

Implementation Strategies Used to Increase Human Papillomavirus Vaccination Uptake by Adolescent Girls in Sub-Saharan Africa: A Scoping Review
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Method
2.1. Inclusion Criteria
2.1.1. Participants
2.1.2. Concept
2.1.3. Context
2.2. Types of Sources
2.3. Search Strategy
2.4. Sources of Evidence Selection
2.5. Data Extraction and Charting
2.6. Data Analysis and Presentation
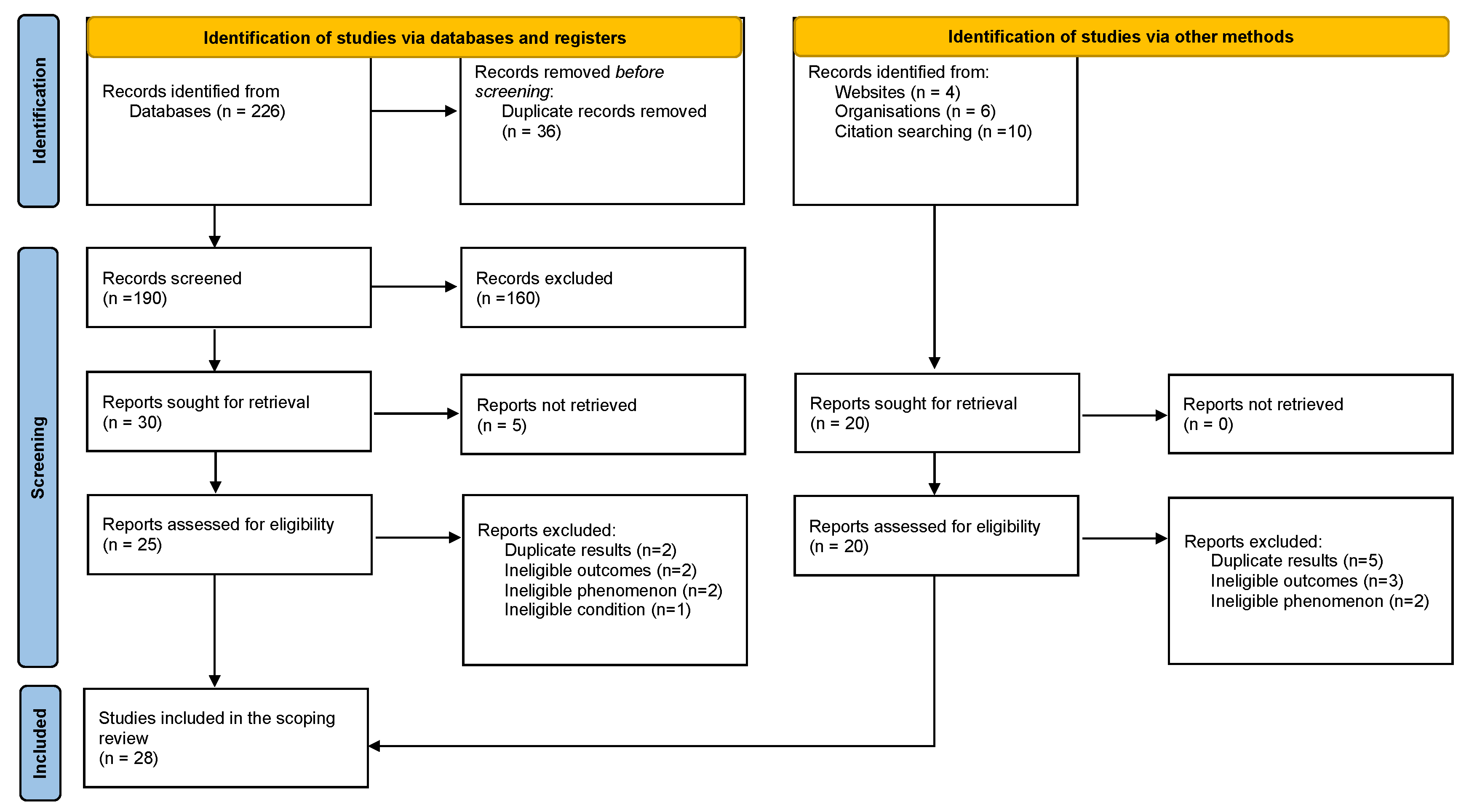
3. Results
3.1. Characteristics of Included Studies
3.2. Characteristics of the Eligible Adolescent Girls
3.3. Vaccine Delivery Approaches
3.4. Implementation Strategies According to ERIC Compilation
3.5. Targeted Stakeholders for Implementation Strategies
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loke, A.Y.; Kwan, M.L.; Wong, Y.-T.; Wong, A.K.Y. The Uptake of Human Papillomavirus Vaccination and Its Associated Factors Among Adolescents: A Systematic Review. J. Prim. Care Community Health 2017, 8, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Weekly Epidemiological Report; World Health Organisation: Geneva, Switzerland, 2009; pp. 117–132.
