/10.3390/vaccines11121733
Ayouni I, Amponsah-Dacosta E, Noll S, Kagina BM, Muloiwa R. Interventions to Improve Knowledge, Attitudes, and Uptake of Recommended Vaccines during Pregnancy and Postpartum: A Scoping Review. Vaccines. 2023; 11(12):1733. https://doi.org/10.3390/vaccines11121733
Chicago/Turabian StyleAyouni, Imen, Edina Amponsah-Dacosta, Susanne Noll, Benjamin M. Kagina, and Rudzani Muloiwa. 2023. "Interventions to Improve Knowledge, Attitudes, and Uptake of Recommended Vaccines during Pregnancy and Postpartum: A Scoping Review" Vaccines 11, no. 12: 1733. https://doi.org/10.3390/vaccines11121733