- Forman, D.; de Martel, C.; Lacey, C.J.; Soerjomataram, I.; Lortet-Tieulent, J.; Bruni, L.; Vignat, J.; Ferlay, J.; Bray, F.; Plummer, M.; et al. Global Burden of Human Papillomavirus and Related Diseases. Vaccine 2012, 30 (Suppl. S5), F12–F23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vuyst, H.; Alemany, L.; Lacey, C.; Chibwesha, C.J.; Sahasrabuddhe, V.; Banura, C.; Denny, L.; Parham, G.P. The Burden of Human Papillomavirus Infections and Related Diseases in Sub-Saharan Africa. Vaccine 2013, 31, F32–F46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruni, L.; Diaz, M.; Castellsagué, X.; Ferrer, E.; Bosch, F.X.; de Sanjosé, S. Cervical Human Papillomavirus Prevalence in 5 Continents: Meta-Analysis of 1 Million Women with Normal Cytological Findings. J. Infect. Dis. 2010, 202, 1789–1799. [Google Scholar] [CrossRef] [Green Version]
- de Sanjosé, S.; Diaz, M.; Castellsagué, X.; Clifford, G.; Bruni, L.; Muñoz, N.; Bosch, F.X. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: A meta-analysis. Lancet Infect. Dis. 2007, 7, 453–459. [Google Scholar] [CrossRef]
- Schiffman, M.; Doorbar, J.; Wentzensen, N.; de Sanjosé, S.; Fakhry, C.; Monk, B.J.; Stanley, M.A.; Franceschi, S. Carcinogenic human papillomavirus infection. Nat. Rev. Dis. Prim. 2016, 2, 16086. [Google Scholar] [CrossRef]
- Yimer, N.B.; Mohammed, M.A.; Solomon, K.; Tadese, M.; Grutzmacher, S.; Meikena, H.K.; Alemnew, B.; Sharew, N.T.; Habtewold, T.D. Cervical cancer screening uptake in Sub-Saharan Africa: A systematic review and meta-analysis. Public health 2021, 195, 105–111. [Google Scholar] [CrossRef]
- Coleman, J.S.; Cespedes, M.S.; Cu-Uvin, S.; Kosgei, R.J.; Maloba, M.; Anderson, J.; Wilkin, T.; Jaquet, A.; Bohlius, J.; Anastos, K.; et al. An Insight Into Cervical Cancer Screening and Treatment Capacity in Sub Saharan Africa. J. Low. Genit. Tract Dis. 2016, 20, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Mumba, J.M.; Kasonka, L.; Owiti, O.B.; Andrew, J.; Lubeya, M.K.; Lukama, L.; Kasempa, C.; Msadabwe, S.C.; Kalinda, C. Cervical cancer diagnosis and treatment delays in the developing world: Evidence from a hospital-based study in Zambia. Gynecol. Oncol. Rep. 2021, 37, 100784. [Google Scholar] [CrossRef]
- Kelly, H.; Weiss, H.A.; Benavente, Y.; de Sanjose, S.; Mayaud, P.; Qiao, Y.-L.; Feng, R.-M.; DeVuyst, H.; Tenet, V.; Jaquet, A.; et al. Association of antiretroviral therapy with high-risk human papillomavirus, cervical intraepithelial neoplasia, and invasive cervical cancer in women living with HIV: A systematic review and meta-analysis. Lancet HIV 2017, 5, e45–e58. [Google Scholar] [CrossRef] [Green Version]
- Nyambe, A.; Lubeya, M.K. Cervical cancer and HIV in Zambian women. Lancet Glob. Health 2021, 9, e734–e735. [Google Scholar] [CrossRef]
- Rohner, E.; Mulongo, M.; Pasipamire, T.; Oberlin, A.M.; Goeieman, B.; Williams, S.; Lubeya, M.K.; Rahangdale, L.; Chibwesha, C.J. Mapping the cervical cancer screening cascade among women living with HIV in Johannesburg, South Africa a. Int. J. Gynecol. Obstet. 2020, 152, 53–59. [Google Scholar] [CrossRef]
- Mukosha, M.; Muyunda, D.; Mudenda, S.; Lubeya, M.K.; Kumwenda, A.; Mwangu, L.M.; Kaonga, P. Knowledge, attitude and practice towards cervical cancer screening among women living with human immunodeficiency virus: Implication for prevention strategy uptake. Nurs. Open 2022, 10, 2132–2141. [Google Scholar] [CrossRef]
- World Health Organisation. Position Paper October 2014. Available online: http://www.who.int/wer/2014/wer8943.pdf (accessed on 20 September 2021).
- World Health Organization. Evidence-based recommendations on Human Papilloma Virus (HPV) vaccines schedules: Back-ground paper for SAGE discussions. Retrieved May 2014, 5, 2017. [Google Scholar]
- World Health Organization. One-Dose Human Papillomavirus (HPV) Vaccine Offers Solid Protection against Cervical Cancer. 2022. Available online: https://www.who.int/news/item/11-04-2022-one-dose-human-papillomavirus-(hpv)-vaccine-offers-solid-protection-against-cervical-cancer (accessed on 11 April 2022).
- Kisaakye, E.; Namakula, J.; Kihembo, C.; Kisakye, A.; Nsubuga, P.; Babirye, J.N. Level and factors associated with uptake of human papillomavirus infection vaccine among female adolescents in Lira District, Uganda. Pan Afr. Med. J. 2018, 31, 184. [Google Scholar] [CrossRef]
- Pugliese-Garcia, M.; Heyerdahl, L.W.; Mwamba, C.; Nkwemu, S.; Chilengi, R.; Demolis, R.; Guillermet, E.; Sharma, A. Factors influencing vaccine acceptance and hesitancy in three informal settlements in Lusaka, Zambia. Vaccine 2018, 36, 5617–5624. [Google Scholar] [CrossRef] [PubMed]
- Wigle, J.; Coast, E.; Watson-Jones, D. Human papillomavirus (HPV) vaccine implementation in low and middle-income countries (LMICs): Health system experiences and prospects. Vaccine 2013, 31, 3811–3817. [Google Scholar] [CrossRef] [Green Version]
- Sankaranarayanan, R.; Anorlu, R.; Sangwa-Lugoma, G.; Denny, L.A. Infrastructure Requirements for Human Papillomavirus Vaccination and Cervical Cancer Screening in Sub-Saharan Africa. Vaccine 2013, 31, F47–F52. [Google Scholar] [CrossRef] [PubMed]
- Falcaro, M.; Castañon, A.; Ndlela, B.; Checchi, M.; Soldan, K.; Lopez-Bernal, J.; Elliss-Brookes, L.; Sasieni, P. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: A register-based observational study. Lancet 2021, 398, 2084–2092. [Google Scholar] [CrossRef] [PubMed]
- Dorji, T.; Nopsopon, T.; Tamang, S.T.; Pongpirul, K. Human papillomavirus vaccination uptake in low-and middle-income countries: A meta-analysis. Eclinicalmedicine 2021, 34, 100836. [Google Scholar] [CrossRef] [PubMed]
- Rujumba, J.; Akugizibwe, M.; Basta, N.E.; Banura, C. Why don’t adolescent girls in a rural Uganda district initiate or complete routine 2-dose HPV vaccine series: Perspectives of adolescent girls, their caregivers, healthcare workers, community health workers and teachers. PLoS ONE 2021, 16, e0253735. [Google Scholar] [CrossRef]
- Ports, K.A.; Reddy, D.M.; Rameshbabu, A. Barriers and Facilitators to HPV Vaccination: Perspectives from Malawian Women. Women Health 2013, 53, 630–645. [Google Scholar] [CrossRef] [Green Version]
- Kayombo, M. Zambia’s Hurdles in Cervical Cancer Fight. Daily Mail. 3 March 2022. Available online: http://www.daily-mail.co.zm/zambias-hurdles-in-cervical-cancer-fight/ (accessed on 3 March 2022).
- Amponsah-Dacosta, E.; Kagina, B.M.; Olivier, J. Health systems constraints and facilitators of human papillomavirus immunization programmes in sub-Saharan Africa: A systematic review. Health Policy Plan. 2020, 35, 701–717. [Google Scholar] [CrossRef]
- Lubeya, M.K.; Chibwesha, C.J.; Mwanahamuntu, M.; Mukosha, M.; Maposa, I.; Kawonga, M. Correlates of Parental Consent to Human Papillomavirus Vaccine Uptake by Their Adolescent Daughters in ZAMBIA: Application of the Health Belief Model. Vaccines 2023, 11, 912. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem; World Health Organisation: Geneva, Switzerland, 2020; ISBN 978-92-4-001410-7. [Google Scholar]
- Powell, B.J.; McMillen, J.C.; Proctor, E.K.; Carpenter, C.R.; Griffey, R.T.; Bunger, A.C.; Glass, J.E.; York, J.L. A Compilation of Strategies for Implementing Clinical Innovations in Health and Mental Health. Med. Care Res. Rev. 2011, 69, 123–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delany-Moretlwe, S.; Kelley, K.F.; James, S.; Scorgie, F.; Subedar, H.; Dlamini, N.R.; Pillay, Y.; Naidoo, N.; Chikandiwa, A.; Rees, H. Human Papillomavirus Vaccine Introduction in South Africa: Implementation Lessons From an Evaluation of the National School-Based Vaccination Campaign. Glob. Health Sci. Pr. 2018, 6, 425–438. [Google Scholar] [CrossRef] [Green Version]
- Niccolai, L.M.; Hansen, C.E. Practice- and Community-Based Interventions to Increase Human Papillomavirus Vaccine Coverage. JAMA Pediatr. 2015, 169, 686–692. [Google Scholar] [CrossRef] [Green Version]
- Acampora, A.; Grossi, A.; Barbara, A.; Colamesta, V.; Causio, F.A.; Calabrò, G.E.; Boccia, S.; de Waure, C. Increasing HPV Vaccination Uptake among Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 7997. [Google Scholar] [CrossRef] [PubMed]
- Mavundza, E.J.; Iwu-Jaja, C.J.; Wiyeh, A.B.; Gausi, B.; Abdullahi, L.H.; Halle-Ekane, G.; Wiysonge, C.S. A Systematic Review of Interventions to Improve HPV Vaccination Coverage. Vaccines 2021, 9, 687. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Powell, B.J.; Waltz, T.J.; Chinman, M.J.; Damschroder, L.J.; Smith, J.L.; Matthieu, M.M.; Proctor, E.K.; Kirchner, J.E. A refined compilation of implementation strategies: Results from the Expert Recommendations for Implementing Change (ERIC) project. Implement. Sci. 2015, 10, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waltz, T.J.; Powell, B.J.; Matthieu, M.M.; Damschroder, L.J.; Chinman, M.J.; Smith, J.L.; Proctor, E.K.; Kirchner, J.E. Use of concept mapping to characterize relationships among implementation strategies and assess their feasibility and importance: Results from the Expert Recommendations for Implementing Change (ERIC) study. Implement. Sci. 2015, 10, 109. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Évid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Lubeya, M.K.; Mwanahamuntu, M.; Chibwesha, C.; Mukosha, M.; Wamunyima, M.M.; Kawonga, M. Implementation strategies to increase human papillomavirus vaccination uptake for adolescent girls in sub-Saharan Africa: A scoping review protocol. PLoS ONE 2022, 17, e0267617. [Google Scholar] [CrossRef]
- Munn, Z.; Aromataris, E.; Tufanaru, C.; Stern, C.; Porritt, K.; Farrow, J.; Lockwood, C.; Stephenson, M.; Moola, S.; Lizarondo, L.; et al. The development of software to support multiple systematic review types. Int. J. Evid.-Based Health 2019, 17, 36–43. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Miller, W.L.; Crabtree, B.F. The dance of interpretation. Doing Qual. Res. 1999, 2, 127–143. [Google Scholar]
- Lamontagne, D.S.; Barge, S.; Le, N.T.; Mugisha, E.; Penny, M.E.; Gandhi, S.; Janmohamed, A.; Kumakech, E.; Mosqueira, N.R.; Nguyen, N.Q.; et al. Human papillomavirus vaccine delivery strategies that achieved high coverage in low- and middle-income countries. Bull. World Health Organ. 2011, 89, 821–830B. [Google Scholar] [CrossRef]
- Galagan, S.R.; Paul, P.; Menezes, L.; LaMontagne, D.S. Influences on parental acceptance of HPV vaccination in demonstration projects in Uganda and Vietnam. Vaccine 2013, 31, 3072–3078. [Google Scholar] [CrossRef]
- Gallagher, K.E.; Howard, N.; Kabakama, S.; Mounier-Jack, S.; Griffiths, U.K.; Feletto, M.; Burchett, H.E.D.; LaMontagne, D.S.; Watson-Jones, D. Lessons learnt from human papillomavirus (HPV) vaccination in 45 low- and middle-income countries. PLoS ONE 2017, 12, e0177773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ladner, J.; Besson, M.-H.; Hampshire, R.; Tapert, L.; Chirenje, M.; Saba, J. Assessment of eight HPV vaccination programs implemented in lowest income countries. BMC Public Health 2012, 12, 370. [Google Scholar] [CrossRef] [Green Version]
- Kabakama, S.; Gallagher, K.E.; Howard, N.; Mounier-Jack, S.; Burchett, H.E.D.; Griffiths, U.K.; Feletto, M.; LaMontagne, D.S.; Watson-Jones, D. Social mobilisation, consent and acceptability: A review of human papillomavirus vaccination procedures in low and middle-income countries. BMC Public Health 2016, 16, 834. [Google Scholar] [CrossRef] [Green Version]
- Tsu, V.D.; LaMontagne, D.S.; Atuhebwe, P.; Bloem, P.N.; Ndiaye, C. National implementation of HPV vaccination programs in low-resource countries: Lessons, challenges, and future prospects. Prev. Med. 2021, 144, 106335. [Google Scholar] [CrossRef] [PubMed]
- Whitworth, H.; Changalucha, J.; Baisley, K.; Watson-Jones, D. Adolescent Health Series: HPV infection and vaccination in sub-Saharan Africa: 10 years of research in Tanzanian female adolescents—narrative review. Trop. Med. Int. Health 2021, 26, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- Ladner, J.; Besson, M.-H.; Audureau, E.; Rodrigues, M.; Saba, J. Experiences and lessons learned from 29 HPV vaccination programs implemented in 19 low and middle-income countries, 2009–2014. BMC Health Serv. Res. 2016, 16, 575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moodley, I.; Mubaiwa, V.; Tathiah, N.; Denny, L. High uptake of Gardasil vaccine among 9—12-year-old schoolgirls participating in an HPV vaccination demonstration project in KwaZulu-Natal Province. S. Afr. Med. J. 2013, 103, 318–321. [Google Scholar] [CrossRef] [Green Version]
- Snyman, L.C.; Dreyer, G.; Visser, C.; Botha, M.H.; Van Der Merwe, F.H. The Vaccine and Cervical Cancer Screen project 2 (VACCS 2): Linking cervical cancer screening to a two-dose HPV vaccination schedule in the South-West District of Tshwane, Gauteng, South Africa. S. Afr. Med. J. 2015, 105, 191. [Google Scholar] [CrossRef] [Green Version]
- Jones, A.; Kawesa-Newell, N. Using branded behaviour change communication to create demand for the HPV vaccine among girls in Malawi: An evaluation of Girl Effect’s Zathu mini magazine. Vaccine 2021, 40, A107–A115. [Google Scholar] [CrossRef]
- Msyamboza, K.P.; Mwagomba, B.M.; Valle, M.; Chiumia, H.; Phiri, T. Implementation of a human papillomavirus vaccination demonstration project in Malawi: Successes and challenges. BMC Public Health 2017, 17, 599. [Google Scholar] [CrossRef] [Green Version]
- Watson-Jones, D.; Baisley, K.; Ponsiano, R.; Lemme, F.; Remes, P.; Ross, D.; Kapiga, S.; Mayaud, P.; de Sanjosé, S.; Wight, D.; et al. Human Papillomavirus Vaccination in Tanzanian Schoolgirls: Cluster-Randomized Trial Comparing 2 Vaccine-Delivery Strategies. J. Infect. Dis. 2012, 206, 678–686. [Google Scholar] [CrossRef] [Green Version]
- Mphuru, A.; Li, A.J.; Kyesi, F.; Mwengee, W.; Mazige, F.; Nshunju, R.; Shayo, B.; Giattas, M.R.; Loharikar, A.; Lyimo, D. National introduction of human papillomavirus (HPV) vaccine in Tanzania: Programmatic decision-making and implementation. Vaccine 2022, 40, A2–A9. [Google Scholar] [CrossRef] [PubMed]
- Mugisha, E.; Lamontagne, D.S.; Katahoire, A.R.; Murokora, D.; Kumakech, E.; Seruyange, R.; Tsu, V.D. Feasibility of delivering HPV vaccine to girls aged 10 to 15 years in Uganda. Afr. Health Sci. 2015, 15, 33–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PATH CHaDCC, and the Uganda National Expanded, (UNEPI) PoI. HPV Vaccination in Africa: Lessons Learned From a Pilot Program in Uganda. 2011. Available online: https://www.path.org/resources/hpv-vaccination-in-africa-lessons-learned-from-a-pilot-program-in-uganda/ (accessed on 12 April 2021).
- Raesima, M.M.; Forhan, S.E.; Voetsch, A.C.; Hewitt, S.; Hariri, S.; Wang, S.A.; Pelletier, A.R.; Letebele, P.; Pheto, T.; Ramogola-Masire, D.; et al. Human Papillomavirus Vaccination Coverage Among School Girls in a Demonstration Project—Botswana, 2013. Morb. Mortal. Wkly. Rep. 2015, 64, 1147–1149. [Google Scholar] [CrossRef] [Green Version]
- Wamai, R.G.; Ayissi, C.A.; Oduwo, G.O.; Perlman, S.; Welty, E.; Manga, S.; Ogembo, J.G. Assessing the Effectiveness of a Community-Based Sensitization Strategy in Creating Awareness About HPV, Cervical Cancer and HPV Vaccine Among Parents in North West Cameroon. J. Community Health 2012, 37, 917–926. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation Africa. First Lady Launches the HPV Vaccine Project for the Prevention of Cervical Cancer. 15 April 2015. Available online: https://www.afro.who.int/news/first-lady-launches-hpv-vaccine-project-prevention-cervical-cancer (accessed on 5 January 2023).
- Drokow, E.K.; Effah, C.Y.; Agboyibor, C.; Sasu, E.; Amponsem-Boateng, C.; Akpabla, G.S.; Ahmed, H.A.W.; Sun, K. The Impact of Video-Based Educational Interventions on Cervical Cancer, Pap Smear and HPV Vaccines. Front. Public Health 2021, 9, 681319. [Google Scholar] [CrossRef] [PubMed]
- Soi, C.; Gimbel, S.; Chilundo, B.; Muchanga, V.; Matsinhe, L.; Sherr, K. Human papillomavirus vaccine delivery in Mozambique: Identification of implementation performance drivers using the Consolidated Framework for Implementation Research (CFIR). Implement. Sci. 2018, 13, 151. [Google Scholar] [CrossRef] [Green Version]
- Chigbu, C.O.; Onyebuchi, A.K.; Onyeka, T.C.; Odugu, B.U.; Dim, C.C. The impact of community health educators on uptake of cervical and breast cancer prevention services in Nigeria. Int. J. Gynecol. Obstet. 2017, 137, 319–324. [Google Scholar] [CrossRef]
- Binagwaho, A.; Wagner, C.; Gatera, M.; Karema, C.; Nutt, C.; Ngaboa, F. Achieving high coverage in Rwanda’s national human papillomavirus vaccination programme. Bull. World Health Organ. 2012, 90, 623–628. [Google Scholar] [CrossRef]
- Casey, R.M.; Adrien, N.; Badiane, O.; Diallo, A.; Roka, J.L.; Brennan, T.; Doshi, R.; Garon, J.; Loharikar, A. National introduction of HPV vaccination in Senegal—Successes, challenges, and lessons learned. Vaccine 2021, 40, A10–A16. [Google Scholar] [CrossRef]
- Engel, D.; Afeli, A.D.J.; Morgan, C.; Zeck, W.; Ross, D.A.; Vyankandondera, J.; Bloem, P.; Adjeoda, K.R. Promoting adolescent health through integrated human papillomavirus vaccination programs: The experience of Togo. Vaccine 2021, 40, A100–A106. [Google Scholar] [CrossRef]
- World Health Organisation Africa. Human Papillomavirus (HPV) Vaccine Introduced in Zambia. 27 May 2013. Available online: https://www.afro.who.int/news/human-papilloma-virus-hpv-vaccine-introduced-zambia (accessed on 23 January 2023).
- LaMontagne, D.S.; Manangazira, P.; Marembo, J.; Chigodo, C.; Zvamashakwe, C.; Tshuma, E.; Marima, E.; Chindedza, K.; Ndlela, E.; Mooney, J. HPV vaccination coverage in three districts in Zimbabwe following national introduction of 0,12 month schedule among 10 to 14 year old girls. Vaccine 2021, 40, A58–A66. [Google Scholar] [CrossRef]
- Watson-Jones, D.; Tomlin, K.; Remes, P.; Baisley, K.; Ponsiano, R.; Soteli, S.; de Sanjosé, S.; Changalucha, J.; Kapiga, S.; Hayes, R.J. Reasons for Receiving or Not Receiving HPV Vaccination in Primary Schoolgirls in Tanzania: A Case Control Study. PLoS ONE 2012, 7, e45231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walling, E.B.; Benzoni, N.; Dornfeld, J.; Bhandari, R.; Sisk, B.A.; Garbutt, J.; Colditz, G. Interventions to Improve HPV Vaccine Uptake: A Systematic Review. Pediatrics 2016, 138, e20153863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krokidi, E.; Rao, A.P.; Ambrosino, E.; Thomas, P.P.M. The impact of health education interventions on HPV vaccination uptake, awareness, and acceptance among people under 30 years old in India: A literature review with systematic search. Front. Reprod. Health 2023, 5, 1151179. [Google Scholar] [CrossRef]
- Rani, U.; Darabaner, E.; Seserman, M.; Bednarczyk, R.A.; Shaw, J. Public Education Interventions and Uptake of Human Papillomavirus Vaccine: A Systematic Review. J. Public Health Manag. Pract. 2020, 28, E307–E315. [Google Scholar] [CrossRef]
- Smulian, E.A.; Mitchell, K.R.; Stokley, S. Interventions to increase HPV vaccination coverage: A systematic review. Hum. Vaccines Immunother. 2016, 12, 1566–1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubeya, M.K.; Nyirenda, J.C.Z.; Kabwe, J.C.; Mukosha, M. Knowledge, Attitudes and Practices Towards Human Papillomavirus Vaccination Among Medical Doctors at a Tertiary Hospital: A Cross Sectional Study. Cancer Control 2022, 29, 10732748221132646. [Google Scholar] [CrossRef]
- Brewer, N.T.; Gottlieb, S.L.; Reiter, P.L.; McRee, A.-L.; Liddon, N.; Markowitz, L.; Smith, J.S. Longitudinal Predictors of Human Papillomavirus Vaccine Initiation Among Adolescent Girls in a High-Risk Geographic Area. Sex. Transm. Dis. 2011, 38, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Holman, D.M.; Benard, V.; Roland, K.B.; Watson, M.; Liddon, N.; Stokley, S. Barriers to Human Papillomavirus Vaccination Among US Adolescents. JAMA Pediatr. 2014, 168, 76–82. [Google Scholar] [CrossRef] [Green Version]
- Howard, N.; Mounier-Jack, S.; Gallagher, K.E.; Kabakama, S.; Griffiths, U.K.; Feletto, M.; Lamontagne, D.S.; Burchett, H.E.D.; Watson-Jones, D. The value of demonstration projects for new interventions: The case of human papillomavirus vaccine introduction in low- and middle-income countries. Hum. Vaccines Immunother. 2016, 12, 2475–2477. [Google Scholar] [CrossRef] [Green Version]
- Kaul, S.; Do, T.Q.N.; Hsu, E.; Schmeler, K.M.; Montealegre, J.R.; Rodriguez, A.M. School-based human papillomavirus vaccination program for increasing vaccine uptake in an underserved area in Texas. Papillomavirus Res. 2019, 8, 100189. [Google Scholar] [CrossRef]
- Muhamad, N.A.; Buang, S.N.; Jaafar, S.; Jais, R.; Tan, P.S.; Mustapha, N.; Lodz, N.A.; Aris, T.; Sulaiman, L.H.; Murad, S. Achieving high uptake of human papillomavirus vaccination in Malaysia through school-based vaccination programme. BMC Public Health 2018, 18, 1402. [Google Scholar] [CrossRef] [PubMed]
- Bonner, K.; Banura, C.; Basta, N.E. HPV vaccination strategies targeting hard-to-reach populations: Out-of-school girls in LMICs. Vaccine 2018, 36, 191–193. [Google Scholar] [CrossRef] [PubMed]
- Oketch, S.Y.; Ochomo, E.O.; Orwa, J.A.; Mayieka, L.M.; Abdullahi, L.H. Communication strategies to improve human papillomavirus (HPV) immunisation uptake among adolescents in sub-Saharan Africa: A systematic review and meta-analysis. BMJ Open 2023, 13, e067164. [Google Scholar] [CrossRef]
- Simas, C.; Munoz, N.; Arregoces, L.; Larson, H.J. HPV vaccine confidence and cases of mass psychogenic illness following immunization in Carmen de Bolivar, Colombia. Hum. Vaccines Immunother. 2018, 15, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, S.; Ueda, Y.; Yagi, A.; Matsuzaki, S.; Kobayashi, E.; Kimura, T.; Miyagi, E.; Sekine, M.; Enomoto, T.; Kudoh, K. HPV vaccination in Japan: What is happening in Japan? Expert Rev. Vaccines 2019, 18, 323–325. [Google Scholar] [CrossRef] [Green Version]
- Stratton, K.; Ford, A.; Rusch, E.; Clayton, E.W.; Committee to Review Adverse Effects of Vaccines. Adverse Effects of Vaccines: Evidence and Causality; National Academies Press: Washington, DC, USA, 2012; pp. 1–894. [Google Scholar]
- Corcoran, B.; Clarke, A.; Barrett, T. Rapid response to HPV vaccination crisis in Ireland. Lancet 2018, 391, 2103. [Google Scholar] [CrossRef] [Green Version]
- UNICEF Human Papillomavirus (HPV) Vaccine: Supply and Demand Update. 2020. Available online: https://www.unicef.org/supply/reports/human-papillomavirus-hpv-vaccine-supply-and-demand-update (accessed on 23 June 2023).


{kind=link}
| First Author Name; Year [Reference] | Title of Article | Country of Study | Type of Data Source | Type of Program | Targeted Stakeholder | School Grade/Age of Girls | Funding Agency |
|---|---|---|---|---|---|---|---|
| Binagwaho, Agnes; 2012 [65] | Achieving high coverage in Rwanda’s national human papillomavirus vaccination program | Rwanda | Perspective | National | Policymakers, Non-governmental organizations, Donor community, Clergy, Teachers, Healthcare workers, parents, adolescent girls, community health workers | Grade 6 or 12 years | Merck |
| Casey, Rebecca M.; 2021 [66] | National introduction of HPV vaccination in Senegal: Successes, challenges, and lessons learnt | Senegal | Research—cross sectional | National | Policymakers, healthcare workers, nongovernmental organizations, parents, adolescent girls | 9 years | The Gavi |
| Chigbu, Chibuike O.; 2017 [64] | The impact of community health educators on uptake of cervical and breast cancer prevention services in Nigeria | Nigeria | Research—pre- and post-design | Sub-national | Nurses | 9–13 years | Out of pocket |
| Delany-Muretwe; 2018 [31] | Human papillomavirus vaccine introduction in South Africa: implementation lessons from an evaluation of the national school-based vaccination campaign | South Africa | Research—cross sectional | National program | District leaders, EPI Leaders, Healthcare workers, teachers, defense forces, nursing schools, politicians, journalists | Grade 4 or 9–13 years | The Gavi |
| Drokow, Emmanuel K.; 2021 [62] | The Impact of Video-Based Educational Interventions on Cervical Cancer, Pap Smear, and HPV Vaccines | Ghana | Research—pre- and post-design | Sub-national research | Parents | N/A | The Gavi |
| Engel, Danielle; 2021 [67] | Promoting adolescent health through integrated human papillomavirus vaccination programs: The experience of Togo | Togo | Evaluation | Demonstration in two districts | Technical partners, healthcare workers, adolescents, family members, community health workers | Grade 5 or 10 years | The Gavi |
| Galagan, Sean R.; 2013 [44] | Influences on parental acceptability of HPV vaccination in demonstration projects in Uganda and Vietnam | Uganda/Vietnam | Research—cross sectional | Demonstration program in two districts | Parents | Grade 5 or 10 years | The Gavi |
| Gallagher, Katherine E.; 2017 [45] | Lessons learnt from delivering HPV vaccine in 45 LMICs | 45 LMICs (SSA countries included) | Research—Ecological study | Demonstration program | Policymakers, healthcare workers, non-governmental organizations, parents, adolescent girls | 9–18 years | Variable |
| Jones, Amy; 2021 [53] | Using branded behavior change communication to create demand for the HPV vaccine among girls in Malawi: An evaluation of Girl Effect’s Zathu mini magazine | Malawi | Research—pre- and post-design | Sub-national research | Girls, parents, and influencers | 9 years | N/A |
| Kabakama, Severin; 2016 [47] | Social mobilization, consent, and acceptability: A review of human papillomavirus vaccination procedures in low- and middle-income countries | 37 LMICs (SSA countries included) | Literature review | LMICs—National and sub-national | Girls, parents, and influencers | Variable, routine | Variable |
| Ladner, Joe; 2016 [50] | Experiences and lessons learned from 29 HPV vaccination programs implemented in 19 low- and middle-income countries, 2009–2014 | LMICS (SSA countries included) | Perspective | Demonstration program | parents, community, government, multiple | 9–13 years | Global Access Program |
| Ladner, Joel; 2012 [46] | Assessment of implementation of HPV vaccination programs in eight of the lowest-income countries (SSA—Cameroon and Lesotho) | LMICs—Cameroon and Lesotho included | Program evaluation | Demonstration program | Policymakers, educators, healthcare workers | 9–13 years | Global Access Program |
| LaMontagne, Scott D.; 2021 [69] | HPV vaccination coverage in three districts in ZIMBABWE following the national introduction of a schedule of 0 to 12 months among girls aged 10 to 14 years | Zimbabwe | Research—cross sectional | National program | Parents | Multi-age cohort (10–14 years) | The Gavi |
| LaMontagne, D. Scott; 2011 [43] | Human papillomavirus vaccine delivery strategies that achieved high coverage in low- and middle-income countries | LMICs/Uganda | Research—cross sectional | Demonstration in two districts | Healthcare workers, community mobilizers, Parents, Adolescent girls | 9–14 years | Merck and Co./Gloxosmithline |
| Moodley, Indres; 2013 [51] | High uptake of Gardasil vaccine among schoolgirls aged 9–12 years participating in an HPV vaccination demonstration project in KwaZulu-Natal, South Africa | South Africa | Research—cross sectional | Demonstration, one province | Nurses, teachers, religious, district health, district education health | 9–12 years | Research grant |
| Mpuru, Alex; 2021 [56] | National introduction of human papillomavirus (HPV) vaccine in Tanzania: Programmatic decision-making and implementation | Tanzania | Report | National | EPI TWG, policymakers, politicians, religious leaders, healthcare workers, community health volunteers, school personnel, media personnel | 14 years | The Gavi |
| Msyamboza, Kelias P.; 2017 [54] | Implementation of human papillomavirus vaccination demonstration project in Malawi: Successes and challenges | Malawi | Research—cross sectional | Demonstration program in two districts | Healthcare workers, policymakers, parents | Grade 4 or 9–13 years out-of-school | The Gavi |
| Mugisha, Emmanuel; 2015 [57] | Feasibility of delivering HPV vaccine to girls aged 10–15 years in Uganda | Uganda | Research—cross sectional | Demonstration project in two districts | District leaders, EPI Leaders, Healthcare workers | Grade 5 or 10 years | Glaxosmithkline Biologicals SA |
| Program for Approriate Technology in Health; 2011 [58] | HPV Vaccination in Africa, lessons learnt from a pilot program in UGANDA | Uganda | Report | Demonstration project in two districts | Policymakers, planners, teachers, community members, adolescent girls, parents | Grade 5 or 10 years | Glaxosmithkline biologicals SA |
| Raesima, Mmakgomo M.; 2015 [59] | Human Papillomavirus Vaccination Coverage Among School Girls in a Demonstration Project—Botswana, 2013 | Botswana | Report | Demonstration program, one district | Teachers, parents, adolescent girls, and healthcare workers | Grades 4 to 6 or >9 years | Pink Ribbon Red Ribbon |
| Snyman, Leon; 2015 [52] | The Vaccine and Cervical Cancer Screen project 2 (VACCS 2): Linking cervical cancer screening to a two-dose HPV vaccination schedule in the South West District of Tshwane, Gauteng, South Africa | South Africa | Research—cross sectional | Sub-national Gauteng and Western provinces | Adolescents and female parents | Grades 4 to 7 or 9 years | Manufacturer donation |
| Soi, Catherine; 2018 [63] | Human papillomavirus vaccine delivery in Mozambique: identification of implementation performance drivers using the Consolidated Framework for Implementation Research (CFIR) | Mozambique | Evaluation | Demonstration—three regions | Healthcare workers, policymakers, community leaders | Grade 4 | The Gavi |
| Tsu, Vivien; 2021 [48] | National implementation of HPV vaccination programs in low-resource countries: Lessons, challenges, and future prospects | LMICs (SSA countries included) | Literature review | National programs | Journalists, healthcare workers, teachers, parents, community leaders, adolescent girls | Variable, routine | Variable |
| Wamai, Richard; 2012 [60] | Assessing the effectiveness of a community-based sensitization strategy in creating awareness about HPV, cervical cancer, and HPV vaccine among parents in North West Cameroon | Cameroon | Research—cross sectional | Regional—one district | Parents | 9–13 years | Church donation |
| Watson, Deborah-Jones; 2012 [55] | Human papillomavirus vaccination in Tanzanian schoolgirls: Cluster-randomized trial comparing two vaccine-delivery strategies | Tanzania | Research—cluster randomized trial | Regional research in two districts | Teachers, Adolescents, Parents | Grade 6 or 12 years | Wellcome trust |
| Whitworth, Hilary; 2021 [49] | Adolescent Health Series: HPV infection and vaccination in sub-Saharan Africa: 10 years of research in Tanzanian female adolescents—narrative review | SSA | Literature review | Regional—SSA | Policymakers, teachers, healthcare workers, parents, adolescent girls | N/A | N/A |
| World Health Organisation; 2013 [68] | Human papillomavirus (HPV) vaccine introduced in Zambia | Zambia | Report | Demonstration in three districts | Policymakers, teachers, healthcare workers, parents, adolescent girls | Grade 4 or 10 years | The Gavi |
| World Health Organisation; 2015 [61] | First Lady launches the HPV vaccine project for the prevention of cervical cancer | The Gambia | Report | Demonstration project in two districts | Political figures, policymakers, parents, adolescent girls | 9–13 years | The Gavi |
| Implementation Strategies Cluster | Total No. of Strategies within Each Cluster | Strategies Used per Cluster across 28 Papers No. (%) | Total No. of Times Strategy Identified by Scoping Review |
|---|---|---|---|
| 1. Use evaluative and iterative strategies | 10 | 100% (10/10) | 113 |
| 2. Provide interactive assistance | 4 | 100% (4/4) | 51 |
| 3. Adapt and tailor to context | 4 | 75% (3/4) | 45 |
| 4. Develop stakeholder interrelationships | 17 | 94% (16/17) | 164 |
| 5. Train and educate stakeholders | 11 | 100% (11/11) | 131 |
| 6. Support clinicians | 5 | 80% (4/5) | 26 |
| 7. Engage consumers | 5 | 100% (5/5) | 65 |
| 8. Utilize financial strategies | 9 | 44% (4/9) | 27 |
| 9. Change Infrastructure | 8 | 63% (5/8) | 46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lubeya, M.K.; Mwanahamuntu, M.; Chibwesha, C.J.; Mukosha, M.; Monde, M.W.; Kawonga, M. Implementation Strategies Used to Increase Human Papillomavirus Vaccination Uptake by Adolescent Girls in Sub-Saharan Africa: A Scoping Review. Vaccines 2023, 11, 1246. https://doi.org/10.3390/vaccines11071246
Lubeya MK, Mwanahamuntu M, Chibwesha CJ, Mukosha M, Monde MW, Kawonga M. Implementation Strategies Used to Increase Human Papillomavirus Vaccination Uptake by Adolescent Girls in Sub-Saharan Africa: A Scoping Review. Vaccines. 2023; 11(7):1246. https://doi.org/10.3390/vaccines11071246
Chicago/Turabian StyleLubeya, Mwansa Ketty, Mulindi Mwanahamuntu, Carla J. Chibwesha, Moses Mukosha, Mercy Wamunyima Monde, and Mary Kawonga. 2023. "Implementation Strategies Used to Increase Human Papillomavirus Vaccination Uptake by Adolescent Girls in Sub-Saharan Africa: A Scoping Review" Vaccines 11, no. 7: 1246. https://doi.org/10.3390/vaccines11071246